
Abstract
This study aimed to explore how diabetes specialist nurses (DSNs) discursively construct and reconstruct their professional position in their working relationships with physicians and thereby the relation with patients in primary healthcare in Sweden. Twenty-nine DSNs working in diabetes care from 21 primary healthcare centres were included in focus-group interviews. The interviews were analysed using discourse analysis. From a social constructionist perspective, findings showed that the working relationship between the DSNs, physicians and thereby the relation with patients was discursively constructed as a relationship within a gendered discourse. The DSNs constructed their subject position metaphorically as ‘mothers’ in this relationship. The construction of doing gender implies that the DSNs became visible as biological women, but invisible in being perceived as competent, well-educated professionals, because skills such as multitasking and versatility are often associated with female abilities.
Introduction
According to international and national diabetes guidelines, a multi-professional team of medical specialists and dieticians should care for persons with diabetes diseases.1,2 In Swedish primary healthcare (PHC), the diabetes specialist nurse (DSN) has an important position in this process mainly for persons with type 2 diabetes. 3 However, several studies have confirmed that the working relationships between different healthcare professionals and between healthcare professionals and patients are not practised to the desired extent.4,5 Earlier studies exploring the professional role of DSNs in diabetes care have shown that the profession is multifaceted and filled with role ambiguities where there is a need for additional role clarity.6,7 In particular, the interaction with patients needs to be emphasised and person centred which might challenge DSNs to alter their professional positions.8,9 Despite the fact that most nurses in diabetes care are women, whereas there is a slight overrepresentation of men as patients and physicians,10,11 research about what consequences this may have for the working relationship have not been thoroughly investigated. Still, the working relationships among healthcare professionals without a gender perspective in diabetes teams have been investigated, 12 with the finding that understanding each other's professional scope of practise and position clarity is critical to facilitate the working relationship. Regrettably, studies related to how DSNs linguistically construct their own position and those of physicians and patients in working relationships are meagre.
In Sweden, The National Board of Health and Welfare 3 regulates work and proposes a working relationship between nurses and physicians in PHC. However, in PHC practise DSNs (mostly women) and physicians (often men) work alone in their own way, even though both perform similar tasks (e.g. physical examinations, documentation in medical journals and adjusting patients' medicine). 3 Nonetheless, the DSNs in general are responsible for coordinating team meetings and organising care, such as controlling metabolic measures and initiating illness education. 13 Over several years, attention has been paid to relationships within the nurse–physician–patient triad as a potential solution to problems existing in healthcare organisations.3,14 These relationships have been emphasised in various healthcare disciplines and with diverse foci, objects and aims. Disciplines such as intensive care,15,16 medical care and surgical care, 17 psychiatric care 18 and primary health and diabetes care5,12,19–21 are some examples. Studies have also indicated that a functioning relationship can be efficient in constructing satisfying work situations,22,23 decreasing personnel absenteeism and enhancing patient safety and the general quality of care.22,24,25
Working together demands a positive, clear and strong relationship between organisations and individuals 26 and can be described as a ‘working form’ or a ‘working norm’. 27 In our opinion, one can see a working form as a structure of an organisation and a working norm as a set of unwritten assumptions about how a person interacts with others in a specific position. A working norm can be related to norms on how DSNs linguistically construct their position and that of others in their working relationships with physicians and patients with diabetes in PHC.
Disclosing different aspects of working relationships
There are a variety of descriptions related to the working relationships between nurses and physicians and thereby the relationships with patients within the healthcare system, most of which are described in terms of cooperation, 28 collaboration, 29 teamwork, 29 or partnership. 30 Cooperation comes from the Latin verb cooperari and is described as ‘the process of working together to the same end’. 31 In healthcare, cooperation is often used to describe a healthcare process, such as the referral of patients between primary and secondary healthcare. 28 Collaboration, on the other hand, derives from the Latin collaboratio – working together. As such, it describes ‘the action of working with someone to produce or create something’. 31 Collaboration requires a commitment from all parties 32 and has been summarised in a review within the primary healthcare context. 29 It is suggested that collaboration can be seen as ‘inter-professional collaboration implemented in practise’ and the term teamwork is used to describe the collaboration between the DSNs and physicians, depicting ‘the deeper level of working together in an interdependent way’. 29 Teamwork is a synonym of collaboration and relates to ‘the work and activity of a number of persons who individually contribute toward the efficiency of the whole’.35(p. 31) Lastly, a working relationship can also be characterised in terms of a partnership, ‘the state of having shared interests or efforts’.35(p. 31) Partnership within healthcare has been portrayed as a key concept necessary for building a care process that is sanctioned from the patient's perspective. 30 In our study, working relationship is used when discussing the DSNs’ work together with physicians and thereby the relation with patients with diabetes in PHC.
Epidemiological framework: Discourse analysis, subject positions and gender
Discourse is an important concept in this study and can be defined as ‘a certain way to talk about and understand the world’.33(p. 7) A discourse analysis can clarify how a special position in a specific time and place/context (e.g. the position of DSNs in PHC) is shaped by the knowledge, values and beliefs that are linguistically expressed. 34 Thus, we all construct and reconstruct our identities linguistically in time and place/context and thereby position ourselves within our linguistic social relations.33–35 These positions are called subject positions (SP).33,34,36 The more a person acts according to the norms and values related to the SP, the more likely it is that this person is socially accepted.34,36
A SP is an analytical concept and as such can be used to analyse contexts in which gender is relevant. With a discursive approach, gender is not perceived as a set of biologic intrinsic properties, but as a system of ideas, beliefs, norms and values that are constructed and reconstructed through linguistic social practise. 37 This means that gender is used in this study as an analytical concept, not as a description of biological women or men. The discursive approach thus means that gender is contextualised, i.e. gender is seen in the context of time, place and the story appropriate for analysis. How gender as a working norm constructs the positions for the DSNs, physicians and patients’ working relationships in PHC has not been a central issue in diabetic-related PHC research. For instance, none of the above-mentioned studies has focused on how a gender perspective influences and constructs the working relationships between different professional caregivers and patients. The focus in our study is how gender linguistically and socially is (re)constructed in the working relationship between DSNs and physicians; on how men and women ‘do’ gender. According to West and Zimmerman 27 and Davies, 38 ‘doing gender’ puts forward subjectivity and active performance and posits that gender and gender relations are not fixed and determined but are formed linguistically in ongoing social activities. ‘Doing gender’ can be seen as a working norm in organisations that construct the social relations and working relationships between the DSNs and the physicians and influence how women and men perceive and position themselves and each other in organisations,39,40 and how both women and men contribute to the construction of gender in their working relationships. It also means that ‘doing gender’ as a working norm is a normative frame illustrating that moral understanding can be viewed as engendered and embedded in practises that have been (and still are) women's work such as the DSNs’ work in caring for patients with diabetes in PHC.
Purpose
In the previous presented study 6 the focus was on DSNs' perceptions of their professional role. However, since language not only examines reality but also helps to construct and reconstruct it and our identities and positions, this present study aims to explore and analyse how DSNs discursively construct and reconstruct their own position in their working relationships with physicians and patients with diabetes in PHC in Sweden. To investigate DSNs' own descriptions of their position through a discursive approach is an effective way to elucidate values and norms within a given context.
Method
Design, setting, participants and data collection
This study is an explorative, social-constructivist study. The data consist of focus-group interviews, 41 (three to eight participants in each group) with in total 29 DSNs employed at primary healthcare centres in northern Sweden. Semi-structured interviews were conducted that included topics about the DSN profession, perceived expectations, perceptions, experiences, facts and values related to DSNs' working relationships with physicians and patients with diabetes in PHC. The semi-structured interviews were audio-recorded and transcribed verbatim. Setting, participants and data collection are thoroughly presented in a previous study. 6
Data analysis
An inductive approach was used to identify and analyse SPs. 33 Exploring SPs involved examining the linguistic expressions the DSNs used when talking about their working relationships in clinical practise, a method also used by others.37,39
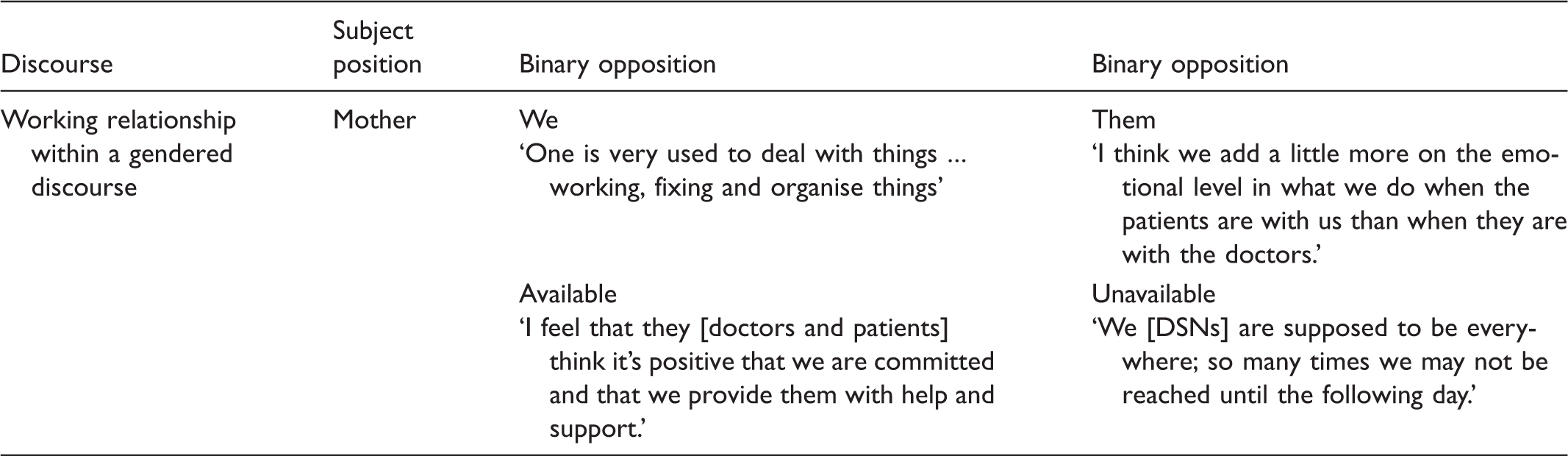
Examples of the binary oppositions that built the discourse (working relationship within a gendered discourse) and the subject position ‘mother’.
Ethical consideration
Data collection was approved by the Regional Ethical Review Board in Umeå (Dno 00-323M, Dno 06-126M). The informants received written and verbal information about the background and the purpose of the research in accordance with the Declaration of Helsinki. 43 They were informed that participation was voluntary and that they could withdraw at any time without consequences. The data were treated with confidentiality and the participants' quotations were de-identified.
Findings
This study showed that the working relationships between the triad of DSNs, physicians and patients are constructed as working relationships within a gendered discourse. Moreover, this study showed that the DSNs discursively constructed their SP metaphorically as mothers in their working relationships with physicians and patients. This position was based on norms, values and expectations that DSNs, like mothers, ought to foster, control, serve and nurture the patients like children and relate to a traditionally patriarchal ‘father’: the physicians. The binary oppositions we–them, subordinated–superior, available–unavailable, relational–solitary constructed the SP ‘mother’ (Table 1).
We–them
With the pronouns ‘we’ and ‘us’, the DSNs described, compared and associated themselves with ‘the other’ (‘them’), such as the patients, physicians and other healthcare personnel. This ‘we’ included a description of the DSNs as a group up-to-date with the latest research and guidelines in medical knowledge in diabetes and diabetes care. This description of ‘we’ also included an opinion that what matters in diabetes care is the DSNs. The statement, ‘If we [diabetes nurses] were not there, there would be no diabetes care’ shows that the DSNs highlighted their importance in PHC for patients with diabetes. According to the DSNs, ‘the others’ rarely had the understanding of the difficulties or the necessity of emotional engagement in diabetes care. Indeed, according to the DSNs, the others were incapable of fully comprehending all the work and effort the DSNs exercised in their daily clinical work. The DSNs meant that none of the others had either the time or the necessary devotion to become involved in diabetes care to the same extent as they did. This circumstance required the DSNs to act alone in a position where they served and took on responsibility for others concerning a variety of activities, expressing their inconvertible and moral action, which had similarities to a position of a mother's position within a family.
The term ‘we’ also included descriptions of the diversity and complexity of DSNs’ activities with the patients (them). These activities were described with verbs, such as support, motivate, educate and care, and exemplify the versatility of the DSNs’ usefulness in which the DSNs compared themselves with ‘potatoes’. ‘They [the DSNs] are like potatoes … nice to have with everything’. The expression ‘they’ also included the physicians, mentioned in almost every situation the DSNs described about diabetes care. The statement ‘They [the physicians] trust a great deal in what we say’ shows that the DSNs were proud to have earned the trust of the physicians. This way of talking about what the physicians thought about them as professionals demonstrated that the physicians were constantly present in the DSNs’ discourse even when they were not physically present.
Subordinated–superior
The relationship between the DSNs and physicians was asymmetrical in terms of power differences and hierarchy, i.e. the DSNs were subordinate to the physicians concerning medical questions. In trying to achieve treatment goals the DSNs sometimes served as a substitute for the physician (e.g. proposing to amend medicine doses for the patient). Here, the DSNs pointed out, ‘It's a huge job we do for the doctors, which they do not need to deal with’. According to the DSNs, to serve as a substitute for the physician was practical and helped solve several situations. Furthermore, it meant no conflict of interest between the DSN–physician relationships, according to the DSNs. However, the statement, ‘If I suggest something, they would buy it’ can be interpreted as implying that the DSNs had to relate to the physicians’ disposition of kindness and intention to understand. Occasionally, the DSNs were forced into making difficult medical decisions to solve an acute situation, where the consequences of these decisions left the DSNs reliant on the benevolence of the superior physician. The DSNs expressed that they had to make difficult decisions tangential to what their legitimate authority entails. The thought, ‘If only they [the physicians] support us then in the end’ was a common concern among the DSNs.
The sentences ‘the patients are not allowed to visit the physicians’ and ‘we [the DSNs] are impossible to reach … because we are occupied with other matters’ are illustrations of the patients’ subordinate position in the relationships with both the DSNs and physicians. This subordination can be interpreted as the expected and customary right of the DSNs to plan and determine the visiting agendas for the patients and the convention of physicians to plan their working-day schedule.
With such verbs as planning, controlling and establishing goals, the DSNs view themselves as indispensable in their commitment to plan, organise and control diabetes care. Commitment was also related to activities exemplified with terms such as support and educate, which describe the relationship between the DSNs and patients, and can also be interpreted as activities that positioned the DSNs in a superior position relative to the patients. The sentence, ‘I descended [from my superior position in the hierarchy] and talked like a friend without it developing into a relationship’ is an expression of an asymmetric hierarchical relationship.
The DSNs’ desire for control was a double-edged sword, where it was obvious that the DSNs’ authority over the patients could sometimes weaken under some circumstances. Thus, even if the DSNs tried to encourage, foster and persuade the patients to follow treatment goals, the patients typically had the final word. The comment, ‘They [the patients] might have well understood, but they do not want to do’ suggests that the DSNs act in a motherly way, perceiving the patients as defiant, obstinate and ‘childlike’.
When the patients failed to reach prescribed goals (e.g. glucose values determined by the DSNs), the DSNs took it as a personal failure. The statements, ‘You feel a little disappointed and unsuccessful’ and ‘we feel responsible and think it's our own fault’, suggest that the DSNs set the goals and not the patients. Such comments about subordination and superiority nicely illustrate the asymmetry between dominant/submissive, i.e. the working relationship between the patients and the DSNs. The remarks also reveal that the DSNs took personal responsibility for the patients’ doubts, which is similar to a mother comforting her children who have failed to meet established goals.
Available–unavailable
The DSNs tried to be available for both the patients and physicians, as suggested by the following comments: ‘to be there for them; they know they can reach me’ and ‘for their comfort and security’. Being there for them referred to answering questions from others while simultaneously doing hands-on work, which required a constant presence to maintain visibility. Thus, the DSNs sought to be available to the needs of the patients and encouraged the patients to contact them at any time. ‘One should be available and easy to reach’ was a commonly expressed idea, almost comparable to a sacred declaration of how the DSNs felt about their position in healthcare.
In their deep commitment to help others, the DSNs felt they were undervalued and taken for granted by the physicians as well as the patients. To be available the DSNs wished that the number of DSNs at each healthcare centre would be increased to meet the needs of the patients and the families they serve. The DSNs maintained having at least one annual appointment with each patient in accordance with hospital and medical staff policies and diabetes guidelines, but could arrange additional appointments if necessary. The DSNs pointed out that ‘they should actually be everywhere’. Such an assertion implies that the DSNs are the major link between the healthcare professionals and the patients and that it should be the DSNs’ responsibility to allocate their time to address the needs of the patients. The DSNs mentioned that having a heavy workload was burdensome being occupied with several tasks, which prevented them from delivering adequate diabetes care and treatment.
Relational–solitary
The DSNs described their SP as relational but simultaneously lonely. Utterances such as teamwork, companionship, communication, loneliness and being on your own are linguistic examples. Despite limited time, DSNs argued for the importance of creating relationships with all their patients and providing appropriate care based on the individual patient's needs and preferences. Independent of time issues, communication was crucial and with adjectives that included the terms engaging, happy and relaxed, the DSNs described the importance of having a positive and empowering approach. Because the DSNs had close and regular contact with the patients, it was possible to build trusting relationships based on genuine and transparent communication. In this respect, the DSNs endeavoured to adapt the appointments to the needs of the patients and tried to communicate according to the patient's agenda instead of an agenda determined by the DSNs themselves. During the actual short meeting, I try to focus on what the patient wants to know.
Communication took place either via individual telephone calls or at one-on-one meetings with the patients. Depending on the situation, the communication forms alternated between discussions, talk rounds, negotiations, recommendations, argumentation, information and narration. For example, the DSNs mentioned situations where they perceived that the patients felt secure and opened up and told their stories. The DSNs also described situations in which the DSNs and physicians communicated on equal grounds. In such situations, the DSNs and physicians felt more compelled to refer to one another with confidence and respect and take the other's knowledge into practice.
However, the DSNs also felt that they often worked in solitude for prolonged periods, hardly knowing what the other professionals were doing with the patients. Because the DSNs were responsible for special catchment areas and because much of their work was organised around waiting lists (fixed guidelines and quality indicators that were filled in during meetings with the patients), the DSNs usually worked alone. According to the DSNs, these lists made their work more rational and efficient (hence, less personal) and gave them a feeling of control over their situation.
The DSNs described the patients’ loneliness and perceptions of alienation, specifying the importance of meeting with the patients: ‘Our meetings are important … we are sort of his family’. This comment may serve as an example of a social community – ‘a family’ – in which communication between the members is of utmost importance. Utterances such as be together, social creature, shared experiences, individual visits and teamwork are further examples. In the DSNs’ working relationships with the patients, the DSNs’ communication skills were important in supporting, encouraging, motivating and listening to the patients’ perspectives, needs and concerns. Through the efforts of the DSNs, the DSNs and patients came together to function as ‘a family unit’ and provide a sort of ‘home’.
Discussion
This study showed that the working relationships between the DSNs, physicians and patients are constructed as working relationships within a gendered discourse. Moreover, the study also demonstrated that the DSNs discursively constructed their SP metaphorically as a ‘mother’ in the working relationships with the physicians and patients.
Doing gender and identities
The DSNs in this study constantly referred to themselves as ‘her’ and to the physicians as ‘him’, illustrating that the working relationship between DSNs and physicians was constructed and reconstructed linguistically and socially as a relationship between women and men. Such a relationship is therefore discursively constructed by norms and values related to the working norm ‘doing gender’, i.e. doing femininity and masculinity. When working together with the physicians and patients, the DSNs constructed their positions like ‘mothers’ while simultaneously carrying out a multiplicity of daily clinical tasks. Emotional, relational nurturing, unselfish service and the care that mothers/females normatively ought to carry out are well documented.40,44–46 These ‘female skills’ are commonly referred to as interpersonal skills 47 or versatility skills, which Segesten et al. defined as ‘performing multifaceted skills as well as carrying out tasks and to go on as usual’.48(p.225) The capacity to multitask is valued as invisible/implicit knowledge in the sense that there is no product to be seen. Such capacities are described as being part of a female embodied identity. 49 In our study, the versatile skills of the DSNs were understood as essential and taken for granted. There was also the demand to take on the main organisational duties and moral responsibility in working relationships with others. However, to embrace the notion that the capacity of performing many tasks at the same time is part of the female embedded and embodied identity raises a problem because it neglects versatility skills as a competence grounded in education, which in turn might exclude DSNs from being visible as competent, educated individuals.
According to many feminist scholars and ethicists, relationships with others are essential for women's female identity.44–46 Like ‘mothers’, the DSNs were often positioned between the physicians and patients, and as such the DSNs’ opportunities and capabilities were limited and constrained in performing nursing skills. It leaves limited opportunities to neglect and ignore so-called female duties related to versatility such as nurturing, service and availability. The DSNs in such cases might be perceived as ‘non-authentic women’. Hence, the versatility skills and effort of the DSNs made the working relationships with the physicians and patients possible, but these skills were probably invisible for the others in the working relationships.
The working relationships between different healthcare professionals within primary healthcare settings have been the focus of some research. 50 Research has shown that spatial-temporal factors have an impact on the working relationships of professional care providers. In our study, the DSNs’ moral responsibility and their versatility skills place them in the same space/place and time as the patients, which is, according to Cohen, 51 because professions should always be available for the patients and their medical superiors. However, sharing of space and time can also be discussed in relation to ‘doing gender’. In our study, the DSNs were expected to be available and visible in space and time so they could perform versatile and multiple tasks in their working relationships with physicians and patients. All the ‘things’ that the DSNs performed and their professional knowledge and skills, however, were seldom visible to others. ‘You never miss the water till the well runs dry’ is a common Swedish proverb, meaning that we tend to take some things and people for granted and just miss the persons/things when they are no longer with us.
Doing gender hierarchies
Hierarchies and asymmetry of power are not just about superiority and inferiority that are linked to different hierarchical professional levels but can also be related to doing gender hierarchies. That is, whatever is gendered ‘feminine’ has a tendency to be undervalued, whereas gendered ‘masculine’ confers higher status and position and is perceived as representing competence and professionalism.39,52,53 In our study this gender difference was obvious regarding the DSNs’ problems having control over their time, needs and activities. As mentioned above, the work of the DSNs was often related to versatility skills and service activities in response to the needs of the patients and physicians. Nursing care requires availability, is hard and takes time. If the DSNs kept up their nursing services and were always available, it naturally facilitated the working relationships with the patients and physicians. In cases in which the DSNs tried to negotiate it away, controversies and irritation arose between the parties. Thus, to avoid conflicts the DSNs would continue the service work, which meant that the problem became invisible for everyone, except for the DSNs because their frustration of not ‘being seen’ and listened to still remained.
While the DSNs described the physicians as being often physically absent and invisible in the working relationship, they were remarkably present and visible in the discourses. For instance, when the DSNs described their own work, they depicted it as the physicians/‘fathers’ representing the ‘gaze of medicine’, 54 the logic of the medical field that determines the decisions of the DSNs. This pertains to what Foucault called ‘governmentality’, 55 which refers to the notion that hegemonic medical knowledge determines gender positions in the working relationship between the DSNs and the physicians.
A working relationship with the patients, according to Fox and Reeves, 14 is a prerequisite to provide person-centred care. Focusing on person-centred care emphasising the working relationship between the parties in PHC can be seen as promising compared with those findings reported in Adolfsson et al., 4 where the majority of Swedish primary healthcare centres seldom included the patients in team meetings and in decision-making processes concerning their diabetes care and management.
In our study the patients were always referred to as ‘patients’, as sexless and genderless beings, or as ‘diabetics’ in their neutral gender position. They were also linguistically positioned as being ‘childlike’ (e.g. unquestioning) in the working relationship with the DSNs, which is consistent with Seymour-Smith et al.’s statement that positioning the patients as a child is in line with earlier research exploring the position physicians and nurses place on patients. 56
These issues are troublesome. First, to construct humans as genderless is to construct them as being neither masculine nor feminine, i.e. as persons without any life conditions, such as gender, which in various ways affect a person's life.57,58 Second, to construct persons, as ‘diabetics’ is to view them as objects. Working relationships occur between people, not between objects or persons without life conditions. Third, to position the patients as ‘childlike’ implies that they lack knowledge or sophistication, are passive and sometimes recalcitrant and disobedient. 59 Such positioning places the patients in a dependent and inferior/vulnerable position and presents them with limited possibilities to interact with DSNs and physicians on equal terms. A reason for this inferiority might be that the gaze of medicine has long been privileged over the voice of the patient, i.e. many patients have traditionally assumed a passive position towards physicians and their own care. 54 However, in the past years the possibilities for patients to influence their care have been addressed in Swedish legislative proposals, 60 which might affect patients with diabetes in PHC in Sweden. However, almost equally important is to challenge and clarify the discourses that construct and influence the working relationships between patients and healthcare personnel and between different healthcare professionals. Hence, the aim, then, is to help stereotypical, linguistic ways of social constructions become visible refractions that are understood and counteracted, as expressed earlier by Malterud, Candib and Code: ‘Yet, any gaze, even the medical one, is refracted through the lenses both of social-cultural stereotypes and of gender, and its seeing are shaped by these refractions’.61(p.8)
Methodological discussion
Describing the norms and values that construct the position of DSNs in their working relationships with others through discourse analysis has been fruitful. Discourse analysis can help to identify a thematic structure for how social relationships are constructed through language in an organisation and how reality is represented. 34 Nevertheless, by carrying out discourse analysis, you shape and elaborate the discourses to be analysed. According to Winther Jørgensen and Phillips, 33 it is difficult to know how to deepen a discourse: where does one discourse finish and the next begin? Where and when the limits are set, will have profound consequences on which social constructions belong to one or another discourse. This approach might have affected the results of the study.
‘Gender’ was in our study and in the analysis understood as an analytical rather than an ontological category. It is not the DSNs’ or the physicians’ biological sex that was the focus, instead it was the norms and values that were linguistically and socially linked to gender and ‘doing gender’ in the working relationships between DSNs and physicians. However, by using the discourse of gender analytically, it is up to the researchers to argue for the limits of their decision. Analysis in this study therefore does not show the only possible preparation of DSNs’ descriptions of their working relationships with others, but provides merely one version of this relationship. Pointing to language constructions that are self-explanatory can be discussed, criticised and changeable. 36
Conclusion
This article contributes to the body of knowledge that the working relationship between nurses and physicians is strongly linked to the construction of doing gender. For the DSNs, there were several issues and expectations connected to this working relationship. An issue was related to expectations of the female DSNs' (biological) sex and expectations related to educational ideals, which were male defined. Therefore, the DSNs became visible as biological women, but invisible in being perceived as competent, well-educated professionals because skills such as multitasking and versatility are often considered to be associated with female abilities.
Another issue connected to the working relationship concerns the construction of the patients as genderless/sexless, invisible beings. The DSNs assume the moral responsibility for the working relationship with physicians, simultaneously making the patients visible only through their illness and thereby objectifying them – making them visible as persons without life conditions (such as gender). The expressions working relationship, collaboration, cooperation and teamwork in diabetes care imply positive effects. However, the inconsistency of a working relationship means that 1) the DSNs construct and position themselves and are discursively constructed as (in)visible mothers, 2) the patients are encountered as childlike genderless objects, and 3) the physicians always are attended but still absent (similar to a traditional father's position). A respectful and positive working relationship should be built on equality and trust but also on grounds that all parties are visible. To explore a working relationship without considering a gendered discourse produces situations in which the working conditions of persons become invisible.
Footnotes
Funding
This manuscript was financial supported by Gothenburg University, Centre for Person Centred Care, GPCC.
Conflict of interest
The authors declare that there is no conflict of interest.