
Abstract
The current study responds to implementation challenges with translating evidence-based knowledge into practice. We explore how appreciative inquiry can be used in in-house learning sessions for nurses to enhance their knowledge in using a guideline on delirium as part of clinical decision making. Through 18 sessions with 3–12 nurses, an appreciative inquiry approach was used. Specialist nurses from the Heart Centre of Copenhagen and senior lecturers from the Department of Nursing at Metropolitan University College facilitated the sessions. Field notes from the sessions were analysed using open and axial coding drawing on the principles of grounded theory. The study shows that appreciative inquiry was meaningful to cardiology nurses in providing them with knowledge of using a guideline on delirium in clinical decision making, the main reasons being a) data on a current patient were included, b) shared learning took place and c) a session about a patient was led by the patient’s nurse.
Introduction
Delirium is a frequently occurring condition in critically ill hospitalized patients,1,2 whereas heart surgical post-operative patients have a prevalence of up to 52%, 3 and the figure is 17% for medical cardiology patients. 4 Delirium is the acute onset of fluctuations in mental functioning, which may have serious consequences such as a greater risk of permanent cognitive dysfunction and increased mortality. 1 The Danish National Clearinghouse in Nursing has developed a clinical guideline containing recommendations for the identification, prevention and treatment of delirium in hospitalized patients. 1
Using clinical guidelines in practice presents a well-known challenge. Translating evidence-based knowledge into practice is difficult. Research shows that there are no clear answers on how to ensure the success of the implementation of clinical guidelines, and that there is a considerable gap between evidence and practice.5–7 A survey of nurses shows that organization, heavy workload, time, education and communication are the main reasons for not using clinical guidelines. 8 Other studies point out that clinicians’ knowledge, motivation, attitudes, lack of support and education, in addition to the condition of patients are possible barriers.9,10 Nurses’ attitudes and motivation regarding the application of clinical guidelines are therefore factors to be taken into account in implementation.
Davies et al. show that an implementation strategy is more likely to lead to success when clinicians are actively involved, and when the strategy is closely related to everyday clinical practice. 11 Competence building is very important for clinicians’ active participation in implementation, and therefore pedagogical and educational strategies for the implementation are essential.12–15 Friedman et al. emphasize the importance of using different teaching and learning methodologies, such as interactive formats, feedback, reminders and reinforcement strategies, and of involving staff in the development of educational programmes on the basis of their training needs. 12 For this reason, educational strategies should include and acknowledge nurses’ attitudes to, and motivation for, the use of clinical guidelines in their daily practice.
Appreciative inquiry (AI) involves participants’ attitudes and motivation by focusing on their resources, aspirations and opportunities in their everyday work with their colleagues. Appreciative inquiry can promote learning and development by focusing on whatever succeeds, as opposed to focusing on problems.16,17 In the healthcare system, AI has been used as a framework in organizational development with regard to quality improvement, as can be seen in Havens, 18 Shendell-Falik et al. 19 and Lazic et al. 20 Trajkovski et al. 21 and Marchionni and Richer 22 emphasize that AI can be used in the development and implementation of evidence-based nursing. There is limited research on how AI can be used in a clinical context as an educational strategy to improve nursing. Yoon et al. show that AI was found to be a useful framework for generating a dialogue among nurses on ways to improve oral care for medical patients at a rehabilitation hospital. 23 Appreciative inquiry can be used as a framework for the implementation and development of evidence-based nursing, but there is a lack of clinical research on nurses’ use of a clinical guideline on delirium in heart patients.
In response to the lack of clinical research, the project Implementation of evidence-based practice: an innovation project between theory and practice was conducted. 24 The project was a partnership between the Department of Nursing at Metropolitan University College (MUC), the Heart Centre of Copenhagen University Hospital and the Centre for Clinical Guidelines. A significant aspect of this implementation project was the use of AI in in-house learning sessions, at two wards with both surgical post-operative and medical cardiology patients, as an educational strategy to enhance cardiology nurses’ clinical decision making (CDM). 25 Here nurses drew on the best available research on the use of a clinical guideline on delirium, integrated with patient preferences and their own expertise. 25 This article will focus on these sessions.
Purpose
The purpose of this article is to explore how the practice of AI improves cardiology nurses’ knowledge in the use of a clinical guideline on delirium as part of CDM.
Methods
Action research 26 is the framework for the intervention, since it focuses on change and development of and in practice, where participants commit themselves to cooperation that creates knowledge. Appreciative inquiry was used as the theoretical framework, with the key concepts of respectful recognition of each other’s thoughts and ideas, exploring topics with open and reflective questions, highlighting successes and the meaningfulness created through working collectively. 16
Those who took part in the intervention were two cardiology nurses with special competencies (NSC), nurses from the Heart Centre and two senior lecturers with qualifications in nursing and education (SL) from the Department of Nursing. At each session, one NSC and one SL participated, together with a varying number of nurses depending on how many were at work on the randomly-selected days of the sessions.
The NSC was the primary facilitator and the SL was the co-facilitator. Appreciative inquiry was used in the facilitation of the sessions: the NSC gave recognition to the nurses’ thoughts and ideas on how the clinical guideline on delirium could be used in CDM, and asked open and reflective questions. The SL was also a participant observer, keeping notes of observations and reflections on the field. 27 The SL took field notes both during and after the sessions. The number of participants, the time frame, the content, the use of AI by both the NSC and nurses, and the interaction during the session were observed and noted down.
The professional content of the sessions was CDM in terms of the clinical guideline on delirium, creating individual care plans focusing on sleep, nutrition and fluid intake, which are important elements in the prevention of delirium, as well as cognitive assessments of patients using the screening tool Brief Confusion Assessment Method (B-CAM).1,28 Both individual care plans and B-CAM are part of the patients’ electronic health record.
Data analysis
An example of a matrix containing concepts, subcategory and main category.
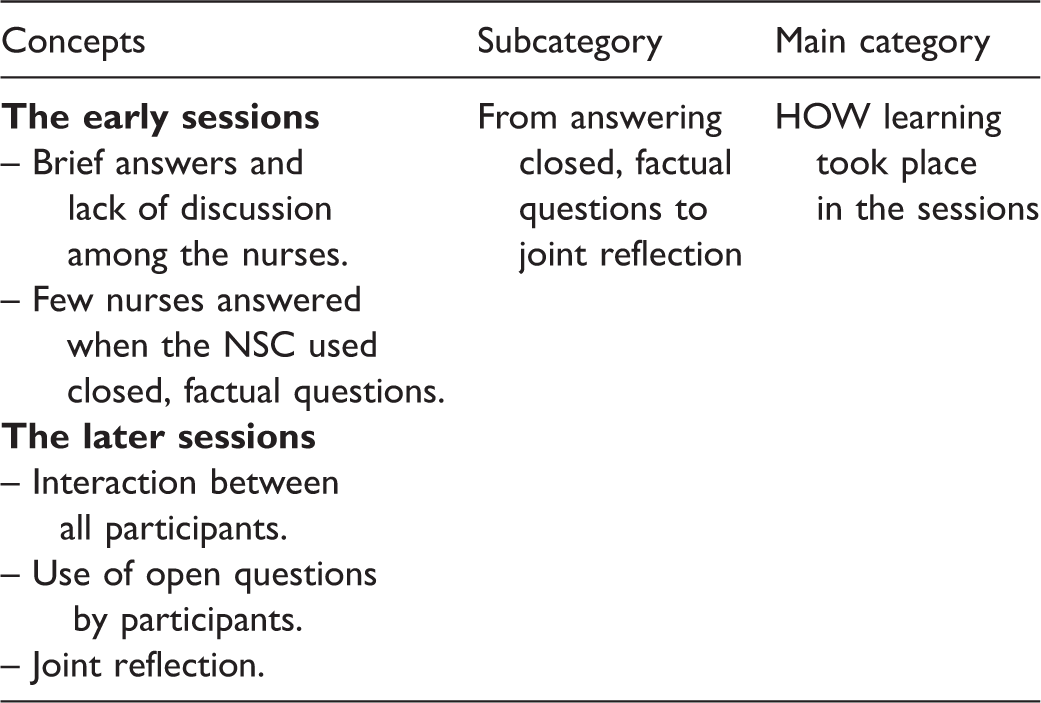
Coding includes choices and is therefore open to interpretation. 32 In the coding process, the analyses of the field notes and interpretations of meaning were first performed individually by two of the authors. This was followed by researcher triangulation, where these two authors and a third separately identified themes, interpretations of the underlying meaning, subthemes and codes. These were finally compared and discussed by the authors until they reached agreement on subcategories and main categories. In this process the three authors were supervised by a trained researcher (the fourth author).
Ethical considerations
The project is not subject to notification to the Danish Data Protection Agency [2015-57-001]. Ethical review by a health research ethics committee is not required for qualitative studies in Denmark. 33 The project is subject to the Metropolitan University College Code of Conduct for Research Integrity, 34 which applies international and national guidelines for responsible research practices.
Nursing staff, NSCs and SLs agreed to participate in the project and were guaranteed anonymity. The quotations used have been adjusted so that the spoken language style, exclamations, etc. are not liable to reveal individual identities. The ethical aspects of a project involving sessions have ensured respect and appreciation for the nurses’ attitudes, knowledge and values.
Findings
For two months, in two non-intensive-care cardiology wards with both surgical post-operative and medical cardiology patients, 18 sessions lasting for 20–90 minutes with 3–12 nurses were held. An NSC facilitated and an SL co-facilitated these sessions using AI.
During the sequence of 18 sessions, the content changed. The first five focused mainly on the introduction and use of B-CAM, the cognitive screening tool for delirium. The following 13 sessions dealt with the enhancement of individual care plans to prevent and treat delirium; the first three of these used data from newly discharged patients, while the final ten dealt with currently admitted patients.
The analysis of the sessions revealed that nurses included the clinical guideline on delirium in CDM when it became meaningful to them. The nurses’ knowledge in using the clinical guideline in delirium in CDM may be expressed in three main categories. Each main category has a subcategory which describes the development through the sessions:
What was the content of the sessions?
‐ From non-practical to practical orientation How did learning take place in the sessions?
‐ From answering closed, factual questions to joint reflection Who took control and ownership of the sessions?
‐ From teacher-led instruction to ownership by the nurse responsible for the patient.
What was the content of the sessions? From non-practical to practical orientation
The first five sessions dealt with the delirium screening tool B-CAM. Here the NSC introduced the screening tool and taught the nurses how to use it. The focus was entirely on the screening tool. The nurses showed little involvement; only a few answered the NSC’s questions, and then only briefly. ‘How often should we screen?’ (NSC) ‘Twice a day’ (nurse). Sometimes the NSC’s questions were met with silence, so she had to answer herself. ‘Why do we screen patients? … To prevent delirium’ (NSC). Although the sessions took place in the cardiology department, no practice-based knowledge of current patients was included. This theoretical approach constrained the possibility of acknowledging nurses’ practice-based knowledge and did not engage them.
The following three sessions were based on how the individual care plan of a discharged patient could be improved. The NSC asked open questions about interventions and suggestions for care using AI, which involved the nurses’ knowledge. The nurses participated eagerly and supplemented each other in the discussion, as the NSC summed up: We must maintain a regular rhythm day and night, shield the patient and remove things that confuse the patient, that is, reduce the stimuli. (a nurse) … yes, and give guidance to relatives so they’re a resource, meaning not that many relatives in the room at the same time. (another nurse) … so concrete nursing care measures that limit the development of delirium. (NSC) According to the clinical guideline, the patient must have a normal circadian rhythm and normal sleep to prevent delirium, but when he’s at home he usually only sleeps for four to five hours, just like now … so what’s the target for his sleep when he’s in hospital? (NSC)
In the course of the 18 sessions, it became clear that the content of the session – what was discussed – had a decisive influence on whether nurses gained knowledge of, and found meaningful, the use of the clinical guideline on delirium in CDM. When the content of the session was far removed from practice, such as the clinical guideline itself or data from the discharged patient, nurses’ knowledge was only recognized to a limited extent and the session did not create the professional commitment necessary for it to be meaningful to nurses to use the delirium guideline in CDM. Conversely, when the content was practice-oriented, based on a current patient, it was recognized that nurses had resources in terms of experience and particular knowledge of the patient, and they were asked challenging reflective questions, which made it meaningful for them to involve the guideline in CDM. This also meant that the NSC changed her role from teacher to facilitator.
How learning took place in the sessions: From answering closed, factual questions to joint reflection
In the first five sessions, the nurses were often taught about the screening tool B-CAM with the use of closed, factual questions. There was no discussion among the nurses and few answered questions. Sometimes the nurses said that it made no sense to use the screening tool. I mean, that stuff [screening], do we really need the same question every time, whether a stone can float in water, eventually they [patients] know it off by heart. You could vary it a bit! … I don’t need these steps [four screening questions], or that form [screening tool], I’ll be skipping it … So basically, I wouldn’t bother with it myself, and my patients would resist it … and that would harm my relationship with them. (nurse)
The final ten sessions were based on current patients. The NSC used a computer projector to allow all the nurses to see, and take part in improving, the individual care plan. The NSC used open-ended questions that reinforced AI to encourage group discussion. ‘When you look at this individual care plan for the patient, there’s something that’s already been described … How can we complete it together?’ (NSC). A nurse stated that the patient had said he was afraid of dying. This gave rise to a keen debate where the nurses and the NSC discussed and challenged various actions, including whether and how nurses could involve relatives in care and offer the patient a permanent care team. This joint reflection culminated in the suggestion of a care approach where nurses use their knowledge of the delirium guideline, previous sessions and their knowledge of the patient, resulting in a jointly agreed and professionally argued enhancement of CDM.
At the end of the sessions, the NSC asked the nurses whether it had been fruitful to discuss individual care plans together. It makes sense to argue back and forth with the others about individual care plans. (a nurse) … I get inspiration from my colleagues’ individual care plans. (another nurse) … and using the projector is a great way for everyone to get together and work together on individual care plans. (a third nurse)
Who took control and ownership of the sessions? From teacher-led instruction to ownership by the nurse responsible for the patient
The first eight sessions dealt with the screening tool B-CAM and individual care plans for discharged patients. The NSC presented screening tools or excerpts from individual care plans for a discharged patient at risk of developing delirium. She had chosen the extracts and prepared relevant questions. The nurses answered briefly without any discussion. One nurse said to the NSC ‘Why don’t you just tell us what’s right, you know what the answer is!’ (nurse). The question from the NSC was perceived as a kind of test of given facts without recognition of the nurse’s possible contribution.
In the final ten sessions, the NSC agreed in advance with one of the nurses responsible for the patient that this nurse would present issues in delirium prevention in relation to her particular patient. Such an invitation to the nurses represents AI, where the NSC becomes more of a facilitator than a teacher. At one session, the NSC started by showing appreciation for the willingness of the patient’s nurse to present her contribution to an individual care plan and for her drawing attention to the successful aspects of the plan. Finally, the fact that the NSC assigned responsibility for further enhancement of the individual care plan was in itself an expression of recognition of the nurses’ resources. Today, I’ll hand over to Anna [anonymized] who’s going to talk about her patient … Anna has already written down several good suggestions for nursing actions, and now she’d like to have your [the nurses’] input to complete the individual care plan for the prevention of delirium. (NSC) Personally, I think it would be nice if the patient was more involved in his individual care plan, but in respect of functioning and activity and pain, the patient is involved. (the patient’s nurse) … according to the guideline, the patient shouldn’t be scored [B-CAM screened] any more, he’s been ok for two days now, but I thought he fluctuated so much in the beginning, and now he’s also got more pain. (another nurse) … yes, it would be a good idea to continue to score him until he gets better. (a third nurse) … at the next session we can work on the individual care plan for his mobilization. (a fourth nurse)
The findings in Figure 1 show that when AI was used in connection with data on a current patient, when there was shared learning and when the patient’s nurse took ownership and leadership regarding her patient, facilitated by the NSC, it became meaningful for the nurses to use the clinical guideline on delirium in CDM. In this way, the nurses’ knowledge of the use of a clinical guideline in CDM was created.
Changed use of AI over time and significance to CDM.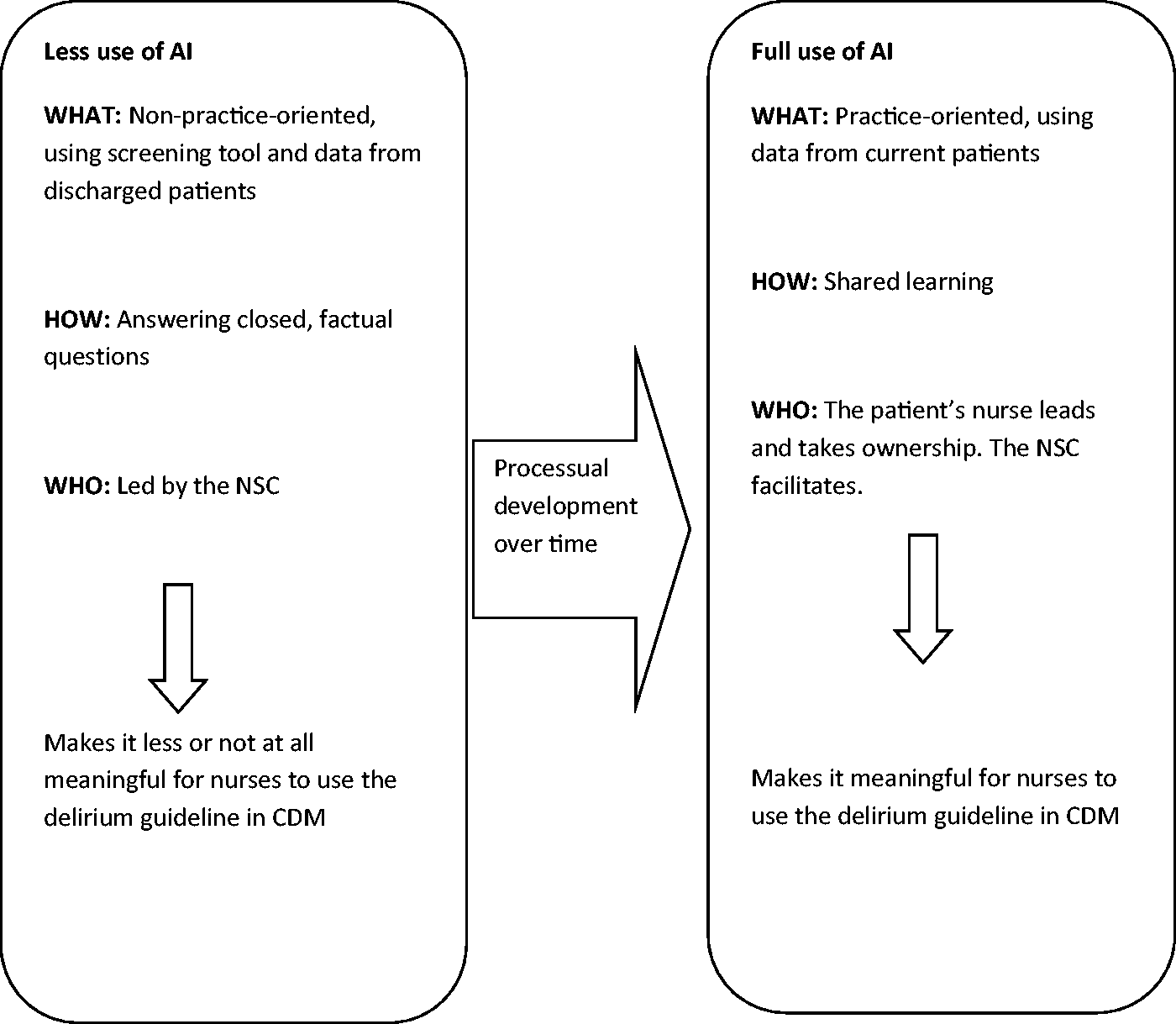
In the course of the 18 sessions, a reciprocal process took place, where the change in the NSC’s role from teacher to facilitator increased the nurses’ knowledge of using a clinical guideline on delirium in CDM, and the nurses’ increased knowledge and interest encouraged the NSC in her adoption of the new role.
Discussion
The fact that nurses want the sessions to be based on hospitalized patients (practical orientation – what) in CDM, and that it is the nurse who has knowledge of the patient who presents the patient’s problems (ownership – who), is confirmed in Teodorczuk et al.’s study. 35 This shows that if care for dementia patients with delirium is to be improved, learning must have a practical focus on both knowledge of the patient and recognition of the clinicians’ knowledge about the patient.
The use of AI with open and reflective questions gave nurses the opportunity to involve each other’s ideas, experiences and knowledge and thus explore and see new potential in CDM. Shared learning allowed the nurses to take independent responsibility for developing CDM and for their own learning processes by taking ownership of the professional discussions in the sessions. This can be understood in light of Bruner’s description of learning as a co-creative process with a focus on language and the creation of meaning in language. 36 Language is social and words gain meaning in a context consisting of relationships with other people. Meaning is created in a communicative process involving the exchange of understandings and explanations, which allows for the construction of new understandings and actions. In this way, the nurses together created professional arguments for CDM and learned from each other. This community of mutual learners, in Bruner’s understanding, is essential for the creation of identity and competence in the individual nurse. 36 This is supported by our findings, which show that it created meaning and great interest among nurses to enhance professional argumentation together. This concurs with Wenger’s understanding of learning as social participation, where active participation in communities allows one to construct, develop and change one’s professional identity. 37 This is confirmed by our findings showing that it was meaningful for the nurses to discuss back and forth with their colleagues and together see and improve each other’s individual care plans.
The nurses’ much greater interest and involvement in the current patient than in the discharged patient can also be understood in the light of Wenger’s description of communities of practice involving mutual commitment to a common activity with a common repertoire, 37 as nurses have a common commitment to care for patients as their jointly negotiated activity and CDM is part of the common repertoire. In Wenger’s communities of practice, the participants have a common understanding of what they are doing and what they are responsible for. It was thus important for the nurses’ commitment that it was the patient’s nurse, as a full member of a community of practice where participation is acknowledged as a competency, who presented individual care plans for the patient. The patient’s nurse controlled and took ownership of the professional enhancement, in contrast to the NSC, who was perceived as having a more peripheral role. In terms of Wenger’s concepts of overlapping and complementary competencies, 37 the nurses may be seen as having overlapping competencies in relation to patient care, whereas the specialist nurse has complementary competencies, such as particular expert knowledge of the clinical guideline. The findings show that her knowledge of clinical guidelines and her knowledge of using AI affected the nurses’ learning process regarding the use of clinical guidelines in CDM. Marchionni and Richer emphasize that the advanced practice nurse is of great importance for the development of evidence-based nursing, since her higher educational level and credibility among nurses can help to launch innovative initiatives and she can transfer knowledge through the use of AI and by positioning herself as an advisor and mentor to support changes in the organization. 22
The action research process allows participants to develop the skills to use AI. This is seen in the findings, where in the early sessions it was a challenge for the NSC to use AI on the basis of a resource focus rather than a problem focus,16,17 while the later sessions saw greater use of AI.
Appreciative inquiry has been criticized for being superficial and manipulative with its focus on positive aspects which suppresses opposition and conflicts within the organization.16,38 The findings include an example where the nurses’ reluctance to use the B-CAM screening tool is not pursued by the NSC which emphasizes that openness, responsiveness and especially the ability to apply AI in organizations is essential.
Methodological considerations
The use of field notes reveals the changes and developments that take place over time in CDM. Field notes and participant observations provided an understanding of the nurses’ location, activity and interaction during the sessions. For example, notes were taken when the patient’s nurse operated the computer and projector, and when the nurses’ commitment was reflected in interactions in the sessions. It would have strengthened the study if the sessions had been audio or video recorded, allowing for more extensive recording and verbatim transcription. The field notes were regularly discussed by the SLs with regard to validation and a critical attitude to their own position.26,39 The nurses’ experiences of their learning processes were indirectly involved, since the content and form of the sessions were regularly adapted to the nurses’ feedback. With an action research tradition26,39 as a framework for the intervention, it would be natural for all participants to discuss the observations to provide both an outside and inside perspective on the nurses’ learning process.
Conclusion
The present study examined 18 sessions where nurses discussed the prevention and screening of delirium in cardiac patients with reference to a clinical guideline on delirium. With the use of AI in the sessions, it became meaningful to nurses to use the delirium guideline in clinical decision making, with a focus on the following:
What the content of the sessions was: this changed from a non-practice oriented approach using data from discharged patients and the clinical guideline in itself to a practice-oriented approach, using data on a current patient. How learning took place in the sessions: here we saw a development from learning by answering closed, factual questions to learning through common reflection. Who took control of the sessions: here there was a movement from the NSC being in charge to the patient’s nurse taking ownership and leading the session about her own patient.
In this way, the nurses’ knowledge of the use of a clinical guideline in CDM was created.
A limitation of the study is that it took place in two wards of the same cardiology department. Such an intervention using AI, where CDM is the focal point in relation to using the clinical guideline on delirium, needs further research in a greater variety of wards and hospitals, particularly in ICUs, where delirium develops in up to 87% of patients. 2
The results of the study could have implications for practice, as nurses will acquire the skills to implement evidence-based clinical guidelines. Nurses will thus understand, interpret and use shared knowledge and experience to translate such guidelines into clinical practice.
Footnotes
Funding
The project Implementation of evidence-based practice: an innovation project between theory and practice was supported by the Danish Ministry of Education and Research special fund for practice-oriented innovation projects. 24
Conflict of interest
The authors declare that there is no conflict of interest.