
Abstract
The aim of this study was to describe partnership activities between a university of applied sciences and a nursing care unit for the elderly, the competences that staff members working across these organizations needed and the outcomes gained. Staff of the organizations took part in nine focus group interviews (n = 39) and completed self-evaluations based on diaries (n = 13) and essays (n = 24). The data were analyzed using qualitative content analysis. The staff planned, coordinated, implemented and surveyed change processes based on a joint development target and developed student supervision. Staff needed competence to analyze their expertise and the organizations’ operations, as well as to manage development work, negotiations, communication and networking. The outcomes included identifying possibilities for cooperation and establishing new partnerships, developing good practices and new expertise, boosting student recruitment and supervision, as well as recruiting staff, mentoring and advancing their career development.
Introduction
Partnerships between higher education and clinical practice have traditionally been restricted to the establishment of teaching hospitals and clinical practice placements, and supervision of thesis work. However, in recent years, participation of higher education in the development of workplaces has revealed a need to develop systematic partnership structures and processes. Transferring traditional classroom teaching to the workplace context has enabled re-examination of teachers’ attitudes, competences, job descriptions, continuing education and leadership culture. It has also challenged the development of pedagogy, learning environments, provision of education and qualifications frameworks.1–4
Partnerships are needed to solve problems that organizations face and cannot manage on their own, thus requiring new solutions by crossing organizational boundaries. Such partnerships provide additional value to organizations and are profitable compared to the costs of partnership. Casey’s literature review suggests that partnership can be defined based on the intensity of the implementation of decision-making. 5 Key characteristics of partnership include conveying decision-making across organizational boundaries and fostering interaction based on negotiation, mutual problem-solving and learning. Additionally, typical features of partnership include voluntariness, mutual trust and equality, respect for the competence of partners, joint development targets, common goals and commitment and strategy related to their implementation, common principles of action and instructions, as well as shared leadership and resources.1,2,5–9
As evident in previous systematic reviews, there are ample research data on factors promoting partnership, but data on the implementation and outcomes have so far been more scarce and produced from small-scale research.5,10 Partnership between higher education and health care has mainly been studied in the United States and United Kingdom. Some of the central features of partnership, such as learning together or participatory change management, have often been studied from the perspective of organizations’ internal processes or multi-professional team activities, excluding partnership as a phenomenon between organizations.11–13 Previous examinations of partnership phenomena between organizations have mainly focused on network analyses, which often did not consider how the partnership was implemented, what was achieved and learned together, and how partnership is best maintained. 14
The present study was part of a larger research project focused on the poorly-studied area concerning partnerships between organizations.5–14 The study was conducted at a university of applied sciences (UAS) and a nursing home. The first phase was a systematic review, 10 whereas the second phase was a study of the factors influencing partnerships. 8 This article describes the activities and competences that staff members working across organizations need in a partnership and the additional outcomes that partnership offers to organizations, i.e. outcomes that the organizations could not have gained without the partnership. 5
Review of previous research
An evaluation of outcomes must consider immediate outputs originating from partnership development, as well as changes in the organizations and outcomes of the development work, which may be indirect, short- or long-term. 1 Here ‘outputs’ refers to action plans based on mutual agreement. Their implementation leads to changes in the participating organizations and possible improvement of staff education and recruitment. Developing partnership takes time and identification of long-term outcomes may be challenging. Further, the many-faceted and multiform nature of operating environments complicates the evaluation process, as well as hampers the identification of intervening factors. 7 It has been estimated that about half of the partnerships in health care remain in action for over a year and that several of them do not achieve their objectives. 2
Gaining outcomes is dependent on the leadership and administration of partnership.7,15 In addition to long-term effects on society, more immediate results of partnership, such as satisfaction with it and its leadership and the quality of partnership processes, should be evaluated. 7 Evaluation of such effects has so far been limited, as have input–output analyses. However, De Geest et al. have reported US and Swiss models that enabled the examination and confirmation of equal distribution of benefits. 6
Partnership between higher education and the health-care environment has enabled the strengthening of research capacity and development of health services and nursing programs, as well as improved possibilities for staff education.1,2,6,12,15 Both numbers of awards and amounts of research funding have increased. 2 Furthermore, partnership has led to development targets on patient care and boosted evidence-based practice.16,17 Other reported attributes include enhancing the image of organizations, improving political means to impact, developing teaching and student mentoring and expertise, as well as improving learning outcomes, staff career development and recruitment. 10
Method
Aim
The aim of this study was to describe partnership activities between a UAS and a nursing care unit for the elderly, including the competences that staff members working across these organizations needed and the gained outcomes.
Research context and participants of the study
The study participants included staff from a UAS offering degree programs in nursing, health care and welfare and staff from a service unit for the elderly from one city in Finland. The organizations recruited together nearly 70 persons in total, categorized as developing teachers (DTs) and developers of the workplace (DWs) to develop partnership as a project. The average annual working time of the DTs on the project was 202 hours, whereas the DWs worked for 95 hours. Partnership was realized in three collaborative subprojects focusing on the development of nursing care for the elderly. The subprojects focused on patient safety, particularly in medical care, preventing errors, rehabilitation, discharge and home care. The forms of collaboration included workshops, project meetings, small groups, joint study visits, joint representation at conferences and pair work. 8 The study comprised 36 female and 3 male participants holding positions as directors, development managers, principal lecturers, lecturers, physicians, head nurses, nurses, physiotherapists, occupational therapists or practical nurses. Their average age was 45 years (range of variation 24–61 years). The duration of their present position was on average seven years (range of variation 6 months–21 years). Less than half of the participants had previous experience of two to three joint ventures between a UAS and the workplace environment.
Data collection and analysis
Description of the data collection methods.
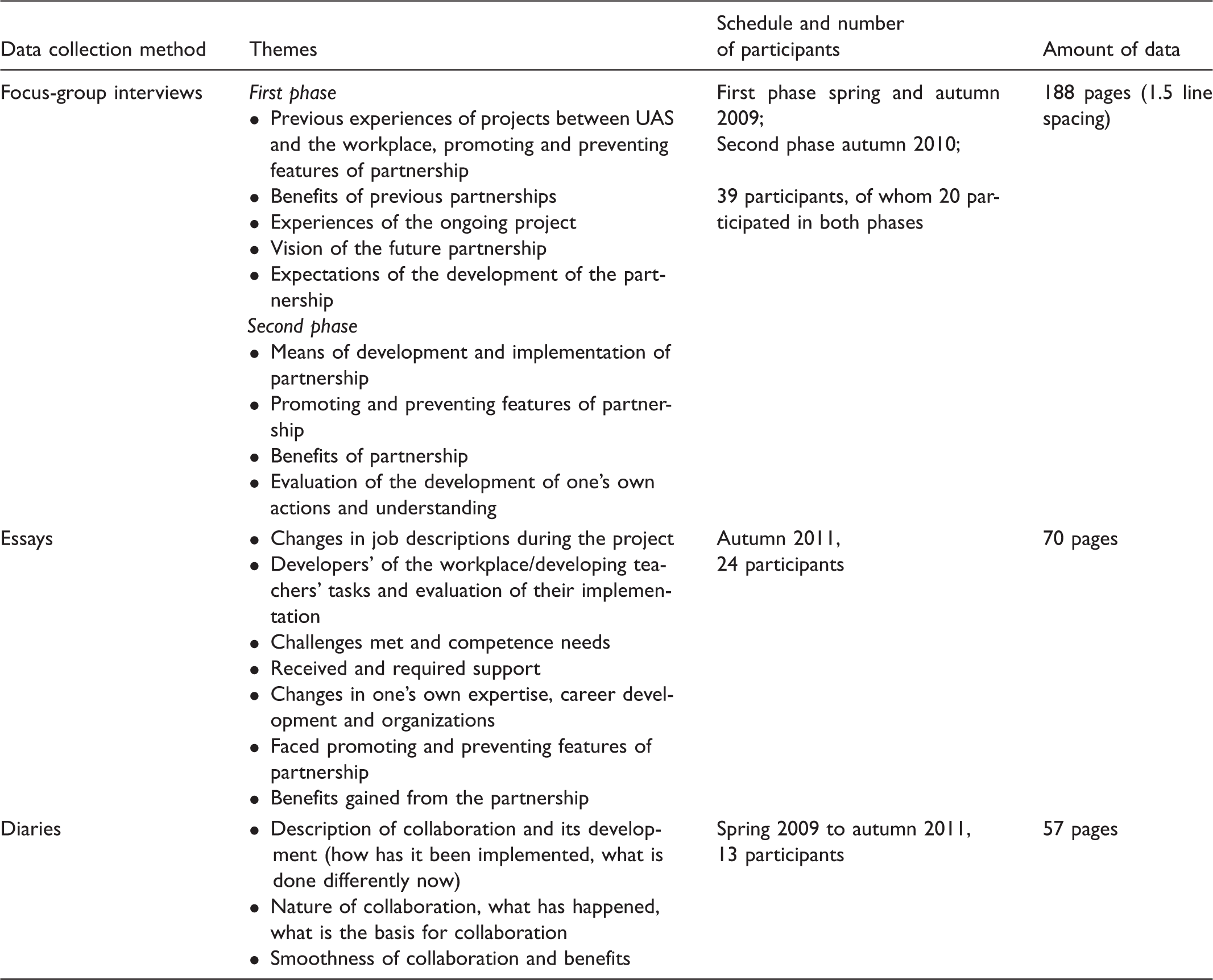
The data were analyzed using qualitative content analysis.
19
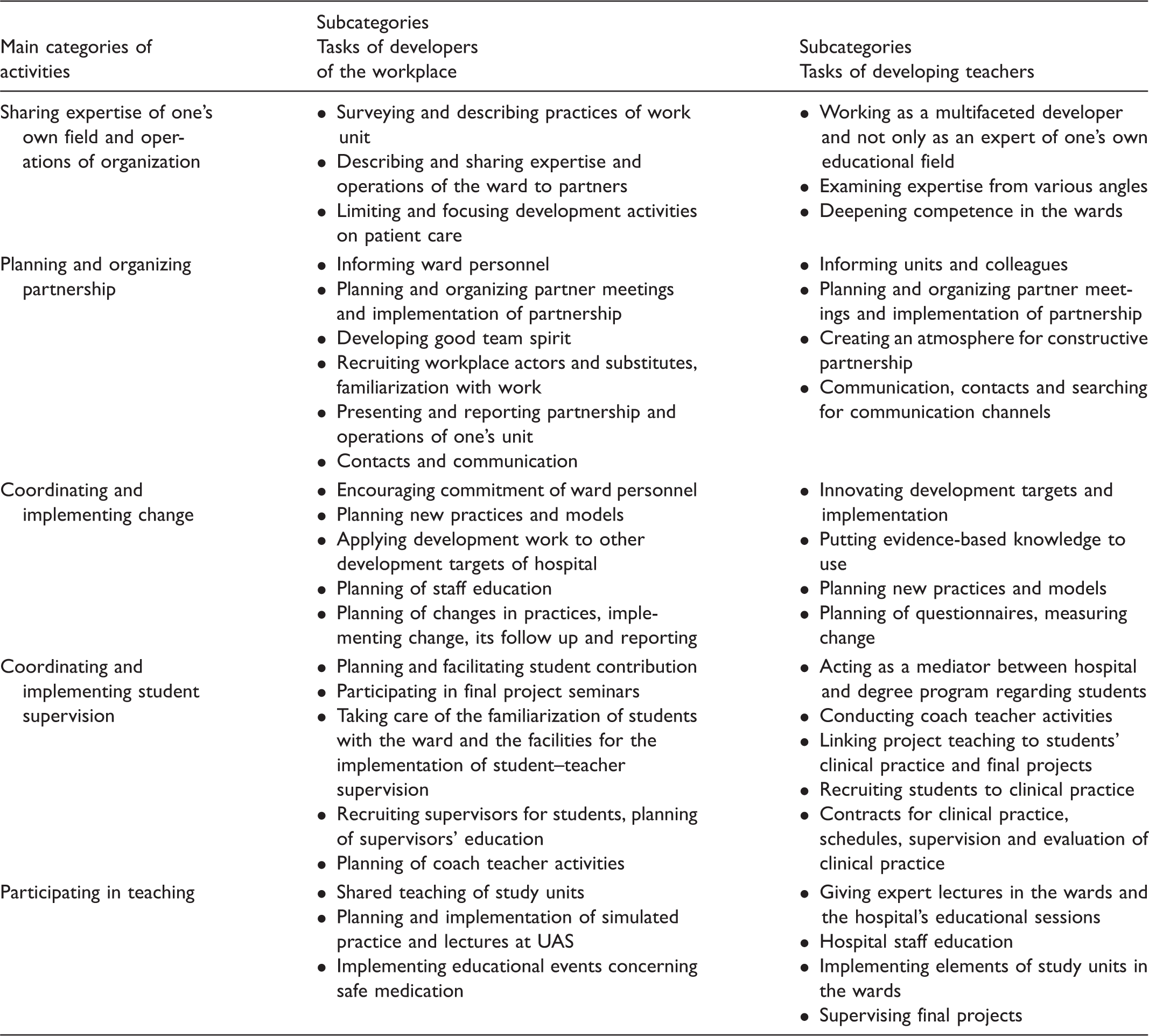
The participants’ statements during the group interviews and their descriptions of their experiences in the diaries and essays were used as the unit of analysis to ensure a full spectrum of experiences was included. Original expressions relating to the research questions were selected from the data and reduced. They were mutually compared based on their similarities and differences. Expressions with the same content were classified into the same subcategory. The subcategories were mutually compared based on their similarities and differences, and subcategories with the same content were combined into main categories. The main and subcategories were named based on their content. Both authors analyzed the data (Figure 1 and Table 2).
Outcomes of partnership. Activities and tasks of the developers of the workplace (DWs) and the developing teachers (DTs) in the partnership.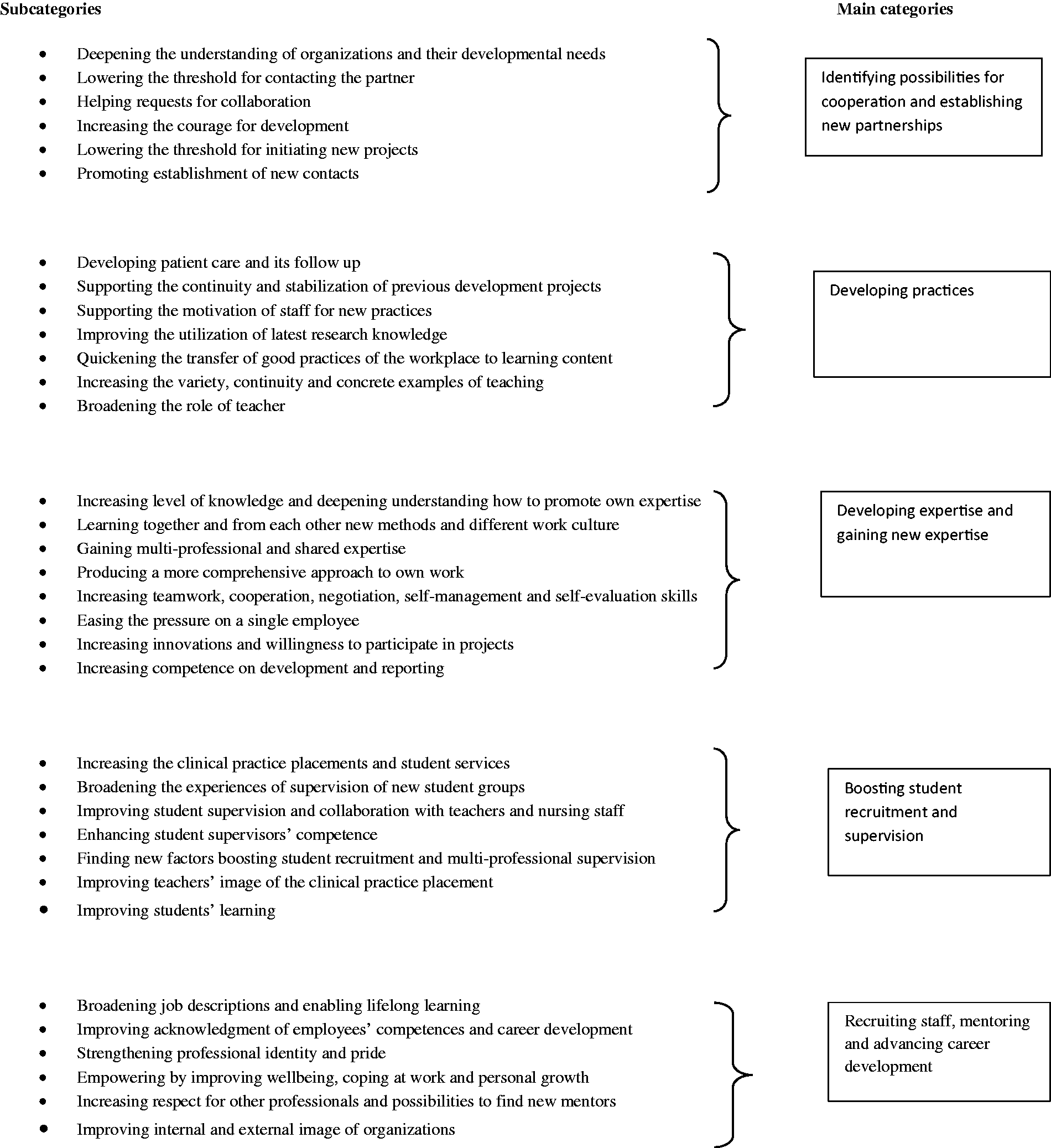
Written consent to carry out the research was received from the participating organizations. The DTs and DWs were informed about the research at the beginning of the project and provided with details on the data collection method and its phases. Their verbal consent for recording the interviews was also sought. Moreover, the participants were informed that they could withdraw from the process at anytime. No personal information was collected.
Credibility and limitations
The participants received a list of the interview themes by email in advance of the interview. This facilitated the analysis of experiences and preparation. The interviewees described their experiences extensively and without hesitation and unnecessary interruptions. Everyone was heard in the interviews and all themes were discussed. The group size was considered appropriate. It was possible to return the diaries or essays anonymously, and it was not necessary to indicate the organization. This enabled thorough reflection on experiences and evaluation of development needs.
Group interviews offered several advantages compared to individual interviews, including the prospect of exercising control between interviewers and interviewees, receiving more versatile data and aiding the participants’ memories. When listening to others, interviewees shared experiences they might not have identified in an individual interview. The interviewees had experiences of the same research context and partnership process. This increased the description of valid data and reduced the need for giving socially acceptable replies. 19 Finally, the validity of the data was increased by triangulation implemented during data collection and because the data were collected during different phases of the development project.
The researchers discussed the implementation of the analysis as well as identified and named the categories describing the results. The relation between the categories and the original data is here indicated by direct quotes enabling the credibility of the evaluation of results. Each main category consisted of several subcategories. Based on them, it can be deduced that saturation was obtained. The results of the analysis have been verified by the participants at workshops and seminars.
The results produced were limited to project actors and two organizations. Experiences of the whole personnel of the participating organizations were not studied. The project actors took part in the project based on their positive attitude toward the partnership and interest in it. This might have lead to overestimation of the outcomes. Another limitation was that data collection ceased at the end of the project. Thus, the results mainly provide information about immediate reflections of the implementation and outcomes of the partnership.
Results
Activities and competences of developing teachers and developers of the workplace
The main activities of DTs and DWs were the same, but their implementation was emphasized differently (Table 2). The DTs were expected to provide more research knowledge and multifaceted expertise to the use of the wards than DWs. In contrast, the activities of the DWs focused more on the implementation of changes and their follow up. However, DTs provided support in the development of follow-up methods related to the implementation of changes. Teaching was implemented by traditional means and the amount of expertise exchange from the hospital to the UAS was considerably less than the amount of information provided through teachers’ lectures in the hospital.
Partnership required adequate experience of one’s own field and readiness to identify and analyze expertise and experiences. Competence related to expertise included skills to identify and analyze development targets, skills to examine the implementation of evidence-based knowledge, as well as the ability and willingness to develop and build on expertise. In the identification of one’s own organization, an emphasis was placed on being aware of the operating processes and practices, as well as the purpose of the support organization and strategic goals.
In the management of the development process, visualizing and understanding entities and change processes, positive attitude, courage, tolerance toward stress and uncertainty, curiosity, innovativeness and the ability to see the outcome were all highlighted as important. Both DTs and DWs were also expected to show willingness to change modes of action, commitment and decision-making and self-guiding skills. Skills to motivate and encourage others and be able to rely on them were essential. During the partnership, important negotiation and communication skills included the ability to speak the same language and appreciation of partners’ competence and equality. Partnership required ability for dialog and reflection and to consider the partner’s interests, as well as courage to present and justify one’s own opinions. This required flexibility and openness. Understanding group dynamics helped in negotiations and orientation to cooperation.
Crossing organizational levels was needed to obtain authorization for the development process and for reporting and presenting results. Developers of the workplace and developing teachers cooperated more with their organizations’ leadership than before. Networking also required familiarity with agreement procedures.
Outcomes
Outcomes of the partnership are presented in Figure 1. The DTs and DWs did not identify any disadvantages or negative impacts of the partnership, and outcomes were identified at both an individual and organizational level.
Identifying possibilities for collaboration and establishing new partnerships
The partnership promoted partners’ understanding of their partner organization. It improved identification of possibilities for collaboration. Partnership also increased understanding of the operations of one’s own organization. The professional language used was easy to understand, facilitating contacts and requests for collaboration. Understanding has increased incredibly and knowledge of all these actors at the UAS and how we can work together at the workplace. (DW, diary) The teacher worked in the ward for a week, presented interesting ideas, on which I gave feedback. (DW, focus-group interview)
Developing practices
Partnership enabled the development of nursing practices and also supported the continuity and stabilization of previous development projects. Development activities were supported by education organized by the partners. Supervisors in the units received support from DTs and DWs to motivate staff. In addition to development activities, emphasis was placed on the introduction and learning of new practices, as well as their follow up. Follow up also included developing teachers’ observations in the wards and on students’ final projects. Evaluation of the study participants’ basic tasks increased. Furthermore, partnership enabled application of the latest research knowledge in the wards. For example, the wards gained evidence-based knowledge of functional and visual capacity that would have been ignored without the partnership. The approach to work changed as it became more rehabilitative, holistic and patient-centered. Because of partnership, the practices of one’s own support organizations became more familiar. We have developed promotion of functional capacity. Working has been more structured and we have adopted a more holistic approach to dealing with patient issues than before. (DW, essay) In the ward, a few very good ‘expert nurses’ were pointed out to me and I was able to have lengthy discussions with them on clinical nursing, implement patient-centered nursing, acquaint myself with administering medication and reporting by means of the Effica system, familiarize myself with current guidelines on hygiene, etc. I now have a lot of written material and knowledge that I have applied to my teaching and have shared with my colleagues. (DT, diary)
Developing and gaining new expertise
The renewal expertise of DTs and DWs manifested itself as increased level of knowledge, deeper understanding and readiness to adopt a more comprehensive approach to issues at hand. In addition, shared expertise was gained when expertise was combined between the two groups. According to the DWs, partnership enabled new expertise to be gained without additional cost. Examining work became more versatile and responsibility for basic work tasks was viewed differently. Interest in developing work and participating in projects, in addition to utilizing students’ final projects, increased. The concept of multi-professionalism and understanding of it also broadened, and belief in working together strengthened. Moreover, teamwork and cooperation skills increased. Self-management, self-evaluation and giving and receiving feedback improved. Finally, working with the project strengthened the readiness to express opinions and present oneself. I have learned to foster a new culture, constructive negotiation and innovation together from the teachers. (DW, essay) Multi-professionalism will have an effect on my teaching now and in the future. It seems there is no return to the monologic learning concept, and trust in working together has become much stronger. (DT, essay) Earlier, I often thought about things from the perspective of my work unit, but now I have changed my way of thinking to a more comprehensive way, considering the special needs and practices of different wards, as well as partly also that of the teachers. (DW, diary)
Boosting student recruitment and supervision
Collaborating in student supervision was new to the partnership organizations, requiring many development actions in addition to the clinical practice placements, such as meal provision and travel costs. New student groups were formed, including students of prosthetics and orthotics, social services, optometry and media technology. Recruiting students was considered the primary route to employ staff. Competent and multi-professional supervision was seen as an important means of recruitment.
Participants organized specific recruitment sessions aimed at students starting their clinical practice and students completing their studies. Factors that boosted recruitment included paid clinical practice in the summer contributing credits for students, formal and informal information sessions given by previous students in the wards and a few days’ supported orientation period before actual clinical practice. Participants felt it was important to inform students that the clinical practice placement enabled learning in a comfortable learning environment. Teachers’ positive image of the clinical practice placement and knowledge of the clientele in basic care were regarded as important.
Partnership promoted student supervision and supported future employees’ graduation. In clinical lessons, the students’ syllabus and objectives of clinical practice were presented. This promoted understanding of the objectives, improved familiarization of students and supervisors, as well as increased the input of teachers. New modes of operation were introduced to achieve these results and students were considered an essential part of the work community. Information provided by the UAS became more relatable to practice. Students had the opportunity to become familiar with the wards in a more diverse way than before. According to the DWs, students’ clinical practice and learning assignments suited the development work in the ward better and focused on issues relevant to students’ learning. The teacher conducted a clinical lesson about this matter. We went through the personal study plan so that we knew what to expect and that the goals were not too high but very concrete and that we can support the students. (DW, focus-group interview) Maybe I can relate to students’ role and experiences better as a teacher now that I have been part of the work community myself. (DT, diary)
Recruiting staff, mentoring and advancing career development
Partnership provided new opportunities for career development, and consequently had positive effects on staff recruitment. It also sparked interest in further studies. Participants hoped that staff in nursing care could in future combine development tasks, research and teaching with their job descriptions, whereas teachers could implement clinical nursing or manage wards. The partners felt that the starting point for this type of career development was initiating staff competence surveys in both organizations. Their purpose was to create an effective and flexible platform for combining the needs of staff competence, work community and organizations. Expanding one’s job description toward another professional group was seen as an important form of career development. This was defined as horizontal learning. It was assumed that these job combinations would increase interest in the work and would particularly attract persons with several targets of interest, who were seen as valuable innovators for the organization.
Moreover, mentoring pairs were formed between the UAS and the workplace. Ideas and opinions of other professionals stimulated innovations at an individual level. In particular, the DWs wanted to learn pedagogical skills and leadership of change from the DTs. The continuing education of staff nurses and study for qualifications became easier because clinical practice could be implemented in one’s own unit and the mentor was one of the DTs. The partnership strengthened professional identity and pride, as well as empowerment. Self-confidence and self-assurance increased. It has been great to show the teachers methods of clinical practice. (DW, essay) I have been implementing new teaching and I hope that in the future I dare be part of diverse teaching. I am not satisfied with implementing a study unit by traditional means, but it would be interesting to be creating something new. When you work within the limits of your competence, you see your shortcomings and development areas and it is positive thing regarding career development. (DT, diary) It is part of multi-professionalism that one person does not have to know everything; there is enough multiple expertise in the unit. (DW, diary) When the group realizes that we can cope, pull together, gather and forward things, it does give confidence and you feel you are not alone. It has empowered me. (DT, focus-group interview) I speak about the cooperation between the UAS and us and I particularly defend the work of the UAS from a new perspective than before this project. (DW, diary)
Discussion
This study contributes new knowledge of partnership. It focuses on a previously poorly-studied topic and provides a new cultural perspective on partnership from Finland.5,10 The concepts identified in this study facilitate the transferability of the results outside the research context.
In this study, participants brought their expertise and routines of their organizations to the partnership. Including this contextual knowledge in the development of work is highly important because in addition to identifying a mutual development target, it helps renew the involved organizations. Changes taking place in organizations must be traced to the level of true actors. It is central to examine the implications of changes and types of new practices that the collaboration generates. Common practices convey the learning outcomes of developers but may represent new organizational routines for other actors, producing a wide range of effects. According to a review by Casey, 5 staff transcending organizational boundaries need adequate resources for their work and clear support from leadership. In addition to one’s own expertise and organizational analysis, interaction skills and skills to bring about change are required. These have also been identified as critical success factors of partnership in previous studies.5,8,15 Establishing partnership requires the means to implement partnership at strategic, tactical and operational levels of organizations. 2
The results indicate that both partnership organizations benefitted equally. According to MacPhee’s classification, the benefits were mostly immediate. 1 The results show that partnership facilitated identification of possibilities for collaboration, improved understanding of both their own and partnership organizations and made contacts with the partner easier. Other immediate and concrete benefits included reinforcing evidence-based nursing in the clinical practice of the wards, as well as identifying development targets. These results are very important. They suggest that partnership between higher education and health care can diminish the gap between theory and practice. Previously, Missal et al. 16 and Weeks et al. 17 arrived at similar conclusions. As for the UAS, it was possible to transfer the good practices of the workplace immediately to teaching, resulting in more comprehensive learning methods being used. Furthermore, expertise developed and deepened. Partnership impacted patient care, student supervision and student and staff recruitment, as well as encouraged a positive image of the organizations. Similar results have been reported by MacPhee, 1 Häggman-Laitila and Rekola, 10 Zwarenstein et al. 11 and Bitton et al. 15 The benefits were interconnected. For example, improved student supervision promoted student recruitment to the hospital.
Apart from the direct immediate changes, indirect benefits were also identified. 1 These included empowering staff, changing attitudes and increasing commitment and courage, as well as improving image. The long-term benefits of partnership consisted of new job descriptions and future opportunities for career development. Utilization of partnership is dependent on its leadership and administration. For example, many work communities that have excellent availability and permanence of staff have established multifaceted partnership agreements with higher education. 7
New practices reinforced learning in the organizations. However, a more systematic learning process and engagement of all personnel to adopt partnership principles would have required crossing the organizational boundaries of the leadership structures. According to the views of the participants, transferring knowhow from the health care environment to develop teaching at the UAS remained less fluent than transferring knowhow from the UAS to develop nursing at the hospital. Participants felt that the partnership was largely driven by the UAS and a balance of power and joint decisions were not achieved owing to a lack of commitment by the leaders. 8 Leadership of partnerships should be an important target for future research. Further research is also needed to identify the requisites for consolidating partnership and the quality of the partnership process. Partnership is methodologically a challenging area of research and requires development of methods and measurement. Likewise, long-term follow up of the partnership process and its benefits requires further research.
Conclusions
The common activities of DTs and DWs were identified as sharing expertise of their own field and operations of their own organizations, planning, coordinating and implementing change in care and reorganizing student supervision and participating in teaching together. However, the implementation of the activities differed to some extent between the DTs and DWs. Developing teachers were expected to provide more research knowledge and multifaceted expertise for the use of the wards than DWs. In contrast, the key roles of the DWs were the implementation of changes and their follow up. However, DTs provided support in the innovation and development of follow-up methods. The crucial competences of staff transcending organizational boundaries included analyzing their own expertise and the operations of the organizations, as well as managing development work, negotiations, communication and networking. Partnership can produce several outcomes to organizations in a short developmental period. Beneficial outcomes identified in this study were identifying possibilities for collaboration and establishing new partnerships, developing practices, developing and gaining new expertise, boosting student recruitment and supervision, as well as recruiting staff, mentoring and advancing career development. Development of leadership structures is needed to maintain the achieved benefits and support the partnership activities.
Footnotes
Funding
This study received support from the Social Fund of the European Union.
Conflict of interest
The authors declare that there is no conflict of interest.