
Abstract
Being the spouse of a patient in a nursing home may be a conflicting experience. This article uses life-history interviews and the understanding of Bourdieu to understand and explain the phenomena. The data consist of five life-story interviews with two women and two men. The article looks at love and marriage structures during the lifetime of the agents. We also look at the development of the nursing home from a historical perspective. The research is based on Bourdieu’s theory with the purpose of understanding and explaining the experiences of the spouse: ‘Why is the experience of having a spouse in a nursing home often conflicting?’ The ambition of praxeological optics is to objectify subjectivist and objectivist factors. The understanding is constructed as a habitus based on the trilogy of Bourdieu. In order to endure and cope with the challenges, spouses need to be strong. According to our analysis lived life expressed in attitudes and actions in marriage and at the nursing home are closely linked. ‘For better or worse, in sickness and health’, is a key element in these relations. Staff need to focus more on spouses in order to avoid conflicts both between staff and spouse and between the spouses themselves.
Introduction
On a summer’s day, the first author sat with his father, while his mother’s life peacefully ebbed away. His mother had been a patient in a nursing home in western Norway for 2.5 years. Her death was expected, and the family was at her bedside day and night during the two final weeks of her life. She received good nursing and felt no pain, yet it is always difficult to let a loved one go. The first involuntary separation between mother and father occurred in 2008 when they were 84 and 81 years old. At the time they had been married for 57 years, but neither father’s nor mother’s physical condition made it possible to remain together. They had no desire to separate, but it had become obvious to their sons that conditions at home were unsustainable. Initially short stays at the nursing home alleviated the problems. Short-term admittance to nursing homes often depends on availability and the quality varies. After a year in a commercial (for-profit) 1 institution, mother moved to a municipal (non-profit) nursing home. Father didn’t always know how to relate to the different institutions and the institutions did not seem to have a consistent plan for how to receive or relate to him. How he was received seemed coincidental and subject to chance. This caused a lot of unnecessary stress. We can look beyond subjectivism and objectivism from the perspective of praxeological optics, by posing the following question:
Why is the experience of having a spouse in a nursing home often so conflicting?
Theoretical framework
The research covering significant others of patients in nursing homes usually refers to all relations. The collectively labelled group ‘significant others’ becomes the median for significant others in general, without any empirical adjustments in individual cases. Spouses, daughters, sons, nieces or others are all treated the same.2,3 In terms of the spouse, however, empirical studies from Scandinavia4,5 describe a lack of planning ahead of committing a spouse to the nursing home. This stage in the process was almost entirely dominated by professionals as well as being characterised by an ambivalent emotional response to the situation. Sandberg et al. 6 published an article in which they conclude that the relationship between staff and significant others in nursing homes are characterised as stressful and superficial. Nolan and Dellasega7(p. 723) conclude that: ‘There is a need to create a partnership between staff and family so that the care of the older person is improved and the carers’ need to remain involved is acknowledged’. According to Ade-Ridder and Kaplan, 8 moving a significant other to a nursing home may be daunting, and this is also confirmed in several other studies.6,7,9 These texts inspired investigations into the objectivistic dimension.
Existing research, based on praxeological optics
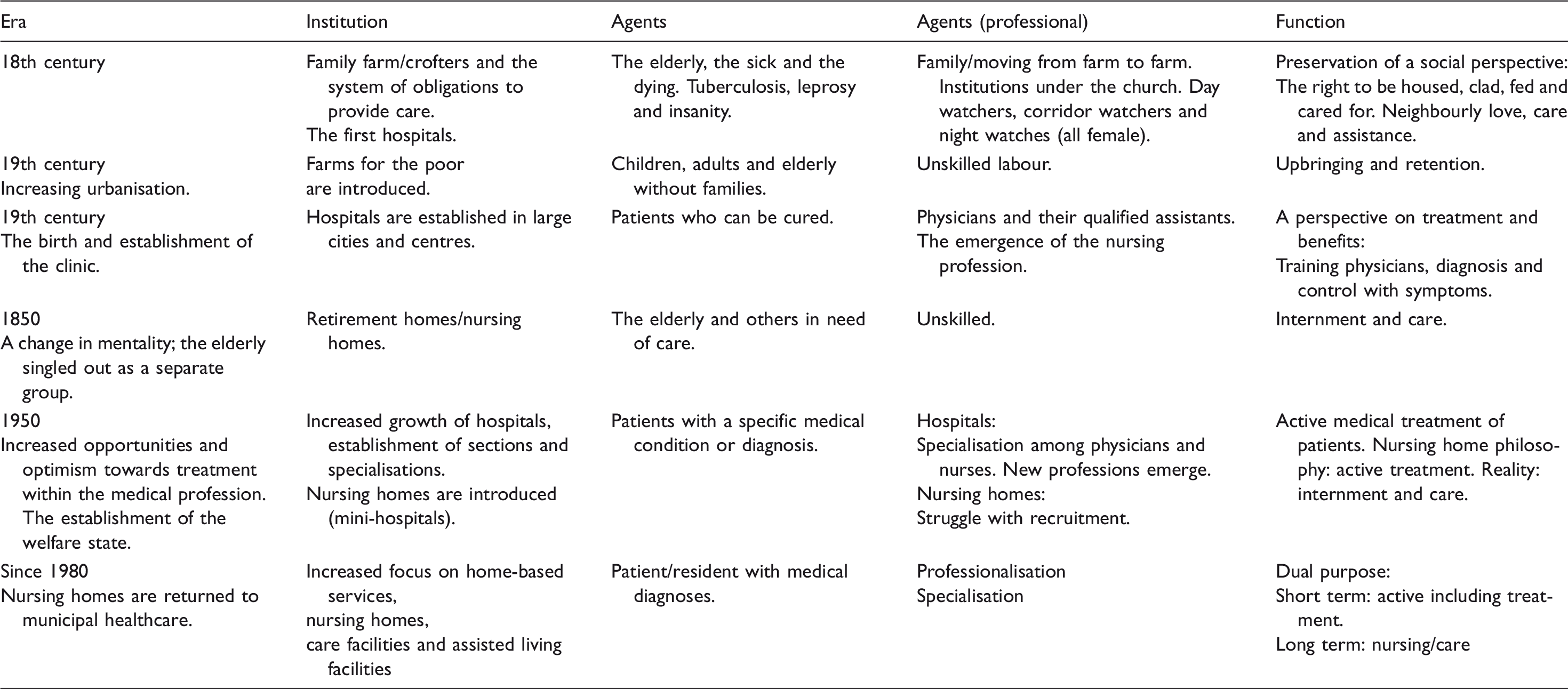
Visualisation of emergence and development of hospitals and nursing homes in Norway.
Situating marriage in a limited survey population
The Marriage Act was revised in 1927 and the burden of household support became a shared responsibility for husband and wife. Work in the home equalled paid labour and spouses were obliged to support each other financially. This may sound like marriage equality, but rights of property and salary still remained unregulated. Both parties retained rights to their separate belongings from before the marriage. 13 The new Marriage Act regulated the value of non-monetary efforts in the household and childcare. In 1995, this effort was valued to 40% of GNP. The major structural changes in marriage regulations occurred after 1950. The role of the traditional housewife changed and it became normal for mothers to take paid employment. In 1979, 70% of all households relied on two incomes, however, men were unaccustomed to childcare and domestic work and there were few kindergartens. 13
A story of love
Emotions are a factor somewhere between our human existence, the times we live in and cultural conditions. 13 Ideals, values, norms and expectations constantly change and family life adapts to these changes. Early modern societies dictated the choice of spouse, based on sense rather than emotion. Social class and class structures were maintained through marriage and childbirth, thereby also the transfer of values and attitudes. 13 Marriage confirmed obligations. Care for the elderly, children, the disabled and others were considered a family responsibility. Societies relied on these family structures to survive, but also societies in the form of neighbours and friends. 13
Method
The data consist of five interviews with two women and two men (aged 69–87 years) who have spouses in nursing homes. Each interview lasted approximately one hour. These couples were born during the 1930s and married during the 1950s, except the youngest born in 1946. The interviews were conducted in their homes but the first of a total of two interviews with Frida was conducted in the nursing home where her spouse lived.
Praxeological methodology: How a marriage is affected by separation
The research was based on Bourdieu’s theory with the purpose of understanding and explaining the spouse’s experiences. A subjective dimension was included; i.e. how the spouse experiences the situation, as well as an objective dimension; i.e. how they structure both the processionals and the patient’s significant others practic in the nursing home. The ambition of using praxeological optics was also to objectify subjectivist and objectivist factors. The researcher’s access to the research data was objectified with the same set of instruments (this is not confirmed by this article). We will not find answers to our questions using interviews alone. We collected data we included in a structural and historical analysis to explain the experiences the agents have encountered. By using constructions, theories and concepts as instruments, we created a possible explanation for the conflicts spouses refer to in their meetings with professional healthcare providers. Experiences provided opportunities for analysis. From a certain position or praxeological perspective we were able to translate these experiences: ‘The explanation of what happens on the spot is not to be found on the spot’.14(p. 202)
The basis for this philosophy was the theory of social practice regarding how people behave. How does a guest at a nursing home behave? Considering the fact that when we act we are often not aware of how and why we act. As humans, we often forget to read between the lines. We can find the tools to study social processes in mixed personal experiences, social conditions, historical preconditions and the cultural references of life histories. The relationship between personal and social conditions was in focus. 15 Bourdieu defined fields as ‘a network of objective relations’, 16 a structured social field comprising its own rules, forms of authority and legitimacy of perspectives and their positions in a cultural, economic and social context. 17 Bourdieu’s terminology was applied to human actions within Bourdieu-inspired research. Careful observance of symbolic violence, the habitus of the researcher and informer and how these interact were essential factors. The understanding of fields and different forms of capital and the positions and dispositions they created also contributed to understanding and explaining the content of the interviews. 18 In order to explain data in Bourdieu’s tradition interviews with agents are insufficient. It is necessary to describe the field and the agents and thereby we created a framework for dispositions as cultural and economic capital.10,19 We analysed content by using Bourdieu’s instruments to understand and explain events. We all experience our own subjective life history as well as an institutional life story.
Habitus as theoretical construct
Habitus is a key concept in Bourdieu’s philosophy and is described as a set of acquired dispositions to act, usually in the form of subconscious responses. 20 Habitus is often described as the socialised body where external structures have merged with internal structures to become cognitive templates for perception and classification. Consequently, Bourdieu talked about relationships between agents rather than what social psychology describes as interaction between agents. Habitus affects perception as well as classification, 16 in how we relate reflexively to the other. 18 Habitus is both an individual and collective embodied history. People before us have treaded the paths in our world. We have forgotten history as history because it appears self-evident and natural. 21 Habitus is a product of our collective history and objective structures that unify dispositions and social class, which often defines how the individual acts. There are, however, differences between disposition and habitus. Disposition refers to an inclination to act. It is invisible until it is set in motion or perhaps not set in motion. An attitude, on the other hand, is much more visible. Habitus is much more a disposition and active point of orientation than an attitude. Although we are unaware of it, habitus directs our actions on a subconscious level. Our responses are keyed in to the situation and the reality we face, yet the agent remains unaware of the orientation behind his actions. 22 The distinction between forms of capital and total volume creates distinctions between social positions. Dispositions represented by income and wealth (economic capital), combined with social capital (spouse, children, grandchildren, family) and cultural capital (education and interests), contribute to defining positions. 22
We can see the relation as a (practical) embodiment of our social lives where the body becomes a reminder of our experiences. Our social and family history has to some extent identical characteristics, which may create some shared characteristics concerning behaviour or tendencies. The outside observer may see this as coordinated behaviour, or as an orchestration without the conductor. 21 Habitus is, in and of itself, not an empirical phenomenon but a theoretical construct. The construct must not be obstructed by pre-constructions or hypotheses where we are guided by assumptions we try to verify or reject. 23
Homologies
‘Homology’ (as Bourdieu has chosen to use it) is the relationship between structures of positions and structures of perception within alternatives for action. Positions, dispositions and positioning dynamically interact. The dispositions cannot be seen, we have to construct them from empirical data. Habitus leaves its mark on a diverse set of expressions that are set in motion in different fields: (habitus) + (capital) + field = practice. 24
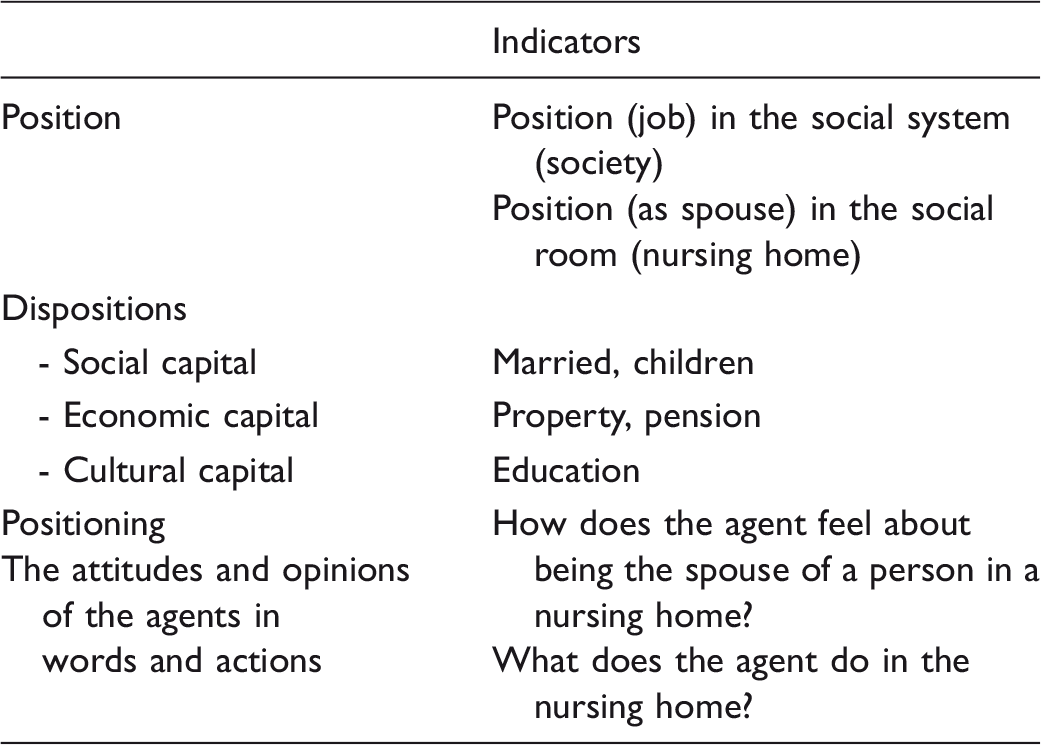
Methodological tools to describe habitus
Bourdieu’s habitus construction within the medical sub-field.
Ethical considerations
The project has been approved by Norewegian Centre for Research Data (NSD). There was no need for approval by the ethical committee since no patient information or interviews with patients appear in the project. The interviews were taped and transcribed in their entirety.
Having a spouse in a nursing home is a vulnerable situation, 19 and the researcher needs to have fundamental respect for the individual since the agents were cognitively adequate and consented to participate. The municipality also gave their consent. The agents were given sufficient and accurate information and were informed of their right to withdraw from the survey. The staff were not permitted to express their opinions of the agents’ statements that may unintentionally give the impression that some statements are subjective criticism. Nursing home staff in general provide excellent care and their effort is invaluable, but our purpose was to create awareness of how spouses may experience the situation.
Findings
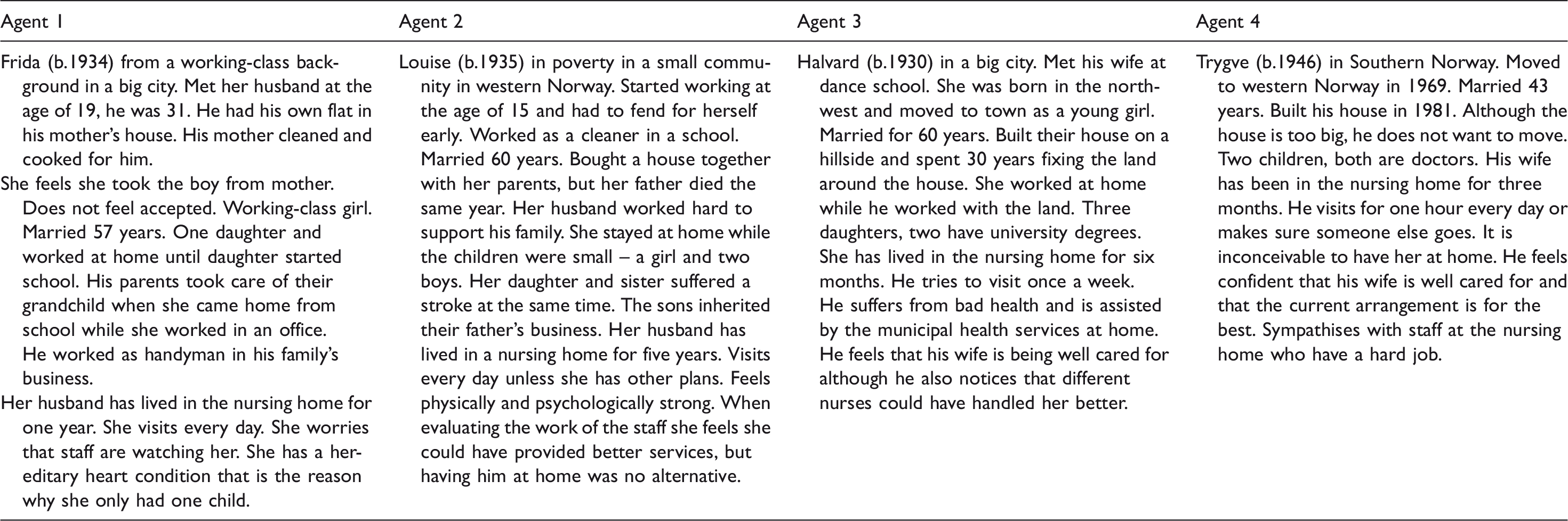
Presentation of agents’ disposition and position (names are fictional).
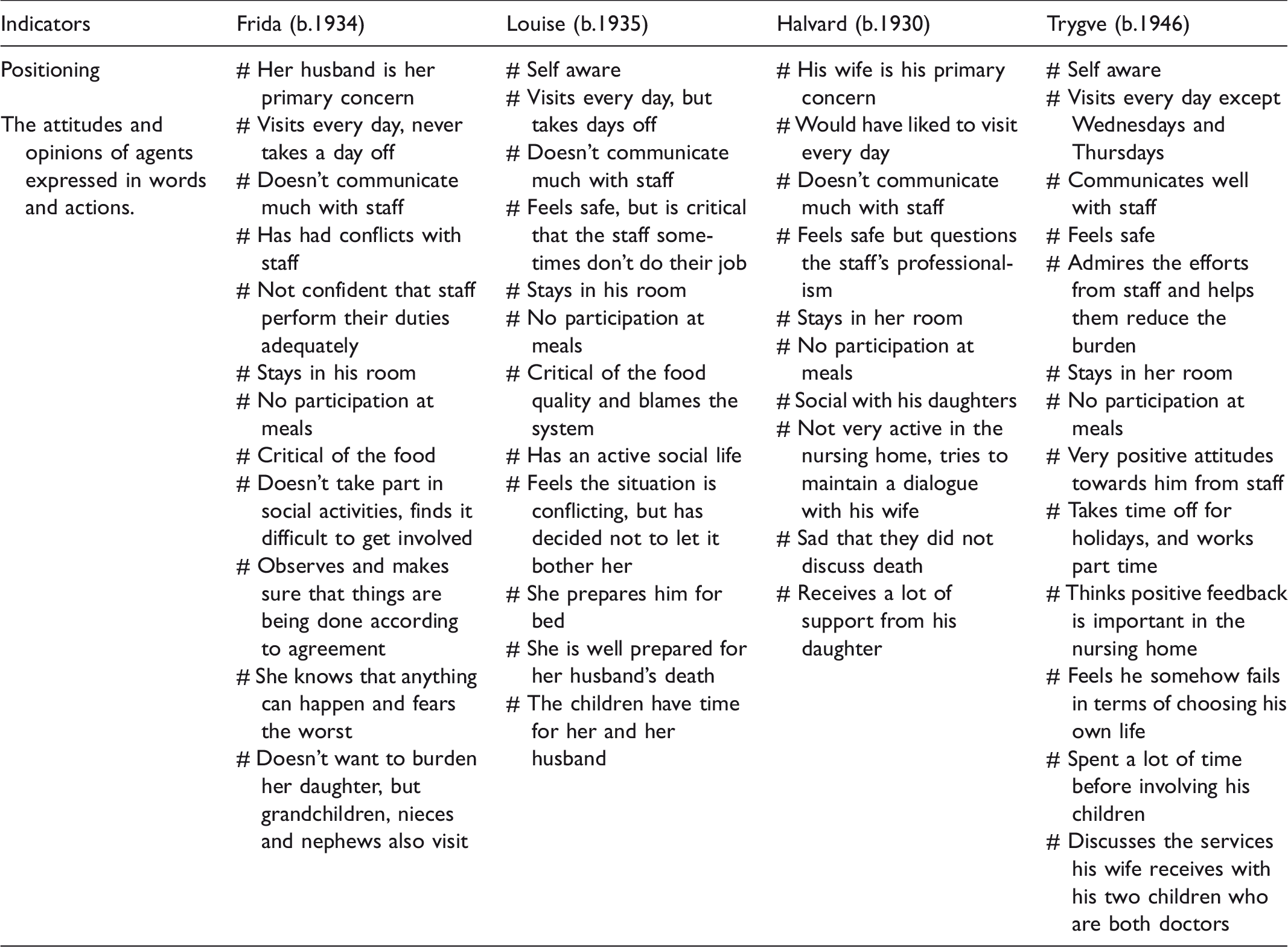
Summary of the agents’ positioning within the nursing home (names are fictional).
In order to describe the analytical process of the material we have chosen to highlight the themes sacrifice, sorrow and roles in the nursing home.
Sacrifice
Some agents have since adolescence maintained an altruistic attitude, which is reflected in their contact with the nursing home. They have sacrificed their own wellbeing in order to spend time with their hospitalised spouse. By adapting the new conditions to how things used to be, the situation becomes what Bourdieu calls ‘a virtue of necessity’. The practices are homological. Before and now share the same logic. Empirical studies describe how agents express the element of sacrifice in four different ways. According to our construct, this may reflect the times they grew up in, or the cultural values accredited to marriage. You can never see a one-to-one relationship between upbringing and actual actions, time and changes interfered and habitus is in an everlasting transformation.
Frida sacrificed a lot. She visited the nursing home every day and refused to come to dinner with her daughter instead of her husband, which upsets the daughter. She no longer spoke to her friends and felt that they had given up on her. ‘I feel I’ve lost touch with them due to the circumstances. The close contact is gone. And my days have become long and tedious’. Louise also made sacrifices, but took time off. ‘He doesn’t like it when I’m not there, but I can’t let it affect me. If I did my conscience would make it unbearable’. ‘I do as much as I can so I won’t have any regrets’. Halvard wanted to contribute but was too ill. ‘Of course, I have felt bad for not visiting more than I do, but I am not able to. I have severe back pains’. Trygve was open to sacrifice, but always on his own terms. He felt that the responsibility was handed over to professionals, but he arranged for others to take turns visiting on specific days. He also saw his visits as a contribution towards the staff. ‘I am not supposed to control at all. Let me rather say that I relieve the staff of some of their duties’.
When explaining the different positionings among the agents, several factors need to be taken into consideration: Frida, Louise and Halvard belong to a generation born between the wars. Times were hard and protestant ethics dominated people’s value systems. Frida and Louise married into a system with classical gender roles. Halvard was aware of his responsibility to his wife as defined by his role as husband. Trygve was born after the Second World War. He is a child of the economic upswing created by the Marshall plan. With the financial growth in Europe, new concepts, such as self-realisation and personal freedom, were introduced.
Sorrow
To be separated in old age, and no longer be able to live together, created sadness among the agents.
Frida lived with her husband at home for as long as she could and felt terrible when he was moved to a new permanency at the nursing home. ‘Every day when I left him it felt like betrayal’. ‘It has always been my duty to care for him, it is part of who I am’. Her husband felt he was living in prison and told her she might as well have him shot. Losing your spouse step by step is much harder than if he is suddenly gone, she says. ‘I feel very much and brutally alone’. Louise told us that all has gone relatively well, although there have been times when she has had her moments of doubt. Then she put on her coat and shoes and went for a walk. ‘I shut the door and leave it all behind since I know it isn’t healthy’. ‘I try to relax instead of worrying about what might happen’. Halvard said it was a sad situation to be in. It was hard when his wife was admitted to the nursing home, but luckily she seemed to be settling in. ‘Initially it was terrible and very painful [almost cries], but now that she has calmed down it is ok’. ‘I tried as long as I could, but my daughters pushed’. ‘Sometimes I look at her and think of all the things we’ve shared she and I. She was an amazing housewife and made all the children’s clothes herself’. Trygve: ‘I felt immensely sad in the beginning, but also relieved that she was in a nursing home. Now I can meet others, be active and take part in life around me’. The sadness was connected to losing his wife early to illness.
The experience of sadness was linked to several factors. Against the dispositions the agents had several factors that were homologically linked to their personal histories and historical contexts. Their justifications can also be described as follows:
Frida lived for a husband she met at a very young age. He has been very important in her life. She suffered much illness in her life and he has remained her main support. ‘My heart told me not to have another child’. When she married, she felt that she took the man away from his mother, something which strengthened her commitment and encouraged a need to stand by the love of her life. Louise left home at the tender age of 15 to find a job and became independent at a very young age. ‘I guess my mother would have been jailed for child labour if it were today [she laughs]’. The spouses share the same attitude to life. ‘He told me again and again that if he died I should look for a new husband. Sure, I told him, I know what I have but not what I’ll get’. She did not worry. ‘If I did I wouldn’t have been able to live with my conscience’. ‘I take each day as it comes’. ‘I don’t want any regrets or to feel that I wasn’t kind enough’. She felt sad that their retirement in Spain ended too soon with her husband’s stroke. Halvard had health issues and sometimes he was barely able to take care of himself, let alone others, but he missed sharing experiences and worries with his wife. ‘After speaking to my daughter I lost sleep’. They had separate roles in the marriage. ‘Yes we’ve had different responsibilities. The land we built our house on was tough and after work, I had dinner and a nap before I started working outside. She took care of everything domestic’. Trygve filled up his life with work, travels and visiting friends. He arranged for substitutes among supportive friends and relatives who visited his wife. ‘I visit – since she was admitted I’ve visited almost every day. Nevertheless, I have had some holidays. Recently I have agreed with her brother and sister in law that they visit every Wednesday. And our daughter has taken Thursdays off with the children so then she cares for her mother a few hours every Thursday’.
A visitor’s role in the nursing home and contact with the staff
This section deals with the interaction with staff and the role the spouse assumes when visiting the nursing home.
Frida – ‘I don’t seem to be able to establish a proper communication structure. I say something and they promise to make a note of it in the patient journal. However, I do not think they ever check the journal’. She was told that her husband was threatening and that he got up from the table and tried to slap a nurse. ‘Why did they have to tell me this? I couldn’t sleep the following night’. She also discovered that her phone messages were ignored. She has not spoken much with the staff nurse. ‘We didn’t seem to communicate well, and her reply is that they’re doing the best they can, that’s all’. Nor has she been much in contact with her husband’s primary caregiver who seems to have been replaced several times. Messages are not responded to, and she often needed to do things alone. Often also lying awake at night wondering whether the night nurses took care of him. ‘The accident with the foot happened at night’. ‘I often wish I had someone to talk to. There is not much I can say to my daughter. This is just long and painful, according to her’. ‘I feel better here than at home because here I am not afraid and the thoughts and worries don’t bother me as much’. Louise: ‘I go straight to his room so as not to be in the way. That’s how I feel – don’t come too close – so I stay in the background’. ‘In the beginning they let me share the evening meal with him, but suddenly that wasn’t allowed anymore. And I guess that’s because I notice things they say – things I’m not supposed to hear’. ‘I do not need to talk to the staff nurse’. Her husband had a primary contact, but they hardly spoke. When she talked to them, they often said they could not offer certain services because they were understaffed. She prepared him for bed, took off his clothes, brushed his teeth and washed his face and hands before she helped him with his night jacket. After having watched TV for a while, she called for help to get him to bed. He became upset if he had to wait too long. Halvard has not discussed much with the staff. There were one or two, but they seemed to change all the time. ‘My worst experiences are when they promise to do something but never follow through’. In addition, there seemed to be a conflict between what the nursing home is supposed to deliver and the rights of the individual patient. Who buys extra pillows for support? Who joins her to see the ophthalmologist? He was never told about his wife’s diagnosis but said; ‘my mother in law had Alzheimer and I learned about the disease’. He brought his daughter along for discussions with the doctor. ‘I spend a lot of time with her alone in her room since people around her easily upset her’. He also thought they were too slow helping his wife when she needs to go to the toilet. From the first moment, Trygve was met with support. ‘They have supported me all the way. They have seen me come and go at all times and seen me struggle. They have even told me to take time out’. When he mentioned that he would like to take a holiday, they said: ‘just go, don’t worry, we’ll take care of things here’. ‘I don’t need control, but she keeps hanging on [to me]’.
We also analysed the positioning in this case. Trygve has a very different relationship to the staff from all the others. ‘I have been a business owner and manager for many years. My mantra has been to be open and respectful in communication with my staff, and I guess I’m quite sociable. This creates a better environment for all’. He was also younger than the others and used to being more independent. They lived active lives and had independent jobs. The agents’ social positions were also reflected in the attitudes of the staff. He was a young man of 69 years. ‘When I come they tell me the coffee’s ready. They know when to expect me and they know I like a cup of coffee’. Trygve’s status and his ability to communicate with people made him welcomed when he visited, but also supported when he chose to stay away. Perhaps the staff admired a civil engineer not much older than they are.
Frida and Louise were women in their 80s. Their communication with staff is characterised by trying to avoid becoming a nuisance. ‘I don’t know but they seem to dislike me somehow, and I have felt that maybe I have asked too many questions lately or something, I don’t know’. Frida and Louise remained close to their husbands and strongly involved their care. While Louise also enjoyed other activities, Frida chose to focus on her tasks as a wife. There is a simple explanation for this since they have both had the role of care providers in their marriages. ‘It’s been like that since I was a child – that’s why I feel that I must see him, I must visit. It was the same with my mother – she moved in with us when my father died, you see’. The role of housewife and the woman’s position in marriage has often been clearly defined. Perhaps nursing home staff feel bothered by these women’s insistence and their high expectations to the quality of care. While being afraid to demand they are also worried that their demands may affect the quality of services their husbands receive. Louise was not too bothered by her conscience whereas Frida thought that everything would be better if she could only have cared for her husband at home. This solution was out of the question for Louise, and she and her husband had already discussed what to do. Halvard was ill and this affected how often he visited. He didn’t relate to staff much. It was impossible for him to have his wife at home in spite of the fact that he felt terrible that she lived in a nursing home.
Discussion
Love and marriage under surveillance
Being a spouse to a person in a nursing home makes you a guest at the institution where your spouse is a patient. You go from the privacy of the home to the public sphere. Historically very little prestige has been connected with chronically ill patients and the elderly, between nurses and physicians alike. Only a few nurses choose to work in nursing homes after graduation. Nursing homes are also often exposed to negative criticism. 10 Very often, the patient is moved to the nursing home against her will. Often the person in question does not even understand the need for it. When the environment and the room is cold or impersonal, this complicates the situation. Usually the patient has been cared for in the home initially, subsequently spending short terms in nursing homes before eventually having to stay there permanently. It is a long process of development, often with conflicting emotions. 8 The spouse’s needs and experiences are often overlooked. 6 It is essential to establish structures for how to receive the patient and his/her spouse in the nursing home. The focus on the patient may be explained by the staff’s focus on the person who will live there. A spouse may feel left out. For many elderly, who grew up between the wars, we may perhaps assume that the institution of marriage and the premise love was built on affects their involvement towards their spouses. Perhaps it is difficult for today’s generations to understand this? People between the ages 80–100 were born between 1918–1938. Consistency and predictability were essential to how this generation chose to live their lives. Children were taught to respect their elders, authorities and parents. 25 The values of the time affected all generations. Ideals, values and self-esteem are also a story about married life. In our material they also mentioned how this contrasts with current value systems. 25 Living for extended periods of time with a diseased spouse often involves a sad realisation that there is no other choice than to move the spouse to a nursing home. It becomes impossible to grow old together the way they had planned. Retirement suddenly becomes very different and the loss of a spouse to a nursing home is often a shattering experience. Talking to others in similar situations may often help. Talking to the children is often difficult since they may not want to share this burden. In addition, it is difficult when children insist that you need to pay more attention to your own needs. The agents preferred visiting their spouses rather than staying at home. It is upsetting to hear staff and friends point out that they needed to pay more attention to their personal needs and not to visit quite as frequently as they do. Spouses feel they do this by visiting their loved ones every day. Sitting at home all alone is worse, and they all feel lonely. The sadness of failure and of not having given sufficient care is strong as well as the sadness of the lost dream of old age together. Also of having to choose between visiting a spouse and visiting one’s children. A better dialogue and closer monitoring of their spouses would perhaps make it easier and safer for a husband or wife to let go and to visit friends and relatives instead. A support group or resource centre is often significant and may offer a common ground for these spouses. In order to alleviate the sadness, loneliness and sense of rejection among spouses it is important to take time to discuss life histories and to welcome the married couple to the nursing home. ‘It has been tough, but it has had its bright moments as well’. ‘It is important to share good memories but to take one day at the time’.
Conclusion
In this material the first author has interviewed spouses of women and men in nursing homes. This is a difficult position to be in. In order to endure and cope with the situation the spouses need to work hard and be strong. We see a tendency that the older the spouse, the more difficult they find the situation. According to our analysis we are talking about a lived life expressed in attitudes and actions (positioning) in marriage and at the nursing home constructed as a habitus based on the trilogy of Bourdieu: position, disposition and positioning within a field. The oldest seem more committed to their marriage vows: ‘For better or worse, in sickness and health’. They are dissatisfied with the situation they find themselves in and feel very sad. Nevertheless, the men seem more content with the nursing home, possibly, because they seem to accept and recognise their own limitations. What we can learn from this is to include the spouse and listen to the life-story of the family, and from there make person-centred care a focus for both husband and wife, patient and spouse.