
Abstract
Providing care for dying patients is demanding for nurses. The aim of this study was to investigate Norwegian and Swedish nursing students’ concerns about dying and sense of coherence in their first and third year. Further, to describe the students’ experiences of caring for dying patients during their education. Nursing students in their first and third year in Norway (n = 64) and Sweden (n = 79) responded to the questionnaire Concerns about Dying and Sense of Coherence Scale. Interviews were conducted with 11 students. In their third year, both groups reported reduced concerns with regard to their own death. Norwegian students with no experience in healthcare before education reported more concerns about dying patients. Caring for a dying patient was experienced as a challenge to endure, perform and learn. There is a need to develop teaching methods and to give individualized support to nursing students during their education.
Introduction
Many people at the end of life need care from health professionals. One of the challenges in delivering end-of-life care is the shortage of adequately trained health professionals, of whom nurses are a key group, as they meet and spend a lot of time with patients and their families in various settings. 1 Nurses experience caring for dying patients as most stressful and they feel unprepared to meet dying patients due to lack of education and knowledge.2–5
Several studies show that nursing students, especially novice students but also students at the end of their education, expressed concerns about dying, and stated that it was demanding to provide care for dying patients and to cope with issues related to death.6–9 In order to assess health providers’ comfort with working with patients who are dying and their general concerns about death, Mazor et al. developed a questionnaire, Concerns About Dying (CAD). 10 The questionnaire comprises three domains: General concerns about death measures normal feelings and beliefs about death, Spirituality measures spiritual wellbeing, and Patient-related concerns about death relates directly to comfort in working with patients who are dying.
The questionnaire was used in a study comparing first-level nursing students from California, Norway and Sweden. The students from California, who had less experience of death, were more concerned about their own death and about caring for dying patients than students from Sweden and Norway. 11 Furthermore, the Californian students were found to be the most religious, while the Swedish students were the least. It is well known that Sweden is one of the most secularized countries, 12 which may be one explanation. A study focusing on Iranian nursing students showed that their attitudes towards caring for dying people were positively affected by a religious view of death. 13 Their attitudes were influenced by their previous experience with death. Near-death experience or the death of someone close decreased positive feelings about caring for dying people, even if those with more experience of death had less fear of death. Nevertheless, caring for a patient at the end of life and encountering the relatives seems to be a stressful experience for nursing students.
Sense of coherence (SOC) can be described as the ability to cope with stressful situations, and mirror a global life orientation. 14 This includes the components Comprehensibility, Manageability and Meaningfulness. People who view their life as meaningful and comprehensible and their life situation as manageable are more able to deal successfully with stressful situations. General resistance resources are, as claimed by Antonovsky, 15 crucial in the development of SOC. These resources include, for example, support from friends, colleagues and personnel at school. Insufficient support to nursing students when they encounter severely ill or dying patients is reported. 16 The students feel that they need more support during their education and that there is a great need to improve the quality of this education. 8
It has been reported that the attention to end-of-life care in the curricula was experienced, for several nursing students, as being insufficient and inadequate, as only a few hours were devoted to this area.17,18 The end-of-life care content is often delivered through traditional teaching methods, such as small group discussions and classroom lectures. 19 With these methods the students may not be given a realistic opportunity to experience their own reactions in the meeting with a dying patient.
As shown in the literature review, nursing students experience caring for dying patients and their families as challenging. However, there is a need for further studies with comparative longitudinal designs and mixed methods to investigate whether the students’ concerns and their ability to cope changes through their education. Therefore, the aim of the study was to investigate Norwegian and Swedish nursing students’ concerns about dying and sense of coherence in their first and third year. Further, to describe their experiences of caring for dying patients during their education.
The aim of the study was addressed through the following research questions:
Is there a difference between first-year and third-year nursing students’ concerns about dying and sense of coherence? Is there a difference between Norwegian and Swedish nursing students’ concerns about dying and sense of coherence? Is there a difference in nursing students’ experience in healthcare before education and sex in relation to their perceptions of concerns about dying and sense of coherence? Is there an association between experience in healthcare before education, age, concerns about dying and sense of coherence? How do nursing students describe their experiences of caring for dying patients at the end of their education?
Methods
Design
A longitudinal study was performed with quantitative and qualitative methods using questionnaires and interviews. Data had been collected from nursing students at two universities during their first and third year in Norway and Sweden.
Curricula
In Norway and Sweden, nursing education involves a three-year full-time program (180 ECTS Credits) leading to a Bachelor of Nursing Science.
In Norway, the curriculum is based on the Regulations to the National Curriculum for Nursing Education (FOR-2008-01-25-128) laid down in 2008 by the Ministry of Education and Research. 20 Clinical studies represent 50% of the programme and include practical training and clinical practice. The regulation and the curriculum at the university studied did not cover any specific learning objectives regarding palliative care or end-of-life care. However, the syllabus for the course Nursing in the Specialist Health Service (10 ECTS Credits) given to second-year students contained acute and chronic illnesses and disorders. Palliative care and end-of-life care were a part of the content.
In Sweden, the curriculum is based on the Higher Education Ordinance (SFS 1993:100, revised 2006:1053, Appendix 2) laid down in 2006 by the Swedish Government. 21 Clinical studies represent 50% of the programme and include practical training and clinical practice. The Ordinance and the curriculum at the university studied did not cover any specific learning objectives regarding palliative care or end-of-life care. In the syllabus for the course Clinical Nursing (7.5 ECTS Credits) given to third-year students, there was a focus on complex unhealthy conditions, in which palliative care and end-of-life care were part of the content.
Sample
The sample consisted of nursing students from two universities, one in Norway and one in Sweden. All first-year students, n = 315, were invited to participate and 247 agreed (response rate = 78%). Of these, 106/157 (response rate = 68%) were from Norway and 141/158 (response rate = 89%) from Sweden.
In the third year, there were only 197 students left out of 247, since some had not completed their education, had taken a study break or had an individual course study. From the group of 197, 143 participated (response rate = 73%); 64/78 (response rate = 82%) from Norway, and 79/119 (response rate = 66%) from Sweden. The present study only included students who responded both in the first and third year of their education.
From the sample of 197, students in their third year were asked to participate in a qualitative interview. In total, 11 students, seven from Norway and four from Sweden, who had cared for a dying patient, agreed.
Data collection
The first data collection was performed at the beginning of the students’ first year while the second data collection was performed at the end of the third year. The students were asked to complete the questionnaire including the Concerns About Dying (CAD) instrument and the Sense of Coherence (SOC) Scale, and four background questions.
The CAD instrument covers three subscales and contains ten items: General concerns about death (CD-General) (four items); Spirituality (three items) and Patient-related concerns about death (CD-Patient) (three items). 10 The response scale ranges from 1 (disagree completely) to 5 (agree completely). The CAD instrument was translated into Norwegian and Swedish in accordance with the steps described by Brislin. 22 The two versions were then tested for clarity on nurse lecturers, five in Norway and five in Sweden, leading to minor linguistic revisions. In the study by Mazor et al., the instrument showed an acceptable validity and reliability. 10 Cronbach’s alphas in this study were 0.75 (year 1) and 0.77 (year 3) for CD-General, 0.44 (year 1) and 0.47 (year 3) for Spirituality, and 0.79 (year 1) and 0.81 (year 3) for CD-Patient.
The 13-item version of the SOC Scale, developed by Antonovsky 23 includes the three components: Comprehensibility, Manageability and Meaningfulness. All items have a seven-point response scale with the anchors defined. By adding the scores of all individual items, a sum score was calculated. The scores could range from 13 (lowest sense of coherence) to 91 (highest sense of coherence). The SOC Scale has been used in several studies and has been found to be valid and reliable. 24 In this study, Cronbach’s alpha was 0.80 (year 1) and 0.86 (year 3).
The four background questions contained students’ age, sex and experiences in healthcare before education (two questions). The questionnaire was completed during a class session and returned in a coded envelope.
Qualitative data were collected with individual open-ended interviews. The following two questions were used: ‘How have you experienced caring for dying patients?’ and ‘How did your education prepare you for caring for them?’ To gain a deeper understanding of the students’ experiences, probing questions such as ‘Can you give some example?’ and ‘Please tell more’, were used. The interviews were performed by two of the authors (KP and MH-L) and one senior lecturer and lasted between 35 and 70 minutes.
Ethical issues
The studies from the two universities were approved in each country. In Norway, the Norwegian Social Science Data Services (ref.nr.21016) approved the study. Approval for the study in Sweden was received from The Research Ethics Committee at Karlstad University (ref.nr C2008/604, C2011/207). The study followed the ethical principles of the Declaration of Helsinki. All the students were informed both verbally and in writing about the study aim, confidentiality, voluntary participation and that they could withdraw from the study at any time without giving a reason. Prior to the study, the student health centre was contacted by the researchers. In case students participating in the study needed to talk to someone, a health professional and a priest were available.
Data analysis
The Statistical Package for the Social Sciences (SPSS) version 22 was used for the statistical analyses. Independent sample t-tests were performed to analyse differences between the two groups of students from Norway and Sweden in their third year with regard to age, experience in healthcare before education, their responses on the subscales CD-General, Spirituality, CD-Patient, and SOC. Fisher’s exact test was run for the variables sex and experience in healthcare before education. Furthermore, a paired t-test was run to test for differences between the students’ responses in their first and third year concerning the three CAD subscales, and SOC. For each country, subgroup analysis with independent sample t-test was used to test for differences between the students’ responses to the three CAD subscales and SOC, and sex and experience in healthcare before education. Correlations for the three CAD subscales, SOC, and experience in healthcare before education were analysed using the Pearson correlation coefficient. Statistical significance was set at p < 0.05. Internal consistency was analysed using Cronbach’s alpha.
The interviews were analysed using inductive content analysis as described in three phases by Elo and Kyngäs. 25 In ‘the preparation phase’ the tape-recorded interviews were transcribed verbatim and the text was read and re-read to make sense of the data and the whole. In ‘the organizing phase’, headings were written down in the margins of the text to describe all aspects of the content. After this open coding, all the headings were classified into mutually exclusive and hierarchically sorted subcategories and generic categories. The categories were labelled using content-characteristic words. During the different steps of analysis, the process went back and forth between the transcribed text and the categorization to secure credibility. Finally, a main category was formulated covering the content of the whole. In ‘the reporting phase’ a description of the categories was made and quotations from the interviews were included to illustrate the content of the categories. 25
Results
Sample characteristics
The mean age for the total student group in the third year was 26.6 years. The students from Sweden were slightly older (m = 27.2 years; SD = 6.05) than the students from Norway (m = 25.8 years; SD = 6.93). Most of the students were women 126/143 (88.1%). In the Norwegian group, there were only six men (9.4%) while the Swedish group contained 11 men (13.9%). The majority of the students, 109/143 (76%), had worked in the healthcare system before their education, in Norway 53 (82.8%) and in Sweden 56 (70.9%). The Swedish students had slightly more experience (m = 42.4 months, SD = 51.80) than the Norwegian students (m = 40.7 months, SD = 43.42). No significant differences were found between the students from Norway and Sweden.
Concerns about dying and sense of coherence
Concerns about dying and sense of coherence reported by Norwegian and Swedish students.
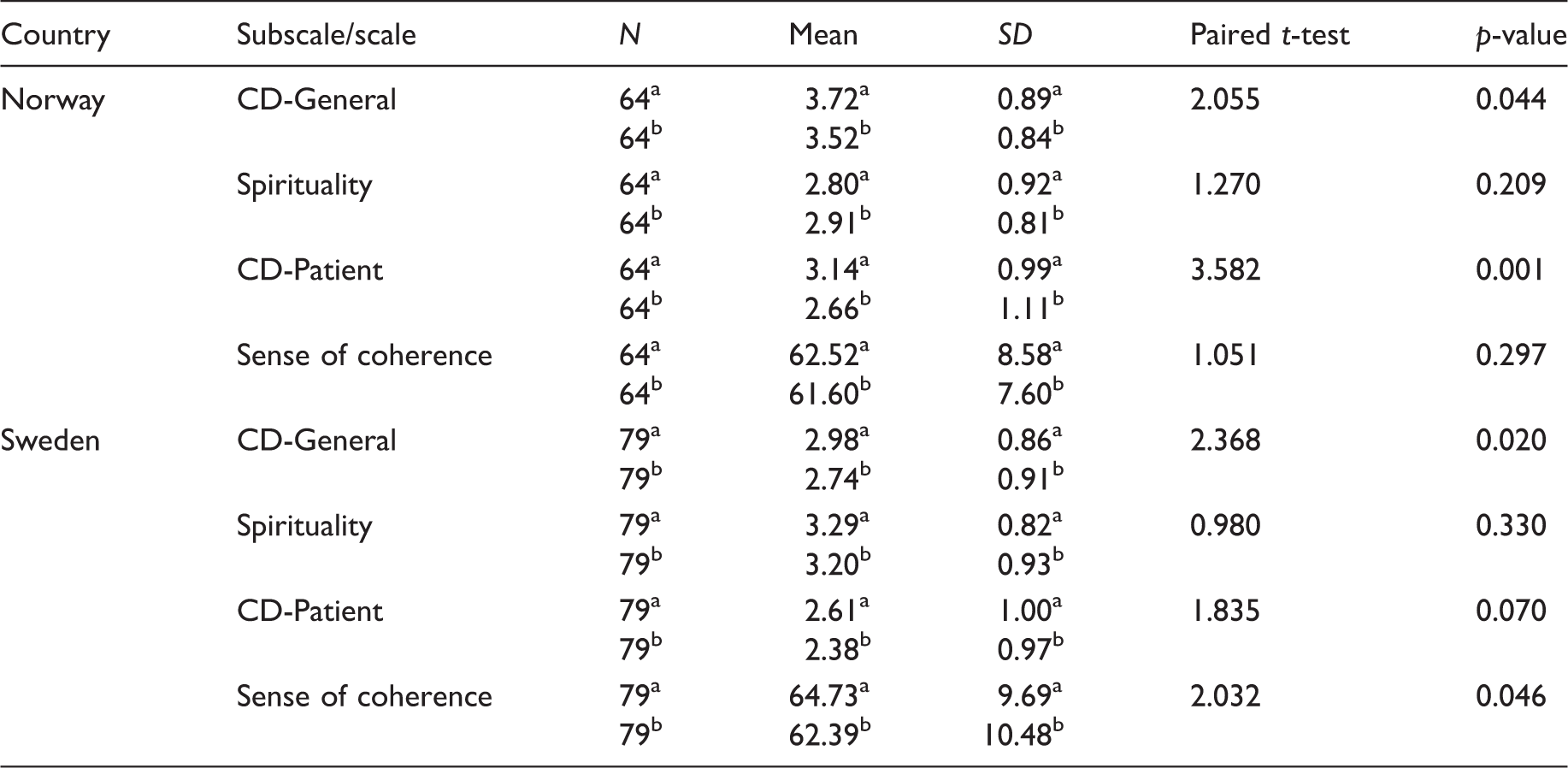
CD-General = General concerns about death.
CD-Patient = Patient-related concerns about death.
Year 1
Year 3
Comparisons between the students from the two countries in the third year showed significant differences only on the subscale CD-General. The Swedish students had fewer concerns with regard to their own death than the students from Norway (t-test = 5.24, p < 0.001).
Comparisons between the students in terms of sex and experience in healthcare before education in relation to concerns about dying and sense of coherence.
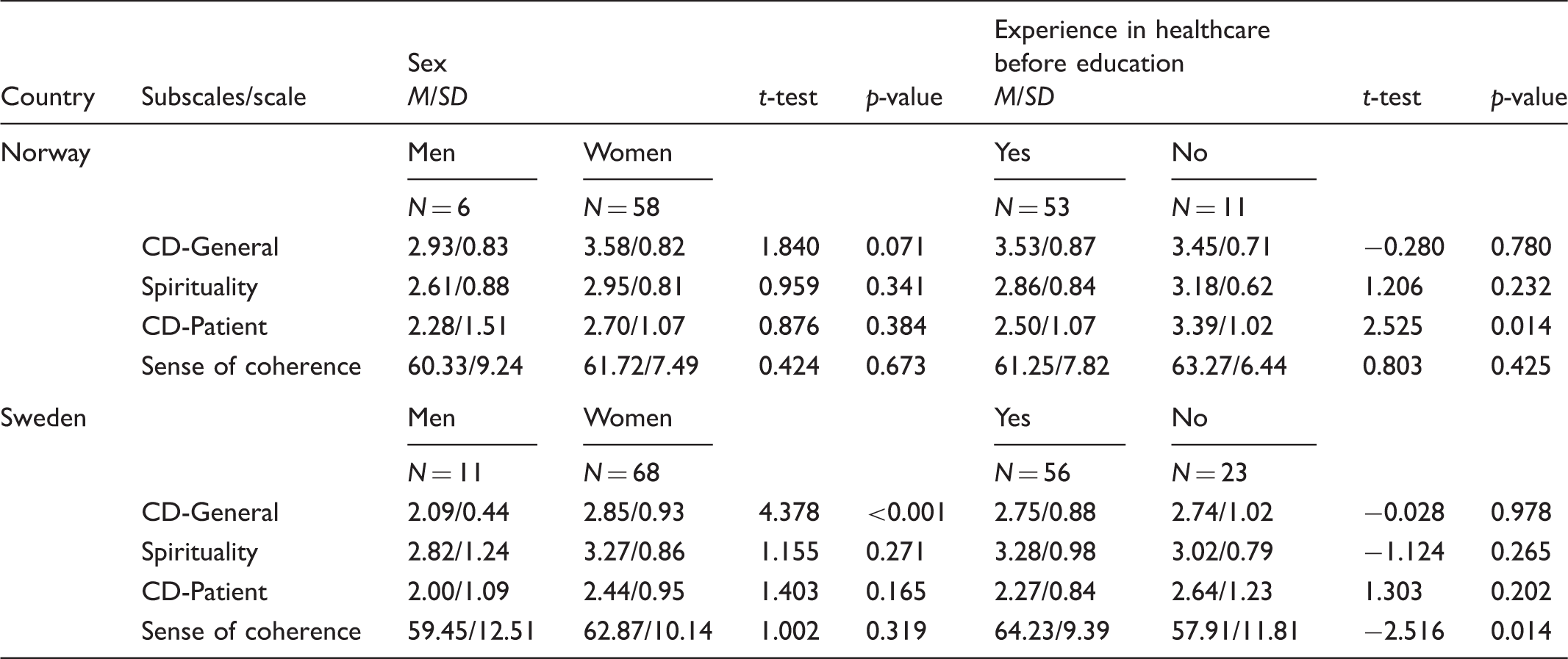
CD-General = General concerns about death.
CD-Patient = Patient-related concerns about death.
Correlations between Concerns About Dying (CAD) subscales, sense of coherence (SOC), age and experience in healthcare before education (year 1).
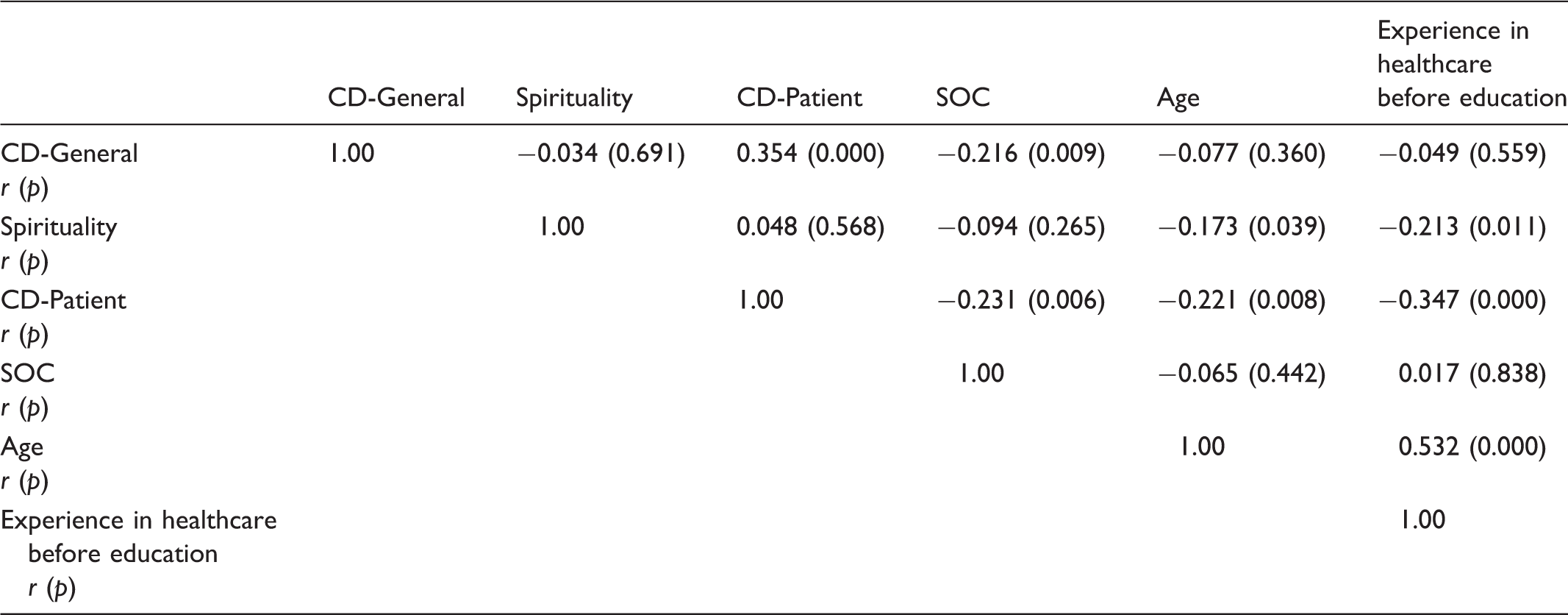
CD-General = General concerns about death.
CD-Patient = Patient-related concerns about death.
Correlations between Concerns About Dying (CAD) subscales, sense of coherence (SOC), age and experience in healthcare before education (year 3).
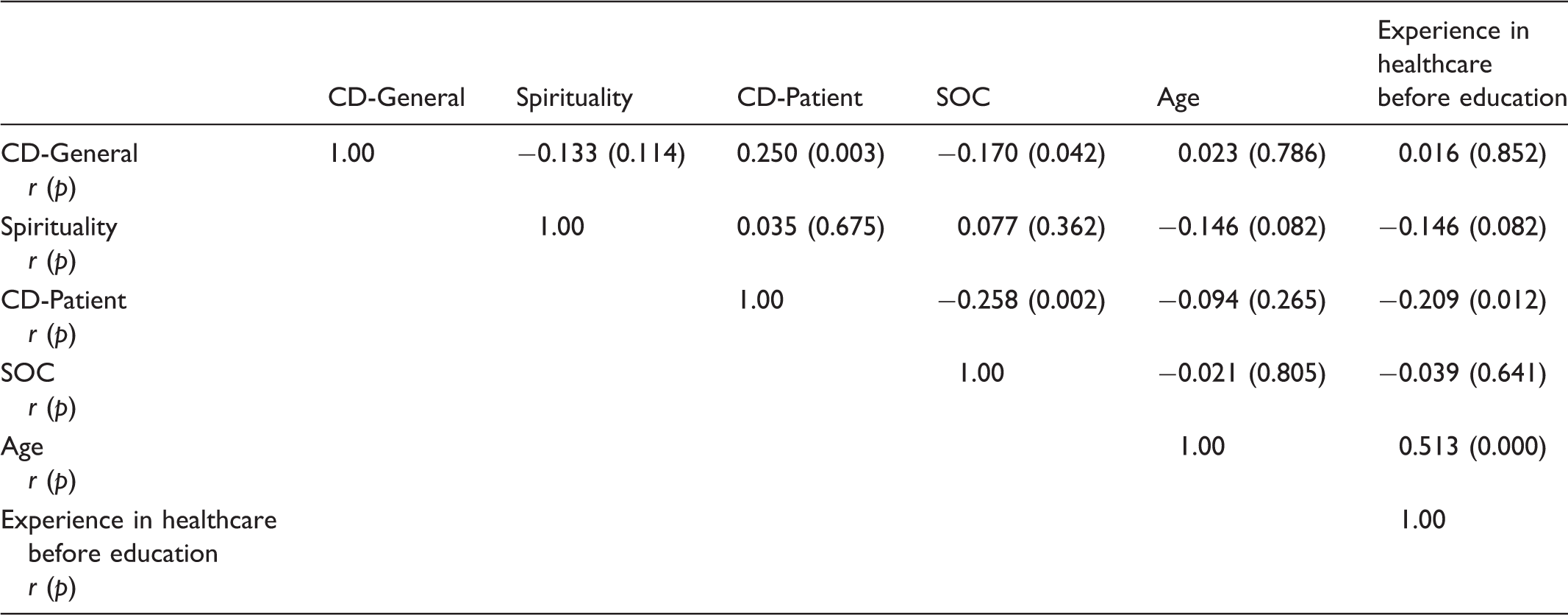
CD-General = General concerns about death.
CD-Patient = Patient-related concerns about death.
Nursing students’ experiences of caring for a dying patient
Caring for a dying patient: A challenge to endure, perform and learn
Nursing students’ experiences of caring for a dying patient.

Attending an unforgettable event
This generic category comprises the students’ encounters with a dying patient and the family members as an experience they will never forget. The situation was experienced differently depending on the patient. If the patient was old and had had a long life, students who had been prepared and informed about the patient’s condition described death as natural and peaceful and they were touched by the situation. To sit alone to support … just being there and follow … gives a very strong impression and a special atmosphere, to be with somebody you know is going to die. The parents insisted … they wanted him to survive … and everything was done to rescue him … but to see a young boy die, it was not natural and a very odd and strong experience, because I am young and I want to live. It was very peaceful, they chose the clothes she should wear … and they became involved in the care … we lit candles … it was a fine ending to a long life.
Delivering a respectful and intuitive care
This generic category comprises experiences of giving basic care to a dying patient, either together with a nurse or independently. The importance of being compliant in meeting the patient’s needs and wishes even if the patient reacted with anger and despair or was unconscious was described. Trying to find out the best way to comfort and calm down an anxious, confused and worried patient was difficult but also satisfying if one dared just to be there and to be able to come in contact with the person. A student had been singing hymns that the patient liked, another hugged a worried and scared patient, which calmed him down. They also described their satisfaction when care was based on respect and attentiveness to family traditions.
The students stressed the importance of protecting the patient’s dignity. When an acute rescue situation emerged with a patient at the ward some students had sheltered the patient from being exposed or chosen to take care of other patients or relatives during the acute situation and to shelter them from the unpleasant experiences. It is not only a patient but actually a human being, it is not my grandma but someone else’s grandma.
Some students had been facing ethical dilemmas when they had witnessed other staff members’ uncaring behaviour towards a dying or dead patient and had not dared to intervene. They saw these as demanding incidents, even if these were also situations to learn from. The first time I took care of a dead person … for me it was a particular occasion … but my colleagues they were so used to people dying that they started to talk about QUITE different things, … but here we were, caring for a person who had just died. I thought it was unworthy … I have thought of this very often and I will never do the same … it could have been my mother or father.
Studying reality
This generic category comprises what the students had experienced and needed in order to facilitate learning during their nursing education. They thought that theoretical preparedness was too scarce to enable them to care for a dying patient and his or her family members. Seminars, small group discussions and theme days in school with nurses from the clinic talking about their experiences of caring for dying patients were worthwhile. It was educative even if it was emotionally touching for some who had recently lost someone close to them. However, some of the students had not attended any lectures or seminars in school during their nursing education. … you cannot learn about this by reading and discussing … you have to do the best you can in that actual situation and act upon the principle of goodness … but it may not be the best for the patient anyhow. It is in the clinic you learn … of course you need to have theory to start from … but it is immensely important to train in practice before you can manage.
Discussion
The aim of the study was to investigate Norwegian and Swedish nursing students’ concerns about dying and their sense of coherence in their first and third year. Further, to describe experiences of caring for dying patients during their education. The two student groups showed quite similar results when comparing the CAD subscales in their first and third year and the students described caring for a dying patient as a challenge to endure, perform and learn.
Both groups reported significantly fewer concerns in the subscale CD-General in their third year. This means that the students were less worried about their own death or the death of someone close. 10 Thus, the Norwegian students showed significantly more concerns than the Swedish students. This result corresponds with the study by Smith-Stoner et al. 11 in which several of the same students in their first year were included. The students in Norway showed a score similar to medical and nursing students in the US, while the lower score of the Swedish group was consistent with hospice nurses’ score. 10 Students’ concerns about their own death or the death of someone close are probably influenced by factors such as personality and earlier experience of death, which the associations between CD-General and SOC indicate.
In the study by Mazor et al. there was a strong correlation between CD-General and CD-Patient, and the authors suggest that the two scales could be combined in studies of staff in healthcare. 10 In our study the correlation was moderate and several of the students had no experience of healthcare when they began their nursing education. Therefore, we decided to report the results separately for the two subscales.
With respect to the subscale CD-Patient, the two groups of nursing students showed more concerns than nursing students in the US. 10 The students’ experiences of caring for a dying patient showed a divided picture. On the one hand it was described as being important and a fine memorable moment, on the other hand as challenging and ambiguous, and as being associated with fearful and frustrating thoughts. However, the Norwegian group reported significantly fewer concerns in CD-Patient in their third year than in their first year. Being able to give the best possible care for each individual patient was important and satisfying, but difficult. The Swedish students also reported fewer concerns, although no significant differences were found between year 1 and year 3. The three-year nursing programme may have contributed to these results and clinical practice probably increased the chances of meeting dying patients. It is confirmed in the interviews that the students felt that clinical placements were the best arena in which to gain a comprehensive understanding of how to care for a dying patient. The negative associations between CD-Patient and experience in healthcare before education also support the importance of clinical practice. Other studies have found that students with experience of death were less fearful,7,26 while Chen et al. reported that students developed more fear later in the nursing programme. 27 Student nurses with extensive experience of death in connection with a natural disaster had less fear but they were also less likely to care for dying persons. 13 Ek et al. found that some students feared to encounter death for the first time, as they did not know what they would face. 8 Our interviews show similar results. Factors such as personality, organizational issues and lack of education and knowledge were found to influence patient-related concern. 5
With regard to Spirituality, the students from Scandinavia were less likely to endorse spiritual views than nursing students in the US.10,11 There were no significant correlations between the subscale Spirituality and the other two CAD subscales, which there were in the study by Mazor et al. 10 Cultural differences, with the Scandinavian countries being more secular than the US, may explain the scores in the Spirituality scale 11 as well as the non-significant correlations. Nursing students with religious view or faith were more positive about caring for dying patients 13 and made them secure in encountering patients at the end of life. 9
The results revealed that SOC decreased between the two measurement occasions in both student groups. SOC is assumed to be stable after the age of 30,28,29 and most of our students were between 20 and 30 years of age. Lindmark et al. found similar mean scores in 20 year olds in a population study, 30 and Eriksson and Lindström have also reported that younger adults had lower SOC mean score than adults older than 30 years of age. 24 The component Comprehensibility was found to explain why 20 year olds had a total low mean SOC score. 30 According to Antonovsky, young people do not have sufficient experience to view life as distinct, ordered and structured. 23 In both countries, female students had higher SOC scores than male students, although there were no significant differences. Similar results were found in the group of 30 year olds in the study by Lindmark et al. 30 Some studies did not find any gender differences, regardless of age,23,31 while other studies revealed that older men had higher SOC than women.24,30 The Swedish students who had experience in healthcare before education had a significantly higher SOC score than the students with no experience. They also showed fewer concerns in the subscale CD-Patient. In a study by Gélinas et al. various stressors, such as organizational, professional and emotional stressors, in connection with providing end-of-life care were identified. 3 A strong SOC contributes to the ability to manage stressors. 28
Nursing students emphasise the need for appropriate theoretical and clinical knowledge to be better prepared to confront situations related to death and dying. 32 The students in this study experienced that their theoretical preparedness when caring for a dying patient was too scarce. Some of them had not attended any lessons related to the subject during their nursing education. The decision not to attend might have been caused by anxiety, fear and the risk of being emotionally touched, also reported by others.8,33 In both universities included in this study, end-of-life care education was not made mandatory and no specific learning objectives were given in the curriculum, but some content was incorporated into the syllabus with an unspecified number of hours. Courses concerning end-of-life care seem to be optional in many countries but a more conscious focus on the topic has been reported.18,34,35 Education in palliative care resulted in less death anxiety and fewer concerns about dying among nurses 36 and affected their attitudes positively and helped to develop communication strategies between nurses and patients. 37 Ballesteros et al. found that a palliative course influenced nursing students’ personalities, which led to a better management of their fear of death. 18 Furthermore, training and education in palliative care for nursing students made them more likely to care for dying patients. 13 Nurse educators have a duty towards their nursing students to ensure that students are adequately prepared for the challenges they will face in clinical practice, 33 and the recommendations are thus to increase content regarding death and dying in nursing curricula.6,11
Various pedagogical methods may be used. The findings in this study indicate that seminars with experienced nurses and small group discussions concerning personal experiences were in demand. Continuous support and opportunities to reflect on and discuss issues related to death and care of the dying throughout nurse education are needed. 8 A review of end-of-life care in nursing education showed different teaching methods, i.e. courses based on literature, art and the humanities, interdisciplinary courses and high-fidelity simulations. 38 High-fidelity simulation is a valuable method for learning about end-of-life care, which also gives the teachers the opportunity to assess students’ abilities to handle the situation both practically and emotionally. 39 When studying nursing students’ perceptions of low- and high-fidelity simulation as a learning method, paper/pencil case studies (i.e. low-fidelity) were most satisfying. 40 This might be transferrable to learning about end-of-life care.
In the present study, the students experienced that real-life study during clinical placement was the most important arena in which to learn. The question is whether all students had the opportunity to encounter dying patients during their clinical placements. Some students had intentionally chosen clinical placements that would provide that experience. Student motivation to be involved in the care of dying patients makes nurses responsible for providing students with patients in need of palliative care. 9 The preceptors should provide the students with this experience and, it is necessary, should debrief them after caring for a dying patient and the patient’s family members. 39 The preceptors’ important role to modify tasks to the students’ competence and to confirm and support them in demanding situations was also described by students in the present study. However, studies of the effectiveness of clinical teaching at end-of-life care are still scarce. 39
Our study is in accordance with other studies and contributes to an increasing understanding of how nursing students in two of the Nordic countries experience concerns about dying during their education. The study was conducted at only two universities in each country, which should be taken into account when interpreting the results. Furthermore, the majority of the students were female, a fact that reflects the unequal gender distribution in nursing education. The Cronbach’s alpha values on the subscale Spirituality (0.44 and 0.47) were lower than in the study by Mazor et al. 10 This might be explained by differences between the countries in terms of religiousness. Further testing of the translated questionnaires into Norwegian and Swedish is recommended. Only 11 students signed up for the interview, maybe because the students were at their clinical placements and did not prioritize the interviews. Another reason may be that they felt it difficult to talk about the subject.
Conclusion
The results of the study show that at the end of their bachelor programme, Norwegian and Swedish nursing students reported reduced concerns related to their own death compared to when they started their education. Experiences in healthcare before education influence how students experience caring for dying patients. Caring for a dying patient is experienced as a challenge to endure, perform and learn. There is a need to develop teaching methods and to give individualized support to nursing students during their education. We recommend more emphasis on finding teaching methods for theoretical and clinical teaching of end-of-life care. The relation between concerns about dying, sense of coherence and nursing education needs further examination.
Footnotes
Acknowledgements
The authors would like to thank senior lecturer Kari Kirkbakk-Fjær for conducting interviews. We also thank the nursing students for their participation.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.