
Abstract
Building trustworthy relationships that promote equal participation is a fundamental feature of daily living in dementia care. Creating a social community is thus a key component of quality of life for residents in dementia special care units. The aim of this study was to explore healthcare personnel’s experiences of enhancing social community in common spaces in dementia special care units. A qualitative descriptive design consisted of four focus-group interviews with 15 healthcare personnel. The transcribed interviews were analyzed inductively using qualitative content analysis. The findings revealed that healthcare personnel’s experiences of enhancing social community in common spaces were related to three main themes, expressed as dilemmas between knowing versus not knowing each other, safety versus unsafety and presence versus absence. Our analysis indicates that to enhance social community, it is essential for healthcare personnel to be able to create different forms of proximity to residents: physical, narrative and moral. Moreover, the meaning and role of ‘proximity’ in dementia care should be further explored as organizational context influences spatial-structural practices and may disrupt proximity in dementia care.
Introduction
Building trustworthy relationships that promote equal participation is a fundamental feature of daily living in dementia care. As the disease progresses, many people with dementia experience increased social isolation and may require long-term care to feel safe, experience togetherness and derive a sense of belonging to others. 1 In dementia special care units (DSCU), facilitating the formation of a community that promotes positive social interaction is a key component of residents’ quality of life.1,2 Over time, people with dementia gradually lose their social skills, and it becomes difficult for them to express themselves, enjoy conversations and/or comprehend their present circumstances. Nevertheless, being in the company of others is essential, because human connectivity may help repair the social rupture that accompanies dementia. 3 In that relationships are related to quality of life in dementia care,1,3–5 it is necessary to understand the significance of the relational components of the social community formed during care. It is therefore important to recognize the contributions that both healthcare personnel (HCP) and residents make toward forming relationships and, thereby, a social community. 6
It is not possible to separate the relationships between HCP and dementia residents and the social community from the DSCU setting (place) itself.7–10 A nursing home is not merely a physical location; it is also a place that holds meaning and attachments for people.11–13 Brown Wilson describes a social community as a place where meaningful reciprocal relationships are formed and company is enjoyed. 14 However, in institutionalized dementia care settings, the creation of a social community can be difficult. 15 As disorientation and uncertainty regarding places and/or expectations connected to places are part of the disease, ‘sense of place’ is an important social element in dementia care. 16 In addition, the cognitive-communicative problems associated with dementia further complicate everyday interpersonal interactions; residents must adapt to living in a community, which entails unfamiliar people and new settings. 17 The formation of a social community is even affected by various ethical aspects, including that dementia can affect people’s ability to exercise choice.18,19
If we take into account the social and cognitive vulnerability of DSCU residents, it is essential that good HCP–resident relationships and concern for each particular resident constitute the focus of care in everyday practice. Quality in dementia care is consequently contingent upon HCP’s proximity in place and space. Malone maintains that proximity with patients is the core of care practice that is fundamentally based on interpersonal relationships. 20 There are three types of proximity, which are ‘nested’: physical, narrative and moral. In DSCU, physical proximity is achieved through nearness when HCP engage in bodily contact with patients during care. Narrative proximity is achieved when HCP come to know a patient by hearing and trying to understand the patient’s story. Moral proximity evolves from the development of physical and narrative proximity and emerges when HCP understand and have knowledge of what each unique patient needs and act on each patient’s behalf. 20
Social community in DCU is associated interaction within place (setting) as a site of healthcare delivery. Architectural considerations of common places in the design of DSCU can facilitate social interaction and thereby enhance social community.21,22 Although the physical setting of DSCU can play an influential role in enhancing social community, it is necessary to understand the significance of the relational components of the social community formed during care. Researchers have highlighted the great complexity inherent in studying the relationships and social communities that people with dementia experience.14,15,18,19,23,24 However, previous research in nursing homes does not provide useful argumentation of how HCP actively deal with the social situations they encounter as part of their work. 25 As the enhancing of social community has not been investigated to the extent desired, additional research is needed to understand how sustaining relationships between HCP and residents can enhance social community in common spaces in DSCU.
Aim
The aim of this study was to explore HCP’s experiences of sustaining relationships and enhancing social community in common spaces in DSCU.
Method
Setting, participants and data collection
This present study has a qualitative descriptive design and its focus on social community derives from a research project concerning psychosocial care in DSCU conducted in a long-term care institution outside a city center in southeast Norway during autumn 2008. 26 The physical environment of the institution was designed specifically for people with dementia, and the institution sought to ensure specialized expertise in caring for dementia patients through competence-raising measures for its HCP over the course of several years. The institution had two sections that together provided long-term care to 28 residents.
In this present study, a focus-group method of data collection was used. The data consisted of four focus-group interviews with 15 HCP. Participants were recruited via the managers of the institution, and inclusion criteria included direct, physical contact with residents and interest in discussing HCP–resident relationships. The participants, all women with 3–30 years of work experience, were divided into two groups consisting of six and nine participants. The interviews lasted two hours, were carried out at the workplace and were tape-recorded and transcribed verbatim. Each group was interviewed twice as multistage focus-group interviews are characterized by a depth exploration of the same subject in more than one meeting, as proposed by Hummelvoll. 27 The interviews were based on a thematically organized interview guide. The study themes were related to how HCP described their relationships with residents, how the institution’s organization of care supported the formation of relationships and how HCP realized the sustaining of relationships and the enhancing of social community. During all interviews, two moderators were present. The lead moderator led the interview and ensured that participants’ experiences were elicited. The assistant moderator recorded observations and contributed to clarification when the lead moderator’s follow-up questions were unclear. Focus-groups interviews were chosen since data collection is improved when participants share similar experiences. 28
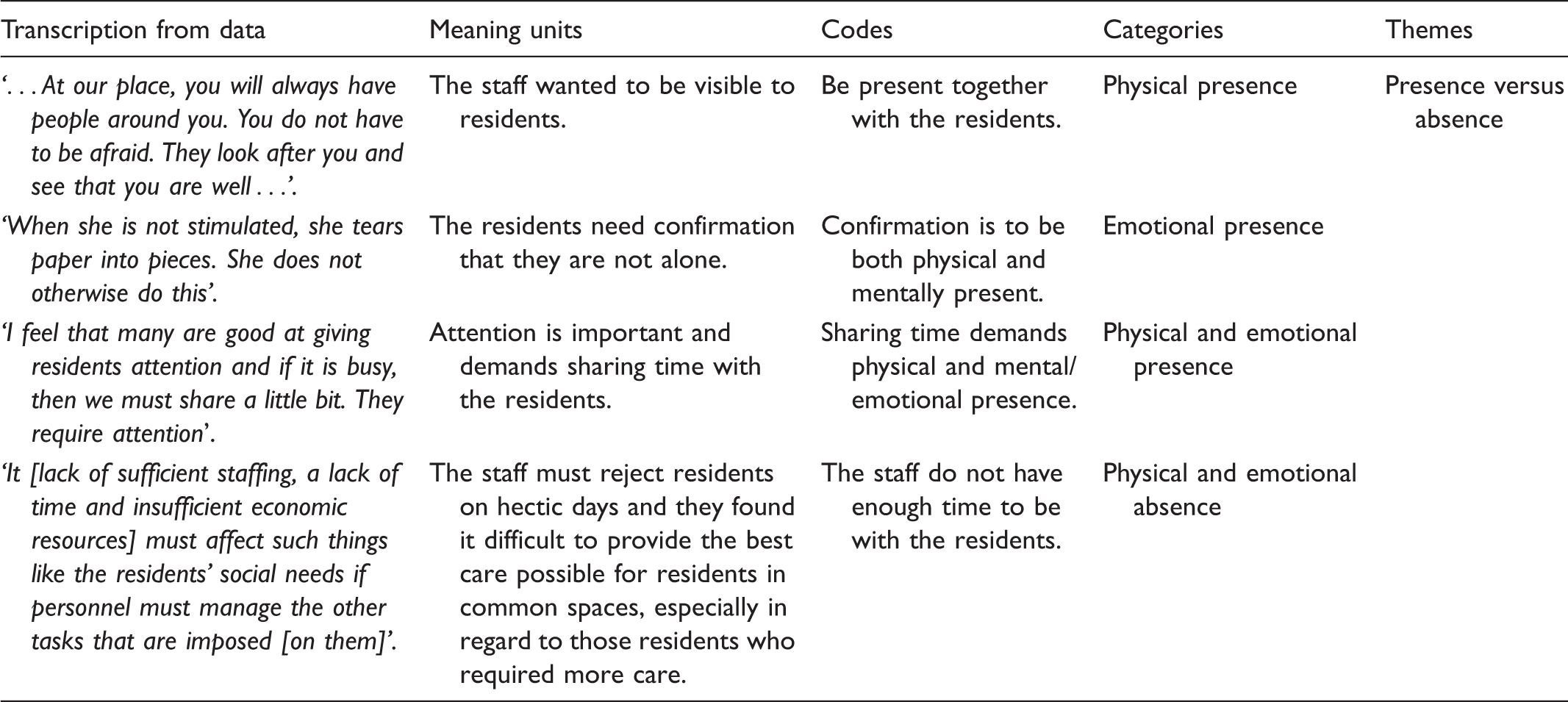
Data analysis
Examples from the data-analysis process.
Ethical considerations
The study was submitted to the Regional Committee for Medical and Health Research, South East, for consideration (reference no. 6.2008.1212). Informants received written and oral information about the background and the purpose of the study. Informants were also informed via a written document as well as verbally that participation was voluntary and that they could at any time withdraw from the study without giving a reason and without consequences for the participants. 30 All informants gave written consent to participate in the study.
Findings
HCP’s experiences of enhancing social community in common spaces were related to three main themes, expressed as dilemmas between knowing versus not knowing each other, safety versus unsafety and presence versus absence.
Knowing versus not knowing each other
Knowing each other was a process of sustaining relationships with the residents in common spaces. According to the participants, it was important that HCP and residents knew each other and that communication between HCP, residents and residents’ families promoted continuity and familiarity. Given that residents’ language and understanding gradually deteriorated as the dementia disease progressed, it was important for HCP to maintain a continuous relationship with each individual resident in order to observe and understand each resident’s personal needs at any time. When the HCP knew the residents well, they were able to understand the residents’ nonverbal expressions: ‘[the residents’] facial expressions can certainly also say quite a lot then … expression … We know each other so well that we can interpret it in many other nonverbal ways: we can, to be sure, do that, all the time’. Such familiarity resulted in HCP’s sensitivity to residents’ needs and wants, which was also important for residents’ dignity: ‘I think it has to do with their dignity, that you meet them. Like with Gerd … it will save the day’.
It was also important for HCP to know the residents’ personal histories and be familiar with their preferences and social and family circumstances. Such information was gathered and retained in a separate document, thereby supporting HCP in offering individualized care: You have to know a little of the pre-history, who they were before. Yes, because we only see the shadow of a life, don’t we? We have to really think about that: who they really are, who we are relating to … reading the case history file, keeping oneself updated, talking with each other. The case history file is also something that remains lying in the drawer.
The participants noted that the continuous exchange of oral information between HCP about residents was equally important with regard to sustaining relationships and enhancing social community. Such exchanges primarily occurred through daily oral reports between the HCP about the residents’ daily conditions. These narratives contained important knowledge and helped the HCP get to know the residents and become familiar with them. ‘We start in room 1 and go through each patient nice and quietly and say what we have done today: how he/she has [been]. It does not take long and it is very valuable. This results in more continuity’.
Still, the participants mentioned that the institution’s management asked the HCP to cease relaying information in oral form and instead to submit written reports, which was presented as a timesaving measure. A tension existed between the written information that was required and found in the standard electronic documentation and the oral information passed between the HCP. According to the participants, the written reports required the use of a more structured language, while the oral reports favored by HCP contained useful information considered impossible to convey in writing. The HCP’s use of oral narrative helped create continuity in HCP–resident relationships, thereby contributing to sustaining relationships and enhancing social community. Moreover, the participants related that they were uncertain what they should include in a written report: We have been told that we should not write ‘Today her daughter visited her’. But this can be quite important for something can have happened when the daughter was there or else something else with them. It is also such things that you convey orally.
Safety versus unsafety
According to the participants, HCP’s ability to maintain security and provide consolation for residents were two of the main factors in sustaining relationships and enhancing social community. Due to residents’ deteriorating memories, it was important that the HCP frequently reminded residents about their situation: Here it is safe and good. Here you always have people around you. Even at night, you do not need to be afraid because we have a night security guard who makes [his] rounds and looks in on you and checks that you are doing well. If you need help, there is always someone here.
The HCP even organized group activities for residents, such as sing-alongs. In general, such activities stimulated social community and provided residents with moments of good experiences. Nonetheless, spending time with others in common rooms could also lead to insecurity and a sense of unease afterwards for residents: They think it is fun to come and [join in] whether it is singing or what it is, but they are awfully tired afterwards and then they easily become confused and uneasy later. I am a little doubtful; it creates a good moment when you take them up with you; they have a good time, but then they become uneasy toward the evening. What is best? What is good for them? There are so many impressions, you know; so much going on. There is so much talking and then we have others who [walk around], don’t they, and then we have someone who is sitting and singing and then it is … Some sing a lot and … not everyone likes it either.
Presence versus absence
The participants related that residents’ sense of security in common spaces was related to the presence of HCP, including the spatial and temporal dimensions of presence. According to the participants, it was during daily routines, such as the provision of personal hygiene, that HCP had the best opportunities to engage residents in one-on-one conversations and establish an emotional connection in the HCP–resident relationship, via dialogue and narratives. The HCP and residents came to know one other through bodily contact, when the HCP attended to the residents’ personal hygiene and so on. In a private room, the residents could be open for meaningful interaction: face-to-face and alone with a familiar HCP. But caring for [someone] is a lot. It is not only washing. It is social initiatives. Some receive care and socialization at the same time. Then care takes longer, doesn’t it?
Health care personnel’s presence allowed them to swiftly alleviate residents’ unease when needed. The participants also described how the presence of HCP in the kitchen or dining room enabled observations of the residents’ various non-verbal expressions and helped the HCP meet residents’ needs. They can show a lot with facial expressions and looks, so we can perhaps understand what they are looking for. They light up when they see others or ‘is no one here?’. If they cannot find the words they can stretch out a hand and want you. Those who can, just walk away: get up and walk away. We do not sit so much because we do not have time for it and because we object to this a little. We do not want to spend so much time on the new PC in the nurses’ station ourselves, although we know that we must and should. We know that they should preferably not have flexi breakfast. They should gather in peace and quiet during mealtimes, but then the time can be almost 11 before breakfast is on the table. There is so much else that we must do before we sit down to breakfast. And it happens that we must ignore them for we should something else or must something else. This occurs all too often. It occurs daily. When she is not stimulated, she tears paper into pieces. She does not otherwise do this … under where she has been sitting there are small pieces of napkin, toilet paper and everything. This does not occur if we speak to her.
Still, the participants noted that the residents were not always given adequate attention, due to insufficient staffing, a lack of time and insufficient economic resources. Even though it was understood that meeting residents’ psychosocial needs was directly related to residents’ well-being, the HCP found it difficult to provide the best care possible for residents in common spaces, especially in regard to those residents who required more care: ‘It must affect such things like the residents’ social needs if personnel must manage the other tasks that are imposed [on them]’.
Discussion
As seen in the findings, HCP’s experiences of enhancing social community in common spaces were expressed as dilemmas. In their efforts to enhance social community, the HCP tried to cope with the dilemmas in line with Malone’s proposal that sustaining relationships in DSCU involves the realization of the different forms of proximity with residents: physical, narrative and moral. 20 Moreover, the findings suggest that HCP’s experiences of enhancing social community in common spaces were related to being bodily present and the possibilities for learning about the residents through their stories and through oral reports between the HCP and to act on the residents’ behalf. The bodily presence of HCP personalized the care being provided, because the HCP and the residents came to know each other and the HCP imbued residents with a sense of security and safeguarded their participation in the community. Due to imposed administrative workloads and a lack of resources, the HCP were required to perform multiple tasks, in addition to caring for residents. This gave rise to dilemmas: knowing versus not knowing each other, safety versus unsafety and the presence versus the absence of HCP – which are in essence ethical questions.
The participants experienced that, because of residents’ spatial disorientation, a need existed to create a proximal space with residents. Increasing disorientation in place and time can lead to disruptions in people’s perceptions of the meaning of a place and, consequently, DSCU can constitute an emotionally challenging place for residents. Such disorientation may cause difficulties with what Örulv describes as ‘placing the place, and placing oneself within it’.16(p.22) Health care personnel’s bodily presence or absence in relation to residents in common areas affected the HCP–resident relationship. The participants experienced that the proximal space included both bodily presence (being there) and availability (being there for). Our findings can also be linked to the findings of Edvardsson, Sandman and Rasmussen, who found that ‘staff presence or absence’ were the most likely social aspects affecting the variations seen in the psychosocial climate and well-being of patients at a dementia unit. 24 In our study, the absence of HCP led to unease among residents while their presence resulted in a good atmosphere and enhanced social community. Bodily presence allowed the HCP to ‘watch over’ residents and ‘know what’s going on’, providing them in turn with opportunities to intervene if misunderstandings arose between the residents and, consequently, safeguard the residents and community from negative events.
The findings from this study showed that the practical realization of enhancing social community is not only dependent on HCP’s physical proximity but also on narrative proximity, i.e. detailed knowledge of the residents’ individualized narratives, which enables the HCP moral proximity. Relational continuity helped the HCP get to know residents, and the participants related that HCP sought to organize their care work so that they and the residents could become close to one another, not only in place and space but also over time. ‘Knowing the person’ is, according to Malone, 20 related to narrative and moral proximity, through which in-depth knowledge of the patient is created and supports HCP’s personal understanding of the residents as a person. In this study, the HCP had the opportunity to be attentive to residents because they knew the residents. The HCP’s familiarity with residents’ histories and preferences was essential for understanding the meaning behind what residents said, and therefore essential to enhancing social community.
We conclude that the HCP’s physical and narrative proximity enhanced social community in common spaces. Malone maintains that a relationship exists between physical, narrative and moral proximity, all of which are interconnected: where physical proximity (presence) and narrative proximity (the sharing of information and narratives) are preconditions for the collective responsibility for patients, i.e. acting and looking out for patients’ interests (moral proximity). 20 As seen in our study, the HCP were able to see what was happening to and between residents and offered professional support by observing residents and providing a sense of security. When forming a community in DSCU, it is important that residents are offered opportunities to participate in the community. 19 Our findings showed that the bodily presence of HCP was significant in regard to residents’ sense of security and also ensured that residents had the opportunity to participate in the community, which can be compared to findings by Helgesen, Larsson and Athlin, 31 who found that the presence of HCP was fundamental to patient participation. Thus, proximity in all its forms is essential if DSCU residents are to become involved in their own daily care.
Shared information and shared knowledge are two fundamental elements of participation in the care relationship.32,33 The study participants described how the DSCU residents, who could not verbally express their needs and wants, shared knowledge and information by expressing themselves through actions. These intentional actions took the form of unique gestures, facial expressions and manners, and thereby demonstrated an evaluative, interpretive manner through which to share knowledge. The residents depended on the bodily presence of HCP in the same space, which enabled the HCP to interpret their movements as being purposeful and meaningful. Bodily presence enabled the HCP to acknowledge the needs and wishes of residents that might otherwise have been undetected, consequently enabling residents to actively contribute to and participate in the care relationship.
However, enhancing social community in common spaces in DSCU was challenging. When physical or narrative proximity was limited, the HCP’s moral proximity was also limited. When such a situation occurred, the HCP were unable to enhance social community. Malone suggested that for moral proximity to endure, it is necessary for HCP to establish a physical nearness to a patient’s body and understanding of the patient’s narrative, if they are to engage with each patient in his/her particularity. 20 The participants were conscious of the collective responsibility they had as HCP to meet residents’ needs, and were critical of care routines that limited their physical or narrative proximity. The institution’s administrative procedures and practices resulted in the absence of HCP in common spaces and limited both their physical and narrative proximity, thereby hindering them in their positions as, ‘hearers and bearers of the residents’ story’.20(p.2321)
Narrative proximity, in the form of a continuous exchange of verbal information on the state or condition of residents, is important when enhancing social community. Narrative proximity occurs when HCP come to know residents, for example by hearing unique stories from residents or residents’ families, or when knowledge about residents is transmitted, in narrative form, to other HCP. The participants in this study related that information was primarily conveyed through oral reports, which provided the HCP with an opportunity for professional communication, including consultation and discussion, and promoted continuity of care. Still, structural changes limited the HCP’s actions. The HCP were required to submit ‘silent reports’ and standard electronic documentation as a timesaving measure instituted by the institution’s management. The participants noted that this not only limited their narrative proximity but also their physical proximity, in that the computers, etc. necessary for the written reports were located separately and away from residents’ common spaces.
According to the participants, the HCP knew what was best for residents but, because of a lack of time or resources, were nonetheless at times required to prioritize or compromise their actions. With many residents to care for, they prioritized building a community in common areas and not ‘one-on-one relationships’ in private rooms. Gathering the residents in common areas provided all residents with the confirmation that they were not alone and that an opportunity existed to participate in their own care. It also allowed the HCP to form a comprehensive view of all residents, which in turn led to an understanding of the residents’ behavior and created possibilities for the HCP to intervene if they saw that residents needed help. By gathering residents together in common spaces, the HCP ensured equal access for all residents to participate in the social community. Still, the HCP’s prioritization of spending time in common spaces – often due to limited resources – was a compromise and limited their abilities to engage in one-on-one relationships. Physically touching and caring for residents in private rooms provided the best conditions for HCP to realize human closeness and emotional connections. Bodily presence created the possibility for private dialogues with residents and, through understanding the residents as unique person, the psychosocial needs of the residents were met. Still, in this study, inadequate staffing limited the ability of HCP to spend time in private rooms, and the HCP organized their work so that physical, narrative and moral proximity was realized in common spaces. However, Brown Wilson found that, in an enriched environment, all relationships must be taken into consideration because they may enhance a care culture and social community. 14
Methodological considerations
Certain aspects need to be reflected on when addressing trustworthiness in qualitative research designs. 29 To strengthen dependability, credibility and transferability, all four focus-group interviews were conducted within four months since repeated data collections show the stability of the data over time and across situations and it was possible to follow the process of analysis. Dependability was strengthened by a critical dialogue among the authors until consensus was achieved. Transferability is also supported by a relevant description of the context and the selections of informants. Since it is known that a hierarchy within a group may affect data, 34 none of the HCP leaders were included in the focus groups. All of the participants were female and this reflects the clinical situation that dementia care in institutions is a female-dominated occupation. Hence, the sample is representative of the professional care providers’ structure of care for persons with dementia. However, different levels of competence among the HCP in the groups may have inhibited the openness of some participants. The participants were colleagues and knew each other which could also limit the nature and amount of data obtained in the study. Still, the selection criteria and research purpose ensured that the reality of the DSCU care environment was reflected. The focus-group discussions provided time for the HCP to reflect on their work and stimulated interaction and encouraged dialogue.
Conclusion
The nature of the cognitive and functional impairments associated with dementia makes it difficult for people with dementia to meet their own needs and, as such, DSCU residents are dependent on others to fulfill their needs. The physical, narrative and moral proximity of HCP are of especial relevance, because the disorientation associated with the dementia disease involves both existential and social dimensions. In this study, mandated structural changes affected HCP’s physical, narrative and moral proximity, limiting them in enhancing social community. The formation of a social community is dependent on the physical, narrative and moral proximity of HCP, and as such, these should not be limited, even if for administrative or economic reasons. Consequently, to gain a more comprehensive understanding of what HCP actually contribute to the care provided in DSCU, the concept of ‘proximity’ in dementia care should be further explored.
Footnotes
Funding
This research received no specific grant from any agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.