
Abstract
The aim of this study was to describe and compare perceptions of critical thinking, attitudes to and availability of research, research utilization and barriers to this among nursing students in Scandinavia and Indonesia. Data were collected at the beginning, middle and end of education from nursing students in Norway, Sweden (bachelor’s diploma) and Banda Aceh (bachelor’s diploma). Critical Thinking and Research Utilization Questionnaires were used along with the Barrier Scale. Descriptive analyses, comparisons between and within groups were performed. At the end of education, all samples exhibited positive attitudes to research and the main barrier was related to the setting. Scandinavian students reported higher critical thinking. Indonesian students perceived greater barriers on two Barrier subscales. No differences were found between the samples regarding research utilization. Significant changes over time varied among the samples except for the Norwegian sample. Indonesian students (diploma) exhibited most changes over time. Teachers must support nursing students to strengthen their critical thinking ability and develop professional competence.
Keywords
Background
This article focuses on Scandinavian (Norwegian and Swedish) and Indonesian (Banda Aceh) nursing students’ professional development in terms of critical thinking ability, attitudes to and availability of research, research utilization and barriers to this during their nursing education. Nursing education in Norway and Sweden differs from that in Indonesia in some respects. Since 2002 and 1993 respectively,1,2 Norwegian and Swedish nurses have been educated at bachelor’s level. In Indonesia, nursing education ranges from senior high school level, via diploma III to bachelor’s level. 3 Only a minority (1%) of nurses in Indonesia have a bachelor’s degree.4,5
Newly graduated nurses are required to employ research-based knowledge combined with clinical experience and patient values in their practice.6,7 The Institute of Medicine (IOM) has pointed out that the nursing profession is important for providing high quality, safe patient care. 8 Recent studies have shown that low professional competence among nurses leads to increased mortality in hospital patients.9,10 The Faculty of Quality and Safety Education for Nurses (QSEN) and The National Advisory Board have defined quality and safety competencies for nurses. 11 This definition is based on the core professional competencies described by the IOM 8 and includes, for example, patient-centred care, and evidence-based practice. Moreover, Kajander-Unkuri et al. have identified competence areas for nursing students within the EU. 12 One area is research utilization.
The use of research findings in practice is an important cornerstone of high-quality patient care. 13 In many countries, utilization of research findings and evidence-based practice (EBP) have become important subjects in nursing education. In recent years nursing curricula have been developed to a more academic level, despite this the theory–practice gap still exists.14,15 Forsman et al. reported that research use occurred in about half or less than half of the working shifts one and three years post graduation. 14 Moreover, Wangensteen et al. found that one fourth of newly graduated nurses were defined as research users, 16 and Andersson et al. showed that newly graduated nurses are not prepared for research utilization. 17 A systematic review 18 regarding barriers to research utilization showed that the most commonly reported items were related to the setting and the research subscales. The barriers included, for example, insufficient time to implement new ideas, and lack of time to read research reports. The barriers were consistent over time, geographic location and other conditions, e.g. study setting.
In order to meet the requirements for EBP, nursing students need to develop their critical thinking ability, as it can result in nurses having the necessary skills and dispositions, e.g. habits of mind, attitudes and traits, to support EBP. 13 Facione et al. described an ideal critical thinker as inquisitive, well informed, open minded, willing to reconsider and orderly in complex matters. 19 Thus, critical thinking is an essential component of professional accountability and quality nursing care. Wangensteen et al. found that nearly 80% of newly graduated nurses reported a strong disposition and positive inclination towards critical thinking. 20 However, mixed results are shown when measuring critical thinking development over time, i.e. before, in the middle and at the end of nursing education. 21
Studies have shown that a majority of nursing students and newly graduated nurses have a positive inclination towards critical thinking and positive attitudes to research utilization. However, low research use and several barriers to research utilization in practice have also been reported. Longitudinal studies of nursing students regarding professional development have been requested. It would therefore be of interest to study these matters among nursing students in different countries. The present study is a part of a larger collaboration project about life-circumstances, health status and professional development among nursing students in Norway, Sweden and Indonesia. This article highlights quantitative results regarding nursing students’ professional development.
The aim was to describe and compare perceptions of professional development, i.e. critical thinking ability, attitudes to and availability of research, research utilization and barriers to this among nursing students in Scandinavia (Norway, Sweden) and Indonesia (Banda Aceh) during their nursing education.
Method
A descriptive, comparative, cross-sectional and longitudinal cohort study.
Sample and procedure
The sample consisted of nursing students recruited from one university college in Norway (bachelor’s), one university in Sweden (bachelor’s), one university (bachelor’s) and two nursing schools (diploma) in Banda Aceh, Indonesia.
Data were collected in 2012 (T1), 2013 (T2) and 2014 (T3). A questionnaire package was administered to the students during the course of ordinary lessons. Teachers, (not involved in the present study), informed the students about the study and handed out the envelopes containing the coded questionnaires. The students returned the questionnaires in a sealed envelope. This process was carried out at the beginning (at the end of the first semester – T1), in the middle (during the fourth semester – T2) and at the end of their education (at the end of the sixth semester – T3).
In Norway 206 questionnaire packages were handed out at T1, 194 at T2 and 183 at T3. The analyses are based on the following figures: T1 n = 162 (79%), T2 n = 75 (39%) and T3 n = 88 (48%).
In Sweden 71 questionnaire packages were handed out at T1, 66 at T2 and 63 at T3. The analyses are based on the following figures: T1 n = 60 (85%), T2 n = 59 (89%) and T3 n = 54 (86%).
In Indonesia (bachelor’s level) 127 questionnaire packages were handed out at T1, 127 at T2 and 141 at T3. The analyses are based on the following figures: T1 n = 124 (98%), T2 n = 120 (94%) and T3 n = 112 (79%).
In Indonesia (diploma level) 153 questionnaire packages were handed out at T1, 139 at T2 and 114 at T3. The analyses are based on the following figures: T1 n = 152 (99%), T2 n = 121 (87%) and T3 n = 114 (100%).
Questionnaire package
The package included three questionnaires intended to measure professional development: Critical Thinking Questionnaire (CTQ), Research Utilization Questionnaire (RUQ), the Barrier Scale and questions about characteristics. The translation process followed the Eurostat procedure. 22
Critical thinking disposition was measured (T1, T2, T3) by means of the CTQ, specifically developed for the present study. The development of the questionnaire was inspired by the California Critical Thinking Disposition Inventory 19 and Watson and Glaser’s Critical Thinking Appraisal. 23 The CTQ consists of 28 items pertaining to critical thinking. The items employ a four-point scale: 1 = completely disagree, 2 = partly disagree, 3 = partly agree, 4 = completely agree. The total score, ranging from 28 to 112, was calculated by summarizing the item scores of each respondent. Higher scores indicate a greater inclination towards critical thinking.
Face and content validity were established by pilot testing of the questionnaire with a group of Norwegian nurse teachers and Swedish nursing students, after which some minor changes to the wording were made. Cronbach’s alpha, was .91 (T1), .66 (T2) and .78 (T3). The CTQ was developed in Swedish, translated into Norwegian and Bahasa.
Research utilization was measured (T1, T2, T3) by means of the RUQ. The RUQ was developed by Champion and Leach 24 and further revised by Pettengrill et al. 25 and Humphris et al. 26 Three RUQ indexes were used: ‘Attitudes towards research’ (12 items), ‘Availability and support to implement research results’ (8 items), and ‘Research use in daily practice’ (9 items) – 29 items in total. At T1 only the attitude index was utilized. All three indexes were utilized at T2 and T3. The items employ a five-point Likert scale: 1 = strongly disagree, 2 = partly disagree, 3 = don’t know/no opinion, 4 = partly agree, and 5 = strongly agree.
The indexes were calculated in two ways. A) The index scores were summarized and then divided by the number of items in the index. The index scores ranged from 1 to 5. B) By summarizing each respondent’s item scores on the index the scores ranged from 12 to 60, 8 to 40 and 9 to 45 respectively. Higher values indicate a more positive attitude towards research, better availability of research and more research use. Cronbach’s alpha, for the ‘Attitude index’ was .74 (T1), .75 (T2) and .79 (T3). The alpha values for the ‘Availability and support index’ were .68 (T2) and .65 (T3) and for the ‘Research use index’ .80 (T2) and .76 (T3).
The RUQ had been translated into Swedish 27 and Norwegian. 16 In the present study the RUQ was also translated into Bahasa.
Barriers to using research in practice was measured by means of the Barrier Scale (T2, T3). 28 The instrument consists of 28 items divided into four subscales: the Nurse subscale (8 items pertaining to nurses’ research values, skills and awareness); the Setting subscale (8 items pertaining to barriers and limitations); the Research subscale (6 items pertaining to the quality of the research) and the Presentation subscale (6 items pertaining to the presentation and accessibility of the research).
The items have a four-point scale where 1 = to no extent, 2 = to a small extent, 3 = to a moderate extent and 4 = to a great extent and a ‘no opinion’ alternative was offered. The subscales were calculated in the following ways: A) The subscale scores were summarized and then divided by the number of items in the subscale. The scores ranged from 1 to 5. B) Each respondent’s item scores on the subscale were summarized and the scores ranged from 8 to 32, 8 to 32, 6 to 24 and 6 to 24 respectively. Higher values indicate greater barriers. Cronbach’s alpha values were, for the subscale ‘Nurse’ .84 (T2) and .84 (T3), for ‘Setting’ .79 (T2) and .57 (T3), for ‘Research’ .79 (T2) and .84 (T3) and for ‘Presentation’ .81 (T2) and .76 (T3).
The Barrier Scale has been translated into Swedish 18 and into Norwegian. 29 The Barrier Scale was also translated into Bahasa for this study.
Statistical analyses
SPSS version 22.0 was used. Comparisons between the samples on gender and marital status were made using Pearson’s chi-square tests. Mean age comparisons were conducted using one-way analysis of variance (ANOVA), followed by Scheffé post hoc comparisons.
Between-group examinations at T1, T2 and T3 on the CTQ, the RUQ and the Barrier Scale were carried out as follows. Firstly, comparisons based on the raw scores were made using ANOVA, followed by Scheffé tests. Secondly, the same analyses were performed with analyses of covariance (ANCOVA) to control for gender (as a factor) and age (as a covariate). ANCOVAs yielding significant F values were followed by Bonferroni tests for post hoc comparisons.
Within-group comparisons on the CTQ, the RUQ and the Barrier Scale across the three assessment occasions (T1 vs T2 and T1 vs T3 or T2 vs T3) were performed by means of paired t-tests.
Reliabilities were estimated by Cronbach’s alpha coefficients. Statistical significance was set at p < .05.
Ethical considerations
The study was approved by the Norwegian Social Science Data Services (NSD) (No. 29212), the Regional Ethical Review Board in Uppsala, Sweden (Dnr 2010/462) and the Ethics Committee of the Nursing Faculty of Syiah Kuala University Indonesia (Dnr 160811301). The students gave their consent by completing the questionnaires.
Results
The results are presented as follows:
Characteristics of the respondents from Norway (N), Sweden (S), Indonesian bachelor’s (IB) and Indonesian diploma (ID), descriptive results pertaining to the professional development scales, the RUQ and the Barrier Scale at T3, between- and within-group comparisons for the CTQ, the RUQ and the Barrier Scale over time.
Characteristics
Characteristics of the Norwegian, Swedish and Indonesian nursing students at the beginning of their nursing education (Time 1). Mean values (M), Standard deviations (SD), percentages (%), p-values and post hoc comparisons are shown.
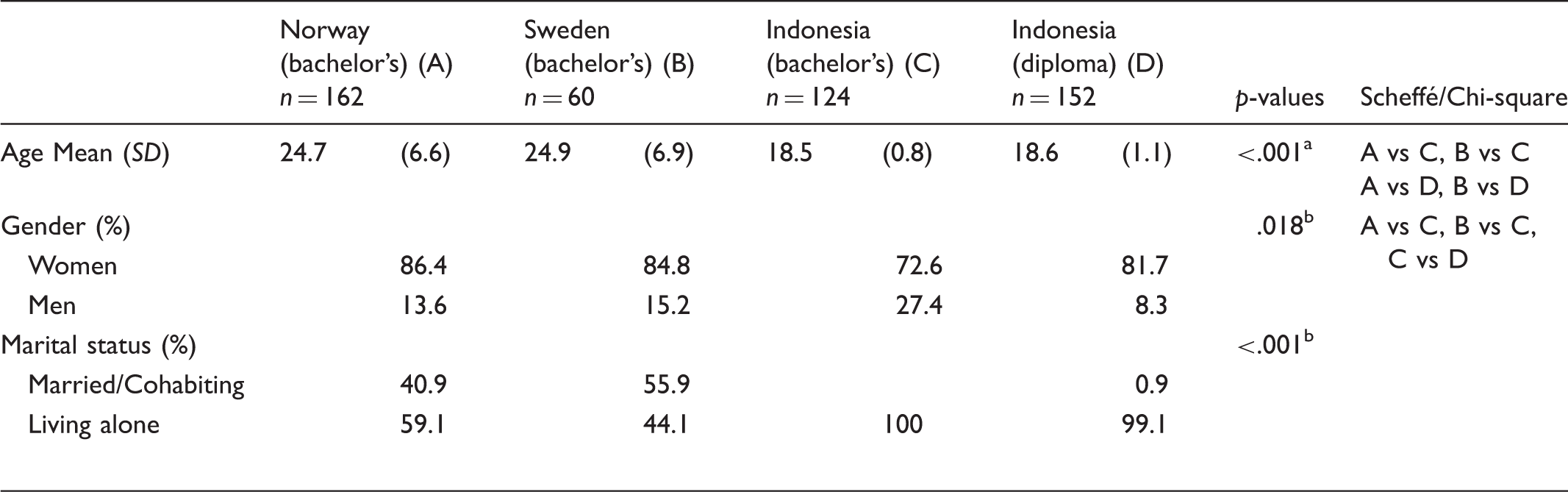
ANOVA, post hoc comparisons (Scheffé); bChi-square
The RUQ at T3: Descriptive data
Norwegian, Swedish and Indonesian nursing students’ perceptions of research utilization at the end of their nursing education (Time 3) – percentages (%) are shown.
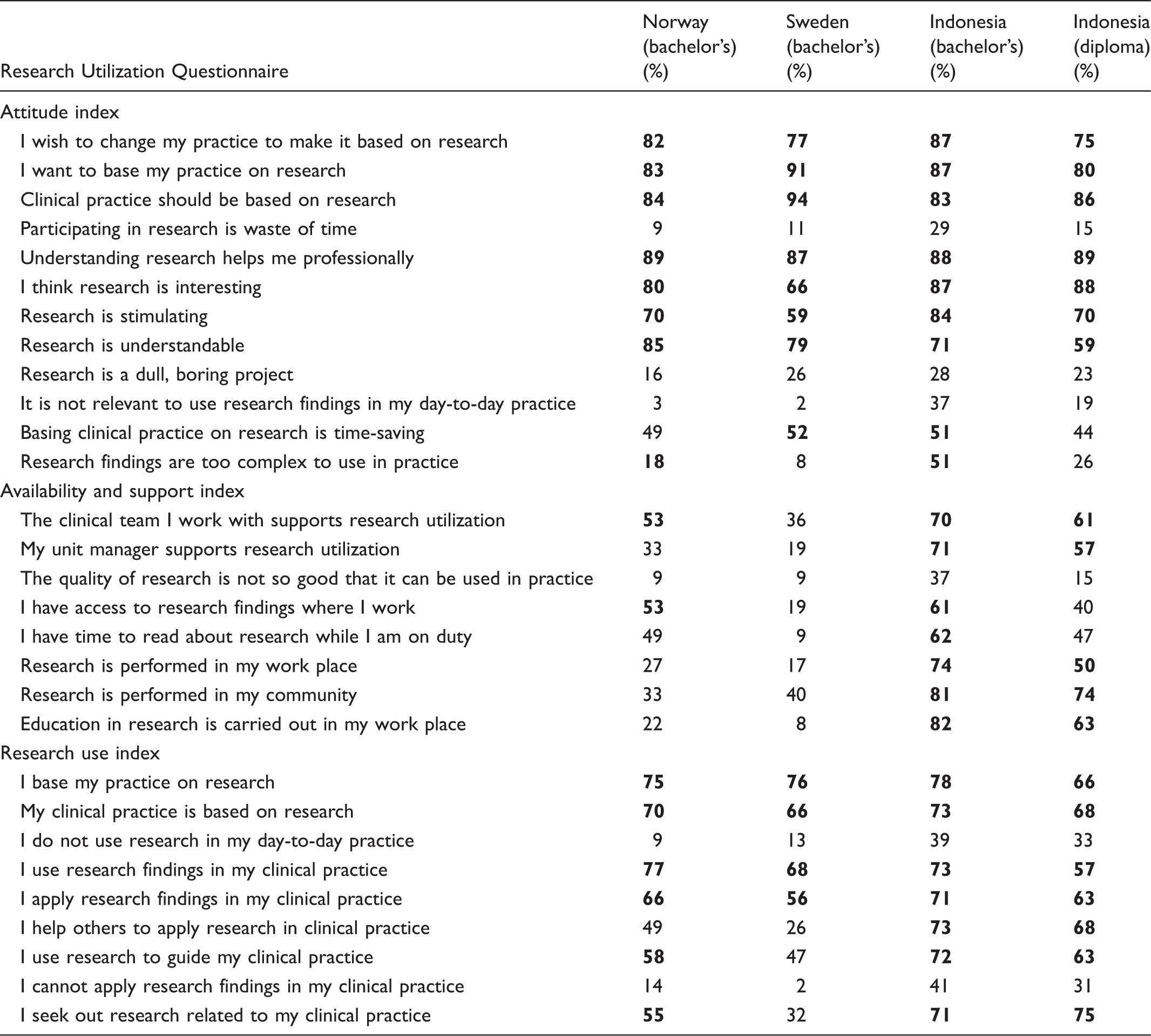
Bold figures show that 50% or more of the respondents agreed partly/strongly to the item.
The Barrier Scale at T3: Descriptive data
Norwegian, Swedish and Indonesian nursing students’ perceptions of barriers to research at the end of their nursing education (Time 3) – percentages (%) are shown.
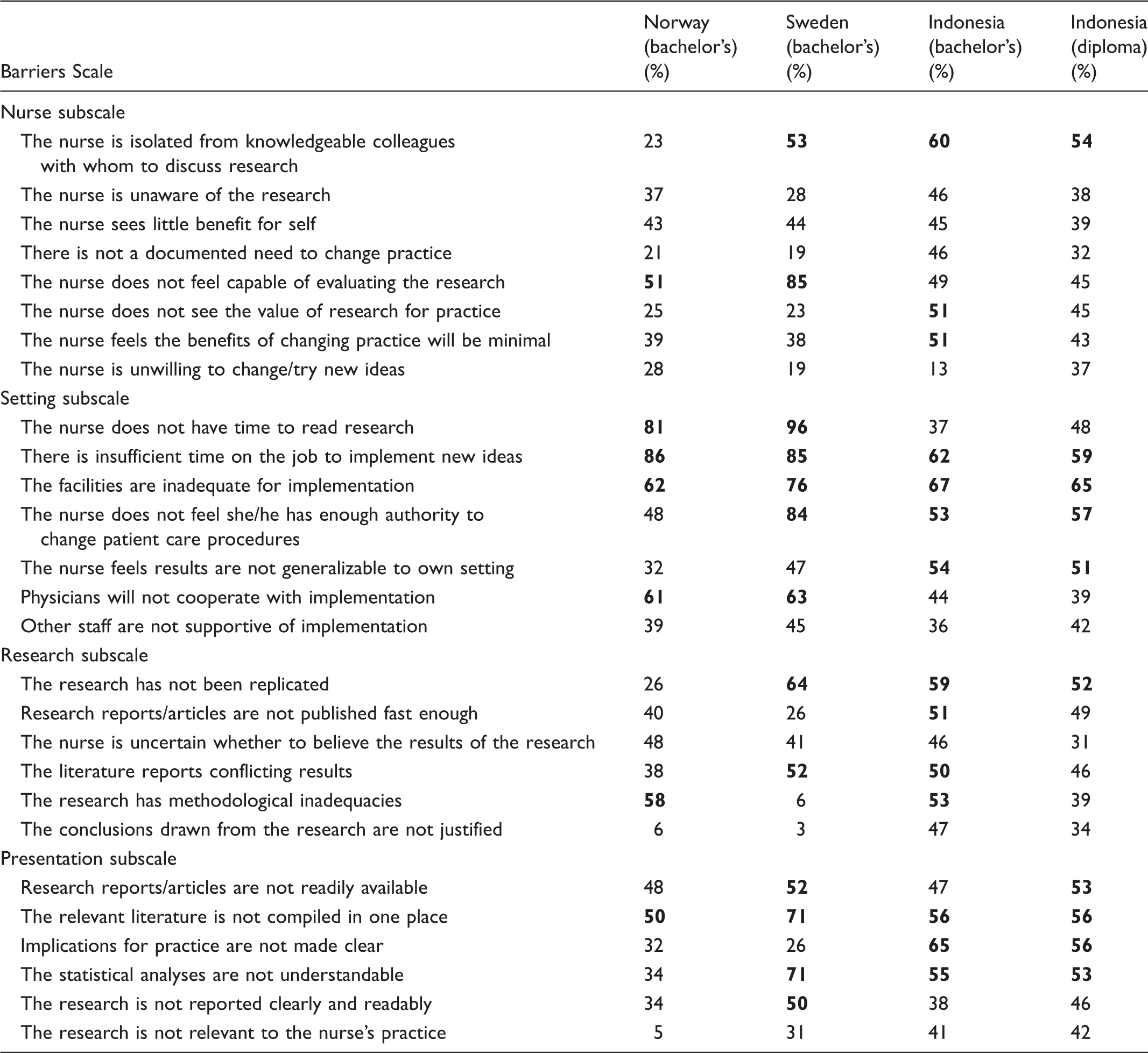
Bold figures show that 50% or more of the respondents agreed partly/strongly to the item.
The CTQ, the RUQ and the Barrier Scale: Between-group comparisons
Norwegian, Swedish and Indonesian nursing students’ perceptions of critical thinking, research utilization and barriers to research during their nursing education. Mean values (M) Standard deviations (SD), p-values (ANOVA) and post hoc comparisons (Scheffé) are shown.
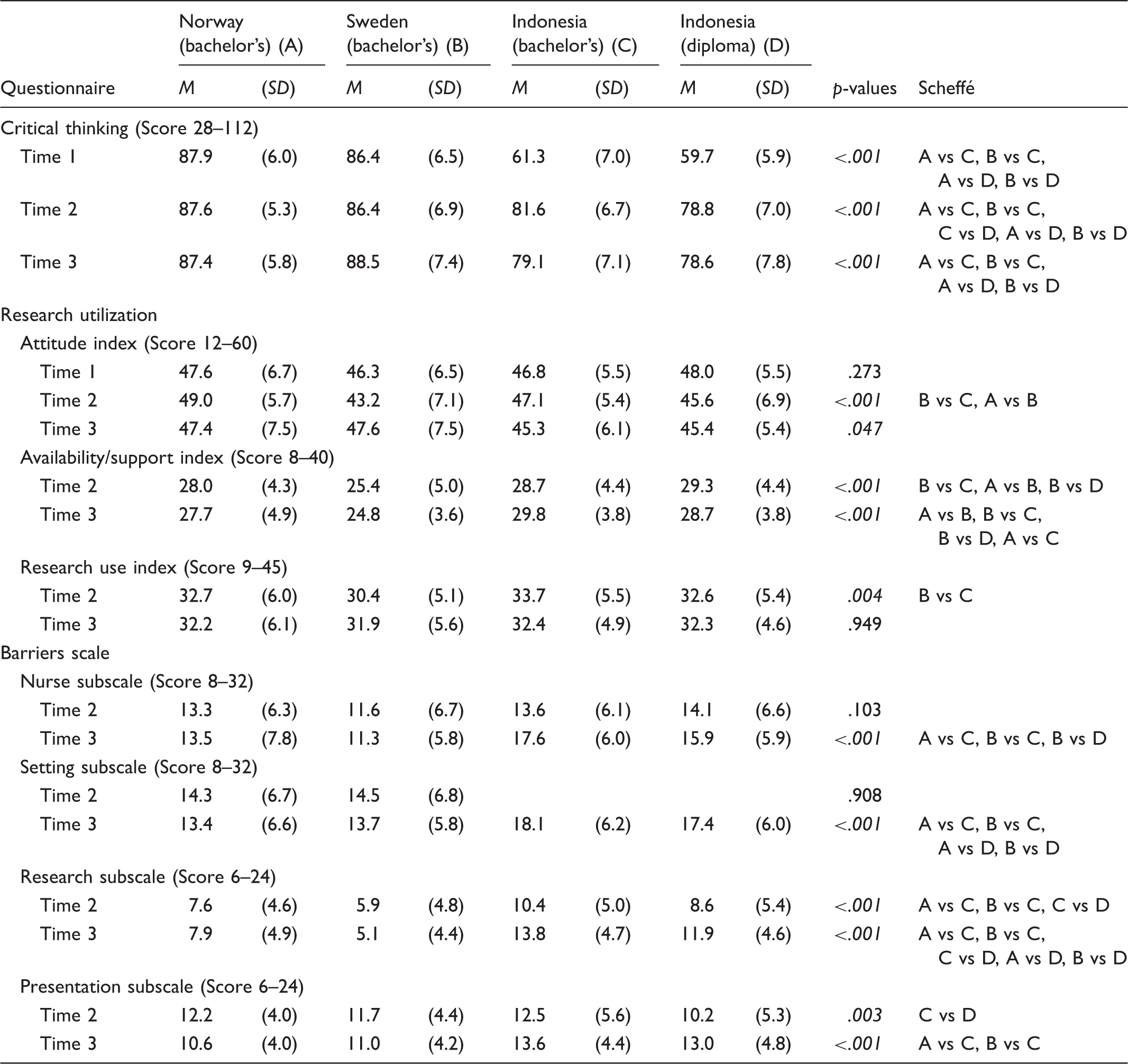
Statistically significant p-values are shown in italics.
Swedish, Norwegian and Indonesian nursing students’ perceptions of critical thinking, research utilization and barriers to research during their nursing education (between-group comparisons). Mean differences (M diff), controlled for age and gender (ANCOVA). Only statistically significant differences are shown.
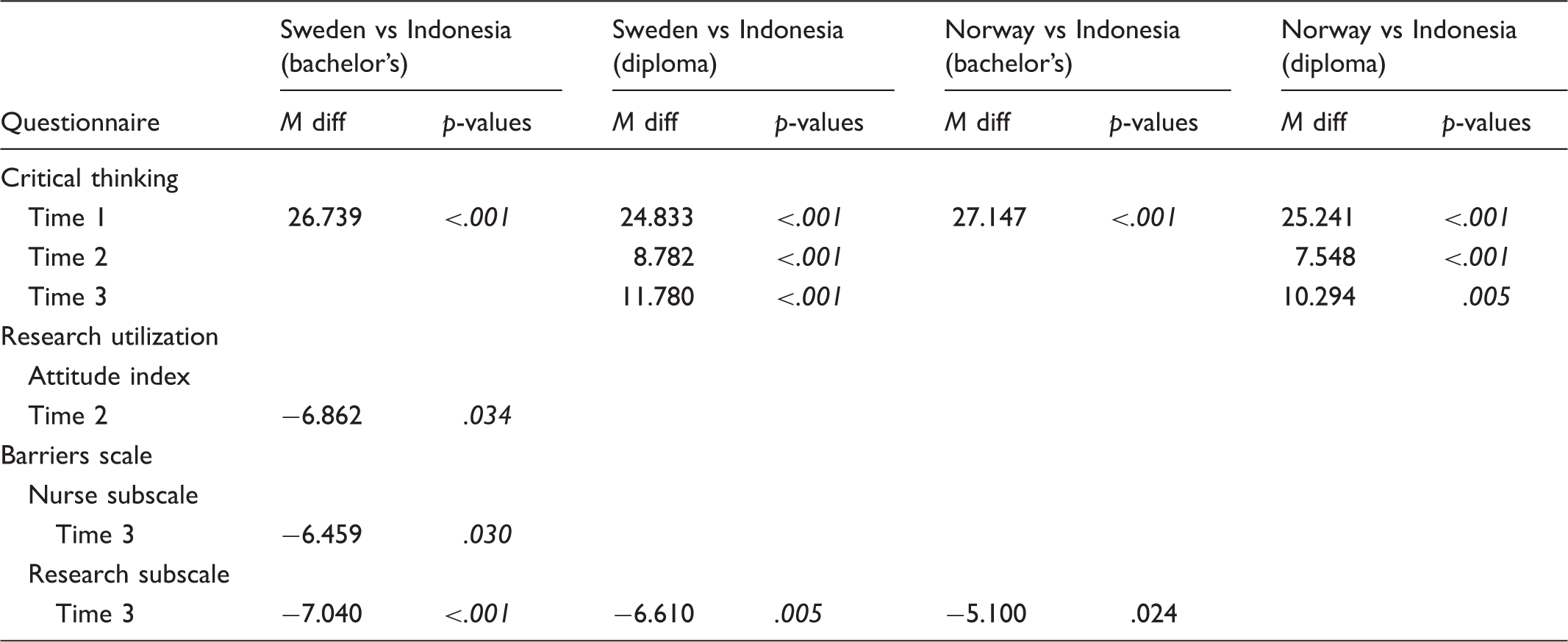
Statistically significant p-values are shown in italics.
As regards research utilization, the Swedish sample scored lower on the attitude index at T2, indicating a less positive attitude towards research compared to the Indonesian bachelor’s sample. On the Barrier Scale, significant differences were noted on the Nurse and Research subscales at T3. The Scandinavian samples scored lower, i.e. perceived barriers in this area to a lesser extent.
The CTQ, the RUQ and the Barrier Scale: Within-group comparisons
Swedish and Indonesian nursing students’ perceptions of critical thinking, research utilization and barriers to research during their nursing education over time within groups. Mean differences (M diff) Standard deviations (SD) and p-values (paired t-test) are shown. Only statistically significant differences are shown.
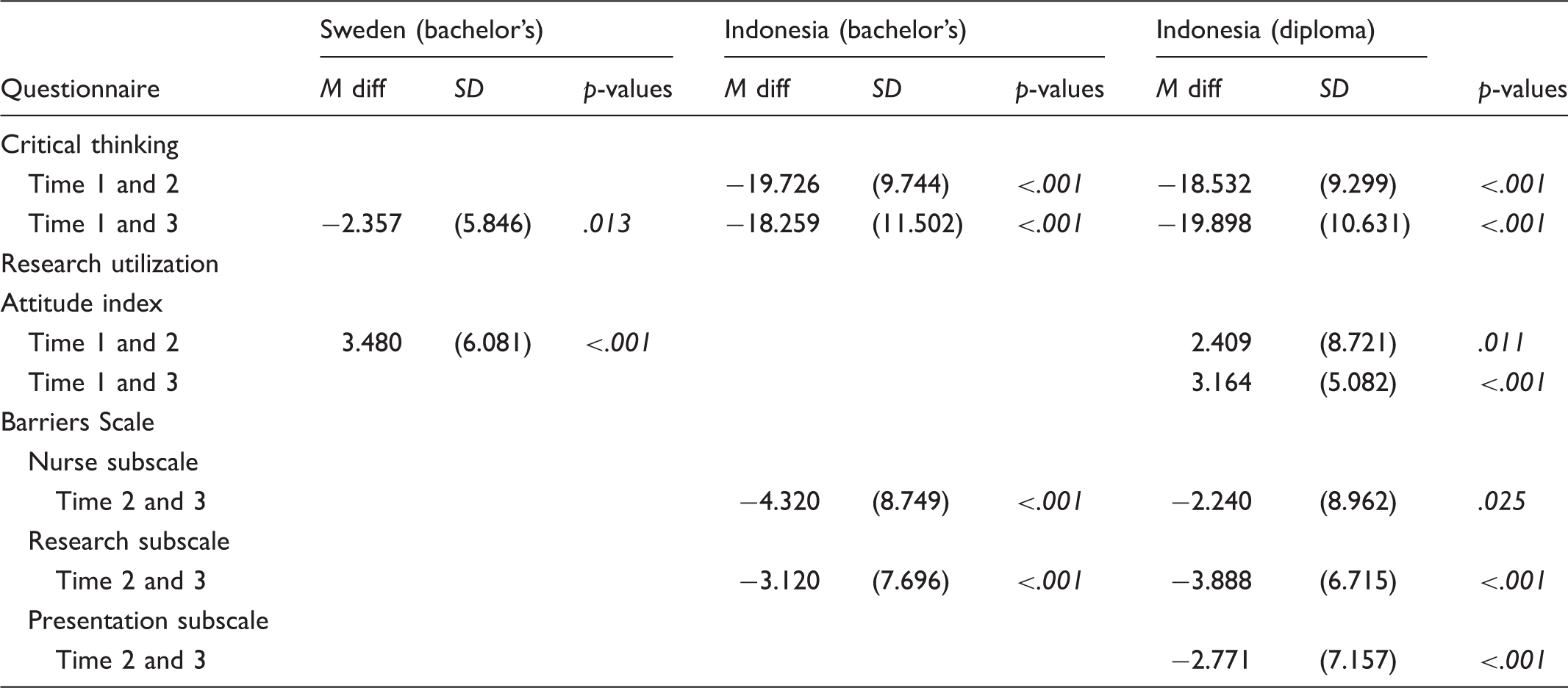
Statistically significant p-values are shown in italics.
Discussion
There is a global challenge for nurses to provide care based on current scientific knowledge, 6 and studies have shown that EBP results in improved quality of care, better patient outcomes and decreased costs. 30 It is of the utmost importance that educational institutions prepare nursing students by providing them with training in research methods, knowledge-seeking and critical appraisal.
The descriptive analyses demonstrated that at the end of their education all samples reported positive attitudes towards research on most items on the RUQ ‘Attitude index’. These results are in line with results among newly graduated nurses. 16 According to Saunders and Vehviläinen-Julkunen, nurses reported positive attitudes towards EBP, but did not use best evidence in practice. 31
Regarding the RUQ ‘Research use index’, the respondents reported fairly high values on half of the items. These figures are somewhat higher than those reported among newly graduated nurses by Wangensteen et al. 16 Forsman et al. reported that 34% of the nursing students intended to use research on more than half or almost every working shift in their future clinical practice. 32
The ‘Availability and support index’ revealed the need for improvement in several areas, e.g. support from the unit manager. Further, support to implement research findings has been shown to be a strong predictor of research use. 16 Support from unit managers is important for the development of nursing care and there is a need to create a culture that facilitates EBP. 33
Comparison of the results of the professional development scales between the samples was initially based on the raw scores showing that the Indonesian samples scored significantly lower than the Scandinavian samples on the CTQ and the RUQ, in addition to reporting greater barriers to research utilization. After controlling for age and gender most of the significant differences disappeared. Critical thinking constituted an exception. One reason for the lower CTQ values might be that the Indonesian samples were younger. This result is supported by Shinnick and Woo who found that age positively predicted total critical thinking skills scores. 34 However, contradicting results have been reported by other authors.35,36
According to within-group comparisons related to the RUQ ‘Attitude index’, the Indonesian diploma sample reported less positive attitudes over time. This might be due to these students developing a more critical view on this aspect, which could be supported by the fact that they scored significantly higher on the CTQ over time. Regarding the Barrier scale, the descriptive analyses indicated that the main barriers were related to the setting. This was also shown in a systematic review by Nilsson Kajermo et al., 18 and in studies by Tan et al., 37 and Wang el al. 38
When age and gender were controlled for, significant differences were noted on the Barrier subscales Nurse and Research. The Indonesian samples perceived barriers to a greater extent. One reason might be limited resources, e.g. teacher competence and availability of learning material.39,40 According to the within-group comparisons of the Barrier Scale, most changes over time were found in the Indonesian samples, who perceived greater barriers related to the subscales Research and Presentation (only the diploma sample). This was not the case among the Scandinavian samples. One interpretation might be that during their nursing education the Indonesian students developed a more critical view over time.
To our knowledge, no longitudinal studies using the Barrier Scale have been carried out. However, it is possible to relate our findings to the results presented in an earlier systematic review showing no significant differences in mean values when comparing studies on barriers to research utilization. 18
Regarding critical thinking, the between-group comparisons revealed that the Scandinavian samples scored higher on critical thinking compared to the Indonesian samples. However, the within-group comparisons showed significantly higher levels of critical thinking over time among all samples except for the Norwegian sample. Increasing levels of critical thinking scores over time among nursing students are also reported by Pitt et al. 21
One reason for the differences in critical thinking and barriers to research utilization might be a divergence in the competence level of Scandinavian and Indonesian teachers. In the Scandinavian countries there are more teachers with master’s degrees and PhDs, while in Indonesia nurses are often offered teaching positions immediately after graduation.4,5,41 Consequently, they have limited clinical experience, 40 which in turn may result in reduced potential for critically observing reality. In addition, the Indonesian education system is influenced by the American curriculum and thus often uses English-language literature. Moreover, due to limited resources there might not be enough literature available for the students. Consequently, the students have to memorize facts that are read aloud by the teacher. According to Diekelmann and Smyth it is well known that passive learning methods like this limit critical thinking development. 42 This does not promote either critical thinking 43 or the development of evidence-based practice, both of which are important for high-quality patient care. As studies have demonstrated that critical thinking is related to research utilization, it is recommended that critical thinking be recognized and strengthened both in nursing education and clinical practice.16,44 Several studies have been conducted in order to develop nursing students’ critical thinking abilities with variable results.45,46 However, problem-based learning (PBL), simulation, and concept mapping seem to be the most common educational interventions used to promote critical thinking development.
Methodological considerations
This study focuses on perceptions of critical thinking, attitudes to and availability of research, as well as research utilization and barriers to this among nursing students in two samples from Scandinavia and two samples from Indonesia during their nursing education. The RUQ and the Barrier Scale have been validated in several other studies and were pilot tested for the target groups in this study. The translation process followed a well-established procedure, 22 which is considered a strength when different countries are involved. The reliability of the RUQ indexes and the Barrier subscales was satisfactory for most scales. The CTQ was specifically developed for the present study and face and content validity was established. Cronbach’s alpha values were satisfactory on two occasions and somewhat low on one. The Cronbach’s alpha coefficients presented in the article are based on the total of all four samples. If computed within each sample within each assessment point (72 computations all together), fairly similar, yet slightly higher, reliability values were obtained.
The response rate is considered high for all samples, with the exception of the Norwegian sample at T2 and T3. According to Polit and Beck, the response rates, apart from two of the Norwegian ones, are satisfactory. 47 Students were recruited from a limited number of settings. Future studies could improve the generalizability by recruiting samples from more settings in different countries.
As the data were self-reported, the assessments of professional development may be influenced by the wish to provide socially desirable responses. This might be a threat to validity and should be kept in mind when interpreting the findings. 9
Summary and conclusions
At the end of their education, all samples exhibited positive attitudes towards research and the main barrier was related to the setting. The Scandinavian samples reported a higher inclination towards critical thinking. The Indonesian samples perceived greater barriers on the Barrier subscales Nurse and Research. No differences were found between the samples in terms of research utilization. Significant changes regarding professional development over time were found to varying degrees among all samples except for that from Norway. The Indonesian diploma sample showed the most changes over time.
It is important for teachers to support nursing students so that their critical thinking ability is strengthened, thus enabling them to develop their professional competence. A suggestion for future research is to focus on strategies to increase professional development among nursing students. It would also be of interest to explore teachers’ level of competence related to evidence-based practice.
Footnotes
Acknowledgements
The authors wish to thank Jari Appelgren for valuable statistical advice and assistance and Monique Federsel for reviewing the English language.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.