
Abstract
Inner strength is reported as an important resource associated with aging, health, and disease management. The aim was to explore inner strength in people (n = 12) aged 65 years and older, who had experienced a crisis in life associated with a disease. The participants had self-rated their inner strength as high. We found that sources of inner strength were mutual love and support, and the fact that tough times have been managed before. Expressions of inner strength comprised focusing on possibilities instead of brooding, facing and take an active part in care and treatment, and being able to confront reality and pick yourself up again. Inner strength is a complex phenomenon. Increased knowledge of inner strength can serve as an aid in efforts to identify the need to promote inner strength.
Introduction
There is an increased prevalence of diseases in people aged 65 years and older and common diseases include heart disease, stroke, cancer, and depression. 1 Suffering from a serious disease can be experienced as a crisis in life and can involve feelings of anxiety, hopelessness, and despair. Inner strength is reported to be a resource associated with disease management.2–4 Our article reports the findings from narratives from old people who have experienced a crisis in life associated with a disease and who have self-rated their inner strength as high.
Inner strength is a widely used term, and within nursing research Rose was one of the first to describe the phenomenon. 5 She interviewed healthy women about how they experienced inner strength. The findings described expressions of acceptance and belief in themselves, as well as being open, trusting and responsible. The importance of having meaningful relationship with other people, and having the ability to solve problems were also described as interconnected aspects of inner strength. 5 A middle-range theory of inner strength in women was developed where inner strength was defined as having the capacity to build self through a development process. A process that positively moves the person through challenging life events, with the desired outcome ‘living a new normal’.6,7 More recently, a model of inner strength was developed, which was based on a meta-theoretical analysis of the concepts of sense of coherence, resilience, purpose in life, self-transcendence, and hardiness. 8 The model describes inner strength as consisting of four dimensions that vary in their degree of interaction: firmness, creativity, connectedness, and flexibility. In short, having inner strength is described as being open to and being able to perceive the circumstances of one’s life, and having the courage and willingness to deal with challenges and opportunities as well as difficulties and adversities in life. Finding life meaningful and worthy of engagement is an essential part of inner strength. 8
Inner strength has been found to be a resource associated with aging and health. In a study based on interviews from the oldest old, inner strength was described as ‘life goes on-living it all’, meaning that inner strength makes one open to possibilities in life. 9 A study exploring the perception of dignity at the end of the life of older nursing home residents described, as part of the theme ‘inner strength and sense of coherence’, the importance of supportive attitudes from family and staff as a way to strengthen old people. 10 Among older Finland-Swedes living as immigrants in Sweden, experiences of health have been explored. 11 As part of the theme ‘health comes from inner strength and external resources’, personal responsibility for health was mentioned. Being stubborn, having a strong character, and having a positive outlook on life were described as important strengths supporting good health.
Inner strength has also been reported to be an important resource in relation to peoples’ experiences with various diseases. Based on interviews with older critically ill, formerly ventilator-treated patients, factors found to be important for the promotion of inner strength were the presence of and support of their next of kin, and having the will to go on living. 2 Among spouses of patients with heart failure complications after cardiac surgery, inner strength together with security and rest for mind and body was described as an unexpected force that the spouses were surprised to find during the difficult situation. 3 A study exploring health experiences among women with rheumatoid arthritis described inner strength as having courage, independence and control, and also having determination and a ‘don’t quit’ attitude. 4
There are some studies using quantitative approaches to describe inner strength in relation to diseases. A study among the oldest old found low degrees of inner strength (measured using an index of resilience, sense of coherence, purpose in life, and self-transcendence) in relation to heart failure, chronic obstructive pulmonary disorder, osteoporosis, and depression. 12 Based on the previously mentioned model of inner strength, 8 the Inner Strength Scale (ISS) was developed. 13 In studies using the ISS, inner strength was found to mediate in the relation between five common diseases (stroke, cancer, depression, diabetes, and myocardial infarction) and self-rated health among old people, 14 and to be associated with reduced prevalence of depression among older women. 15
It is important to learn more about old people’s inner strength in order to be able to identify and, if needed, promote inner strength among old people affected by disease. By focusing on inner strength in interviews with old people, both men and women, who have scored highly on the ISS despite their experiences of a crisis in life, it might be possible to gain a deeper understanding and broader perspective of inner strength. The aim of the present study was to explore inner strength among old people with high inner strength, who had experienced a crisis in life associated with a disease.
Methods
The study forms part of the GErontological Regional DAtabase (GERDA) Botnia project that was an interdisciplinary joint project between two counties in Sweden and Finland. 16 Extensive data on old people’s living conditions, outlook on life, health, diseases and illnesses were collected with a focus on the dignity, social participation, and health of old people. 17 A qualitative interpretive design was used in the present study.
Participants
Potential participants were persons 65 years of age or older who had participated in the GERDA Botnia project in 2010 by answering and sending in the GERDA questionnaire. Inclusion criteria in this study were that they had answered ‘yes’ to the question had they experienced a crisis in life during the past year and also answered ‘yes’ to the question that asked if the crisis was related to disease. If they had answered ‘yes’ to other causes of the crisis in addition to disease (e.g. death in the family) they were excluded. The second inclusion criterion was that they had scored highly on the ISS that was part of the GERDA questionnaire. The range of possible total scores on the ISS is from 20 to 120, with a higher score denoting a higher degree of inner strength. 13 A population study enrolling participants (n = 6119) from Finland and Sweden found a total mean ISS score of 98.5 (SD = 12.6). 18
Out of 218 persons, in the Swedish sample, who met the inclusion criteria of experiencing a crisis related to disease, the 24 who scored the highest on the ISS were selected. Out of these 24, 12 agreed to participate. This group consisted of seven men and five women between 67 and 82 years of age with total ISS scores of 107 to 120 (Mean = 114.8). They lived in their own house (n = 8) or apartment (n = 4), they were married (n = 8), cohabiting (n = 1), divorced (n = 1), or widowed (n = 2), and a few had home care service (n = 2). Diseases that they suffered from and had experienced as a crisis in life were prostate cancer (n = 3), stroke (n = 3), heart disease (n = 2), lung disease (n = 2), blood disease (n = 1), and neurological disease (n = 1).
Procedure and interviews
Written information with an inquiry about participating in the study through an interview was sent out. Within a week someone from the research team, usually the person who intended to do the interview, made an inquiry by telephone. Four of the study authors performed the interviewing, from September to October 2012. An interview guide was constructed and the opening question ‘Please, tell me about the crisis related to disease that you have experienced during recent years’, was used as a starting point and to provide context for the continuing interview. The following questions were about the interviewee’s thoughts on his/her own inner strength. For example: ‘Do you feel that you have inner strength?’ ‘What is inner strength for you?’ The interviews were performed either in the participant’s home (n = 10) or in the library at the department of nursing (n = 2), and lasted between 30 and 90 minutes (average 45 minutes). The interviews were audio-recorded and transcribed verbatim.
Data analysis
Data were analysed using latent qualitative content analysis. 19 This method is suitable for systematic analysis of interview text. 20 The analysis was performed in several steps and all of the study authors were involved in the analysis process to varying degrees. First, the interviews were read through to get an overall understanding of the content. Second, meaning units that related to the aim of the study were identified and extracted from the text. The meaning units could consist of one or several sentences or a block of text. In the third step, the meaning units were condensed and coded. The meaning units and codes were intended to serve as a tool for the researchers to analyze the text in a more manageable way without missing the context that the codes represented. Fourth, the coded meaning units were sorted into domains, with underlying themes based on the content. Throughout the entire process of analysis, the research team met several times to analyze the findings. The manuscript was also discussed in a seminar with research colleges from other fields to gain consistency in the interpretation.
Ethical considerations
All interviewers were experienced nurses and researchers who were well aware of the effects and consequences an interview can have when the topic is about difficult and painful occasions in the person’s life. Therefore, the interviewers were keen to have a sensitive ear to the person’s reactions during the interview. Before the interviews started, each participant was informed that he or she could abstain from answering questions and stop the interview whenever he or she wanted without giving any reason. The interviews were coded, in order to respect participants’ anonymity and to protect confidentiality of the data. The study was approved by the Regional Ethical Review Board.
Results
Domains and themes.
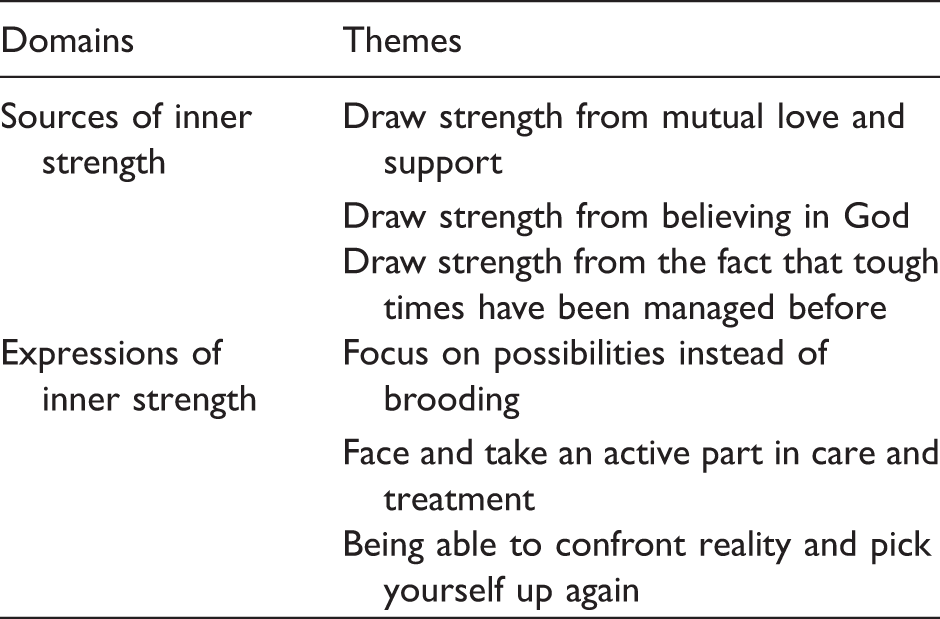
Sources of inner strength
Draw strength from mutual love and support
In the narratives, all of the participants included family such as their spouses and children. Their families seemed to have a significant role in the participants’ inner strength during the disease. Some participants also included close friends in their narratives, as being important to talk to about the worries and anxieties linked to the disease. To experience love and support helped strengthen the participants. Two of the participants expressed this by saying: Strength is when you feel grateful for what you have, that you have a husband, children and grandchildren, which is wonderful. Just the feelings that you still, even in a situation like this, have someone who loves you and that you go on with, then you just have to fight on. When you have people who need you then you really want to keep going.
Draw strength from believing in God
For some of the participants, belief in God was important and had been an essential part of their lives. This was something that provided inner strength during the life crisis they had experienced: I went inside myself and said, ‘God, you have helped me before and you have to help me again because I can’t manage this’, and that has carried me all the way.
Draw strength from the fact that tough times have been managed before
As part of the narratives, the participants described events from their childhood or previous stages of life. It was often a serious life event or a tough time in life that they believed had had bearing on their inner strength today: I have been through things that have made me strong. I think that the upbringing when you were a child means a lot [for developing inner strength], my mother was poor but we never starved. I wrote my diary and that was really good, it has helped me. When I looked back, I felt that things have been even worse than they are now.
Expressions of inner strength
Focus on possibilities instead of brooding
To focus on possibilities and have a positive view of life when struck by disease seemed to be essential elements in the participants’ narratives about inner strength: The ones who give up and think that they can’t do that anymore, or they don’t dare do that, or perhaps think that they will get sick again, they probably don’t feel as well as I did after the last stroke. It [the cancer diagnosis] was nothing I got upset with …I wasn’t. Instead I thought that I would get help with it. I have views on life that you should not dig yourself down, it gets no better. I take the days as they come. I don’t feel sick at all in some way now, although I am not cured. This disease [prostate cancer], I have not been in pain because of it, I have not been sick really. I don’t have any worries and I have no need to be seen as someone other than who I am. There is really not much that I’m afraid of anymore.
Face and take an active part in care and treatment
In the narratives, the participants described themselves as being active in various ways, such as taking an active part in the care and treatment of the disease. To be able to take an active part, the participants said that it was important to be listened to and respected by the health care professionals: I feel that there are a lot of decisions taken over my head, this is the treatment you should have and so on. Finally, I said to the doctor that you must tell me what this is all about and motivate me to do this. My view is that I am responsible for my own body and you are my helper. I had to nag them to get to do a PSA [prostate specific antigen] test, and that process took at least half a year. I myself should do what’s possible for it to go well. I have thought all the time that I will do my best to make something good of my time. I know that it is short, but nevertheless, that it is filled with quality in some way. I go in via the computer and there are a lot of webpages. There is also information to read that I received from the health-care center. The diagnosis [Parkinson’s disease] is not funny when you don’t have any knowledge about it. Knowledge is very important and now I know much more of what it’s all about.
Being able to confront reality and pick yourself up again
In the narratives, the participants gave several examples of how they adjusted their daily lives in various ways to accommodate their disease, e.g. changing their diet, fixing the moped when it was recommended not to drive the car, or always knowing where there was a toilet: Incontinence after radiotherapy affects almost everybody [with prostate cancer], but it’s no worse, it’s surmountable. You just have to know where the toilet is. If it goes, it goes, and if not we have to rethink, quite naturally. I wanted to try to come back. I did go on talking and talking, and of course my wife sometimes got tired when I talked and talked simply to learn it again. Certainly it is a crisis, the whole life. The life is redirected to manage the new situation that you are in, partly by health care and then … because you can’t cope much longer. You have to go down to the bottom and then rise again.
Discussion
The result reflects inner strength among old people, who self-rated their inner strength as high, and had experiences of a crisis in life due to a disease. Both sources and expressions of inner strength were described. A very important source of inner strength, which was found in all of the narratives, was to experience mutual love and support. This can be interpreted as a form of connectedness. As described in the model of inner strength, connectedness concerns feeling engaged with and connected to family and friends as well as society, nature, and the universe. 8 Connectedness seems to be a crucial part of inner strength, and numerous of studies have reported that to feel connected, to share everyday life with someone, to do good things for others, 21 have faith in others 9 and to be able to give and receive support and care 7 are important sources of inner strength. Associations between people’s wellbeing and close relationships and being part of social communities are also shown. In a review, connectedness was found to have positively contributed to quality of life among older people in long-term care. 22 Unsurprisingly, in times of crisis in life, to experience mutual love and support was shown to be central in the narratives about inner strength. A conclusion is that inner strength is strengthened from ‘outside’, i.e. from the participants’ surroundings.
Some of the participants emphasized a belief in God in their narratives, which indicates the importance of considering religion and spirituality in caring for old people. Religion may be seen as part of the broader concept of spirituality, and spirituality does not always involve religion. 23 In a concept analysis of spiritual distress, impairments in seven dimensions of people’s sense of spirituality were described. One of the dimensions of people’s sense of spirituality was ‘inner strength and energy’ that was described as a dynamic, creative, and vital life force that gave hope and motivation. Another dimension was ‘connectedness’ that included connectedness to self, others, nature and the environment, and to God. 24 Our findings give further evidence to the idea that inner strength is influenced by people’s total life situation, as connectedness in terms of both everyday, down-to-earth levels and more spiritual levels is an essential part of people’s lives.
To draw strength from the fact that tough times have been managed before indicated the impact previous life events have had on the participants’ inner strength. This suggests that hard times in childhood and earlier in life had influenced their inner strength today. A study among socially active and healthy elderly women also described how previous events had influenced their inner strength, by enabling them to transform adversities into meaningful experiences. 21 Undoubtedly, previous experiences affect our lives in different ways, however, a question still not fully answered is in what way inner strength influences or is influenced by events in our lives. Longitudinal studies may provide some answer.
The second domain describes expressions of inner strength when struck by a disease. The theme ‘focus on possibilities instead of brooding’ is consistent with some other studies.7,21,25 In a study exploring inner strength in older women with chronic illness the participating women described a focus on what they could accomplish rather than what they could not. 7 A study among socially active elderly women described the importance of carrying out what one has started, and of making the best out of the situation. 21 Positive attitudes toward life that comprised a balance between anxiety and strength was found among old people with multiple comorbidities. 25 A 10-year follow-up study investigated the impact of positive life orientation among old people and found that those who had a positive life orientation had lower mortality rates than the rest of the sample. Those with positive life orientation experienced better health than the rest and one domain that seemed to be essential was the feeling of being needed. 26 Our findings show that having the ability to maintain a positive view of life and trying to benefit from past experiences rather than seeing them as burdens are important aspects of inner strength.
Patients’ desire to participate in decision-making and care is reported in many studies, particularly concerning the patient–physician relationship. In a review study it was concluded that a majority of patients wished to share in the decision-making process and that this group had increased over the years. 27 However, another study found a wide variation in patients’ desire to be involved in medical decisions and suggested that such participation might not be appropriate for all. 28 In interviews among old people with multiple comorbidities the participants aimed at ‘keeping their diseases under control’, meaning that they tended to follow recommendations concerning lifestyle changes and dietary adjustments. Concerning medication, however, they were more critical. They were also in general well informed about their diseases by seeking knowledge from books or the Internet. 25 Creativity, in the model of inner strength concerns the willingness and ability to deal with changes and challenges in life and to see them as opportunities for growth. 8 This was reiterated in our findings, as the participants described the life crisis they had experienced as a challenge. The crisis was not something they had wanted, but their inner strength facilitated their ability to deal with it.
Our findings concerning ‘being able to confront reality and pick yourself up again’ can be related to a study exploring how people with a chronic illness integrated the illness into their daily lives. 29 They described the integration process as a complex and multi-factorial co-existence between ‘living an illness’ and ‘living a life’ where the latter included making adjustments and feelings of self-worth, inner strength, and personal growth. This has similarities to what was described in the theory of inner strength among women. 6 They proposed ‘living a new normal’ as an outcome of inner strength where the new normal is to discover meaning, self-determination, and mastery. The model of selection, optimization, and compensation describes strategies old people use to adapt to life circumstances. 30 Selection focuses on goal-setting and the fact that lack of resources (e.g. time, energy, functional capacity) often necessitates a selection of goals. Optimization describes strategies of using one’s internal and external resources as optimally as possible to achieve the selected goals. Finally, compensation describes strategies for maintaining a goal when loss or decline makes it necessary to compensate for losses in various ways. 30 Both flexibility and creativity as interacting dimensions in the model of inner strength can be related to the ability to adjust in daily life and to find solutions to problems that emerge. Flexibility is about having the ability to resist and endure when life becomes difficult and demanding, and creativity is about the willingness and ability to deal with changes in life conditions. 8 Our findings show that having inner strength is a resource for having the motivation and power to be able to rise up and adjust to the conditions associated with diseases and crises in life. The participants had all experienced a crisis in life associated with a disease. We do not know how they perceived their inner strength before being struck by disease. However, it has been found that inner strength, sometimes surprisingly, can be perceived when people are confronted with harsh life circumstances, e.g. affected by disease. 31 This does not mean that people should not be able to express their vulnerability and sadness, which may also be important in the process of regaining health after a severe crisis in life.
Methodological considerations
There are some limitations to discuss. The interviews were conducted nearly two years after the GERDA questionnaire had been answered. Essential details may have been forgotten during this time, however, in the narratives, it emerged that the participants had clear and vivid memories of their experiences. The self-rated ISS scores were also from the GERDA questionnaire nearly two years before the interview. It may have been of value to know the ISS scores in relation to the interviews among the participants, but we felt it was inappropriate to measure ISS scores on this occasion. This is because, to measure the ISS score before the interview could have affected the interview, and to measure the ISS score after the interview could have affected the ISS score. For this reason we refrained from measuring it. Important to emphasize is that we sought to have an open approach in the interviewing and data analysis, although using the ISS scores as a criterion for selection of the participants. We obtained rich narratives from those who did participate.
Conclusions and implications for practice
Inner strength is a complex phenomenon, and our findings emphasize that sources of inner strength can be found within oneself and in connectedness with others. Expressions of inner strength were shown, in various ways, to facilitate for old people the management their disease. Our findings contribute to increasing the knowledge and understanding of the phenomenon of inner strength among old people with self-rated high inner strength and provide further evidence of the important role it plays in old people’s wellbeing. It has become a subject of growing interest within nursing to give more attention to people’s inner resources. Increased knowledge of the phenomenon of inner strength in old people improves the possibilities of finding proper individual interventions that can support those who are experiencing a crisis in life such as being afflicted by a serious disease. Within clinical practice, it is important to consider old people’s needs to feel connected to family and, therefore, to strive to provide good conditions for connectedness, and not to forget the spiritual aspects of connectedness. Old people’s past experiences and outlook on life and the potential influence it has on their experiences and management of the current situation should be considered. This could be by providing opportunities for the person to express experiences both from the past and from their present situation. Our findings also showed that it is important to consider how much information old people need and want to have regarding their own care, in order to feel that they are able to influence their situation and take an active part in their treatment. To be open and sensitive to old people’s personal thoughts about their abilities to adjust to changed conditions related to being afflicted by a serious disease is an important aspect of enhancing their inner strength and their ability to go forward in life.
Footnotes
Acknowledgments
The authors would like to thank the participants for sharing their experiences with us.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by the European Union and European Regional Development Fund (Dnr 304-9348-2008).