
Abstract
Thirteen carers were interviewed about their ethical reasoning when using a common staff approach to restricting smoking for a psychiatric in-patient. A constructed case structure and a vignette method were used in the interviews, and manifest content analysis of the texts exposed five ethical positions adopted by the carers: ‘best for the person’, ‘best for the patient’, ‘best for others involved with the person/patient’, ‘best for me as a carer’, and ‘best according to rules and regulations’. A second manifest content analysis of language showed terms that expressed value judgments in regard to the carers’ personal experiences. Some carers argued at first from one ethical position, but when the question was changed, they argued from an opposite ethical position. Results may be understood in light of dialog philosophy; ethical reasoning during use of a common staff approach tends to focus either on relations with others or with oneself.
Introduction
This article is about ethical reasoning among carers when applying a common staff approach toward patients in psychiatric care. Carers working in psychiatric care may have different ideas about the social norms a patient should accept and conform to. 1 In Sweden, however, a structured care program is regarded as important for successful care episodes and for meeting the patient’s need for security in a controlled environment. 2 Carers try to achieve a stable milieu through a adopting a similar approach in interactions with the patient. A ‘common staff approach’ should here be understood to include the social process in which carers in psychiatric in-care or working at communal group dwellings formulate a common approach in their behavior toward a single patient. 3 In this social process the carers characteristically negotiate with each other about how to deal with the situation, while the patient in focus has little or no knowledge of or influence over the process. The carers describe their desire to preserve and restore order by adopting a common staff approach, but also their difficulties in maintaining the common approach over time. In an additional study nine carers were interviewed about their experiences in situations that included a common staff approach towards a single patient in psychiatric in-care. 4 This study showed that individual carers had a difficult choice between focusing on their relations with their colleagues or relations with the patient, who appeared to suffer when a common approach was used. When a common staff approach was present the carer became aware of their own values and those of others, aware of the patient’s suffering, and more likely to feel judged by others and by their own consciences. In a related study, nine patients with psychiatric in-care experiences were interviewed about their experiences of being cared for with a common staff approach. 5 The main result was that patients suffered greatly under the common approach, but they also felt secure when the carers took over their responsibilities for them.
Background
A number of studies have explicitly aimed to investigate the ethical and moral standpoints and actions of carers, most often nurses, in psychiatric care.6–9 Related studies of carers’ experiences of providing psychiatric nursing care at communal group dwellings or psychiatric in-care settings highlight ethics,10–13 empowerment, 14 or control and protection of patients. 15 Earlier studies of a common staff approach in psychiatric care have shown that ethical questions and conflicts between ethical perspectives arise when carers have to choose whether to be loyal to their colleagues or to the patient.3–5 However, although nurse-initiated rules in psychiatric care have been investigated 16 no study to our knowledge has aimed explicitly to investigate the common staff approach from an ethical perspective. Psychiatric patients are in a vulnerable situation when being cared for; often not being able to control their personal milieu when admitted to a psychiatric ward. This makes it of utmost importance to investigate carers’ ethical reasoning when a common staff approach is present. How does the carer’s personal standpoint influence the care received by the patient? The aim of this study was to describe ethical reasoning among carers when applying a common staff approach toward patients in psychiatric care.
Method
Participants
Characteristics of the participants.
Specialization in psychiatric care, three nurses.
Ongoing training for specialization in psychiatric care, two nurses.
Data collection
Methods for data collection
A vignette method was used to prompt the interviewees to disclose their ethical reasoning. A vignette, or short story, describes a situation or episode with characteristics that the researchers regard as important and critical to a person’s choice of action in a specific situation.17,18 This method has been used previously to explore ethical standpoints held by nursing staff in relation to forced feeding 19 and the use of physical restraints. 20
The vignette, based on knowledge obtained in earlier studies of the common staff approach,3–5 was constructed to elicit the interviewees’ personal ethical reasoning in a hypothetical case of a common approach used to restrict smoking in a psychiatric in-patient. The interviewees were aware of the aim of the vignette and of the study. The vignette consisted of two parts: a situation presented to the interviewees (Appendix 1), and four scenarios for respondents to consider depending on the interviewee’s response to the vignette (Appendix 2: these questions were asked but not shown to the interviewees).
In the first stage of the interview, the interviewee was handed the vignette in writing and asked to read it for a few minutes, after which they were asked to answer three questions: ‘What is your decision?’ ‘How would you act in practice?’ and ‘What are your arguments (what is your reasoning) for your decision and action?’ Depending on the interviewee’s decision to give or not to give cigarettes, follow-up questions were asked based on four constructed scenarios (Appendix 2). Finally, all interviewees were asked what other condition might influence them to change their original decision to give or not give cigarettes.
All interviewees spontaneously said they were familiar with the situation described, and one person said, ‘This is a classic’. Several interviewees asked for more information in order to find a practical solution to the situation, but they were directed back to the information that was given in the vignette and asked to interpret it based on their own experiences. Nine of them expressed difficulty articulating a specific standpoint in relation to the scenarios and said there was more than one way to act. The researcher then asked them for the alternative they would be most likely to use.
All interviews were held in private rooms at the wards and lasted between 45 and 75 minutes. Interviews were tape-recorded and transcribed verbatim, and the transcriptions were validated against the tape.
Analysis
Two separate content analyses were performed in order to describe ethical reasoning among carers. One analysis of language to grasp ethical language used by the carers; and another analysis of text in order to describe ethical standpoints made by the carers. The two analyses can be seen as supplementary in order to understand more about the phenomenon studied.
Analysis of language
A content analysis of language was performed from a non-normative perspective, 21 seeking the manifest content. The aim was to present a picture of the carers’ ethical language in reasoning about a common staff approach towards a single patient. The interviews were read line by line, and terms expressing values were sorted into three predetermined categories: 1) axiological terms expressing value (e.g. good, bad, helpful, healthy, ill); 2) deontological terms concerning rights and obligations (e.g. right, wrong, permitted, responsibility, duty); 3) anthropological terms concerning human actions (e.g. aim, motive, will, feeling, action). 22
Analysis of text
Qualitative content analysis,18,23 seeking the manifest content, was used to describe carers’ ethical reasoning when using a common staff approach. The interviews were read line by line and analytic units, expressing arguments for carers’ actions in relation to the vignette, were identified. These analytic units were then coded and categorized (including subcategories when necessary) in order to describe the carers’ ethical reasoning.
Ethical considerations
The Regional Ethics Committee of Umeå, Sweden, approved the study (permit Dnr 2010-47-31). Contact with participants joining the study was mediated by an education nurse at the clinic. If willing to be interviewed the career contacted the principal investigator. Written consent was asked for and obtained from each participant. Special attention was paid to explaining the purpose of the study to the interviewees. All participants were given time to reflect on whether they wanted to join the study, and all who contacted the investigator chose to be interviewed.
Results
Analysis of language
In the manifest content analysis of language, 55 axiological terms were identified, of which 31 were judged to hold a negative value, for example ‘nagging’, ‘disturbing’, and ‘stupid’; 15 terms were linked to a positive value, for example ‘democratic’, ‘participant’, ‘broad-minded’; and the remaining 9 terms were judged to hold a neutral value, for example ‘strictly’, ‘harmless’. There were 97 deontological terms detected, mostly two-words phrases such as ‘common decision’, ‘stay put’, and ‘respect for’. These terms were mainly about responsibility and restricting other people’s actions. Anthropological terms formed the largest group, consisting of 210 terms, mainly linked to personal experiences, which could also include two-word phrases such as ‘under pressure’, along with single words such as ‘failure’, ‘disappointment’, and ‘safety’.
Interestingly, when carers expressed views that were not in favor of the patient, they often used the pronoun ‘we’, speaking on behalf of the entire staff, but when they expressed opinions in opposition to their colleagues’, they would use ‘I’.
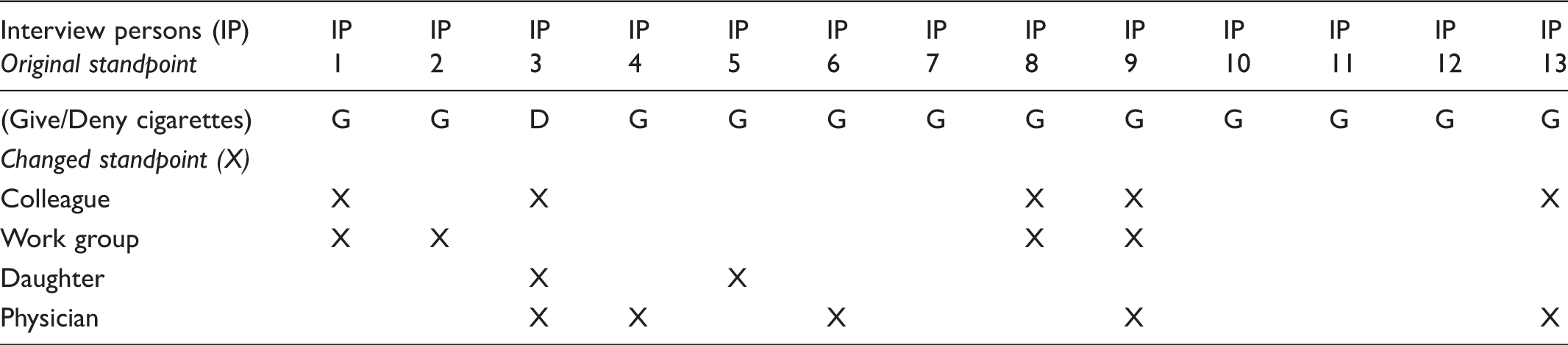
Analysis of text: Initial standpoints
Conditions that would make carers change their personal standpoints on giving (G) or denying (D) extra cigarettes.
Ethical reasoning
Categories in text analysis.
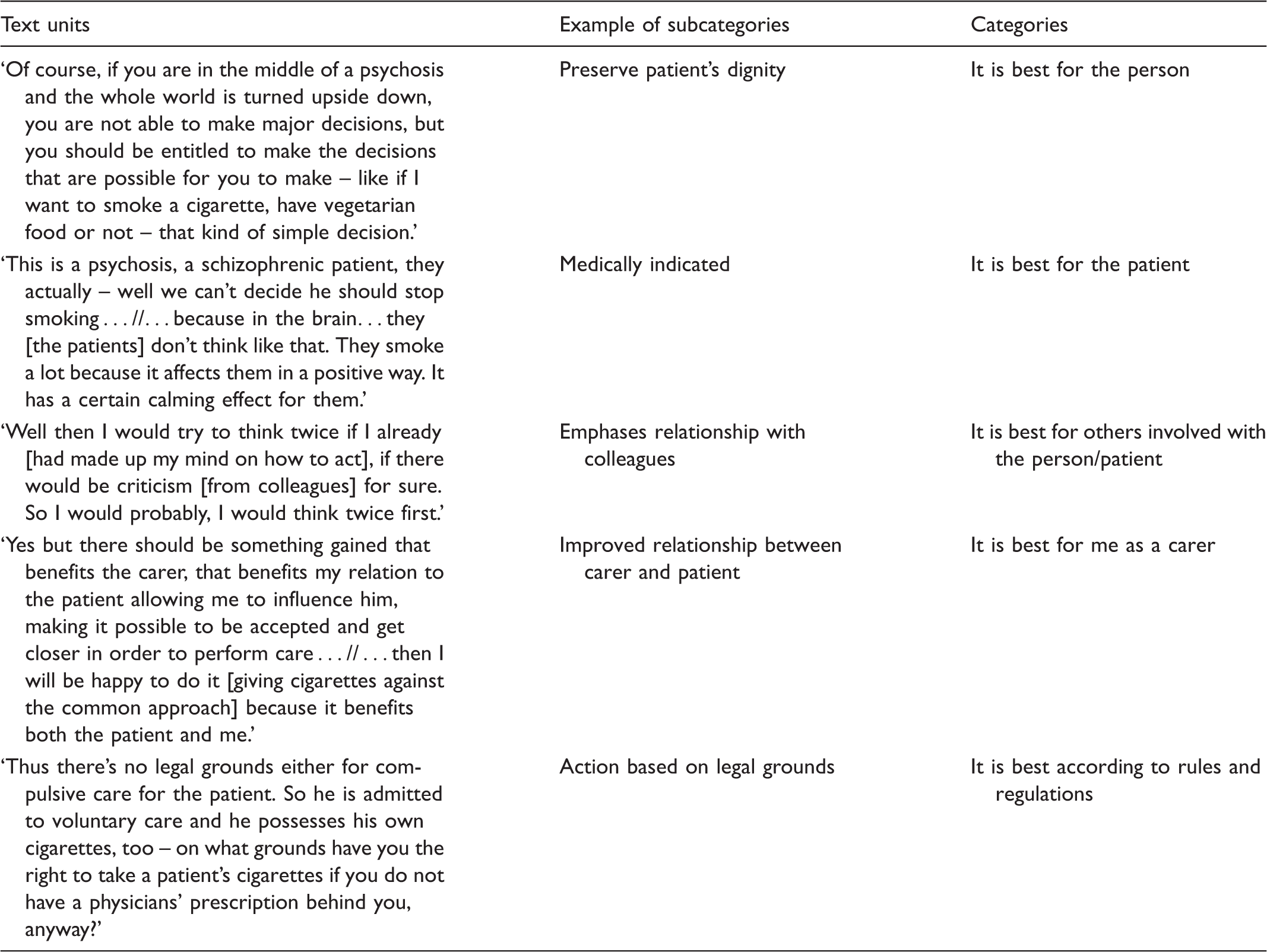
Category: It is best for the person
In this category the carer argues for actions based on how they will affect the patient as a person and how the carer thinks the person will perceive the carer’s actions in a given situation. This means the carer focuses on the person’s lifestyle and choice of living and not on being a psychiatric patient.
Give cigarettes
The carers argue for giving cigarettes in order to preserve the person’s autonomy and to allow the person, as much as possible in psychiatric in-care, to make his own decisions, such as whether or not to smoke. Of course if you are in a middle of a psychosis and whole world is turned upside down you are not able to make great decision but you should be entitled to make the decision that is possible to make – as if I want to smoke a cigarette, have vegetarian food or not – that kind of simple decisions.
Deny cigarettes
Carers arguing from this perspective for denying further cigarettes suggest that it would prevent problems for Steve in the long term by helping him learn to make his cigarettes last longer when he is out of hospital: The patient will not be able to buy new cigarettes when these ones are gone. So you give a specific number per day … // … And it is definitely done out of concern, otherwise this person will be standing without cigarettes only three days after he gets his pension.
Category: It is best for the patient
In this category arguments are based on what is deemed best for the patient’s physical and/or mental health, and the patient is assumed to be incapable of taking responsibility for his own situation; therefore, the carers have a responsibility to act in the patient’s interest. This means the carer argues from a professional’s medical perspective. The person is seen primarily as a psychiatric patient.
Give cigarettes
Arguments for giving cigarettes in this category assume that the patient is unable to take responsibility for his smoking because of his mental illness, and because of this the carers have to ensure the patient has cigarettes. The carer reasons that if the patient’s state could deteriorate as a result of mental stress caused by the common decision not to give him cigarettes, it will promote the patient’s health to give him cigarettes, even if it means going above the limit of 20 per day: Yes, but then I would say the patient isn’t … he is in bad mental shape due to his illness. He is unable to see, and it could be a behavioral tic, his nagging [for cigarettes].
Deny cigarettes
The argument in this category to deny cigarettes is that the patient’s bad physical health, coughing, and breathlessness may make it medically indicated to deny any further cigarettes at all: Well, if I knew there was something wrong with his lungs or something, him coughing blood or not being allowed to smoke because of … well danger for his life to smoke – then I would not give him a cigarette. But I think this is the only obstacle.
Category: It is best for others involved with the person/patient
In this category the reasoning is based on how the carers think their actions affect people other than themselves or the patient, such as colleagues, relatives, and fellow patients.
Give cigarettes
Arguments in this category include protecting other patients from the patient who may beg or be otherwise annoying to people in his environment when out of cigarettes: Yes, and fellow patients will be affected if he does not get his cigarettes. My experience is that it will not turn out well and it will get grouchy, unpleasant, and tense between patients when one [patient] walks around and begs. And there are those who have a hard time saying no, who give away more cigarettes than they ought to.
Deny cigarettes
Initial arguments in this category to deny the patient further cigarettes are mainly based on the opinion that a patient who harasses the carers, nagging them and shouting at them, should not be rewarded for such behavior by getting a cigarette. Carers in this category against giving cigarettes also argue that if the patient fails to meet carers’ expectations of behavior, by trying to manipulate them or lying about how many cigarettes he has obtained earlier, the common approach of not giving the patient further cigarettes should remain strictly in force: If I tell you – on this specific ward, it would not benefit him if he got the chance to negotiate. It would not benefit the staff either … // … to have to take the fight, so to speak. No it would only get worse.
Category: It is best for me as a carer
In this category arguments are based on how the carers think the situation affects them and their ability to care for the person/patient. Carers argue they should not be tied to the common staff approach when that approach does not benefit or ease the situation the carer is in with the patient.
Give cigarettes
Initial arguments from this perspective maintain that the specific situations carers find themselves in give them the right to act from their own understandings and interpretations. Carers also argue that if they were not involved in the common staff agreement, they would have no obligation towards upholding the decision as they do not recognize the authority of colleagues on one shift to make binding decisions about how they should act on their shift. Carers also expressed the opinion that in the face of decisions that they feel are not feasible, carers should express their own personal beliefs in choosing what action to take and follow their own decisions.
Others argue that common-approach decisions are ineffective because the patient will always manage to get around it somehow, and therefore it is useless to follow it. Another argument from this perspective is that the common approach puts the carer’s desire to avoid conflict and to preserve good relations with the patient by not following the staff approach in opposition to avoiding conflict and maintaining good relations with colleagues. Yes but there should be something gained that benefits the carer, that benefits my relation to the patient allowing me to influence him, making it possibly be accepted and get close in order to perform care … // … then I will be happy to do it [giving cigarettes against the common approach] because it benefits both the patient and me.
Deny cigarettes
Carers who argue from the primacy of their caring relationship with the patient can also argue in favor of following the staff approach and denying cigarettes based on their own power, precedence, and better knowledge of what is good for the patient: Then I will override his opinion because of, of … I am the one that is caring for him, in fact harsh … // … and then from the perspective of my profession I will take the right to deny him.
Category: It is best according to rules and regulations
This category includes ethical arguments that rely on rules and regulations to govern choices of action. These range from law and government regulations to local policies.
Give cigarettes
In this category, those who would give cigarettes to Steve argue that a common staff approach that overrides the patient’s will to control his own smoking goes against the intention of the healthcare act, and is thus prohibited: If you have a patient who is admitted to in-hospital care voluntarily you cannot do anything really against the patient’s will. So the patient is responsible for his own cigarettes and we [the staff] can think what we want about it.
Deny cigarettes
On the other hand, the carer can feel obliged to follow formal and informal local rules at the ward, even if the carer disagrees with them: Well I can stand firm in my beliefs but still it can be like: but no we work in this way at this ward, we will take the fight [with the] patient. And then I might give in [to the staff] even if I disagree. But had it been up to me I would have given him cigarettes.
Discussion
The main results show that ethical arguments for deciding how to act are personal and based on a variety of perspectives and values that can shift or even reverse in the same carer, depending upon who is affected by the action in question. Shifting grounds of ethical reasoning could be seen in the scenario in which colleagues were in favor of not restricting smoking; some carers abandoned their earlier arguments for allowing cigarettes, based on promoting patient autonomy, and began to argue for denying cigarettes on the basis of preserving their good relationships with colleagues. Furthermore, the same grounds for argument could be used to support different positions, such as when advice from a physician as a medical expert overrode concerns about patient autonomy on one hand and staff solidarity on the other. Isobel has shown nurses in psychiatric care can be frustrated over rules and policies they have to implement about banning smoking or phone restrictions, criticizing colleagues for using rules as a way not to be engaged with the patient. 16 Løgstrup asserts that every person has an ‘ethical compass’ within, guiding the person to make the right ethical choices in life. 24 In this study this is seen in several statements such as ‘Well I stay firm in my beliefs but still it can be like: but no we work in this way at this ward, we will take the fight [with the] patient …’ even if the carer choses to override his/her personal opinion in the end. This reasoning is diametrically opposed to Kant who believed that moral laws are the only moral basis for action, and actions based on feeling never can be moral. 21 Interestingly the same situation citied above can also be seen as an example of a Kantian ethic – promoting rules as being right before personal feelings. In other words it is a matter of perspective how carers’ ethical reasoning about using a common staff approach in psychiatric care can be apprehended and understood.
In this study the results deal with the fact a person can also be a patient and vice versa. Being a person focuses on the human being in a humanistic tradition and without reductionist limitations, 25 while being a patient is to be in a constructed role defined by others, 26 for example, someone bearing pains or trials 27 or a person receiving or registered to receive medical treatment. 28
Jansson and Norberg 19 found when investigating ethical reasoning among nurses experienced in dementia care that the principle of autonomy was prioritized by the nurses; and Karlsson, 20 who investigated restraint use in elderly care, found the principle of beneficence was the most common ethical principle. In the present study, the specific ethical principles used were not investigated; however, no particular principle seem to be favored. The categories did, however, take different approaches and adopt different values: ‘It is best for the person’ respects the other person’s life-world; ‘It is best for the patient’ takes a more authoritative view, with arguments based on the carer’s superior ability to handle the situation; ‘It is best for others involved with the person/patient’ is concerned with preserving equilibrium on the ward and not upsetting colleagues, relatives, or other patients; ‘It is best for me as a carer’ focuses on the carer’s individual situation on shift; and ‘It is best according to rules and regulations’ argues to enforce the will of a superior, outside authority. This variety of ethical bases can partly be understood as support for Løgstrup’s statement about each individual’s own moral position. 24 It remains to be explained how the argument changes in the same individual in the same given situation – to give or to not give extra cigarettes – based only on the suggestion of various other people’s opinions; although some carers did maintain their original opinion and ethical reasoning, no matter how the scenario was changed.
The results may also be understood in light of dialog philosophy,29,30 which is inspired by phenomenology, and can be seen as a part of modern philosophical anthropology that assumes a human’s being is linked to the world and to other people. 26 Friedman writes about the ‘self in context’, in which ethical reasoning may follow two directions, as in this study; the first direction is represented in arguments that focus on interpersonal relationships, I confirm You, even if we don’t agree, ‘the confirmation of otherness’. 30 This direction respects the other person’s life-world and what is created between people. The other direction does not lead to complete confirmation of other; the argument doesn’t fully recognize the other person’s experiences and will not go into an ontological dialog, in this study represented by arguing ‘this is best for me as a carer’. An earlier study on carers’ lived experiences of caring when a common staff approach has been adopted has shown it is a difficult choice for carers to choose whether to focus primarily on the patient or their colleagues, since by they are unable to chose both in that situation. 4 The content analysis of the language shows the identified words are words used to position people in relation to others, which may partly support the dualistic approach of argument focused primarily either on others and relationships or on the self. Also as mentioned above, to be a patient, and especially a psychiatric patient, can be seen as being forced to adopt a constructed role defined by others.26,31 Even though the analysis of language 22 has been performed in a non-normative perspective 21 the results might indicate there are several ethical norms held by the interviewees.
An earlier study showed that the use of a common staff approach towards individual patients can be associated with increased suffering for the patient. 5 The use of a common staff approach is probably very common in Swedish psychiatric care, 3 therefore, we need to increase our knowledge about carers’ ethical reasoning when using this approach in psychiatric in-care in order to humanize this care.
Methodological considerations
A vignette gives a limited situation, a common frame of reference for the people interviewed, and it should be easy to follow and understand, logical, fairly simple, and trustworthy. 17 Though smoking is banned at many hospital facilities in Sweden, psychiatric in-patients can often be heavy smokers. Because of this the vignette used was constructed with a topic a carer easily could recognize and have to cope with on daily basis. The aim of the vignette can be open or closed to the interviewee.18,32 When using a vignette technique there are limitations to consider about the validity of responses; for example in responding to the hypothetical case, the carers’ interpret the text individually and fill in any missing information from their own experiences. It is also uncertain how accurately answers reflect interviewees’ behavior in real situations.17,18 In this vignette study, the questions were constructed to produce answers that were as in depth as possible and every answer was followed up with a new question asking for further details of the carer’s opinion.
In this study, two methods were combined to better illuminate data relevant to the research question. A qualitative content analysis of the text was performed parallel to a content analysis of the language. When using content analysis, one must bear in mind there is no clear specific scientific ground for the method, even if traces of structuralism 33 and communication theory 34 can be detected. However, the same strict criteria as when using other scientific methods must be applied. Kvale35,36 writes that ‘truth value’ must be considered the object in all qualitative research and lists three criteria to obtain it: ‘coherence’ – it should be possible to follow threads of meaning in the constructed themes; ‘construct validity’ – there is not a single universal truth, instead the themes should reflect a social construction of reality; and ‘trustworthiness’ – when using qualitative methods credibility, dependability, and transferability should be ensured.23,37 For example in this study all steps when constructing the vignette, in collection and data analysis were discussed among the authors. The authors also separately read each text and discussed coherence. It should also be recognized that there is a slight risk of blur in framework when nurse-researchers conduct research in the clinical field, mixing scientific research methods with nursing competencies and their own personal and moral values, as described in a vignette study by Wilkes et al. 38
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.