
Abstract
The aim of the study was to describe nurses’ experiences of how stigma affected the care and health of patients with leprosy. Health-related stigma exists worldwide and affects patients, relatives and caregivers. Mere word ‘leprosy’ is often met with disgust, shame and fear. Knowledge of health-related stigma is important for developing care in different parts of the world. The study has a qualitative, descriptive design. Seven semi-structured individual interviews were conducted with nurses working at a hospital specializing in leprosy care. The study was carried out in the central region of Ghana. Data were analysed using qualitative content analysis. The findings are presented as one theme, ‘Increased knowledge and holistic interventions are important in care for patients with leprosy’, and three sub-themes: ‘knowledge and beliefs are intimately interlaced with leprosy-related stigma’, ‘information is important but not enough to change behaviours and attitudes’ and ‘long-term interventions in a social context’. We conclude that caring for patients with leprosy involved long-term interventions, not at least in relation to education on a society level as well as concerning patients’ abilities to learn a skill to make an income in order to be less dependent on healthcare facilities.
Background
In a globalized world with increased migration different expectations and understandings of health and illness arise, including those surrounding health-related stigma. Health-related stigma exists worldwide and affects patients, relatives and caregivers. Leprosy is a disease that has long been associated with stigmatization and the mere word ‘leprosy’ is often met with disgust, shame and fear.1–3 The origin of the word ‘stigma’ was a tattoo mark, placed on criminals, slaves or traitors to facilitate others avoiding the person. According to Goffman, stigma is defined as someone being different and less desirable than people in general, a weak, bad or dangerous person.4,5 Rejection, avoidance, prejudice and discrimination are further described in relation to stigma. 6
Leprosy, also known as Hansen’s disease, is a slowly progressive chronic disease caused by the parasite Mycobacterium leprae (M. leprae). The disease is transmitted via droplets from the nose and mouth during close contact with infected people who have not been treated. 7 Those primarily at risk of being infected are people living in poor socioeconomic conditions and those with weak immune status. Factors such as gender, race and age have no effect on the occurrence of leprosy. If leprosy goes untreated it can lead to crippling, blindness and deformities.8,9
Earlier studies show that stigma derives from several factors, including knowledge, attitudes and behaviours, 2 and influences a person’s life and wellbeing.2,7,10,11 Health-related stigma is often characterized as social disqualification of people and groups with certain health issues. It can be considered as both a consequence and a cause of health issues 10 and is associated with low self-esteem, poor social adjustment and inferior quality of life. 12 Previous research shows that leprosy is often accompanied by mental distress. For example, a South African study showed that one third of those who had received a diagnosis of leprosy contemplated suicide. 2 Women with leprosy were found to be more severely rejected and isolated than men in the same situation, partly due to losing the emotional closeness to their children due to fear of transmission. 13 Furthermore, the care encounter is affected for patients with leprosy, who are shown as being stigmatized by healthcare workers and refused treatment. 14 Others avoid seeking care or seek care at a late stage when disabilities are already developing as consequences of health-related stigma.7,10,11 Efforts have been made in healthcare to tackle stigma and discrimination. However, the effectiveness of these efforts is not known, due to a lack of tools for evaluation, especially in developing countries.3,15 There are some systematic reviews in the field of health-related stigma and leprosy, e.g. in relation to efficacy of interventions 16 consequences of stigma 17 and in comparison to other neglected tropical diseases. 18 However, to the best of our knowledge there has only been limited research into nurses’ experiences of health-related stigma in relation to patients affected by leprosy. At the same time, healthcare workers, including nurses, generally hold a position of authority in society and thus have a significant role to play in preventing fear and stigma related to certain diseases.5,19 Therefore it was considered important to know more from the perspective of nurses caring for patients with leprosy. The aim of the study was to describe nurses’ experiences of how stigma affected the care and health of patients with leprosy.
Methods
A qualitative descriptive study design was used. Data were collected during 2014 from interviews with nurses working with leprosy patients in the central region of Ghana.
Participants and setting
Information about the study was presented to the staff of a hospital in the central region of Ghana by a hospital employee. The hospital is a small primary hospital owned by the government. It began as a leprosarium in the 1950s but now works as a leprosy and general hospital. The hospital consists of two leprosy wards, one female and one male, a surgical ward, a delivery unit, an emergency ward, a rehabilitation centre, two theatres as well as a pharmacy. The hospital staff consist of registered nurses (RNs), doctors (MDs), midwives, physiotherapists as well as administrative staff. The RNs rotate between each of the wards. The leprosy wards could hold 35 patients each and two RNs are in charge of each of those wards. Of the nurses who were willing to participate in the study, four were selected by the Deputy Head Nurse of the hospital based on the inclusion criteria: to be currently working as a nurse and to have experience of working with patients with leprosy.
Data collection
The initial interviews were performed by one of the authors using a semi-structured guide (Appendix I) and were all performed at the hospital in a secluded office. The interviews lasted between 25 and 50 minutes and were tape-recorded and transcribed by two of the authors (Love Bergman and Asabea Britton). After reading the first interview transcriptions it was found that data gained were not sufficient to answer the aim of the study. Additional questions were therefore developed (Appendix I) and follow-up interviews were conducted with three of the participants (the fourth participant was not available for a second interview). Two of the follow-up interviews were performed in the hospital and one in the home of the participant. These interviews were conducted with two of the authors present, one taking notes and handling the recording device, whilst the other acted as the interviewer (Love Bergman and Asabea Britton). Later on the interviews were transcribed by the same two authors.
Data analysis
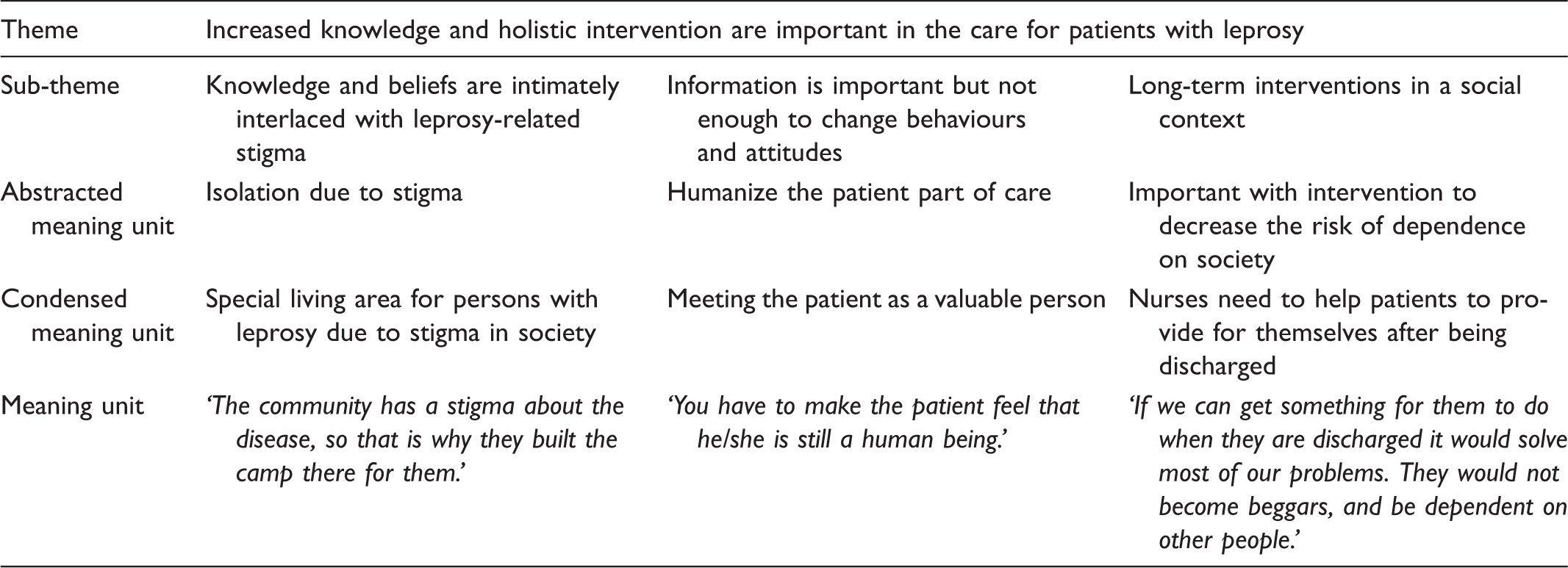
The analysis process, inspired by Graneheim and Lundman, 20 involved moving through the steps ‘meaning units’, ‘condensed meaning units’, ‘abstracted meaning units’, ‘sub-themes’ and a ‘theme’. Qualitative content analysis was considered appropriate, allowing different levels of abstraction based on the available text. 20
Example of the analysis procedure.
Ethical considerations
The Research Ethics Committee at the Department of Health Care Sciences at Ersta University College, Stockholm, Sweden approved the study (1404/A) and the study was performed in line with the council’s scientific code of ethics, 21 e.g. in relation to how to treat personal data. To protect the individuals and to guarantee anonymity, participants’ names were decoded. The data was saved on a USB memory stick and stored in a safety deposit box.
Participants in the study received both verbal and written information about the study stating that their participation was voluntary and that they could withdraw from the study at any time up until analysis of the data had been conducted. It was discovered that one of the participants had not read the information letter prior to the interview, and only received verbal information from the head nurse. The participant therefore received verbal information directly from the interviewer on the day of the first interview and after that gave her informed consent to participate. The participants were compensated for the time it took to perform the interviews with pay corresponding to their hourly salary.
Findings
The analysis resulted in one theme, ‘Increased knowledge and holistic intervention are important in the care of patients with leprosy’, and three sub-themes: ‘knowledge and beliefs are intimately interlaced with leprosy-related stigma’, ‘information is important but not enough to change behaviours and attitudes’ and ‘long-term interventions in a social context’. The findings reveal the impact stigma has on daily life and health for patients with leprosy, together with the complexity of needs nurses have to consider for this group of patients.
Increased knowledge and holistic intervention are important in the care of patients with leprosy
According to the nurses in the study, leprosy-related stigma had a major negative impact on the patient’s wellbeing, and care for those affected by the disease had to be different due to specific needs. The nurses stressed that knowledge and education were essential for reducing stigma. They described how a lack of knowledge among nursing colleagues and in society as a whole had negative consequences for patients and their relatives. To serve as educators and to provide holistic care with long-term goals were both described as essential for the nurses.
Knowledge and beliefs are intimately interlaced with leprosy-related stigma
Negative attitudes due to lack of knowledge were considered the main reason for stigmatization. Experience was expressed of a community where people believed leprosy to be highly contagious, creating fear and discrimination. Patients with leprosy were excluded from social interaction by being denied physical contact and closeness. For some of those people who are not educated they think it’s like a curse. They think that these people have done something for which they should be cursed. If common people in the marketplace see that your hands are deformed due to leprosy no one will greet you, or touch you, or come near you, or even give you a bowl to share a meal with you … So that is why they built the camp there for them. I thought that if I ate well and exercised and all those things I wouldn’t get the disease, even though I have read that it is not eating well that will help prevent you getting it … because it is a droplet infection. Now it’s better than it used to be. I used to go there, to the camp, when I was young, and there was a lot of discrimination, the stigma was very marked, but now it’s better, the patients are being accepted. There is a church and a cemetery right next door, because before when you came here as a patient you would probably also die here.
Information is important but not enough to change behaviours and attitudes
Stigmatization affects the health of and care for those suffering. The nurses experienced an unwillingness to seek care, both among men and women, which they directly attributed to the stigma of a leprosy diagnosis. However, according to the nurses, women tend to seek care more often and at an earlier stage compared with men, resulting in women barely having any deformities, while deformities were common among men. Patient education was considered important and to be one of their main duties as nurses. Because they know me as a health professional and know that I am talking from experience and will accept it. So we educate them on the condition, how to prevent it from getting worse, for instance what shoes to wear and the importance of not waiting to seek care. We touch them. We greet them. We are different, we are health personnel, we’ve been informed, but the information hasn’t really got through to ordinary people. There is nothing there for them to do unless they beg, so some of them when they leave us don’t take good care of themselves. Then they come back again. And when you want to discharge them, it’s a problem. Some of them, after we have discharged them, can be here for as long as two months before they go, and when they go it won’t be more than six months before they come back with even worse ulcers, and ulcers take time to heal, so they are here for a long period of time. They are in and out the whole time.
Long-term interventions in a social context
The nurses stressed the importance of not letting the general negative view of leprosy in society affect the care of their patients. Instead they looked to their Christian beliefs to guide the care. Even though more prestigious working positions were available the nurses talked about caring for patients with leprosy as a moral choice. One nurse said that she would not want to change her workplace because in the end she thought she would be rewarded for the work she was doing with the patients with leprosy in her current position. We Ghanaians, what we believe is that the clouds are the eyes of God. So God sees all that we do. And I have told them [the other nurses] that if you care for these people you will be rewarded. Some of them, because of the stigma, are not able to get work. Some keep making complaints so that we keep them here for as long as possible. Some of them keep coming back. They develop ulcers that they don’t keep clean so that they can be admitted again, so that someone will care for them. I think if we can get something for them to do when they are discharged it would solve most of our problems. We wouldn’t get the beggars, we wouldn’t get those who are dependent on other people […] if there is something that could be done that could generate income, I think it would help.
Discussion
In the present study, caring for patients with leprosy meant facing and dealing with a general lack of knowledge of the disease, which affected the care and overall health of patients, as well as the role of nurses. Caring for this patient group involved supporting them to continue to contribute to society, giving them a meaningful existence in their community and improving their financial situation. Watson 22 describes the holistic approach encompassing establishing faith and hope in the caring process together and strengthening and humanizing patients. Holistic care with long-term intervention was a way of minimizing the risk of the patient returning to hospital just to get food and shelter. This is further described by Stevelink et al., 23 who found that unemployment and difficulty when seeking work were two of the major issues for patients with leprosy.
Physical impairment caused by the disease could hamper being able to continue with one’s previous work. However, it was mainly due to stigma that patients were devalued by society. Similar findings related to mental illness in Ghana were described. Barke, Nyarko and Kleecha found that being treated at a psychiatric clinic in Ghana was associated with being abandoned by one’s family. 24 Avoidance of healthcare and delayed treatment were seen by nurses as obstacles to successful treatment and a consequence of stigma, which is all in line with other studies focusing on leprosy.25–27
Ghana is making considerable advances with regard to health outcomes and services even if health-related Millennium Development Goals (MDGs) set for 2015 have not yet been met. 28 Additionally, it is important to remember that health-related stigma is not only a problem in developing countries, it also exists in developed societies, in regards to for example Alzheimers’s disease, 29 alcohol disorders, 30 psychiatric illnesses, 31 and HIV/AIDS.32–35 The existence of leprosy camps, as a sign of the alienation of patients with leprosy in the present study can be compared with alienation due to other disease and care settings, e.g. mental institutions.27,36–38 At the same time Premkumar 39 found that leprosy sanatoria, with time, significantly contributed to new knowledge and treatments of the disease as research could be better coordinated. Lack of information and education for patients, relatives, and the community and healthcare providers was understood in this study to be the main reason for stigmatization. These results are consistent with Sobrinho et al. 37 and White’s 38 claim that education and information are important if stigmatization is to be reduced. This is further confirmed in a systematic review that described information, education and communication programmes, together with socioeconomic rehabilitation as important for reducing stigma. 16 Nurses in this study viewed education as one of their main duties, and through education nurses tried to improve the patients’ understanding of their health as well as their overall life situation. In line with Watson, 22 increasing teaching and learning in order to help patients gain a sense of self-control was seen as a core element of care. Knifton 40 found that religious or supernatural explanations decreased stigma. In this study religious motivation and hopes of religious reward were incentives for nurses to care for this patient group, but were not described as acting to decrease stigma.
Even if stigma in this study is specific to leprosy, the consequences show similarities to health-related stigma as a whole. Stevelink et al. 23 found that health-related stigma had the same negative consequences for the person affected, regardless of the type of disease. In this study, providing education for society as a whole and at the same time being sensitive to patients’ wishes and needs presented a dilemma for nurses. Others have shown that changing the name of the disease and counselling have been successful strategies to reduce stigma. 16 Complying with the wishes of the patient not to use the hospital’s full name involving the word ‘leprosy’, was a way of showing sensitivity to patients, but could on the other hand be counterproductive to efforts to educate the public and the patients’ relatives in a process of demystify the diagnosis. This illuminates the complexity of caring for patients with a diagnosis associated with stigma.
Methodological discussion
The number of participants is not what is essential in a quality research, rather the variation of experience. However, more participants could have provided a broader foundation for findings.41,42 In order to illuminate the participants’ experiences, follow-up interviews were conducted with the aim of providing more extensive data. According to Bengtsson, 43 cumulative data collections increase the possibility to deepen the understanding of the phenomena of interest.
Even if it is considered a disadvantage that the participants were selected by the Deputy Head Nurse and not by the authors of the study, this was found to be the only possible way to proceed due to the hospital organization and expectations of staff. However, the selection of nurses was based on the inclusion criteria and the nurses had various work assignments, which probably increased the likelihood of achieving a variation of experience of the studied phenomena. 44 At the same time it has to be taken into account that there is a risk that the Deputy Head Nurse also had other criteria for actually selecting nurses. However, it has not been seen in the result of the study.
It would have been beneficial to organize the interviews outside of working hours without interference with their regular salary, or as a part of their ordinary workday. However, as this was not manageable it was considered best to compensate the participants with the salary they lost when participating in the interviews during regular working hours. As the amount paid was more or less equal to their regular salary it was considered as not to any greater extent affecting nurses’ decisions to participate in the study. Strategies to increase transferability as well as the validity of the study have been to describe the selection process for participants with examples of the analytical steps.45,46 Furthermore, the analytical steps and findings were shared at seminars as a form of ‘peer debriefing’, 20 thus increasing the likelihood of being open to the phenomena of interest and for discussion of different analytical pathways.46,47
It was considered to enhance the validity of the analysis process that two of the three different authors transcribed the interviews as the authors became familiar with data both in oral form and later on as text and then in a later phase shared their understanding of the text with each other. The present study was conducted in a limited geographical area and concerned a stigma related to a specific and rare disease. However, several similarities were found between the findings of this study with research concerning health-related stigma for other diseases. One way of understanding more about a certain phenomenon is to step away from one’s ordinary or ‘taken-for-granted’ life, to go behind what one takes for granted in everyday life and to question everyday practice. 45 Findings from the present study may therefore also be considered valuable in other contexts for other patient groups. The possibility of transferability is further raised by Hofstraat and van Brakel finding in their systematic review that lessons from leprosy can be used in order to understand more about health-related stigma in relation to other diseases. 18
Conclusions
Stigma has a negative impact on the physical as well as the psychological and financial wellbeing of the patient, with consequences for their care and the role of nurses. Education for patients, relatives in the community and for colleagues was a central nursing intervention. Caring for patients with leprosy involved addressing a range of different needs as well as focusing on long-term interventions and goals. The need for holistic care and massive educational support was thought necessary to enable the patient with leprosy to stay out of hospital and to live a more independent life. Nurses in the present study raised the importance of nurses being role models for reducing stigma and showing a different way to treat this group of patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.