
Abstract
This article describes the development, organisation and significant elements of an Umbrella Model, which has been demonstrated to support knowledge and practice development in a large Danish hospital department. The aim is to inspire, support and guide implementation of the Umbrella Model in other settings. A shared theme overarching several minor projects is the core of the model and is exemplified in three completed programmes: Young people with cancer, Relatives and the cancer patient’s social network and Future cancer care – short but high quality. Commitment is achieved through close dialogue, supervision and programmes dealing with local needs and complex problems in clinical practice. The model unites clinical and academic competencies, has produced new knowledge and developed nursing care, and it has directed nurse leaders’ attention to the pivotal role they play in supporting a learning environment.
Introduction
The challenge in healthcare to deliver more efficient and effective care for less money and still ensure that patients and their needs are put first1,2 results in a constant search for new developments in clinical practice. This search includes production and use of knowledge and implementation of new ways of working. Healthcare organisations cannot afford to waste time and labour on projects that are not finalised, documented and, if successful and relevant, implemented. Therefore, healthcare organisations such as hospitals and clinical departments have to effectively use employees’ potential, competencies and skills to collaborate on the development of clinical practice and consolidation of changes. Motivation and active participation are crucial factors in achieving this. 3 These can be accomplished by a bottom-up approach involving practitioners in the identification of problems to be addressed and simultaneously by taking context and facilitation into account as significant factors of successful implementation. 4
Research-based development models in clinical nursing practice that involve entire organisations are sparsely documented in the literature. A search conducted in September 2015 in the databases CINAHL, PubMed, Scopus and Embase (using the following keywords in different combinations: collaboration, collaborative model, action learning, nursing, nursing staff, graduate, academic–practitioner partnership, faculty–nursing relations, staff development, and clinical practice) revealed that most studies deal with undergraduate teaching and learning, and curriculum development.5,6
Therefore, the aim of this article is to describe the development and details of a practice development model, the Umbrella Model, that has been demonstrated to work continually for a period of 10 years in a large clinical setting, in order to support and guide implementation of the model in other settings.
The description will comprise:
The origin of the Umbrella Model, its foundation on action learning principles and the organisation behind the model. Programme structure and phases. Achievements of the programmes based on the model.
Formation of the Umbrella Model
The Umbrella Model has been developed and practiced over the last 10 years (2005–2015) in a large cancer department at a Danish public university hospital. The department is led by one matron and a chief medical doctor. Ten ward managers lead the staff, wards and clinics. About 650 staff members are employed; 280 are nurses. The department consists of in-patient wards, day-care and out-patient clinics, a large radiotherapy clinic and a palliative team unit. A nursing unit for education, development and research (NEDR) is established and engages seven nurses with academic competencies who have reference to the matron.
The Umbrella Model grew out of processes and experiences developing a practice research programme in the department (2005–2008) dealing with the overarching theme ‘Young people with cancer’. 7 At that time a couple of nurses in the department had obtained academic degrees at master’s level. It was therefore decided that the programme should include these academic nurses as well as from the staff. Subsequently, two additional two programmes using the Umbrella Model have been completed in the department.
Under a shared overarching theme that forms the umbrella, clinical nurses, and if possible multidisciplinary colleagues with different experiences and competencies, carry out development and practice research projects in the same programme.
Learning in action
The Umbrella Model uses action learning principles.
8
Action learning and practice research aim at producing useful knowledge for and with practice in order to establish sustainable changes
9
and address potential learning transfer barriers.
10
Learning takes place in cycles, and involves concrete experience, reflective observation, abstract conceptualisation and active experimentation.
11
It is an essential developmental process that encourages creative and innovative thinking. Although the concept is defined in different ways, Revans’ description of action learning as a reflection-in-action approach that is embedded in a group setting, working on a real-life problem and resulting in exploration of alternative ways of practice, captures its essence well.
8
Likewise Zyber-Skerritt
12
has identified general features in action learning as:
learning from concrete experiences; critical reflection on the experience through group discussion; trial and error, discovery, and learning from and with each other.
As suggested by Zyber-Skerritt, we have distinguished between action learning projects and action learning programmes. A programme consists of several projects and it is facilitated by one or more experienced mentors or advisors. The objectives of an action learning programme are described as: team and vision building, networking, clarity of project focus, definition of the problem and each action step, commitment to personal and group reflection and learning, input into each other’s projects and an appropriate evaluation of both the learning process and the outcomes.12(p.119)
Organisation
The organisation of the Umbrella Model (Figure 1) consists of one or two ‘umbrella holders’/project facilitators who are supported by a steering committee that surveys the programme and supports needed actions in order to reach the goals and learning objectives. Three groups are affiliated to the steering committee: a group of active staff members working with self-decided single projects under the overarching theme; a group of supervisors; and a group of ward managers in charge of the nurses involved.
The organisation behind the Umbrella Model.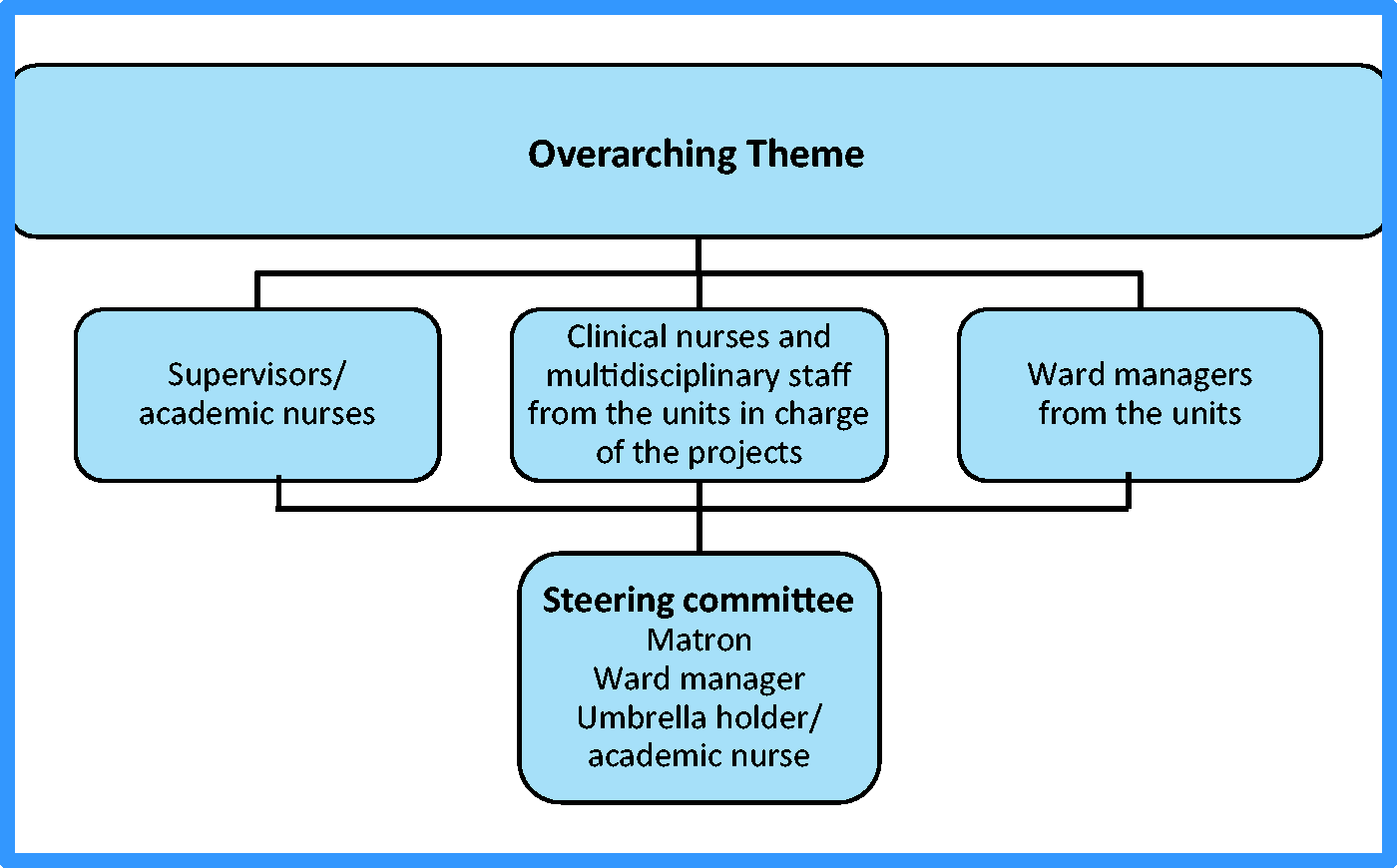
Programme structure
The programme is divided into four phases: 1) pre-programme, 2) preparation, 3) project implementation and 4) completion. Phases 2–4 each last about one year (Figure 2). The single projects take place in each ward/unit in parallel with clinical work. Therefore, it is important to assure enough time for each phase is available, in order to avoid forcing the process and creating stress. However, by committing oneself to be part of the programme and to conduct a project members of staff must be willing to invest some spare time.
The dynamic structure of the Umbrella Model showing phases and processes of the programmes inspired by an action learning approach.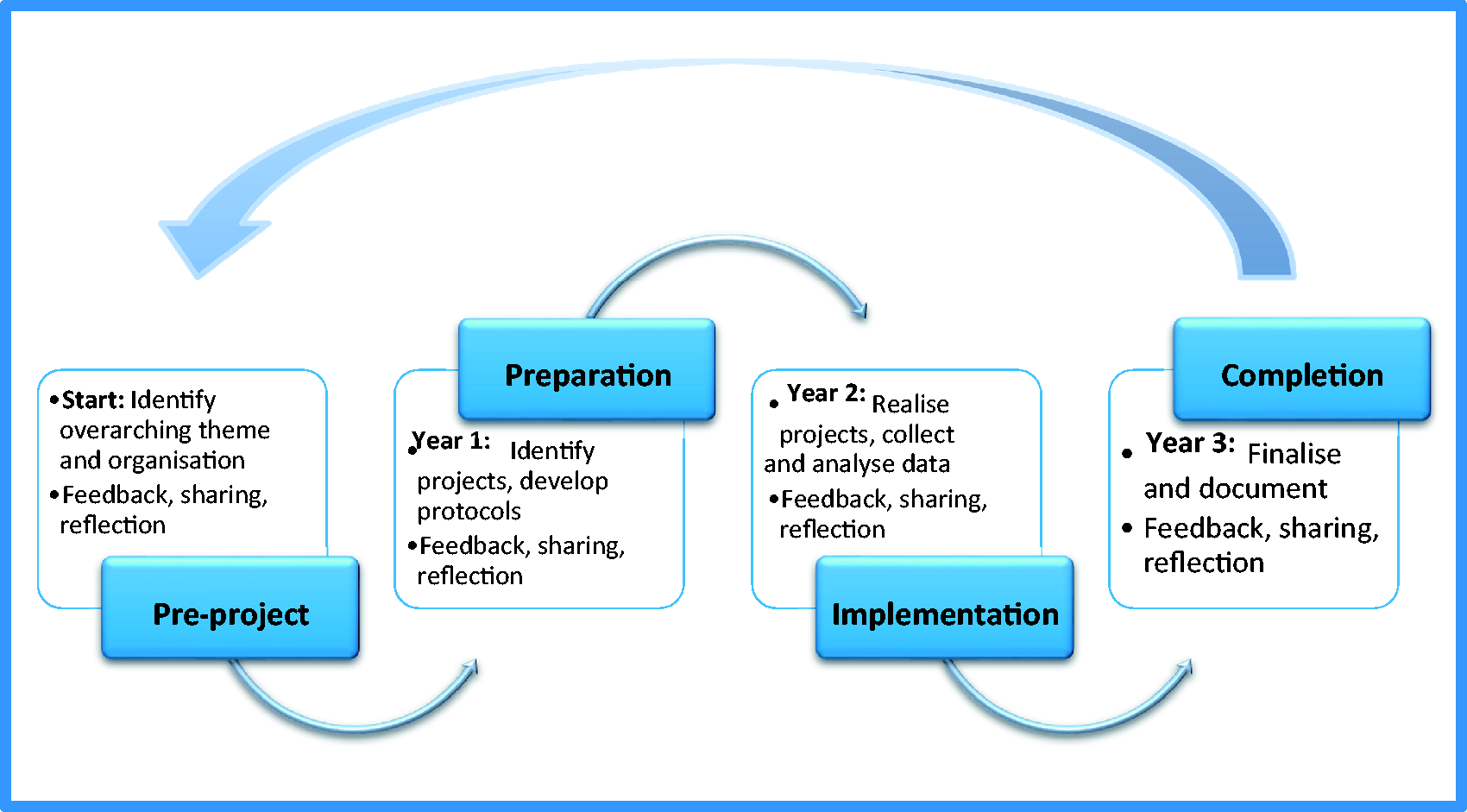
Agreement of a programme with an overarching theme (pre-programme)
Initially, ward managers discuss with the nurses what they currently find most important and relevant to explore, qualify and develop in practice. Ideas, topics and themes are also discussed in the steering group and in a forum of all nursing leaders, educators and clinical nurse specialists, and finally consensus determines which overarching programme theme is chosen as the overall ‘umbrella’ headline. As an example the three programmes completed since 2005 in the department had these overarching themes: ‘Young people with cancer’, ‘Relatives and the cancer patient’s social network’ and ‘Future cancer care – short but high quality’. These projects were supervised in close dialogue with academic colleagues.
The umbrella holders (pre-programme)
The programme is facilitated by one or two umbrella holders/programme facilitators. The facilitator is a nurse with academic competencies preferably at doctoral level, who is responsible for organising the programme, including informing, teaching and supervising, arranging all-day meetings twice every semester, participating in meetings with the steering committee and editing the book published about the completed programme and single projects.
The first programme was facilitated by an associate professor (second author). The second programme had an overlapping phase of one year with two facilitators (both authors). This was in order to secure a smooth transition of roles while the second author completed her PhD. The second author now shares the role as umbrella holder/programme facilitator with a nursing colleague with a master’s degree.
The programme participants (pre-programme)
Each ward/unit decides a specific topic that fits into the overarching theme which is relevant for their local context, their practice or group of patients. One, two or a group of clinical nurses/staff sign up and become responsible for carrying out the project in their ward/unit. The member of staff engaged have usually had no further formal education since graduation in nursing.
Formal research studies such as PhD or post doc studies can be part of and gain from participation in the programme. This was, for instance, the case for the current umbrella holder (first author) who conducted her PhD under the first theme/umbrella.
Initiating and planning of each single project (preparation – first year)
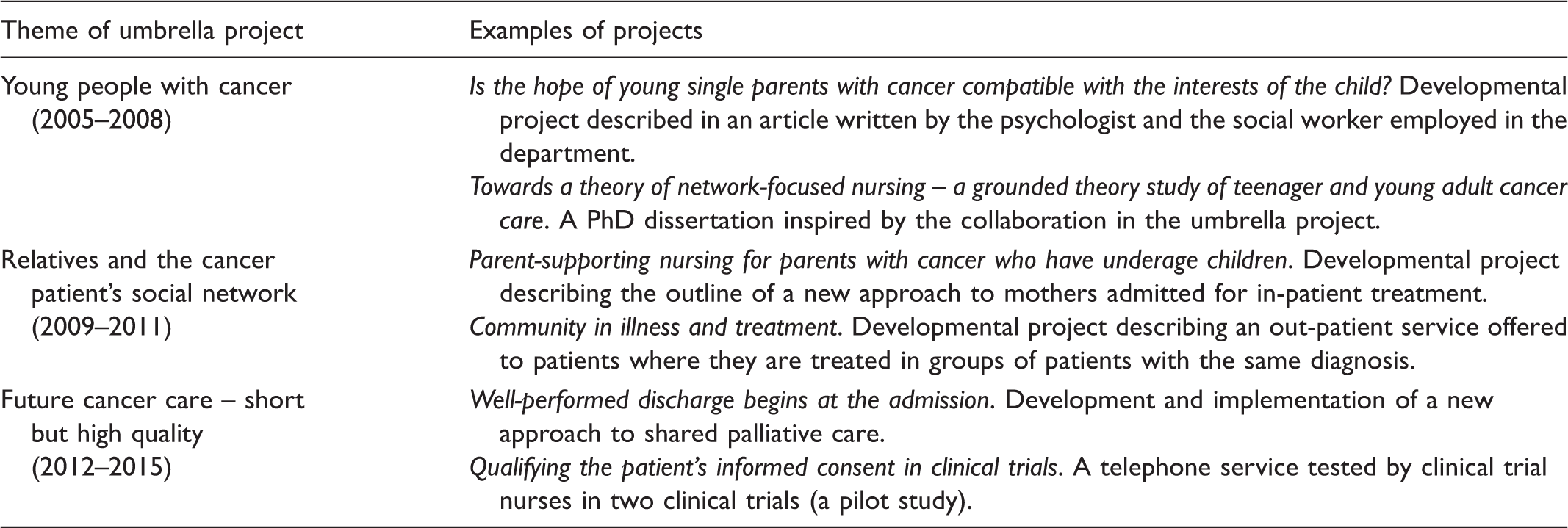
Examples of projects performed in each of the three umbrella programmes.
Collective reflections, inspiration and sharing experiences (preparation – first year)
In parallel with working on their protocols and projects the nurses participate in two all-day meetings in each semester, where they meet with each other, their ward managers and supervisors. The meetings are facilitated by the umbrella holder(s). In accordance with action learning principles,8,12 these meetings aim to support inspiration and networking between the participants, to allow them to share reflections and learn to give and receive constructive input, feedback and support. The meetings are the cornerstones of the development process in creating a progressing spirit within the programme. They create the experience of working on a collective programme, and it is here that potential, ideas, and barriers are shared and reflected on across the department and in dialogue with leaders.
Ward manager and supervisor participation in these meetings is important. It shows their commitment to and support of the programme. This attention stimulates the nurses’ motivation to carry out the projects. One ward manager expressed it like this: I experienced that we leaders profited from our participation [in the all-day meetings] because the education was very relevant and because it made us stay in touch with the development in all parts of the department when we exchanged knowledge and experiences with the projects. The programme became our project. The strong support from the leaders influenced the participating staff and made it easier for them to conduct the projects. (authors’ translation)13(p.147) I have learned a lot and have gained from participating in the planned meetings where we had excellent opportunities to get response and constructive input from the other participants in the programme. (Nurse A) (authors’ translation)7(p.218) It has been inspiring to follow the other participants’ projects … [and] it has given us who have participated a better understanding of the work conditions and what is going on in the other units. (Nurse B) (authors’ translation)7(p.218)
Supervision (preparation – first year)
To support the writing of protocols, the nurses follow the same guidelines. The supervisors actively engage in the projects by supervising the writing of protocols and the final reports in order to develop the nurses’ competencies in for example literature searching and clarifying purpose and aims in the projects. They also ensure that both research and experiential evidence are included to structure the background of each of the protocols, and make certain that plans are realistic. When the protocols are completed and final drafts approved, implementation of the projects can start.
Realising the single projects (project implementation – second year)
During this phase, the nurses realise their projects. Depending on possibilities in the specific wards and on appointments with the ward managers, the nurses get on average one day off duty per month to work on their projects and they continue to meet with all active members in the programme twice every semester.
From the second phase of project preparation and through the third phase of project implementation it is crucial that the nurses make an effort to keep their colleagues informed and engage them in reflecting on the learning and knowledge gained through the projects. This can create the best possible foundation for change and the implementation of new approaches, interventions and actions in clinical practice.
Finalising and writing up the single projects (completion – third year)
The implementation of the projects continues into the completion phase, and during this year the programme is finalised. Each project is evaluated in relation to its purpose and aims. Often the nurses write up a report or an article which is presented to and discussed with their colleagues. During this discussion, it is collectively decided how to use the results of the project and whether certain aspects or practises should be implemented to clinical practice.
All participants write up their projects as articles or book chapters for publication in a book about the completed programme. Some have succeeded in writing professional or research papers for national and international journals. The books have shown to be cornerstones in the development of the programmes, for, as burdensome it may seem to write articles and chapters, and sometimes about projects that have failed, the satisfaction and pride that is expressed by all programme members the day they hold the book in their hands speaks for itself.
At the end of the third year, a nursing symposium takes place in the department. Here, the completion of the programme is celebrated, the published book is presented and the nurses orally present their individual projects. A press release about the main programme and the book is sent to the media. As a consequence, all hospital staff are informed, as is the public through the Internet, the hospital Intranet, newspapers and local radio programmes.
Achievements
After the completion of three programmes following the Umbrella Model, achievements can be divided into four main areas, a) single projects, b) publications, c) synergy and implementation, and d) development of competencies.
Single projects
In the first programme ‘Young people with cancer’, eight projects involving 11 nurses and other healthcare professionals had protocols accepted. Seven projects were completed. One project was not completed due to lack of resources in the unit.
In the second programme ‘Relatives and the cancer patient’s social network’, eight projects involving 15 nurses had protocols accepted. Seven of the projects were completed. In addition to the programme, a course for nurses becoming Family/Relatives Ambassadors was established and a paragraph for the patients’ relatives was added to the department’s web page. One project was not completed because it turned out not to fit the patients’ spouses’ needs.
In the third programme ‘Future cancer care – short by high quality’, eight projects involving 20 nurses had protocols accepted. They were all completed.
Publications
The three programmes based on the Umbrella Model have led to publication of professional articles as well as research articles in international journals,14–18 three books7,13,19 and one PhD dissertation. 20 The majority of the professional articles published in national journals were written by nurses who had never published before. The projects, programmes and the Umbrella Model have been presented a number of times at local symposia, and at national and international meetings.
Synergy and implementation
The feedback from programme participants, nurses, managers and supervisors indicates that the all-day meetings, sharing ideas, networking and reflecting on possibilities and barriers were cornerstones of developing a shared programme identity. This is in accordance with Revans’ description of action learning as a reflection-in-action approach, embedded in group settings characterised by a safe environment. 8
The projects raised attention to several new perspectives and produced reflections and discussions among the staff. In that respect, the reflections worked as ‘eye openers’. We [social worker and psychologist] represent two different professional approaches. These are to some extent in agreement but are significantly different in aim, methods and theoretical assumptions. Our cooperation has therefore caused interesting and fruitful discussions. (authors’ translation)13(p.219)
Development of competencies
The design of the umbrella programmes made it possible for staff at many levels to gain new competencies. Nurses who had never participated in structured projects before learned to write a project proposal, search literature and work in depth with a clinical problem. They conducted interviews, made participant observations, wrote professional articles and presented their projects orally and on posters. They learned to take responsibility for a project in their own clinic and to engage their colleagues in focusing on the issues involved. They also became more aware of their department as an organisation and the importance of their contributions for the further development of high quality care. Encouraged by the success of their projects and the new skills learned, some nurses were motivated to enrol in education at postgraduate level. From a leader’s perspective it is wonderful to see engaged staff and how competencies develop among the project active members, but it is, in particular, positive to see how the quality of care raises when the professional development happens to all staff members. (Ward manager) (authors’ translation)13(p.148)
In addition nurses with academic backgrounds were further trained as supervisors, umbrella holders and researchers, and nurse leaders gained more insight into the complex dynamics of large projects.
The projects have drawn nurse leaders’ attention to the pivotal role they play in building a learning environment that supports project engagement and a constant focus of the staff on the topic chosen. They have also resulted in a common experience of the need for sharing across the wards and units in the department.
The umbrella holders for their part have, through this model, found a way to support interaction and knowledge exchange between academia and clinical practice. They have supplied their academic competencies with skills to lead professional development in large groups, to keep up the spirits and motivation of the staff involved and used their skills to edit books for publication.
Discussion
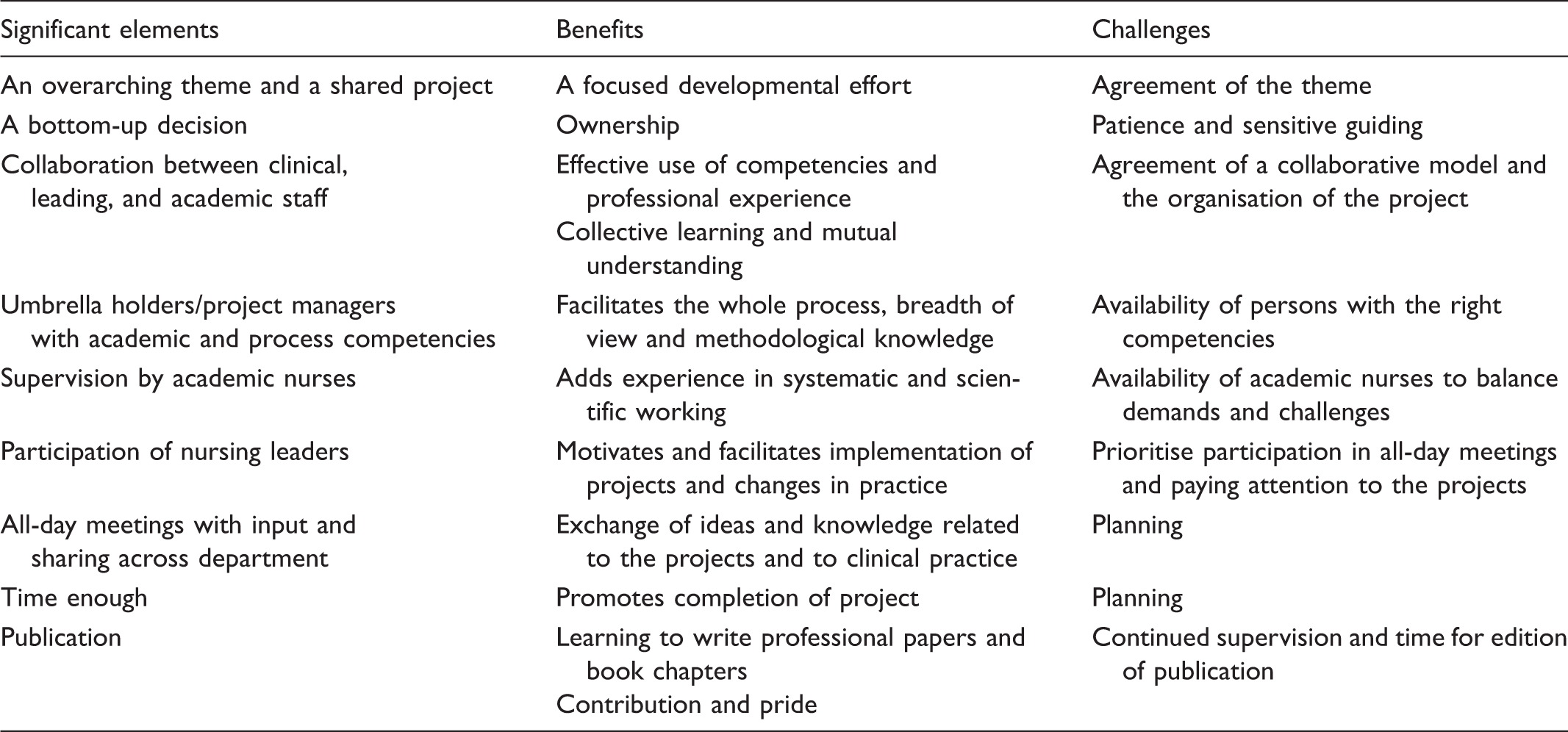
Significant elements, benefits and challenges of the Umbrella Model.
The agreement of programmes with overarching themes encompassing the entire department has created a shared direction and the experience of moving together. The simultaneous bottom-up approach in the single projects has founded ownership and all the reflection and learning processes have been essential. Owing to this, knowledge has spread in the organisation and founded the basis for development and planned change. These elements are similar to the shared vision and team learning characteristic of organisational learning.22,23
The all-day meetings have a central role and reflect collaborative action learning programmes. 12 When staff, during the meetings, share experiences, processes and lessons learnt with each other, their leaders and supervisors, they build a network, common consciousness and knowledge. Further, these dialogues have the potential to elevate participants’ understanding to a higher level of abstraction and thereby exceed the concrete situations. 24 In this way, reflection is created ‘in action’ collectively 8 and simultaneously forms a base for change and development in the organisation.
As recommended by Rycroft-Malone, 4 the Umbrella Model aims at taking the simultaneous relationship between evidence, context, and facilitation of implementation processes into account. However, it must be recognised that though results of action learning have potentially greater possibility to be implemented in practice, the model does not guarantee that this will happen. There is a need for leaders at all levels of the organisation to consciously and continuously adhere to implementation plans and to try to secure the context and facilitation necessary – also after the completion of the three-year programmes.
In concordance with action learning, it is crucial that the overarching programme theme refers to clinically relevant challenges experienced by the leaders and participating nurses in their day-to-day practice. Likewise that the programme has momentum, meaning that participants experience the movement of the project in both speed and direction. 25 Three years is a long time to keep up engagement and many changes can influence the completion of single projects. The timeline of an umbrella programme must be based on local possibilities and staff competencies; however, it is important that processes are not forced or incompatible with the clinic. The management of the programme is the responsibility of the umbrella holders with back-up from the steering committee. They need to be capable of sustaining the aims, maintaining meaningfulness and keeping the programme on the track.
Action learning approaches have been described to generate learning skills which make individuals capable of handling complex situations in the future and, consequently, support individual and organisational learning.26,27 By bringing novice and experienced practitioners, clinical experts, leaders and researchers together, the Umbrella Model seems to have supported progress for individual as well as collective learning. However, when staff did not have either postgraduate educational training or had demonstrated interest and skills in working systematically with practice development, the process was considerably more difficult.
Conclusion
A shared theme that overarches several minor projects in the organisation is the core of the Umbrella Model. Research and developmental projects are often separated in clinical practice and placed on different levels in the evidence hierarchy. 28 The Umbrella Model aims at bridging this separation by bringing both kinds of projects together.
After the first programme was completed, the model was demonstrated to be sustainable through the following two programmes in the same department. The dynamic nature of the model allows it to continually develop and adjust in accordance with feedback from participants and the steering committee. In all three programmes, approximately 46 staff members – mainly nurses – from eight in-patient and out-patient units in total have accomplished 22 large or small single projects as part of the Umbrella Model.
Thus the projects under the Umbrella Model have produced new knowledge, learning strategies and processes and by doing so developed nursing care in close collaboration with local needs, and in partnership between clinical nurses, nursing leaders and academic nurses. Project participants have been included in all phases of the process – from identifying relevant questions, planning the projects, collecting and analysing data, informing and sometimes transforming the findings into new methods in practice. The Umbrella Model has not been used as part of a formal educational programme, however, its potential to informally train the staff in systematic work, has indeed contributed to the participants’ competencies. The programmes have had a clear organisation and the fact that multiple minor projects were performed under the same overarching theme strengthened the learning process and the feeling of moving forward collectively and in the same direction.
The aim of this article was to support and guide the implementation of the Umbrella Model in other organisations by introducing details of its fundaments and phases. Though the Umbrella Model has been shown to be useful in structuring development projects and processes in a large organisation, it can be further cultivated and shaped to fit other settings.
Footnotes
Acknowledgements
Thank you to former Chief Nursing Officer Kirsten Bruun Hermansen and former Matron Inger Vithen at Aarhus University Hospital, who back in 2005 believed in the potential of the Umbrella Model and offered financial support and staff resources to conduct the first umbrella project and development of the model. Thank you also to Professor Julie Taylor, University of Birmingham, UK, for fruitful comments on this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.