
Abstract
Psycho-educational interventions can moderate the negative impact of cancer on patients’ mental wellbeing, although studies of the effect on colorectal cancer (CRC) patients are scarce. Hence, the primary aim of this study was to test whether a nurse-led psycho-educational programme (PEP) could affect the emotional wellbeing of persons being treated for CRC and anal cancer. A secondary aim was to test whether there were any differences in emotional wellbeing in the patients before undergoing a PEP compared to a subset of the Swedish population. A randomized controlled trial was used. In total, 86 patients were randomized either to a PEP comprising seven lectures followed by discussions and reflections with peers or to standard treatment. Mental wellbeing was measured with the Mood Adjective Check List. The PEP significantly (p < 0.04) increased the patients’ overall mood one month after the end of the intervention. The PEP seemed to have a short-term effect on patients’ overall mood. Other outcomes such as self-efficacy could be useful measures when evaluating PEP.
Introduction
Colorectal cancer (CRC) is a commonly diagnosed cancer in both men and women, with an incidence of 1.36 million cases each year worldwide. 1 Both the number of CRC cases in the world and patient survival rates are increasing. 2 The primary treatment for CRC is surgery, with resection of the tumour and sometimes additional adjuvant radio- and chemotherapy. In addition to the resection of the tumour, a stoma can be formed if the rectum is removed or when there is a risk of anastomosis leakage. 3
Anal cancer is a rare form of malignancy with an estimated incidence of between 0.2 and 1.4/100,000 worldwide. 4 In the present study, patients with anal cancer treated with radiation and abdominoperineal resection were included because the treatments were similar to those for rectal cancer.
The treatment and recovery process after treatment for colon or rectal cancer involve many difficulties including physical symptoms such as pain, diarrhoea,5,6, fatigue,6,7 nausea, and sexual dysfunction.6,8 In addition to physical difficulties, cancer patients face existential questions concerning an uncertain future connected to the cancer diagnosis.9–12 Moreover, studies show that patients with CRC experience psychological distress, such as anxiety and depression.13–15 However, some studies have reported that depression in patients with CRC is rare.16,17
Rehabilitation programmes for patients with malignancies and their caregivers have been developed to reduce the negative impact of cancer on emotional wellbeing.18,19 Psycho-educational programmes (PEPs) are common rehabilitation approaches in which groups of patients are provided with information about their cancer as well as with an opportunity to discuss their experiences with others in a similar situation.
After participating in PEPs, cancer patients have reported lower levels of anxiety20,21 and depression. 21 The groups have also been described as creating a sense of belonging to a ‘new family’, of closeness and understanding with people who have had similar experiences. 22 According to Edelman’s review, patients benefit more from psycho-educational groups than groups with only a support function. 23 Nevertheless, because of methodological considerations, reviews have conclud ed that there is a lack of strong evidence for the efficacy of psycho-social interventions for patients with cancer.21,23,24 To our knowledge, no one has tested the effect of a PEP on the mood of patients with CRC. Hence, the primary aim of this study was to test whether a nurse-led PEP could affect the emotional wellbeing of persons being treated for CRC and anal cancer. A secondary aim was to test whether there were any differences in emotional wellbeing in the patients before undergoing a PEP compared to a subset of the Swedish population (Swedish norm).
Methods
Study design
This was a prospective, longitudinal, randomized controlled study testing the effects of a PEP on the wellbeing of patients with CRC and anal cancer.
Participant selection and care
Participants were recruited from a surgical clinic at a university hospital in the middle of Sweden during 2007 and 2010. Persons treated surgically for anal or colorectal cancer with an expected survival of more than two years (evaluated by a colorectal surgeon) were invited to participate in this study. To identify eligible patients, surgical code numbers were examined from the medical records.
A total of 196 patients were eligible and 105 consented to participate in this study, although only 86 returned the baseline assessment (Figure 1). Patients were invited to participate in the study either by personal meeting at the hospital, a telephone call at the time of their discharge from the hospital after surgical resection, or at a return visit one month after discharge. Exclusion criteria included those with difficulties to communicate in Swedish, those with known addiction problems, and persons with recurrent CRC. Some patients had previously met the first author as a nurse at the ward. To avoid having patients feeling obliged to participate, they were encouraged to read the information at home and to return the letter of consent as well as the questionnaires by mail if they agreed to be included in the study.
Psycho-educational programme study.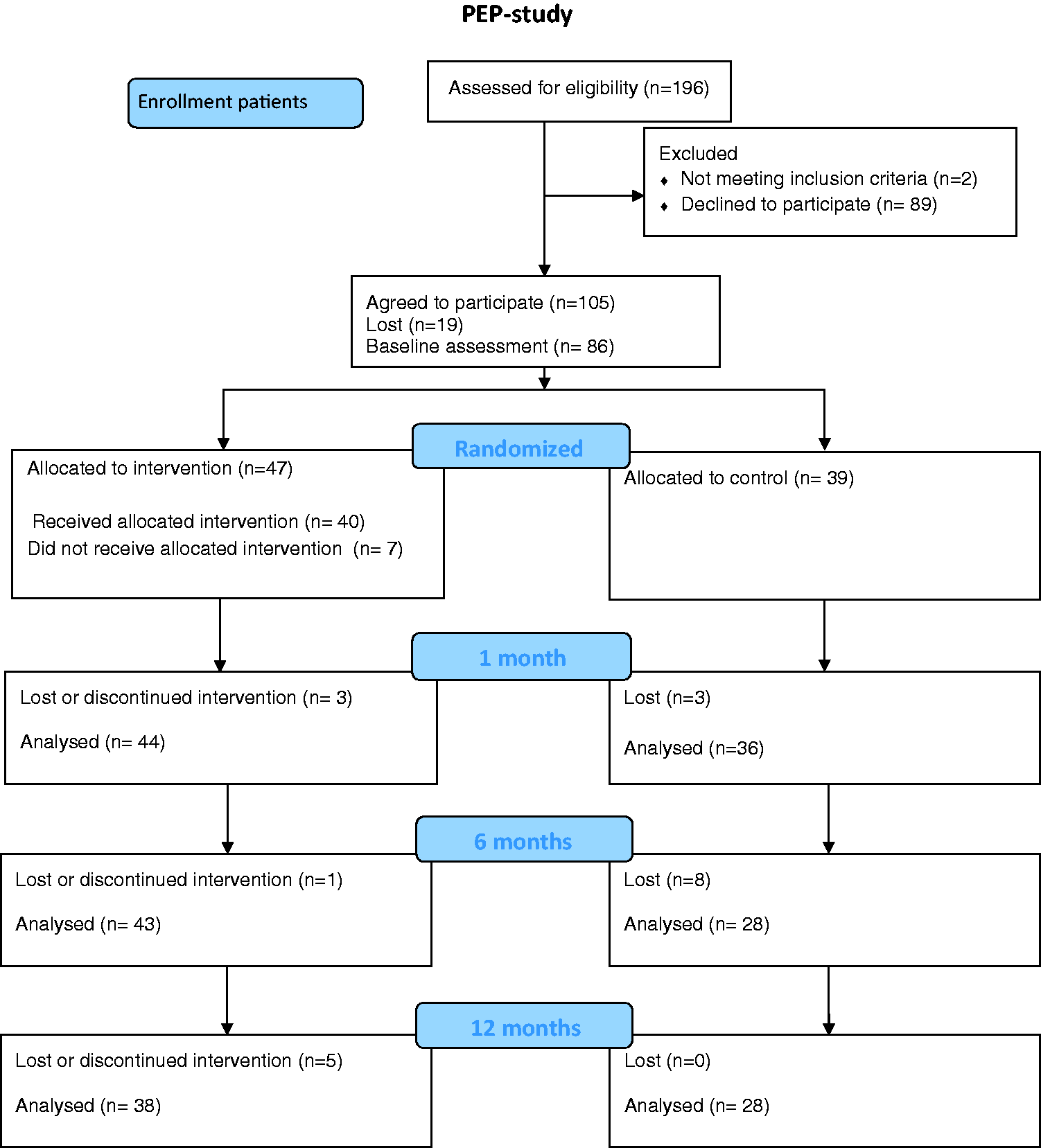
Randomization
Patients were randomized in blocks of 20 patients to either the intervention group (PEP group, n = 10) or to the control group (n = 10). The groups were assigned by drawing blank envelopes containing patient codes. This randomization was performed two weeks before the PEP started and the baseline scores were collected before randomization of the block. A total of five programmes were provided over 2.5 years. A total of 47 patients were randomized to the PEP group. The attendance rate varied between 11 patients who attended all meetings, and seven patients who attended none (Figure 2). Patients in the control group received standard treatment and care. This care included one phone call from a nurse on the third day after surgery if the patient had returned home, and a return visit to the surgeon after one month. A hospital social worker introduced herself to all patients with a cancer diagnosis. If the patients wanted to, they could make appointments for a session. The participants in the control group were offered a place in a PEP group after the end of the study.
Attendance rates.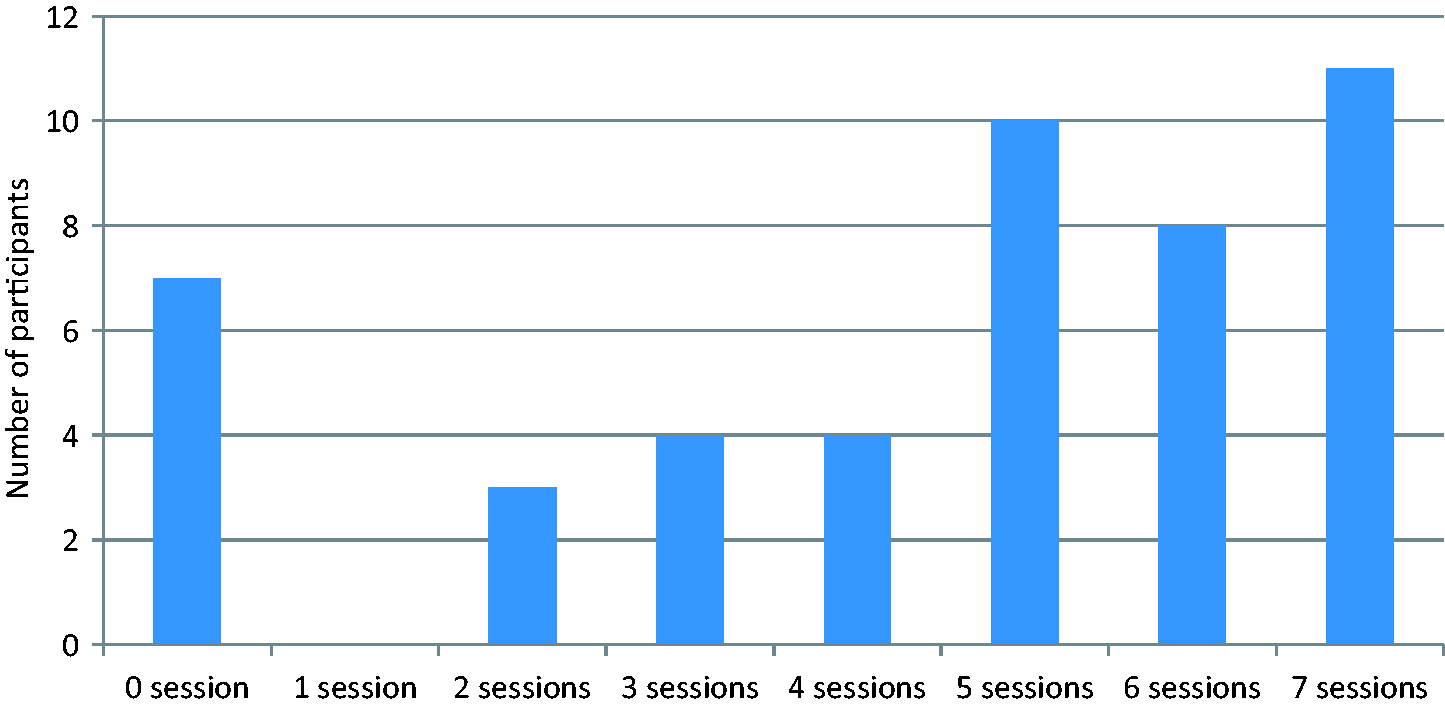
Intervention
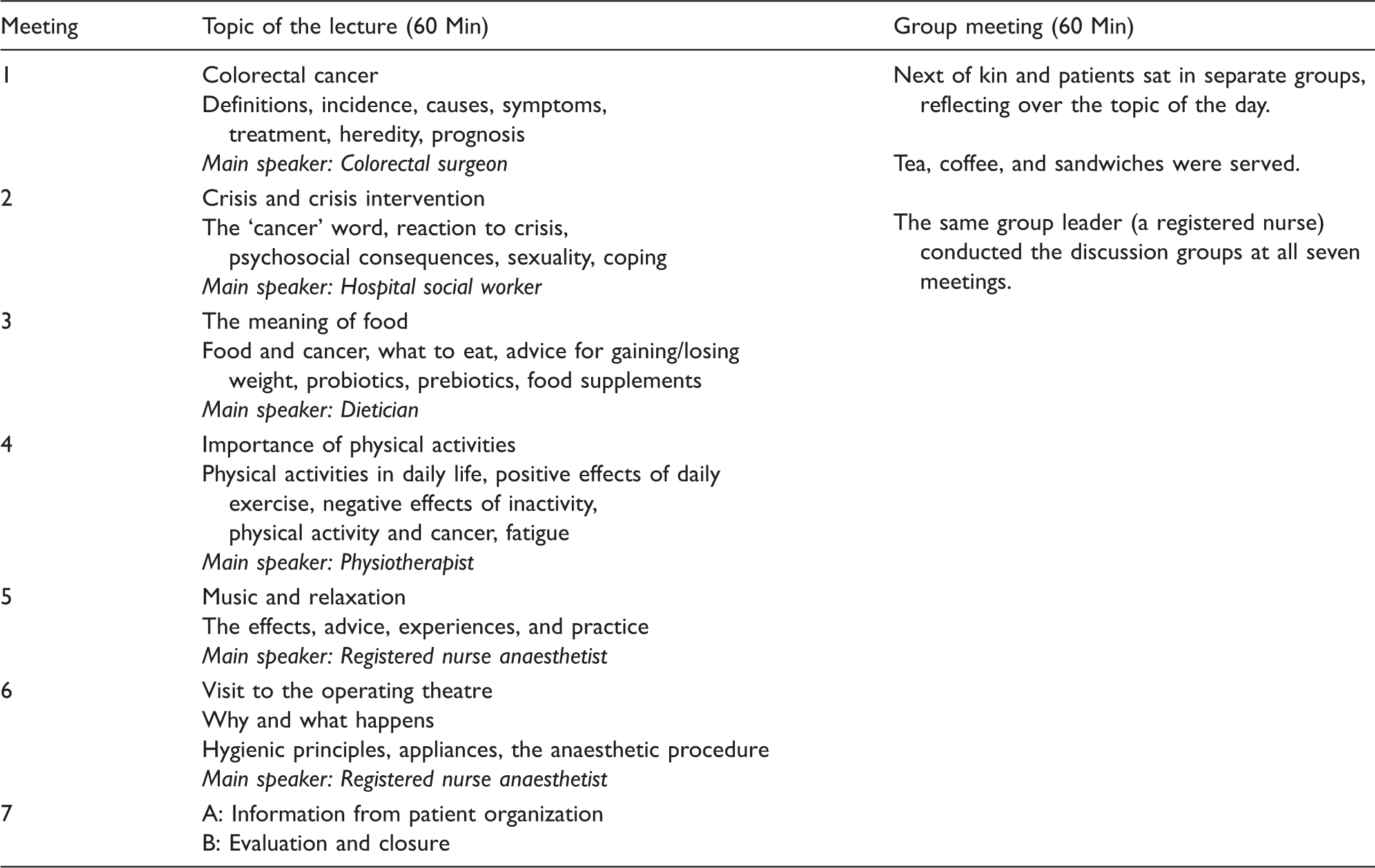
Structure and content of the psycho-educational programme.
Outcome measures
Mood was measured with the Mood Adjective Check List (MACL), 29 a self-assessment instrument comprising 38 items measuring three dimensions of mood: pleasantness (e.g. satisfied, optimistic/depressed, resigned), activation (e.g. alert, active/passive, apathetic), and calmness (e.g. relaxed/tense, distressed). In each dimension, the scores range from 1 to 4, with higher scores indicating a more positive emotional state. A summary score of three dimensions, the overall mood score, was calculated.
The Swedish normal means have been estimated to be 3.17 for overall mood, 30 3.21 for activation, 3.05 for calmness, and 3.25 for pleasantness. 31 The instrument has been found to be valid in several groups of patients as well as in the general population. 29 In the present study, Chronbach’s α for overall mood was 0.94.
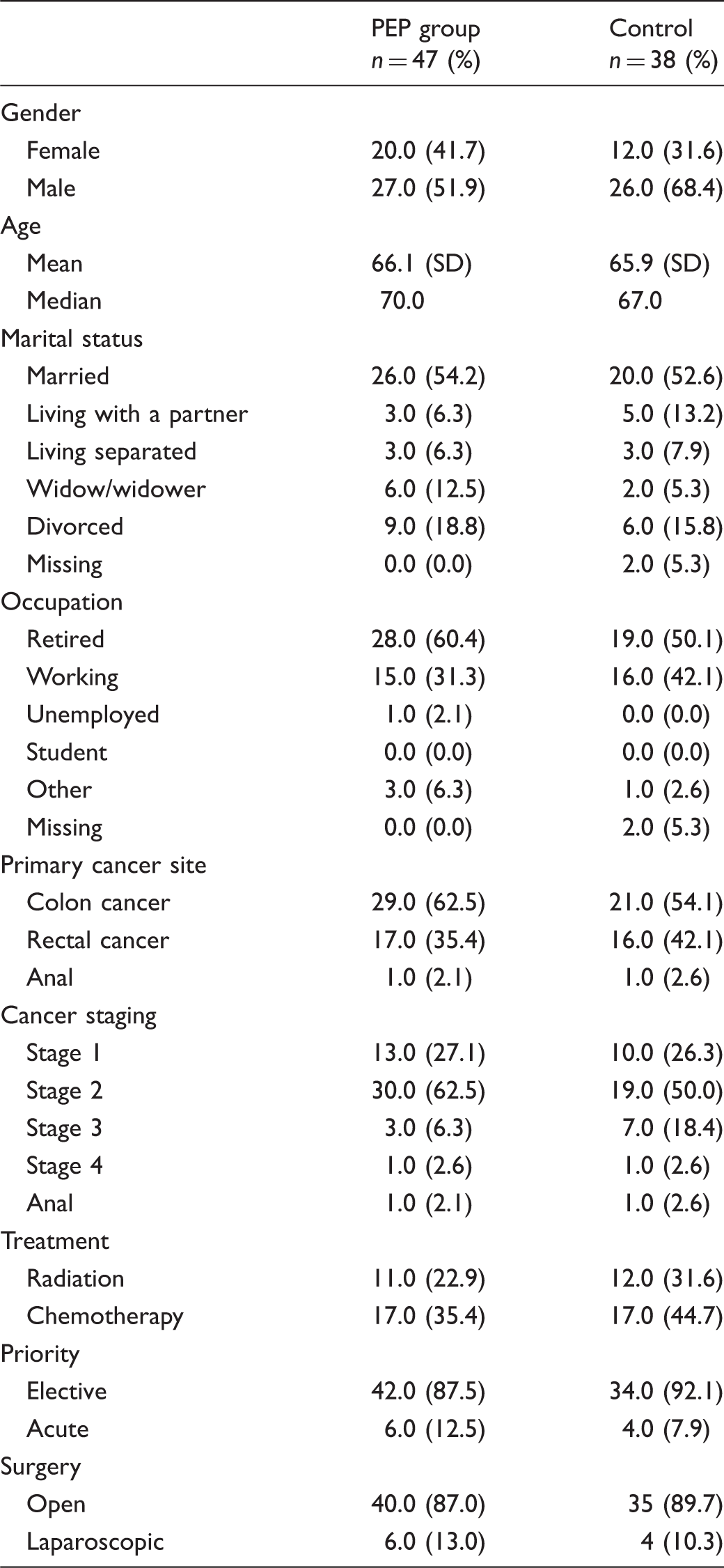
Demographics including age, gender, marital status, and occupation were obtained from a standardized self-reported questionnaire (Table 2). Cancer stage, cancer site, stoma, and type of surgery, radiation, or chemotherapy were obtained from medical records. Demographic data were collected at recruitment, and baseline measurements were collected before randomization.
Data collection
The questionnaires were distributed by postal mail with a prepaid envelope attached one month after the patient was discharged from the surgical ward and again one, six and 12 months after the end of the PEP. Each individual was instructed to complete the form alone. If the instruments were not returned within two weeks, a reminder letter was mailed, which included another questionnaire and another prepaid envelope.
Statistical analysis
The statistical analyses were performed using SPSS version 17. Reported p-values are two-tailed, and p < 0.05 was considered to be statistically significant. A descriptive analysis was performed to assess the characteristics of the study population. The mean value and standard deviation (SD) of the MACL scales and summary scores are presented to facilitate comparison with other studies; however, the statistical testing was based on rank. Significant differences between groups in overall mood, activation, calmness, and pleasantness were tested using the non-parametric Mann–Witney U-test. Within-group changes from baseline were measured at one, six and 12 months after the intervention, and significance was tested using the Wilcoxon signed-rank test.
The magnitudes of between-group differences were analysed by calculating effect size (ES). We calculated differences in ES between the PEP group and the control group by taking the difference between the mean group scores and dividing by the pooled SD. The standardized response mean (SRM) was used to estimate changes within a group. The SRM was calculated as the mean change between two assessments divided by the SD of the change. We interpreted ES magnitudes with Cohen’s ES index (small ES = 0. 2 to < 0. 5, moderate ES = 0.5 to < 0.8, and large ES = > 0.8). 32 A univariate analysis of variance was used to test whether marital status or gender had an effect on the MACL scales (activation, calmness and pleasantness) and the summary score overall mood. The results from the groups were analysed according to their randomization regardless of whether they actually received the allocated intervention. 33 Missing values were imputed according to the principle of ‘last observation carried forward’. 34 P-values for significant differences are reported in the results section; however, if the ES indicated a small, medium, or large effect, non-significant p-values are reported as well.
Ethical approval
This study was approved by the Regional Ethical Review Board of Uppsala (2007/010). Oral and written information about the study and the ability to withdraw from the study at any time were given to those who took part. Written informed consent was obtained from all participants.
Results
Participant description at baseline
Patients’ characteristics at one month after resection surgery.
Effect of the psycho-educational programme on overall mood
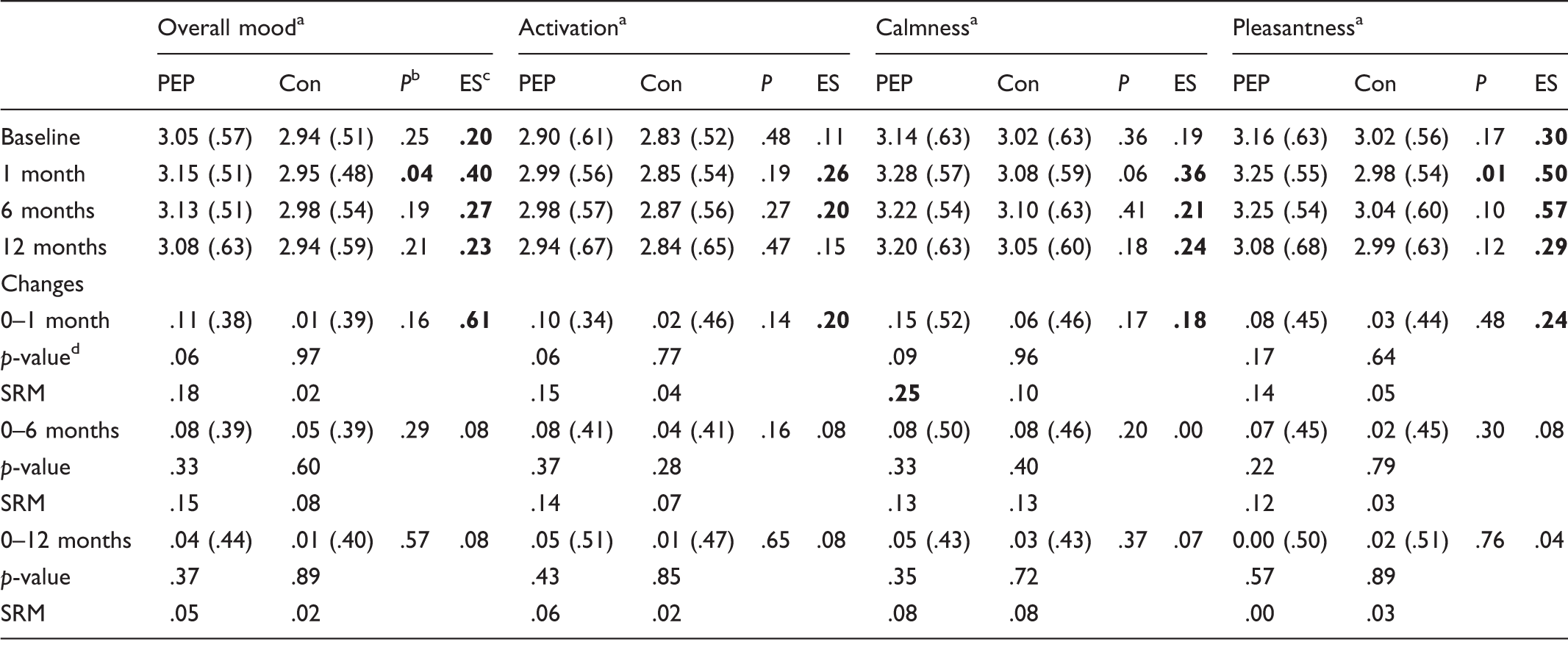
Abbreviations: MACL = Mood Adjective Check List; ES = effect size; SRM = Standardized Response Mean.
Values (except p-values and SRM) represent the mean (SD) score. Bold numbers indicate a significant difference or ES ≤ 0.2.
Scales had a range of 0–5. Higher scores indicated better mood.
Test of between-group differences (Mann–Whitney U-test).
ES (Cohen’s effect size index: 0. 2 to <0. 5 = small, 0.5 to <0.8 = moderate, and >0.8 = large effect).
Test of within-group change from baseline to follow-up (Wilcoxon signed-rank test).
Effect of the psycho-educational programme on activation
There were no significant differences between the PEP group and the control group in the dimension activation when comparing changes over time or in the standard response mean (Table 3). A small ES between the groups (ES 0.26 and ES 0.20, respectively) was noticed after one and six months as well as in changes over time after one month (ES 0.20).
Effect of the psycho-educational programme on calmness
There were no significant differences between the PEP group and the control group in the dimension calmness or in changes over time (Table 3). The ES indicated a small effect of the PEP after one (ES 0.36), six (ES 0.21) and 12 (ES 0.24) months. A small change over time was indicated by the SRM of 0.25 within the PEP group after one month.
Effect of the psycho-educational programme on pleasantness
The PEP group reported significantly higher pleasantness (p < 0.01) (ES 0.50) compared with the control group one month after the end of the programme (Table 3). However, no differences were found after six or 12 months and there were no changes over time in any of the follow-ups. After six months, the ES indicated a difference of moderate magnitude (ES 0.57). After 12 months, there was a difference of a small magnitude (ES 0.29). The ES indicated a small difference in change over time (ES 0.24).
Participants’ mood compared to the Swedish norm
Compared to the Swedish norm values, patients in this study reported significantly lower overall mood (3.17 [SD 0.40] vs 2.99 [SD 0.54]; p < 0.001), activation (3.21 [SD 0.48] vs 2.89 [SD 0.56]; p < 0.001), and pleasantness (3.25 [SD 0.53] vs 3.09 [SD 0.60]; p < 0.01) at baseline.
Discussion
The CRC patients in this study reported significantly lower overall mood, activation and pleasantness than the Swedish norm. The PEP seemed to have some effect demonstrated by higher scores for overall mood and pleasantness one month after the end of the programme. However, these effects were not seen after six or 12 months. The higher scores for overall mood after one month is of importance, since it is known that the quality of life of this group decreases during the first months after the surgery.35,36 The modest results of this study can be further explained by the phenomenon of selective reporting and response shift. 32 Cancer patients tend to ignore or discount problems they believe are unrelated to their illness (selective reporting). 32 Response shift is a change in the self-evaluation of the quality of life where a recalibration and/or reprioritization occurs because of an adjustment to long-lasting symptoms/problems. 37 It is not possible to state definitely why the intervention did not significantly improve the mood at the later follow-ups; however, 15% of patients (7 of 48) allocated to the PEP group did not attend any of the meetings. An indication of differences between the groups can be seen by the ES, although with a larger attendance rate this might have resulted in a significant statistical difference as well. There are no clear limits for clinical importance in measurements of quality of life because it differs depending on the type and stage of the disease. 38 A 0.5 difference on a seven-point scale has been found to be of clinical importance in several diagnoses. 32 With a narrower scale such as the MACL, perhaps a smaller difference may be of clinical importance, which would indicate that the present result is of clinical importance.
The programme
The content of the PEP was consistent with the concerns of cancer patients and their need for information as described previously.39–41 Learning more about colorectal cancer and the latest news about food and cancer might be educational, but would be unlikely to elevate a patient’s low mood. The lecture on crisis and crisis intervention can provide an understanding of one’s own as well as one’s family members’ reactions, although the mood-elevating effect might also be limited. The lectures on physical activity and music and relaxation might have been more targeted and may have eventually affected the mood of the patients, although the ‘dose’ might have been insufficient. Ease of access to information through the internet might alter the need for disease-related information, although internet access does not guarantee that patients will be able to ask professionals questions in real life in the way that the PEP participants were given the chance to do. The PEP offers information on several topics as well as an opportunity to think about, discuss and compare experiences with others in real life and in the presence of experienced professionals such as nurses and the invited lecturers. These interactions with others might encourage patients to discuss the difficult existential questions that individuals treated for CRC may struggle with. 11 The second part of each meeting where the patients reflected over the topic of the day and related their own experiences were expected to have a peer-supportive function that might be the main explanation for the elevated mood at the first one-month follow-up. Since the patient’s caregiver could attend the meetings, this could have had an impact on the result. The PEP became a social event with the possibility of finding a new sense of belonging and understanding. 42 Perhaps this contributed to experiences of higher mood for patients.
Anal cancer
Two patients with anal cancer were included in this study, one in each group. These patients were included because their treatments were similar to those of patients with lower rectal cancer tumours; i.e. radiation and abdominoperineal resection of the rectum. In most aspects, the patients with anal and rectal cancer are more similar to each other than patients with colon cancer are to those with rectal cancer. The programme seemed suitable for the anal cancer patients because the lectures did not focus on any specific cancers except for the first lecture which was given by an experience colorectal surgeon. However, the surgeon also had knowledge about anal cancer and answered questions regardless of the type of cancer.
Strength and limitation of this study
The strength of the study is the randomized controlled study design that enabled an evaluation of the PEP. A limitation of the study is the small sample size, which weakens the statistical power and increases the risk of a type II error. 43 We did, however, reduce the risk of type II errors by calculating the ES and the SRM, methods that are not as sensitive to the sample size for calculating the size of the difference. 44 There was a large individual variation in answer responses, which caused large SDs that would require large groups in order to detect statistically significant differences. Based on the results of the present study, 300 patients would be needed to provide a power of 80%, with a significance level of 0.05 to find differences in overall mood and calmness at the one-month follow-up.
The refusal rate to participate in the study was 43% (n = 89). The reasons given for not participating varied from feeling too old or too ill, not wanting to leave home, or not wanting to think about cancer anymore. The reason for not attending or dropping out might be that individuals did not feel that they would benefit from the intervention. 45 With the perceived difficulties of recovering from surgery and receiving chemotherapy as well as of advanced age, participation in the study could be tiring because it was given during the first year after surgery. Psychosocial rehabilitation/interventions like the PEP have not previously been systematically offered by healthcare services, and might need to be better known to attract these patients. It is possible that the patients who declined participation did not know what they turned down. Using the general Swedish population as the reference group enabled comparison of patients’ mood to that of the Swedish norm and proved that the mood of CRC patients was lower than that of the general population.
Implications and future research
This study addressed patients who were willing to participate in a psycho-educational intervention, and the results cannot be generalized to all patients treated for CRC. The effect of the PEP on overall mood was small and should be confirmed in larger studies. Further studies are needed to confirm whether or not a PEP can reduce unexpected visits or re-admissions to hospitals. Different assessments of outcomes such as self-efficacy or spiritual awareness are needed to further evaluate the effects of PEPs. A revision of the topic of the programme, with fewer lectures and more interactive and flexible content, might be more effective in increasing the mood of patients treated for colorectal cancer.
Conclusion
The PEP seems to have had a short-term effect on patients’ overall mood and pleasantness scores. Other measured outcomes such as self-efficacy might be more targeted when evaluating a PEP.
Footnotes
Funding
The authors received funding from the following sources: Region Örebro Research Committee (Grant/Award Numbers: OLL-140651 and OLL 179131).
Conflict of interest
The authors declare that there is no conflict of interest.