
Abstract
The aim of this observational study was to investigate the occurrence of pressure damage caused by endotracheal tubes (ETT) when the tube is repositioned from one corner of the mouth to the other every third day. For the assessment of oral condition and the eventual damage caused by ETT, a modified version of the Oral Assessment Guide (OAG) was used. The oral condition was assessed once per day in all adult patients who were orally intubated with a tube for over 24 hours. Thirty-eight patients were included in the study. Most patients (n = 33, 86.8%) had no pressure damage. Five patients (13.2%) had pressure damage on the oral mucosa and lip caused by endotracheal tubes. The group with damage to the oral mucosa was treated with noradrenaline, had bleeding problems and clotting disorders and had significantly more intubated and study days. The assessment of the oral mucosa according to the OAG reflected the worsening oral condition in the group with pressure damage. Endotracheal tubes may need to be repositioned more often than every third day to avoid pressure damage in patients with a high risk of complications, and individually tailored care may need to be implemented.
Background
An intensive care unit is a high-tech unit where patients with multi-organ failure are cared for. 1 Patients may need respiratory assistance from a ventilator to maintain breathing and oxygenate the blood. The reasons for requiring ventilator assistance may originate in the brain, spinal cord, neuromuscular system, chest, respiratory tract and/or the lungs.2,3 The first days on the ventilator usually involve oral endotracheal ventilation.
However, the oral endotracheal tube (ETT) can cause harm, which means that there is a balance between benefit and harm. As reported by several authors, pathogenic bacteria may colonize the oral cavity if the mouth becomes dry and the saliva is unable to rinse away debris and plaque,3–5 increasing the risk of bacterial growth in the mouth. Pathogenic bacteria can cause ventilator-associated pneumonia (VAP) after 48 hours of respiratory care6,7 due to manoeuvres such as the sucking up of secretions through the ETT, repositioning of the tube and the patient coughing. These events can lead to the leakage of pathogenic bacteria into the lungs. 8 Other risk factors include pressure damage to the oral mucosa, infections, coagulation abnormalities, dysphagia or tracheal damage.9–15
Pressure ulcers in patients in intensive care are predicted by the following factors: age > 70 years; medical conditions, such as diabetes mellitus, cardiovascular and respiratory failure; treatment with extracorporeal membrane oxygenation (ECMO); pharmacological treatments (e.g. norepinephrine) and the number of days in the intensive care unit (ICU).16–20
The prevention of pressure ulcers caused by the ETT involves several nursing interventions, such as suctioning and oral care, which must be performed on a regular basis. In the literature, the incidence of ulcers caused by the ETT varies between 1.03 and 11.5% in intensive care patients over 18 years of age.9,11,13 One nursing intervention used to prevent pressure ulcers is the repositioning of the tube from one corner of the mouth to the other, an adjustment that can negatively affect the heart rate, blood pressure and respiration.3,15 There is also an impending risk when the position of the ETT is adjusted that the tube does not end up in an optimal position and therefore causes temporary or permanent damage to the vocal cords and lungs.10,15,21
Evidence-based guidelines on how often an ETT should be repositioned from one corner of the mouth to the other is lacking; however, the recommendation in the literature is to reposition the tube from one corner of the mouth to the other every 24 to 48 hours to avoid ulcers.2,3,22 To avoid the negative effects of repositioning without putting patients at risk of developing pressure ulcers from the ETT, the current clinical practice at our clinic is to reposition the ETT every 72 hours if no risk factors are present. Therefore, the aim of this study is to examine the occurrence of pressure damage in the oral cavity caused by endotracheal tubes in which the ETT is repositioned from one corner of the mouth to the other every third day.
Methods
Design and setting
The study was conducted as an observational study of current practice as part of the ongoing quality improvement work in a 12–bed thoracic intensive care unit at a university hospital in Sweden. The unit is primarily for patients in post-operative care after heart surgery.
Sample
All patients ≥ 18 years of age who were on mechanical ventilation and who were orally intubated with an ETT for more than 24 hours were observed. Observations were conducted from 24 February 2014 until 19 July 2014.
Data collection
Observational chart.
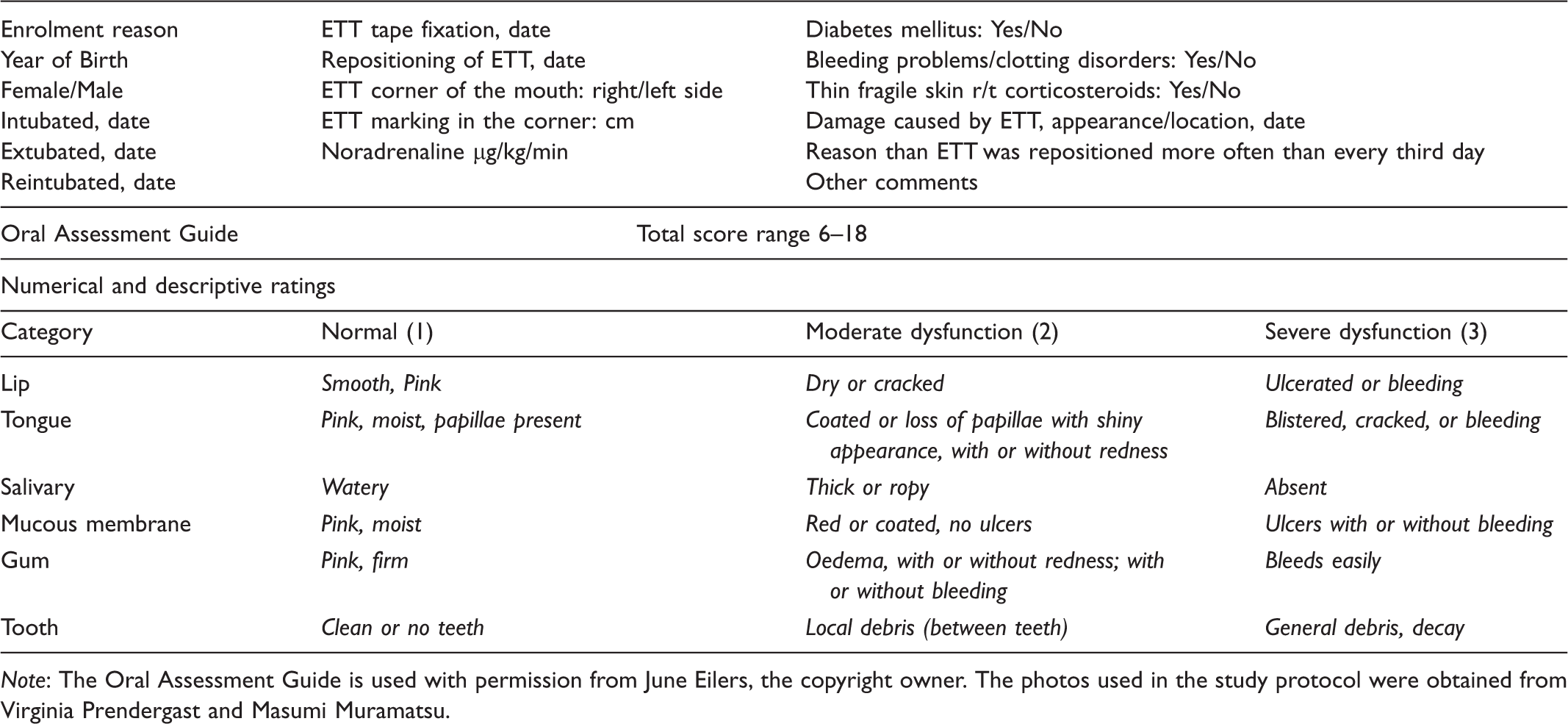
Note: The Oral Assessment Guide is used with permission from June Eilers, the copyright owner. The photos used in the study protocol were obtained from Virginia Prendergast and Masumi Muramatsu.
The OAG assessment instrument and other data
The information in the observational chart is described in Table 1. For the assessment of oral status and the eventual damage caused by ETT, a modified version of the OAG from Barnason et al. 9 for orally intubated intensive care patients was used (inter-rate reliability r = 0.92). As a supplement to the OAG, photos from the BOE (Bedside Oral Exam) and a modified version of the OAG was used to describe the different categories of OAG. 23
Data analysis
The data from the observational chart were manually recorded into Microsoft Excel 2010 and analysed using IBM SPSS statistics for Windows version 22.0 (IBM Corporation, Armonk, NY, USA) and were presented in tables of descriptive statistics (numbers and percentages). The Mann–Whitney U test (Wilcoxon’s rank-sum test) was used for non-parametric analyses, and independent group t-tests were used for parametric analyses. A P-value of < 0.05 was considered to be statistically significant.
Ethical considerations
The study was designed to meet the ethical principles for research described by the 1964 Declaration of Helsinki. The observations did not in any way interfere with the care or treatment of the patient. There was no reference to the patient’s identity in the observational chart in accordance with the Declaration of Helsinki. Approval from the ethics committee was not needed as the observations were part of a quality control of performed care according to Swedish regulations.24,25 Approval to conduct the observations was obtained from the head of the department of cardiothoracic surgery and anaesthesiology.
Results
Repositioning of the ETT and characteristics of the patients
Characteristics of the 38 participating patients with either endotracheal tube damage or no damage.
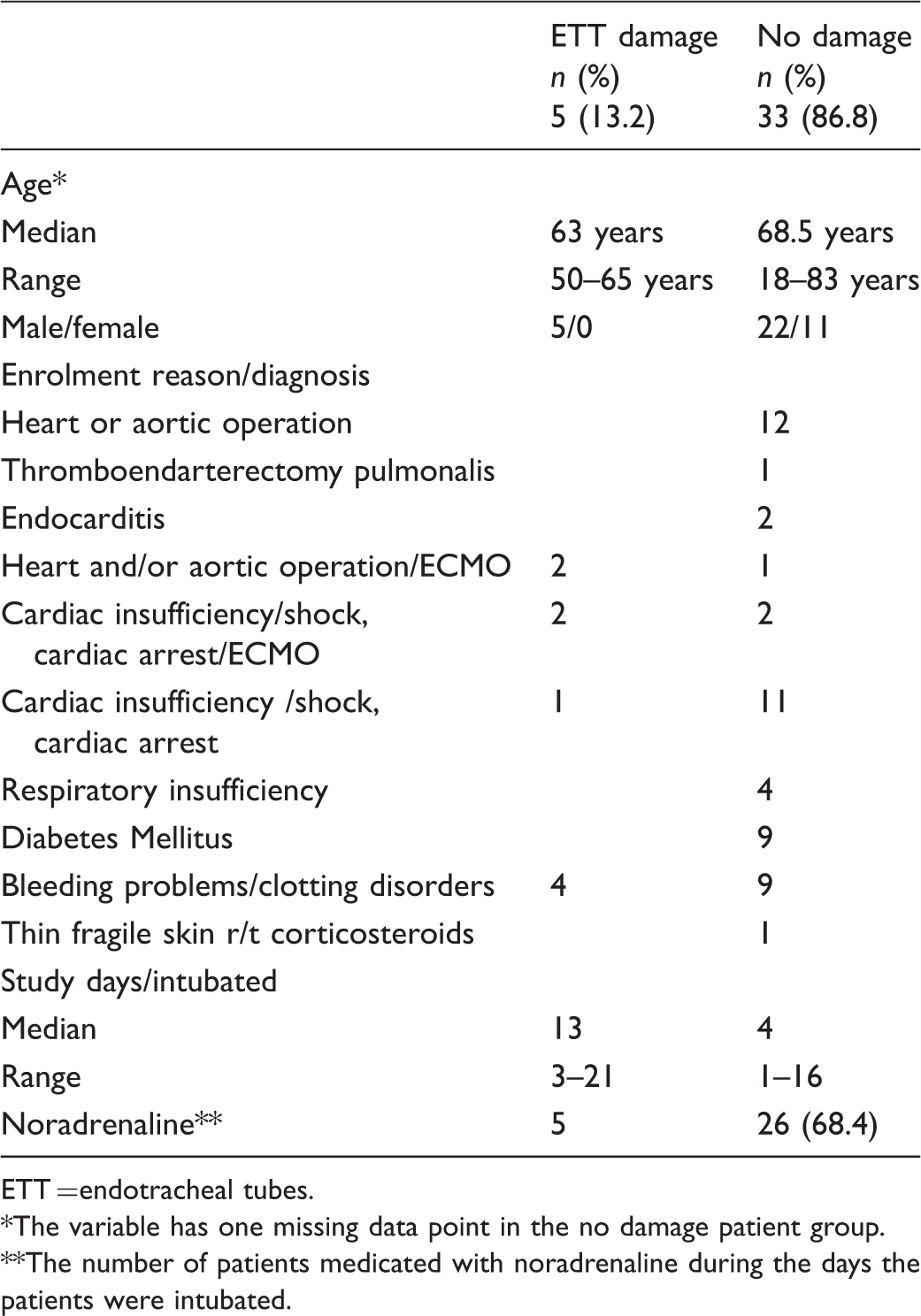
ETT = endotracheal tubes.
The variable has one missing data point in the no damage patient group.
The number of patients medicated with noradrenaline during the days the patients were intubated.
All five patients (13.2%) who developed pressure ulcers were male. In one of the five patients, the damage was caused by an armoured ETT that led to a crush injury to the oral mucosa. One patient with a bleeding disorder was intubated for 21 days. In this patient, the tube was repositioned every third day, and the patient subsequently developed a pressure ulcer. In the other four patients with pressure damage, the ETT was repositioned sometimes more often than every third day due to signs of damage. In one of the four patients, the tube was repositioned for the first time on the fourth day. There was a significant difference (P < 0.001) in ‘study days/intubated’ between patients with ETT-induced damage compared to those with undamaged mucosa. However, the effect in the two groups was not related to age.
The OAG median was higher in patients who sustained damage from the ETT from day 1 (day after intubation) compared to patients without damage (Figure 1). The ETT caused both bleeding and non-bleeding ulcers on the lips and the corners of the mouth during the first week of intubation.
The oral condition of patients (n) from day 1 (≥24 hours) to day 11 according to the median score on the Oral Assessment Guide.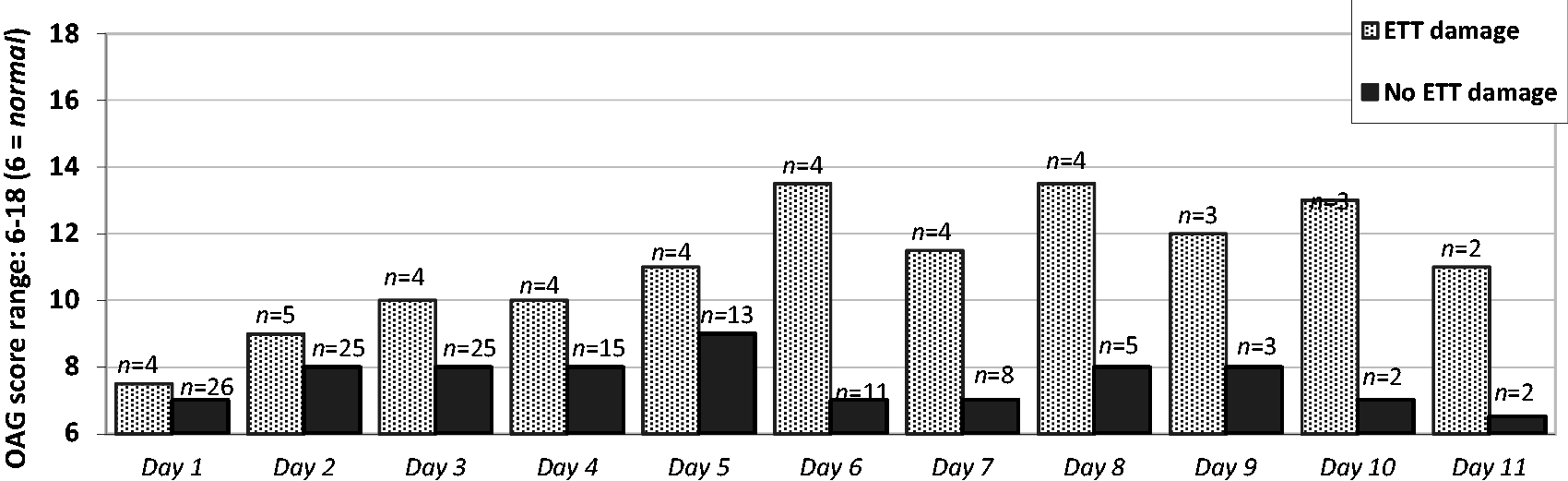
There was a total of 21 days (9.6%) in which OAG assessments were missed, and on the first study day eight assessments were not made.
Discussion
Our results show that there was no sign of a pressure ulcer caused by the ETT in 71% of the 38 patients. Five patients (13.2%) developed pressure ulcers in our study, which is in line with the results from Barnason et al., 9 who showed an 11.5% rate of pressure damage despite the fact that ETTs were repositioned every 12 or 24 hours. However, our rates are considerably higher than the results from Coyer et al. 13 and Black et al., 11 who found ETT damage in 1.03–2.4% of patients. Whether the low incidence of pressure ulcers caused by the ETT was due to differences in the inclusion criteria, the assessment tool or differences in the length of ETT time is not clear and should be investigated further.
One explanation for the differences in the occurrence of pressure damage is the differences in patient characteristics, such as age and comorbidities. In the future, more studies that compare different patient characteristics to the occurrence of pressure damage in relation to the ETT should be considered. General factors that are reported to predict the development of pressure ulcers (i.e. age > 70 years, diabetes mellitus,16–18 or fragile skin 26 were not observed among the patients who developed ETT-induced pressure ulcers.
Among our patients, the damage sustained from the ETT in two out of the five patients can be partly explained by 1) a different type of tube used in one patient (an armoured ETT that caused a crush injury to the oral mucosa) and 2) the repositioning of the ETT four days after intubation in the other patient. In four of the patients, the ETT was sometimes repositioned more often than every third day according to the recommended policy that, when signs of damage are noted, the ETT should be repositioned more frequently.
The results show that significantly more pressure ulcers developed with longer ETT time, which is in line with the results shown by Prendergast et al. 27 Among our patients who were orally intubated for less than three days, the OAG assessment showed no signs of pressure ulcers; therefore, special considerations should be made to improve oral hygiene in patients with longer ETT time. In our study, we observed all patients who were intubated for over 24 hours, as the aim was to investigate the presence of pressure damage. Of the 38 patients included, 32 (84.2%) were intubated for a period of three days or longer. The OAG assessment, along with the option to specify ETT damage in the observational chart, ensured the validity of the study. We occasionally missed OAG assessments (total 21 days = 9.6%), but this was accepted as long as the chart was able to verify any damage.
The number of patients we observed was few, which undermines the statistical validity of the study. However, the results show possible synergistic factors that predispose patients who are seriously ill and who are being treated with ECMO to ETT-induced damage. All of the patients had acute congestive heart failure and/or respiratory failure.16,18–20 The peripheral vasoconstrictor drug norepinephrine may have reduced blood supply to the tissue 17 and increased the risk of not providing enough oxygenated blood (hypoperfusion) to the skin in those treated with ECMO.19,20
The results of our study and the routine of repositioning the ETT every three days can be adopted in other intensive care units. However, routine exceptions must be made to ensure patient safety and avoid damage. The ETT may have to be repositioned more often in patients with bleeding or clotting disorders, those who are treated with ECMO, those who are administered norepinephrine, and those on oral ETT for longer periods of time. Larger studies will need to be conducted in the future to identify new factors and confirm the factors identified in our study.
Conclusion
What is known about this topic
ETT can cause pressure ulcers in the oral mucosa. There is a lack of evidence on how often an ETT should be repositioned. Repositioning of the ETT involves risks. What this paper adds The routine of repositioning the ETT every third day can be adopted in other intensive care units. However, ETT repositioning should not be conducted in all intensive care patients. There is an increased risk of pressure ulcers caused by the ETT in patients with bleeding problems/clotting disorders, and the risk increases with the number of ETT days. An individually-tailored plan of care is needed.
Footnotes
Acknowledgements
We thank the unit’s director of education, Unni Fet, who helped with conducting the study according to plan, which was important for obtaining results. We would also like to thank the first author's colleagues who assessed the oral status and documented the data based on the observational chart. For help with translating the manuscript into English, we would like to thank Dr Gilian Barker.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.