
Abstract
Insertion of indwelling urinary catheters should be performed in a way that minimizes the risk of introducing bacteria to the urinary bladder. Nurses and assistant nurses from three departments at an acute-care hospital in Sweden answered a questionnaire about their insertion of urinary catheterization. Of the 563 nurses, 92% answered the questionnaire. Among the 492 who performed catheterization, 58% (n = 287) said that they followed the hospital guideline. Two-thirds of those following the hospital guideline said that they used clean technique and one-third sterile technique. In all, 82% considered the catheter should be kept sterile while inserted but only 16% described all the prerequisites to achieve this. Over 90% of the respondents performed catheterization less than once a week. Our conclusion is that a guideline should describe every step of catheterization in detail and that an evidence-based process for implementation of the guideline is necessary to achieve uniformity in performance.
Keywords
Introduction
Indwelling urinary catheter (IUC) use is associated with symptomatic urinary tract infection, usually called catheter-associated urinary tract infection (CAUTI), as well as asymptomatic bacteriuria. CAUTI constitutes an important risk for blood stream infection.1–3 The prevalence of indwelling urinary catheter use among inpatients in the US and Europe is in the range of 17–24%.4,5 Among inpatients in Sweden the prevalence of IUC use in 2017 was 22.6% according to the yearly national survey covering just over 15,000 patients. 6
As pointed out in previous studies, use of indwelling urinary catheters should be limited and when used catheter insertion and maintenance should be performed in a way that minimizes the risk of introducing bacteria to the urinary bladder.1,2,7 Guidelines from The Centers for Disease Control and Prevention (CDC) and The European Association of Urology Nurses (EAUN) recommend ‘sterile technique’ when inserting an indwelling urinary catheter. Sterile technique includes a sterile catheter, sterile equipment and maintaining sterility during catheter insertion.8,9
A method for urinary catheterization called ‘clean technique’ was introduced in the early 1970s by Lapides et al. as a safe way to perform intermittent self-catheterization in patients with neurogenic bladder dysfunctions.10,11 Since around 1990 the Swedish national guidelines for urinary catheterization were altered from sterile technique to clean technique not only for intermittent self-catheterization performed by patients but also for indwelling urinary catheterization performed by professionals. 12 Sterile technique included a sterile catheter, a sterile set for catheterization, sterile gloves, sterile equipment, sterile draping and sterile fluids for peri-urethral cleaning before catheterization. With the introduction of clean technique in the Swedish national guidelines for urinary catheterization, a sterile set for catheterization was excluded and the need for sterile draping of the catheterization area was not included. Further, non-sterile equipment as well as non-sterile gloves and fluids were introduced. With these changes, sterile draping was no longer mandatory, and the sterile urinary catheter could be held and inserted with non-sterile gloves and/or non-sterile forceps. These changes from sterile to clean technique for insertion of an indwelling urinary catheter have influenced what has been taught at nursing schools for professional education in Sweden during recent decades.
The purpose of the present national guidelines, revised November 2017, is to emphasize the importance of maintaining the sterility of the indwelling urinary catheter during insertion. There is, however, no recommendation for sterile equipment and non-sterile examination gloves are recommended. 13 The confusion about catheterization techniques in practice has been observed by the European Association of Urology Nurses (EAUN). 14
In Sweden, urinary catheterization of patients at hospitals is mostly performed by nurses but also by assistant nurses after personal written delegation from a nurse. Local hospital guidelines are based on the national guidelines. The local guideline for urinary bladder catheterization via the urethra, at the hospital that participated in this study, was launched in 2006 and updated in 2011. The terms ‘sterile technique’ and ‘clean technique’ are not used and in contrast to the national guidelines it is clearly stated that the urinary catheter should only be touched by sterile gloves or sterile forceps. Draping is not mentioned in the guideline.
In the light of these changes of the routines for indwelling urinary catheterization in Sweden over the years our aim was to investigate how nurses and assistant nurses described their performance of catheterization in daily work, their opinion on sterility of the catheter, how they denominated the routine they practice, and whether they followed the local hospital guideline for urinary catheterization.
Method
Design
The study design was comparative and descriptive, and the study was based on a structured questionnaire.
Measurement
The questionnaire included seven questions concerning occupation, time of professional education and time of employment and 12 questions concerning performance of indwelling urinary catheterization (i.e. frequency of catheter insertion, type of equipment used when inserting an indwelling urinary catheter, sterility requirements for the catheter and equipment used and designation of insertion technique).
Setting and participants
The participants were nurses and assistant nurses employed at the acute-care hospital with 600 beds. All participants worked on wards caring for inpatients at the departments of cardiology and internal medicine and surgery. At the end of 2015 the medical director at the hospital and the managers of the three departments were contacted by email to inform them about the study and to gain their permission to perform it. At the beginning of 2016, head nurses of the included departments were contacted to inform them about the study. Head nurses from 15 wards answered that insertion of indwelling urinary catheters was practiced in their ward and 14 of them accepted participation in the study. A list containing names and professions of all the nurses and assistant nurses working in each ward was received from the head nurses. Employees on long-term sick leave and parental leave were excluded. All other nurses and assistant nurses were included. Each included person received a serial number and the questionnaire received the same serial number. During spring 2016 the questionnaires were distributed to all included persons together with written information about the study. Verbal information was given in groups and, in some cases, individually. The participants were asked to not discuss the questions in the questionnaire during the period of participation. Each participant received a preaddressed envelope and was informed that participation was by choice. They were asked to return the completed or unanswered questionnaire in the preaddressed envelope to the study conductor within two weeks. No information was given to the head nurses concerning who answered the questionnaire and who did not.
Construct validity
Prior to the study being conducted a nurse and an assistant nurse at another hospital in Stockholm County Council individually answered the questionnaire to evaluate the comprehensiveness of the questions.
Data analysis
Microsoft Office Excel was used for entering the data from the questionnaires. Statistical analysis for significance was performed with the chi-squared test by using the software Epi-info 7™ (https://www.cdc.gov/epiinfo/index.html). Odds Ratios (OR) > 1.0 and p-values < 0.05 were regarded as significant.
Ethical considerations
Participation in the study was by choice. During the process of entering and analysing data in the computer only the serial numbers were used. The study was not subject to judgement by an ethics committee as it was regarded as a quality evaluation project.
Results
Distribution of nurses and assistant nurses from the departments of cardiology and internal medicine and surgery.
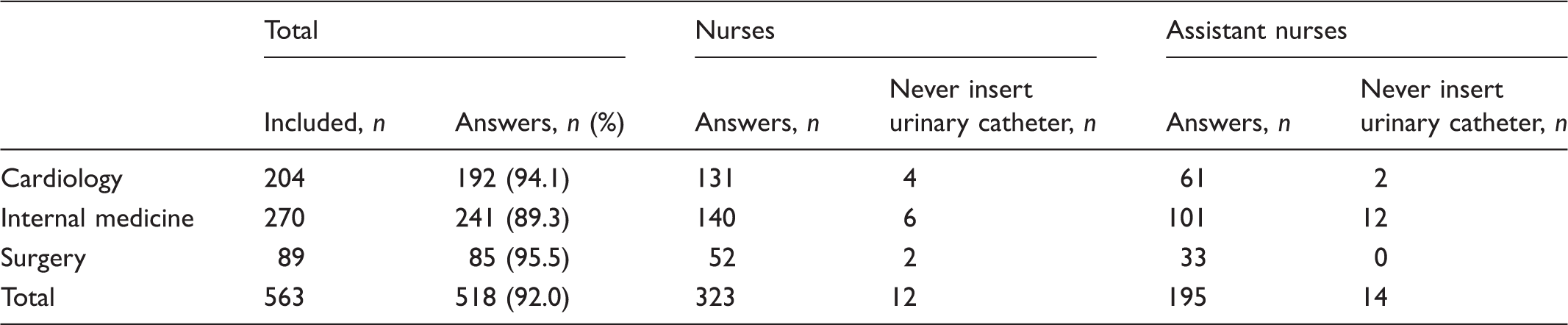
Below we present results from 7 of the 12 questions concerning performance of catheter insertion. Answers concerning peri-urethral cleaning, single-use equipment, hand disinfection and bladder irrigation will be presented separately.
Adherence to the hospital guideline
Number (n) and distribution of staff belonging to different categories among respondents who answered ‘Yes’ to the question ‘Do you perform insertion of indwelling urinary catheters according to the hospital guideline?’
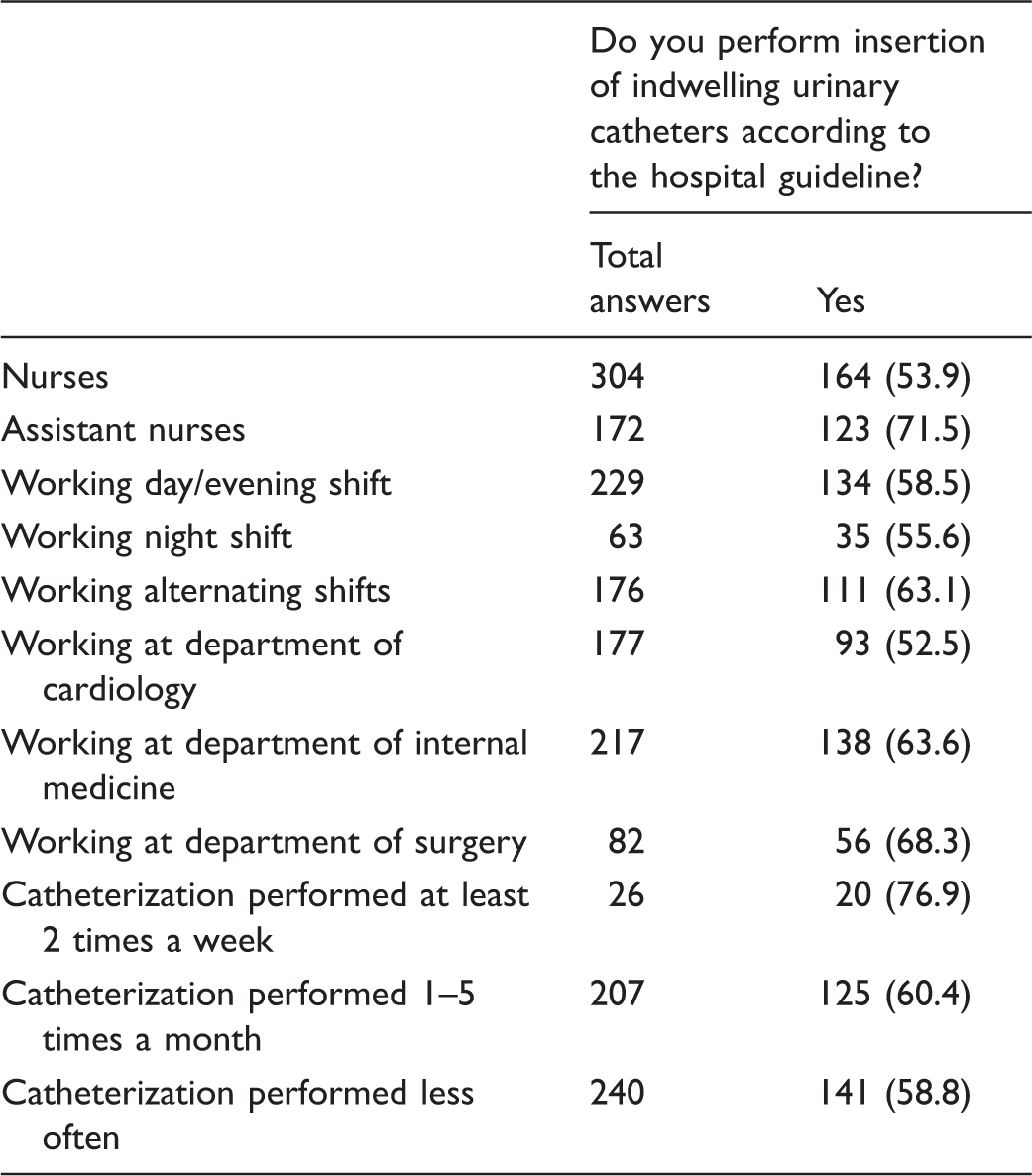
Among the 287 persons who said that they followed the hospital guideline for catheterization, 280 answered the question about sterile or clean technique. Of those, 88 (31.4%) said that they used a sterile technique and 192 (68.6%) said that they used a clean technique.
Sterile and clean technique
Among all nurses and all assistant nurses, 20.6% (64/311) and 41.4% (75/181) respectively said that they used a sterile technique when inserting a urinary catheter irrespective of whether claiming that they kept to the hospital guideline or not. Clean technique was self-reported to be practiced by 75.6% (235/311) of the nurses and 52.5% (95/181) of the assistant nurses. The question was not answered by 12 nurses and 11 assistant nurses.
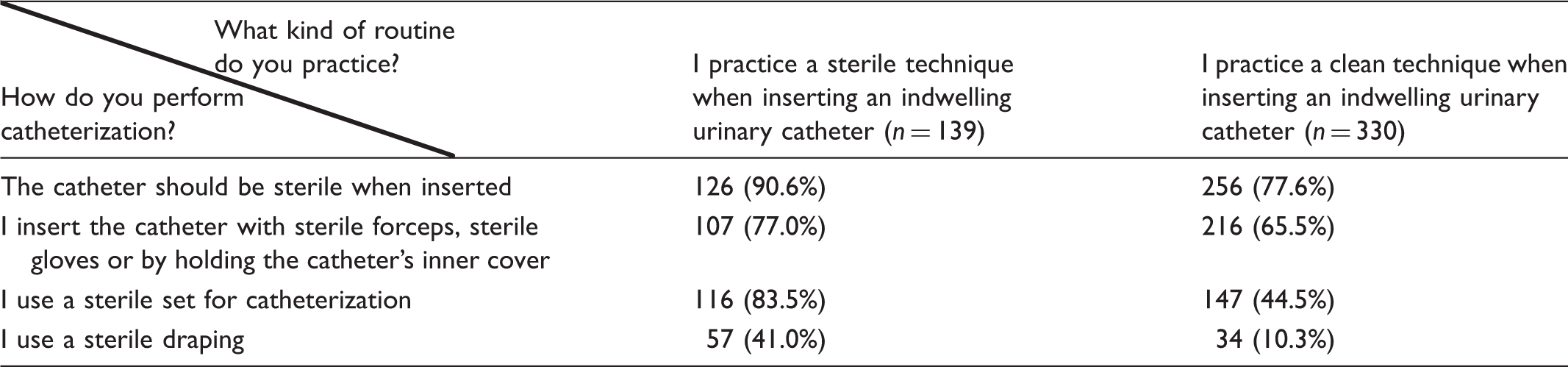
Performance during insertion of an indwelling urinary catheter in relation to catheterization technique.
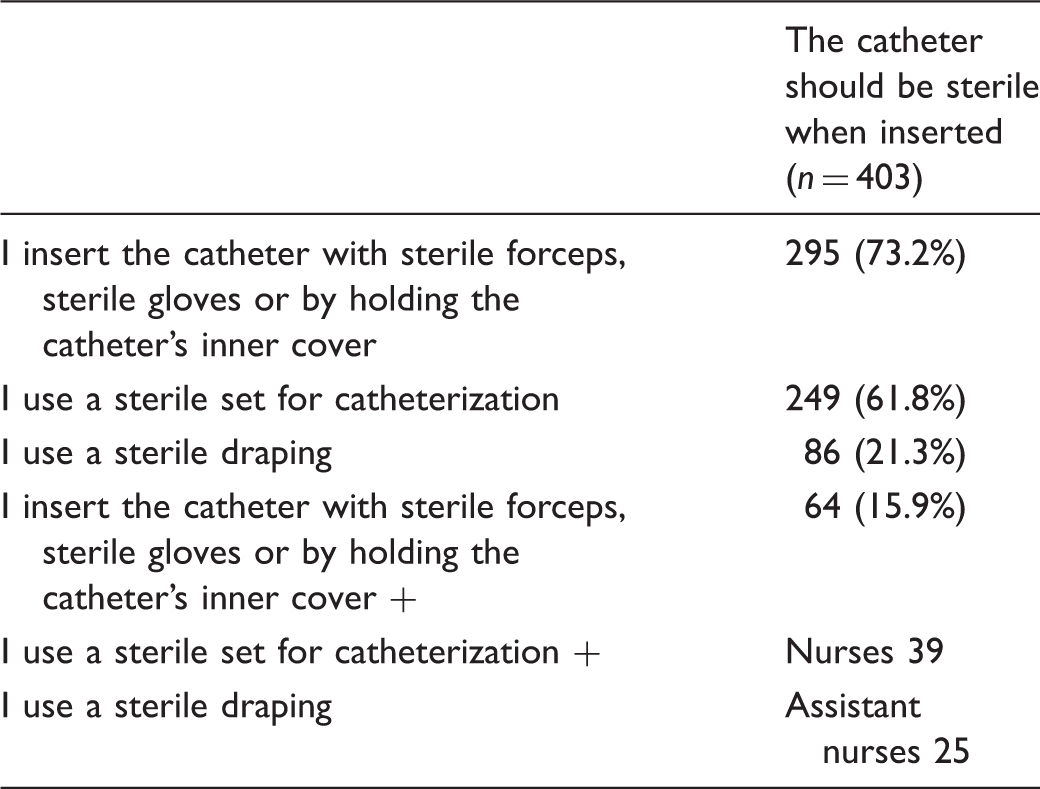
Sterility of the urinary catheter
Performance during insertion of an indwelling urinary catheter in relation to desired sterility of the catheter.
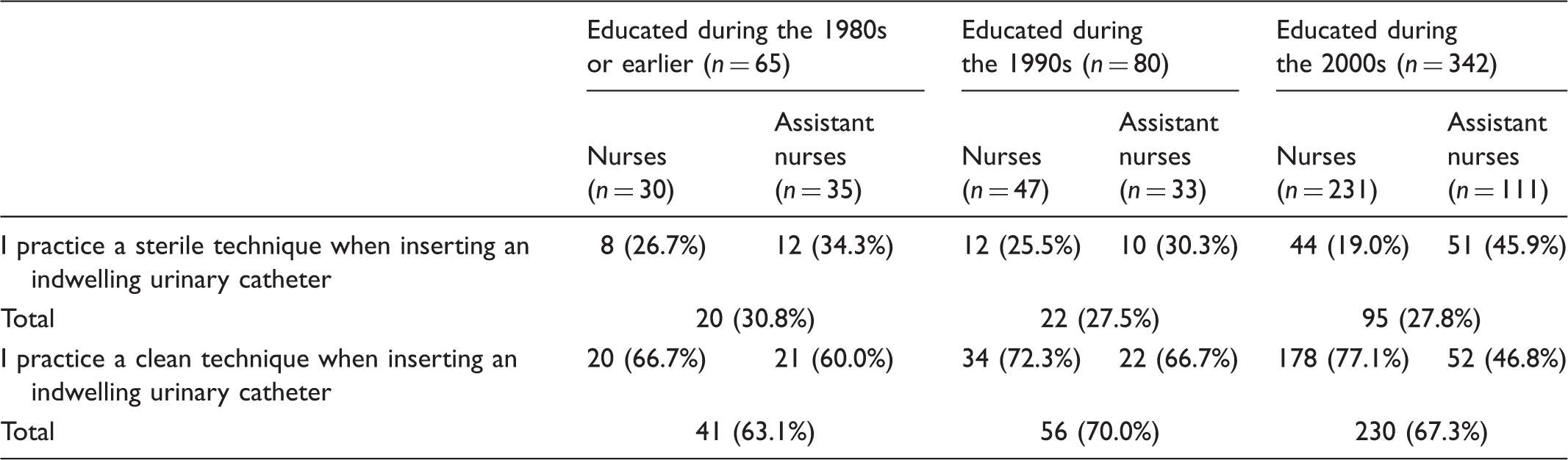
Opinion on sterile and clean technique in relation to time of education
Practice of sterile and clean technique when inserting an indwelling urinary catheter in relation to date of professional education.
Discussion
One of the strong recommendations in the CDC guidelines for prevention of catheter-associated urinary tract infections is to provide and implement a guideline for insertion of urinary catheters. 8 South Hospital, Stockholm, where this study was performed has one single guideline for urinary catheterization. The guideline is easily reached on the hospital internal website and should be well known by all staff. Nevertheless, only 58% of the participating nurses and assistant nurses said that they followed the hospital guideline. Among those who said that they followed the hospital guideline around two-thirds related to an insertion technique which they called clean technique and one-third a technique which they called sterile although the hospital guideline does not use either of those terms.
The results from our study reflect that the participants called their insertion technique, ‘sterile’ or ‘clean’ in their description of performance when inserting an indwelling urinary catheter, and showed a wide variation within the two groups. There was no significant difference between the two groups, ‘sterile’ and ‘clean’, as shown in Table 3. There were no differences in performance of catheterization irrespective of when nurses and assistant nurses went through their professional education.
Even though there is a single guideline for urinary catheter insertion at the study hospital this seems to be insufficient to achieve uniform practice. Nicolle emphasizes that besides written policies for catheter indications, catheter selection, insertion and maintenance, it is crucial to have sufficient staffing, staff education and adequate supplies in an infrastructure to support an effective programme for implementation. 1 The necessity of education, performance evaluation and feedback to employees is pointed out by many others.15–19 A single simulated skill checkoff is not enough according to the studies conducted by Gonzalez et al. and Manojlovich et al.15,20
The results from our study show that there is a need for recurrent theoretical education and simulated skill training on a regular basis to achieve knowledge about the hospital guideline for urinary catheter insertion as well as a more uniform performance of catheterization. Lack of repeated education and training regularly given to all nurses and assistant nurses may have contributed to maintenance of an insertion technique adopted during their professional education.
As at least 20% of Swedish hospital inpatients receive an indwelling urinary catheter it could be anticipated that the catheterization procedure was performed frequently by all nurses and assistant nurses. 6 In our study, however, 94% of the 473 participants answering the question about frequency of catheterization said that they performed indwelling urinary catheterization once a week or less often, which furthermore stresses the importance of a written, well known and implemented guideline.
Apart from influence from Lapides et al. who introduced ‘clean intermittent catheterization’ in the early 1970s the Swedish national guidelines for urinary catheterization were probably affected in the 1990s by a study by Carapeti et al. published in 1994 where 156 patients were randomized to sterile or non-sterile urethral catheterization when inserting an indwelling urinary catheter.10,11,21 The conclusion from that study was that clean technique is good enough for indwelling urinary catheterization. However, the urinary catheter was kept sterile in both study groups. The misinterpretation of the studies by Lapides et al. and Carapeti et al. and the confusion concerning the different techniques supports a need for clarification of terms both in national and local guidelines as pointed out by the EAUN. 14
Comparing the two groups in our study referring to practice of either ‘sterile technique’ or ‘clean technique’ there was a difference in opinion on sterility of the catheter as 91% in the ‘sterile technique group’ but only 77% in the ‘clean technique group’ claimed that the catheter should be kept sterile, although the hospital guideline stresses that the catheter should be kept sterile during catheterization. This difference in opinion did not significantly influence the performance of catheterization. Uncertainty concerning this important matter might lead to jeopardized patient safety.
Catheter insertion was mostly performed by using sterile forceps and/or sterile gloves in both the ‘sterile technique group’ and the ‘clean technique group’, which was in accordance with the hospital guideline. There were, however, about one-fifth of members of the ‘sterile technique group’ and about one-third of the ‘clean technique group’ who handled the urinary catheter with non-sterile forceps or non-sterile gloves, thus not keeping the catheter sterile. Among all participants declaring that they used clean technique in the questionnaire, 27 answered that they inserted the sterile catheter by holding it by its inner plastic cover, while there were no respondents performing this method among participants using sterile technique. Inserting a urinary catheter by its inner plastic cover is a difficult skill which not all have mastery of. Further, inner plastic covers on sterile indwelling catheters can have different constructions for opening, leading to difficulties to manage the catheter without touching it.
Using sterile forceps and sterile gloves is not enough to meet the requirements for aseptic technique in attempts to keep the sterility of the indwelling catheter while insertion. The sterile catheter must be protected from contact with the physical environment. This can be achieved by using sterile drapes to cover the insertion area. 8 Draping is not mentioned in the hospital guideline although a sterile draping to our opinion is a prerequisite for keeping the indwelling catheter sterile.
Only 15.9% of all participants in our study described their catheterization performance in a way that secured sterility of the catheter regardless of what they called their insertion technique. To secure patient safety and to minimize the risk of introducing bacteria to the urinary bladder during catheterization the national and local guidelines for indwelling urinary catheterization need to clarify exactly how to maintain the sterility of the urinary indwelling catheter while insertion. Further, the terms ‘clean technique’ and ‘sterile technique’ should not be used in the guidelines as this might cause confusion about the correct performance.
Limitations and strengths
A limitation of our study can be the possibility of misinterpretation of the question asked about whether draping was maintained during the whole process of catheterization or just used prior to catheter insertion when washing the outer genitalia. Self-reporting of behaviour rather than observation could affect the results of the study. However, the intention of the questionnaire, and the included questions, was to identify differences rather than the ‘correct’ technique. Self-reporting made it possible to include participants from different professions and departments. The response rate of the questionnaires was very high at 92% (518/563). This can be attributed to the interest and acceptance of the study among the medical director and other approached managers in the hospital. The information about the study given personally to the head nurses and the participants before the questionnaire may also have contributed to this high response rate.
Conclusions
Our study highlights that nurses and assistant nurses have different interpretations of the terms ‘sterile technique’ and ‘clean technique’ when they describe their performance of indwelling urinary catheterization. These variations in interpretations and techniques seem not to support an effort to minimize the risk of CAUTI and may jeopardize patient safety. In efforts focused on preventing healthcare-associated urinary tract infections, the results from our study may add to increased knowledge and more uniform practice in the procedure concerning catheterization techniques.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.