
Abstract
“Sandwich grandparents” are middle-aged and older adults who have both living parents (or parents-in-law) and young grandchildren. They are faced with competing demands for caregiving from multiple generations. This study examines the prevalence, trends, and patterns of caregiving by sandwich grandparents in China. Drawing on nationally representative longitudinal data, this study estimates that more than 150 million Chinese adults aged 45 and older were sandwich grandparents in 2011. Among them, more than 17 million were dual caregivers who provided care to their own older parents and young grandchildren simultaneously. These numbers fluctuated considerably between 2011 and 2018. This study further tests the associations between three aspects of intergenerational solidarity and caregiving patterns among Chinese sandwich grandparents. Longitudinal regression analysis reveals a significant association between normative solidarity and intergenerational caregiving, but no evidence of functional or structural solidarity at work.
Introduction
In the research on aging, the concept of the “sandwich generation” was originally used to describe middle-aged adult children who are under pressure to care for their dependent children and aging parents (Brody, 1981; Miller, 1981). However, older adults who are grandparents may also be sandwiched between older parents or parents-in-law (i.e. great-grandparents) and two younger generations (adult children and grandchildren). At least in developed countries, it is not a new phenomenon for grandparents to be members of four-generation extended families. For example, based on survey data from nationally representative samples collected in 1962, a cross-country study estimated that 40% of people aged 65 and older in the USA, as well as 23% in Britain and Denmark, respectively, were great-grandparents (Shanas et al., 1968: 141). Social gerontologists soon took notice and called research attention to middle-aged individuals who are faced with competing caretaking demands from their aged parents and young grandchildren (Townsend, 1968).
In recent decades, many important demographic changes have occurred in both developing and developed countries. These include, among others, increased female labor force participation, delayed marriage and childbearing, a declining fertility rate, and improved life expectancy. In the absence of quality, affordable childcare and old-age support, these demographic forces together have led to rising demands on “sandwich grandparents” caring for their older and younger relatives in the USA (Abramson, 2015), Europe (Huvent-Grelle et al., 2015; Luna et al., 2016, 2019; Železna, 2018), and China (Xu, 2019a). A study of 14 European countries estimated that nearly 30% of grandparents provided care to both great-grandparents and grandchildren, and those who cared for great-grandparents were, contrary to conventional wisdom, more likely to care for grandchildren, compared with those who did not care for great-grandparents (Železna, 2018). In China, recent estimates showed that more than one in four grandparents belonged to the sandwich generation, and among them, more than one in 10 were dual caregivers—providing informal care to both great-grandparents and grandchildren (Xu, 2019a).
Providing unpaid, informal care to family or extended-family members is commonly perceived as a stressor that, when prolonged, may have negative psychological, behavioral, and physiological effects on caregivers’ daily lives and health (Pearlin et al., 1990; Pine and Steffen, 2019). Several studies have explored the health risks faced by sandwich grandparents in France (Huvent-Grelle et al., 2015), Spain (Luna et al., 2016, 2019), and China (Xu, 2019a; Xu et al., 2022). However, not all sandwich grandparents are involved in intergenerational caregiving. Some of them may be dual caregivers—providing care to both their older parents and grandchildren simultaneously, while others may not provide any intergenerational care at all. With a focus on health outcomes, the handful of studies of sandwich grandparents have largely ignored the underlying process through which sandwich grandparents self-select into different states of intergenerational caregiving.
This study adopts a four-generation perspective to document the patterns of intergenerational caregiving and to examine the associated factors among Chinese sandwich grandparents. Situated in the Chinese context, this study applies the framework of intergenerational solidarity and tests three hypotheses related to family values (normative solidarity), time-for-money exchange (functional solidarity), and health selection (structural solidarity).
Theoretical background
The framework of intergenerational solidarity was originally developed to describe relationships between older parents and adult children in aging families (Bengtson and Roberts, 1991). However, it can also be applied to the study of the sandwich generation's involvement in intergenerational caregiving activities. For example, previous studies from Great Britain and the USA have shown that late-middle-aged parents provide help (e.g. money, help with chores, grandchild care) to both their own older parents and adult children when they have a strong sense of family solidarity, close intergenerational ties, or are influenced by cultural expectations (Grundy and Henretta, 2006; Henretta et al., 2002). In their revised conceptual model, Bengtson and Roberts (1991) proposed six dimensions of intergenerational solidarity, namely association, affection, consensus, resource sharing (or functional solidarity), the strength of familism norms (or normative solidarity), and the opportunity structure for interaction (structural solidarity). Among them, normative solidarity, functional solidarity, and structural solidarity are most relevant to this study. Unfortunately, the survey data used in this study do not include any measure of affection or consensus, while association was embedded in caregiving activities.
Normative solidarity
Normative solidarity refers to the degree of commitment to embracing family values, to performing familial roles, and to fulfilling culturally prescribed obligations to family members (Bengtson and Roberts, 1991). In the Chinese context, filial piety is arguably the fundamental value that defines traditional family relationships. Rooted in the Confucian ideal of familial interdependence, filial piety is a family value based on the principles of hierarchy, obligation, and obedience (Xu, 2019b). It stipulates that children are obligated to obey their parents and provide old-age support to them. After 1949, filial piety as a Confucian ideology was not denounced. Instead, due to the lack of social welfare programs for older adults, the traditional practice of filial piety was reinforced by the enactment of marriage and family laws which mandated that adult children provide instrumental, financial, and emotional support to their aging parents. (Luo and Zhan, 2012). Therefore, despite their own aging challenges, in accordance with the cultural mandates of filial piety, there has been a strong expectation that sandwich grandparents will take care of their older parents in four-generation families.
On the other hand, the traditional practices of filial piety have been challenged by dramatic demographic and socioeconomic changes since China's market-oriented reform was launched in the 1980s. For example, the traditional notion of filial piety emphasizes upstream support from adult children to their elderly parents and does not charge grandparents with primary responsibility for the care of grandchildren (Short et al., 2001). However, in recent decades tens of millions of children have been left behind in the countryside by their rural-to-urban migrant parents because hukou (household registration)-based institutional barriers prohibit them from enrolling in public schools or enjoying other social welfare benefits enjoyed by their urban peers (Xu and Xie, 2015). As a result, rural grandparents are often forced to provide custodial care for their “left behind” grandchildren (Xu, 2022). Nevertheless, the arrangement of such intensive intergenerational care is meant to promote the well-being of the extended family as a whole, and therefore is still consistent with the traditional doctrine of maintaining strong intergenerational ties in Chinese families (Chen et al., 2011; Luo and Zhan, 2012). One study found that older parents in inland rural China did not perceive their children as less filial due to their having migrated away for work (Luo and Zhan, 2012).
Other scholars argue that the practice of filial piety continues to evolve. For example, despite rapid industrialization and modernization, Chinese parents remain influential in adult children's choices of dating and provide financial support for their marriages (Xu and Peng, 2021). In return, adult children provide social and emotional support to their aging parents, who value intergenerational solidarity and continuity of the family lineage more than economic support from adult children (Liu, 2021). Changing practices of filial piety may be more prevalent in urban Chinese families, but evidence of significant rural–urban differences in grandparenting norms is limited (Choi and Zhang, 2021). With such strong cultural impetuses at work, intergenerational care provided by sandwich grandparents can be unconditional and not tied to, for example, receiving financial compensation from older parents or adult children. To the extent that Chinese families still value filial piety and close intergenerational ties as important family norms and that providing intergenerational care is consistent with these norms, the notion of normative solidarity predicts that:
Functional solidarity
Functional solidarity refers to sharing resources and exchanging financial, physical, and emotional assistance between generations (Bengtson and Roberts, 1991). In the contemporary Chinese context, many researchers have noticed a family model of intergenerational time-for-money exchange in which grandparents spend time providing grandchild care to allow their adult children to seize economic opportunities and thus to contribute to the material well-being of the grandparents through reciprocal transfers of money or living necessities (Cong and Silverstein, 2011; Sun, 2002). Financial support from adult children is particularly important for Chinese grandparents in rural areas, where the poverty rate remains high and a formal social security system is absent. Using data from a rural region in China with massive labor force migration, several studies found that the amount of grandchild care provided by grandparents was positively related to the amount of remittance received from their migrant children, which in turn not only improved their nutrition and physical health by allowing them to purchase food and afford health care, but also improved life satisfaction and reduced depressive symptoms (Cong and Silverstein, 2011; Silverstein et al., 2006).
In urban China, the public pension is generally available, but daycare services are less accessible or affordable. Grandparents can help their daughters or daughters-in-law remain in the labor market by taking care of their grandchildren during working hours. One study estimated that the labor force participation rate of urban Chinese mothers increased by 24%–29% with access to daycare services and by 38%–43% with access to childcare provided by grandparents (Du et al., 2019). Even though urban grandparents are less likely than their rural peers to need or receive financial support in exchange for grandchild care, they still enjoy the emotional and psychological benefits of having regular intimate interactions with adult children and grandchildren (Xu, 2019a). However, it is unclear what resources sandwich grandparents may receive for caring for their older parents, other than emotional benefits. Therefore, the notion of functional solidarity predicts that:
Structural solidarity
Bengtson and Roberts (1991) originally defined structural solidarity as the opportunity structure for intergenerational relationships reflected in the number, type, and geographic proximity of family members. They also proposed three empirical indicators of structural solidarity: the residential proximity, number, and health of family members. However, geographic proximity is often viewed as a precondition of intergenerational caregiving and treated as a control variable in empirical research, whereas the number of family members and the health of caregiving family members are intrinsic to understanding the self-selection into caregiving and the health implications of being a caregiver (Liu and Chen, 2022; Xu, 2019a). Therefore, this study will focus on the number of family members and the health of grandparents as the main indicators of structural solidarity and predicts that:
Data and methods
Data and sample
Individual-level data were drawn from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative longitudinal survey of adults aged 45 or older and their spouses, if available. CHARLS sampled 17,708 residents from 150 counties across 28 provinces in China, with a response rate of 80.5%, in 2011. This study focuses on the CHARLS respondents aged 45 or older who were grandparents sandwiched between their older parents or parents-in-law (i.e. great-grandparents) and young grandchildren (under age 16). This age restriction is similar to previous research on Chinese grandparents using the CHARLS data (Choi and Zhang, 2021; Ko and Hank, 2014; Liu and Chen, 2022), since younger respondents are unlikely to be grandparents.
National follow-up surveys of CHARLS have been carried out in 2013, 2014, 2015, and 2018. However, the 2014 wave was devoted to collecting retrospective life history data, and the 2015 wave did not collect data on caring for older parents. Therefore, this study only draws on data from the 2011, 2013, and 2018 waves to describe the trend in intergenerational caregiving among sandwich grandparents over time. There were 16,574 respondents aged 45 or older with valid information about their family members in the CHARLS baseline survey. Among them, only 4824 (29.1%) respondents were sandwich grandparents who had at least one living parent or parent-in-law and at least one grandchild under age 16 at the time of interview, irrespective of coresidence. This number dropped to 1920 (out of 14,539, or 13.2%) in 2013 and increased to 4106 (out of 17,202, or 23.9%) in 2018. The fluctuation in the number of sandwich grandparents was due to longitudinal sample attrition in 2013 (about 12%) and refreshment sampling in 2018 (about 32%), as well as transitions into or out of the sandwich generation (e.g. via the death of older parents or the aging out of young grandchildren; about 48%).
For longitudinal regression analysis, only data from Waves 1 (year 2011) and 2 (year 2013) were used because the time gap between Waves 2 and 4 (year 2018) was too wide to consider independent variables measured at Wave 2 as appropriate predictors for caregiving status reported at Wave 4. Among the 1920 sandwich grandparents aged 45 or older at Wave 2, there were 457 new respondents who did not participate in the baseline survey and thus had completely missing data on their baseline characteristics. Another 120 respondents were excluded due to missing data on one or more independent variables, resulting in the final sample size of 1343 for longitudinal regression analysis.
Measures
The outcome of interest was sandwich grandparents’ self-reported family caregiving in the past year. In every wave except 2014, respondents who had any grandchildren under age 16 were asked whether they spent any time taking care of their grandchildren in the past year. Respondents were also asked whether they took care of their parents or parents-in-law in the past year (except in the 2015 wave). A multicategorical variable was constructed to distinguish four types of intergenerational caregiving among the sandwich grandparents: not a caregiver, caring for grandchildren only, caring for older parents (i.e. great-grandparents) only, and caring for both grandchildren and older parents (i.e. dual caregiving). Those who provided any intergenerational care were further asked how many weeks and how many hours per week they spent caregiving. However, previous research has expressed concerns about both the accuracy and the reliability of the self-reported time spent caregiving in CHARLS, which led to a large amount of missing data (Falkingham et al., 2020; Liu and Chen, 2022; Xu, 2019a).
As a proxy for normative solidarity, family values were captured by a vignette question about preferred intergenerational living arrangements. In both Waves 1 and 2, respondents were asked about preferred living arrangements for two hypothetical older persons. The first hypothetical person was described as an older person who had a spouse and adult children and maintained good relationships with the adult children, while the second hypothetical older person had no spouse (presumed to be deceased) and only adult children and maintained good relationships with them. For each vignette, respondents were asked to choose what the best living arrangement would be for the hypothetical older person. The choices included living with adult children, living in the same community or village with adult children but not in the same house, living in a different community or village from adult children, living in a nursing house, and other unknown options. The vignettes could capture respondents’ family values because living with adult children is consistent with the traditional norm of multigenerational coresidence, whereas living in different households or even different communities reflects a more modern value of independent living in old age. Given the description of no spouse in the second vignette, it was not surprising that more than two-thirds of the respondents preferred the scenario in which the older person would live with adult children and another 20% preferred that they live in the same community or village. Therefore, only the first vignette was used to construct a categorical variable with three values after combining several response categories with small sample sizes: multigenerational coresidence (i.e. living with adult children), living nearby (i.e. in the same community or village), and living far away.
As a proxy for functional solidarity, intergenerational transfer was measured by the financial support sandwich grandparents received from older or younger relatives in exchange for providing intergenerational care. In Wave 1, respondents were first asked whether they had received any economic assistance from their parents (or parents-in-law), adult children, or grandchildren, respectively, in the past year. If yes, respondents were then asked to report the amount of monetary support (in Chinese yuan) and to estimate the cash value of in-kind support (e.g. food, clothes) they received. Starting in Wave 2, respondents were directly asked to report the amount of monetary support and to estimate the cash value of in-kind support they received from their parents (or parents-in-law), adult children, or grandchildren, respectively, in the past year. The distribution of the reported cash value of both monetary and in-kind support was highly skewed with excessive zeros and outliers. Therefore, two dichotomous variables were created to indicate whether a respondent received any economic assistance (monetary or in-kind) from parents (or parents-in-law) and adult children (or grandchildren), respectively, in the past year.
Structural solidarity was measured by the number of living children, the number of living siblings, and the sandwich grandparents’ health. The latter was assessed by self-reported health indicators and behaviors. Self-rated general health status was measured on a 5-point Likert scale, ranging from “very poor” to “very good”. The number of mobility limitations was coded as a seven-item summary of any difficulty with mobility activities, which included walking 100 meters, climbing several flights of stairs, getting up from a chair, stooping or kneeling, extending arms above one's head, lifting 10 kilograms, and picking up a small coin. A number of doctor-diagnosed diseases were coded as a 13-item summary of health problems diagnosed by a doctor, namely hypertension, diabetes, cancer, lung disease, heart disease, stroke, arthritis, dyslipidemia, liver disease, kidney disease, digestive disease, asthma, and psychiatric problems. Two dichotomous variables indicated whether a respondent had ever drunk alcohol (1 = yes, 0 = no) or smoked cigarettes (1 = yes, 0 = no), respectively.
Demographic and socioeconomic characteristics were controlled in longitudinal regression analysis. Demographic control variables included age, gender (male or female), marital status (currently married or not), and rural or urban household registration (hukou). Socioeconomic control variables included educational attainment (no formal education, primary school or less, middle school, and high school or above), employment status (not working, agricultural work, non-agricultural self-employed work, and non-agricultural employed work), and pension status (receiving pension or not).
Statistical methods
Given that the dependent variable was categorical, multinomial logistic regression was employed to examine the associations of intergenerational transfer, family value, and health selection with intergenerational caregiving status among sandwich grandparents while controlling for demographic and socioeconomic characteristics. Because respondents were asked about their caregiving activities in the past year, regressing the dependent variable on the independent variables measured in the same wave could be theoretically problematic. Therefore, the multinomial logistic models regressed the dependent variable measured at Wave 2 on the independent variables measured at Wave 1. Using the lagged independent variables also helps to alleviate the concern about potential reverse causality.
To account for the complex multistage, probability-proportional-to-size sampling scheme in CHARLS, Stata's survey data analysis commands were used for point estimation, model fitting, and variance estimation in descriptive and regression analysis (StataCorp, 2021). Administrative villages in rural areas and neighborhoods in urban areas were specified as the primary sampling units, and longitudinal weights were used to correct for nonresponse bias, sampling-frame errors, and sample attritions over time (Zhao et al., 2014). Standard deviations (in descriptive analysis) and standard errors (in regression analysis) were calculated by using the Taylor-linearized variance estimation method.
Results
Descriptive statistics
Table 1 reports the estimated numbers of sandwich grandparents with different intergenerational caregiving activities in 2011, 2013, and 2018, respectively. A total number of 150,699,202 (or 29.7%; 95% CI = 130,336,086–171,062,316) adults aged 45 or older were estimated to be sandwich grandparents at the baseline. The prevalence rate of sandwich grandparents dropped sharply to 11.9% in 2013 and rebounded to 19.5% in 2018. A similar trend existed for grandfathers and grandmothers (see Appendix Table A1). Given the longitudinal nature of the CHARLS data, these fluctuations could be attributed to several factors including, among others, young grandchildren aging out, older parents dying, and sample refreshing.
Estimated prevalence rates of sandwich grandparents and caregiving patterns over time.
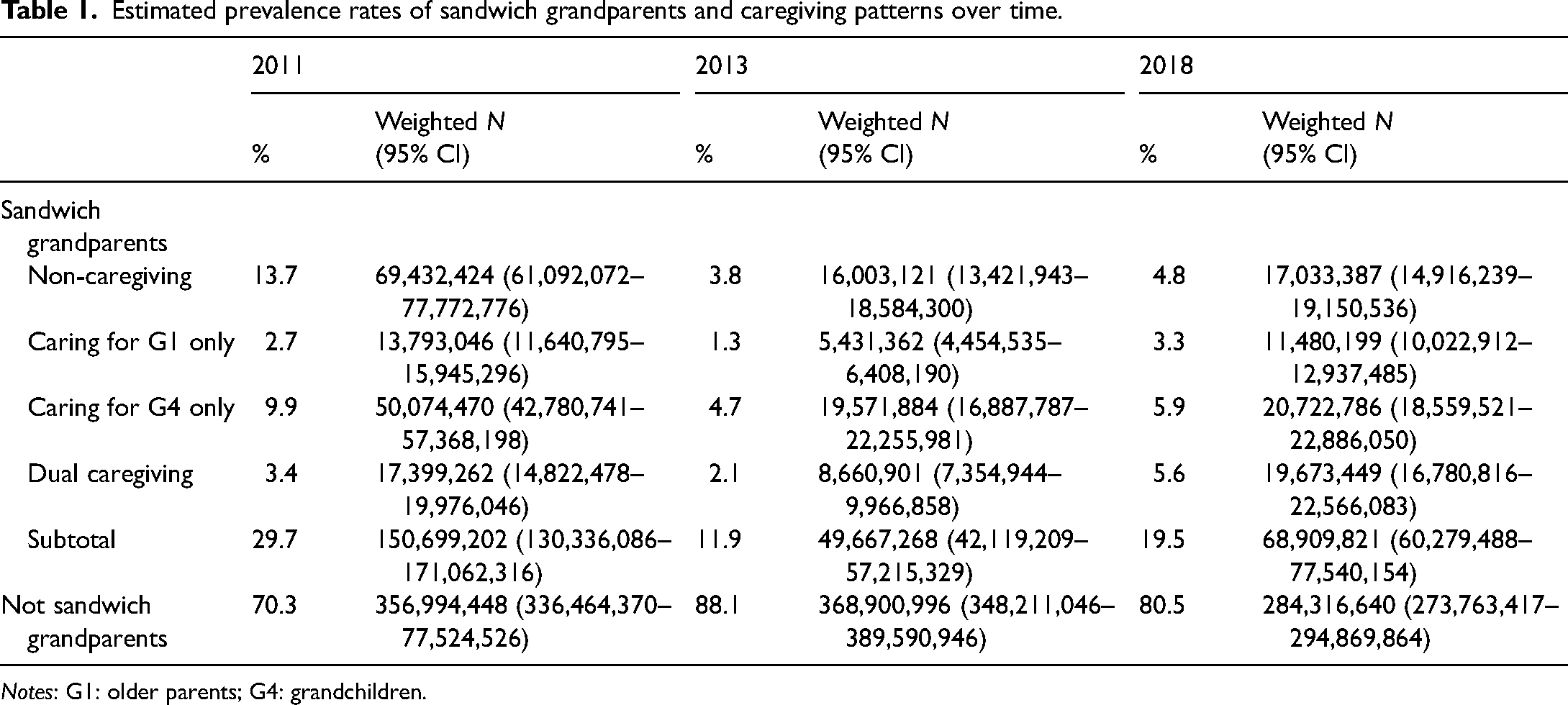
Notes: G1: older parents; G4: grandchildren.
Among the sandwich grandparents at the baseline, 69,432,424 (or 46.1%) did not care for older parents or grandchildren, 13,793,046 (or 9.2%) only cared for older parents, 50,074,470 (or 33.2%) only cared for grandchildren, and 17,399,262 (or 11.5%) provided care to both older parents and grandchildren. The proportion of non-caregivers declined over time as more sandwich grandparents became caregivers. By 2018, dual caregivers (28.5% of the sandwich grandparents) had outnumbered non-caregivers (24.7%).
Table 2 reports the descriptive statistics of the independent variables measured in 2011 and used in the regression models of the intergenerational caregiving status in 2013. These descriptive statistics were weighted, adjusted for survey design, and calculated for both the entire analytical sample and subsamples of four different caregiving status. Differences between subsamples were assessed by Wald tests (for continuous variables) and design-based chi-square tests (for categorical variables).
Descriptive statistics of the independent variables at Wave 1 (2011) stratified by caregiving status at Wave 2 (2013).
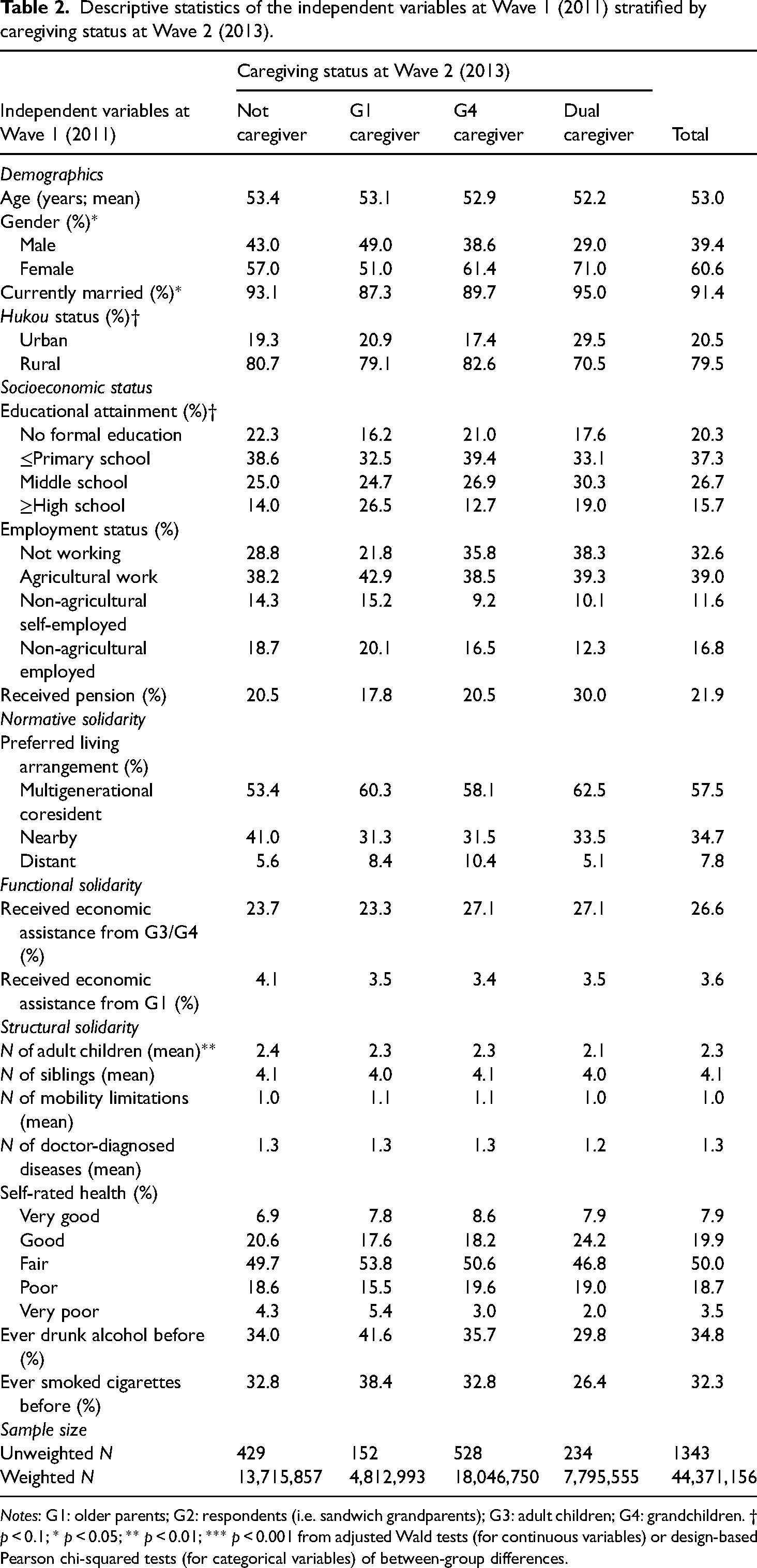
Notes: G1: older parents; G2: respondents (i.e. sandwich grandparents); G3: adult children; G4: grandchildren. † p < 0.1; * p < 0.05; ** p < 0.01; *** p < 0.001 from adjusted Wald tests (for continuous variables) or design-based Pearson chi-squared tests (for categorical variables) of between-group differences.
The sandwich grandparents in China were relatively young with an average age around 53 years. Given the typical gender gap in life expectancy, it was not surprising that sandwich grandparents were more likely to be women than men. However, there was a statistically significant difference in the gender composition by caregiving status. For example, the sandwich grandparents who provided care to older parents only were nearly gender balanced, with 49% being men and 51% being women. In contrast, 71% of the sandwich grandparents who were dual caregivers—providing care to older parents and grandchildren simultaneously—were women. The percentage of married grandparents ranged from 87.3% of those who only cared for older parents to 95% of dual caregivers, and this between-group difference was statistically significant. Most of the sandwich grandparents maintained rural household registration status, but dual caregivers had a higher percentage of urban-status households (29.5%) than the other subgroups (ranging between 17.4% and 20.9%). This between-group difference in household registration status was marginally significant.
Overall, the sandwich grandparents in China had low socioeconomic status. Only 26.5% of those who cared for older parents had received a high school or higher education, followed by dual caregivers (19.0%), non-caregivers (14.0%), and grandchild caregivers (12.7%). The between-group difference in educational attainment was marginally significant. About one-third of the sandwich grandparents were not working (e.g. unemployed, retired), and 39% were agricultural workers. Only 16.8% were employed and 11.6% were self-employed in non-agricultural sectors. Dual caregivers had a much higher percentage of pension recipients (30.0%) than the other sandwich grandparents (ranging between 17.8% and 20.5%), but this between-group difference was not statistically significant.
Turning to the key independent variables, most of them did not show any statistically significant difference between different subgroups of the sandwich grandparents. Regarding the vignette question about living arrangements, more than half of the sample (57.5%) preferred multigenerational coresidence, about one-third (34.7%) preferred living in the same neighborhood with adult children, and only 7.8% preferred living in a different neighborhood from adult children. Dual caregivers had on average significantly fewer children (2.1) than the other sandwich grandparents (ranging between 2.3 and 2.4), but they all had similar numbers of siblings (ranging between 4.0 and 4.1). About 26.6% of the sample had received any economic assistance from their adult children or grandchildren in the past year, and only 3.6% received any economic assistance from their older parents in the past year. On average, the sandwich grandparents reported about one mobility limitation (out of seven) and one doctor-diagnosed disease (out of 13). Half of the sample perceived themselves to be in fair health status, and about one-third had drunk alcohol and one-third had smoked cigarettes.
Regression results
Table 3 reports the coefficient estimates (log relative risk ratios) from multinomial logistic models of the associations between independent variables measured in 2011 and intergenerational caregiving status measured in 2013. The reference group was the sandwich grandparents who were not caregivers. There was strong evidence supporting Hypothesis 1 regarding normative solidarity. Those who preferred multigenerational coresidence were more likely to provide care to older parents (β = 0.437, p-value = 0.076), grandchildren (β = 0.345, p-value = 0.029), or both (β = 0.502, p-value = 0.017), compared with those who preferred to live independently (in the same neighborhood as adult children but different households).
Multinomial logit models (with adjustment for complex survey design) of intergenerational caregiving status among Chinese sandwich grandparents aged 45 or older.
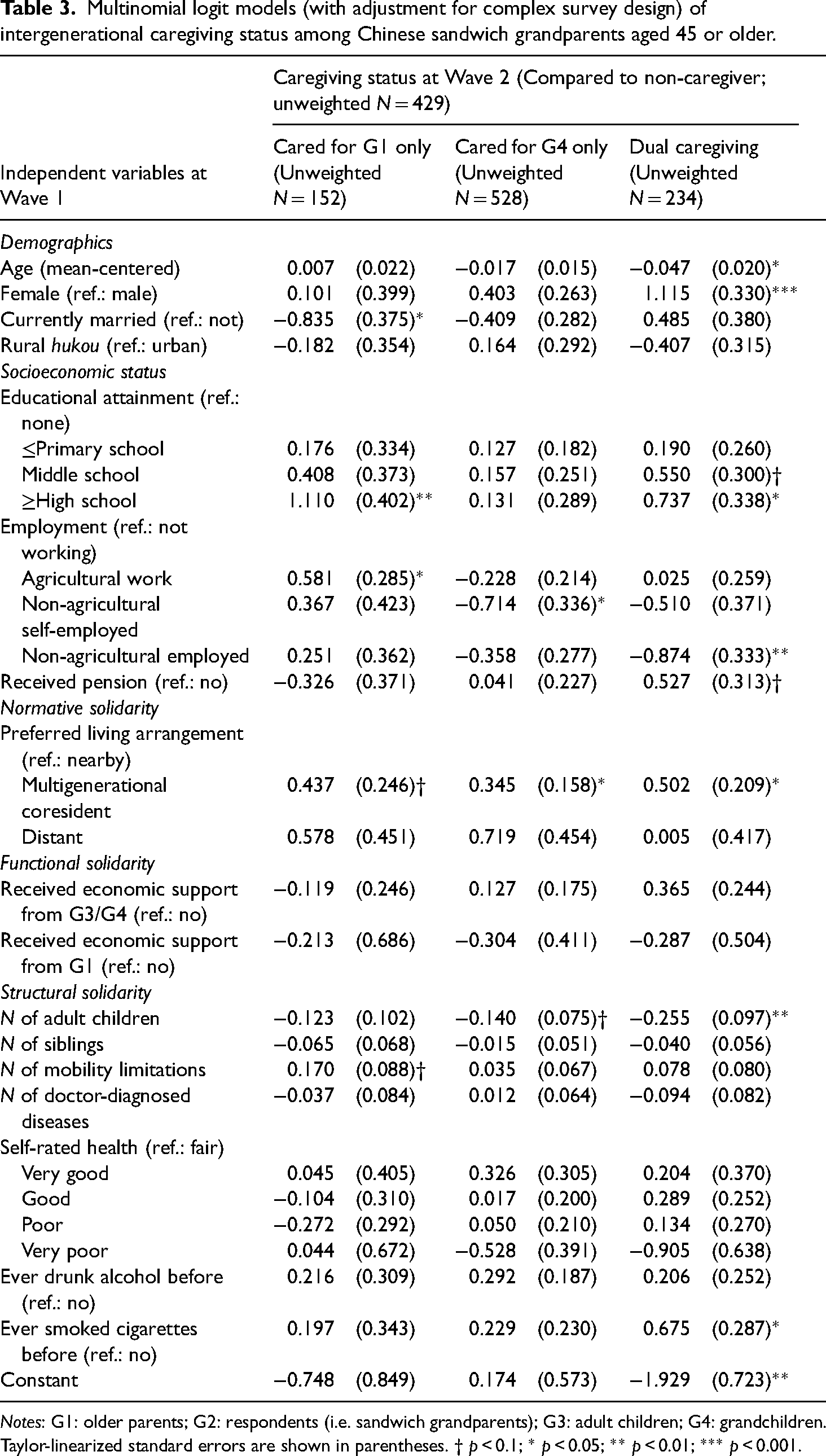
Notes: G1: older parents; G2: respondents (i.e. sandwich grandparents); G3: adult children; G4: grandchildren. Taylor-linearized standard errors are shown in parentheses. † p < 0.1; * p < 0.05; ** p < 0.01; *** p < 0.001.
There was no evidence supporting Hypothesis 2 regarding functional solidarity (i.e. time-for-money exchange in this case). Receiving economic support from older parents or adult children was not associated with a significantly higher likelihood of providing care to older parents, grandchildren, or both. There was also little evidence supporting Hypotheses 3–5 regarding structural solidarity. Contrary to Hypothesis 3, having more adult children was associated with lower odds of caring for grandchildren (β = −0.140, p-value = 0.065) or being a dual caregiver (β = −0.255, p-value = 0.009). It is possible that adult children help their siblings with childcare to reduce their older parents’ burden in providing intergenerational care. The number of siblings was not associated with the likelihood of providing intergenerational care, and neither were most indicators of health status. Surprisingly, the sandwich grandparents who reported a greater number of mobility limitations were more likely to provide care to their older parents (β = 0.170, p-value = 0.053), and those who had smoked cigarettes were also more likely (β = 0.675, p-value = 0.019) than non-smokers to provide care to both older parents and grandchildren.
Turning to the demographic control variables, older sandwich grandparents were less likely than their younger peers to simultaneously take care of older parents and grandchildren (β = −0.047, p-value = 0.017), while women were much more likely than men to be dual caregivers (β = 1.115, p-value < 0.001). Being married was associated with reduced odds of caring for older parents (β = −0.835, p-value = 0.027). In terms of the socioeconomic control variables, there was a positive association between educational attainment and being a caregiver. Most notably, sandwich grandparents who had received a high school or higher education were more likely to care for older parents (β = 1.110, p-value = 0.006) or to care for both older parents and grandchildren (β = 0.737, p-value = 0.030), compared with those who received no education at all. Compared with those who were not working, agricultural workers were more likely to care for older parents (β = 0.581, p-value = 0.042), non-agricultural self-employed workers were less likely to care for grandchildren (β = −0.714, p-value = 0.034), and non-agricultural employees were less likely to be dual caregivers (β = −0.874, p-value = 0.009). Lastly, receiving a pension was associated with higher odds of being dual caregivers (β = 0.527, p-value = 0.093).
Robustness checks
The first robustness check assessed the impact of using lagged dependent variables to account for temporal autocorrelation. Specifically, caregiving status at Wave 1 (2011) was added as an independent variable into the multinomial logistic regression model of caregiving status at Wave 2 (2013). It was worth noting that about 20.55% of the analytical sample (or 269 respondents) were not sandwich grandparents at Wave 1. As shown in Table 4, there was a strong autocorrelation between caregiving status at Wave 1 and that at Wave 2. Those who provided intergenerational care in any form at Wave 1 were very likely to remain as caregivers at Wave 2. For example, those who cared for their older parents at Wave 1 were almost seven times more likely to continue to do so at Wave 2 (β = 2.054, p-value < 0.001) than non-caregivers; similar trends were found for grandchild caregivers (β = 1.479, p-value < 0.001) and dual caregivers (β = 2.155, p-value < 0.001). In addition, providing care to older parents only or grandchildren only at Wave 1 was associated with higher odds of becoming a dual caregiver at Wave 2.
Multinomial logit models with lagged dependent variable (and adjustment for complex survey design) of intergenerational caregiving status among Chinese sandwich grandparents aged 45 or older.
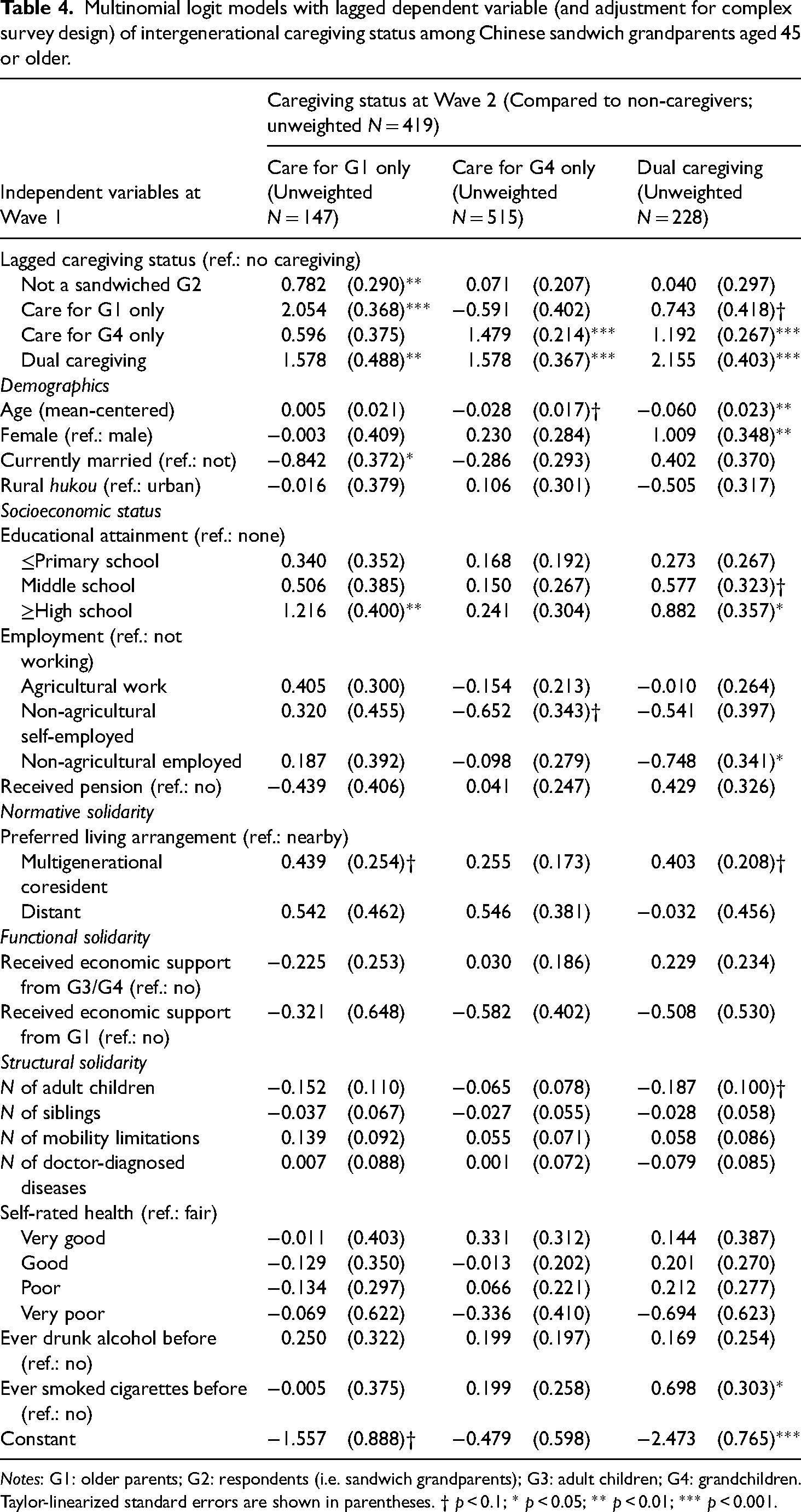
Notes: G1: older parents; G2: respondents (i.e. sandwich grandparents); G3: adult children; G4: grandchildren. Taylor-linearized standard errors are shown in parentheses. † p < 0.1; * p < 0.05; ** p < 0.01; *** p < 0.001.
Incorporating the strong autocorrelation of caregiving status into the regression model reduced the statistical significance of a few coefficients. For example, the number of mobility limitations was no longer associated with providing care to older parents, and preferring multigenerational coresidence was no longer associated with providing care to grandchildren. The number of adult children was no longer associated with providing care to grandchildren and only marginally associated with being a dual caregiver (β = −0.187, p-value = 0.100). However, smoking cigarettes remained a significant predictor of being a dual caregiver (β = 0.698, p-value = 0.022), and preferring multigenerational coresidence was still marginally associated with providing care to older parents (β = 0.439, p-value = 0.084) and being a dual caregiver (β = 0.403, p-value = 0.053).
The second robustness check evaluated the impact of sample selection. As mentioned above, because the analytical sample was restricted to the respondents who were sandwich grandparents at Wave 2 (when the dependent variable of caregiving status was measured), some of them (269 out of 1343) were not sandwich grandparents at Wave 1 and might represent a heterogeneous subgroup. As a sensitivity check, these respondents were dropped, resulting in a sample of respondents who were sandwich grandparents at both Waves 1 and 2. Despite the reduced sample size, the main findings remained robust (see Appendix Table A2). In fact, excluding these heterogeneous respondents increased the statistical significance of certain coefficients, especially those pertaining to the health selection hypothesis. The coefficient for the number of mobility limitations changed from marginally significant at the α = 0.1 level to significant at the α = 0.05 level. Those who self-rated as being in very poor health were significantly less likely to provide care to grandchildren (β = −0.886, p-value = 0.040), whereas those who had drunk alcohol were significantly more likely to take care of grandchildren (β = 0.495, p-value = 0.017).
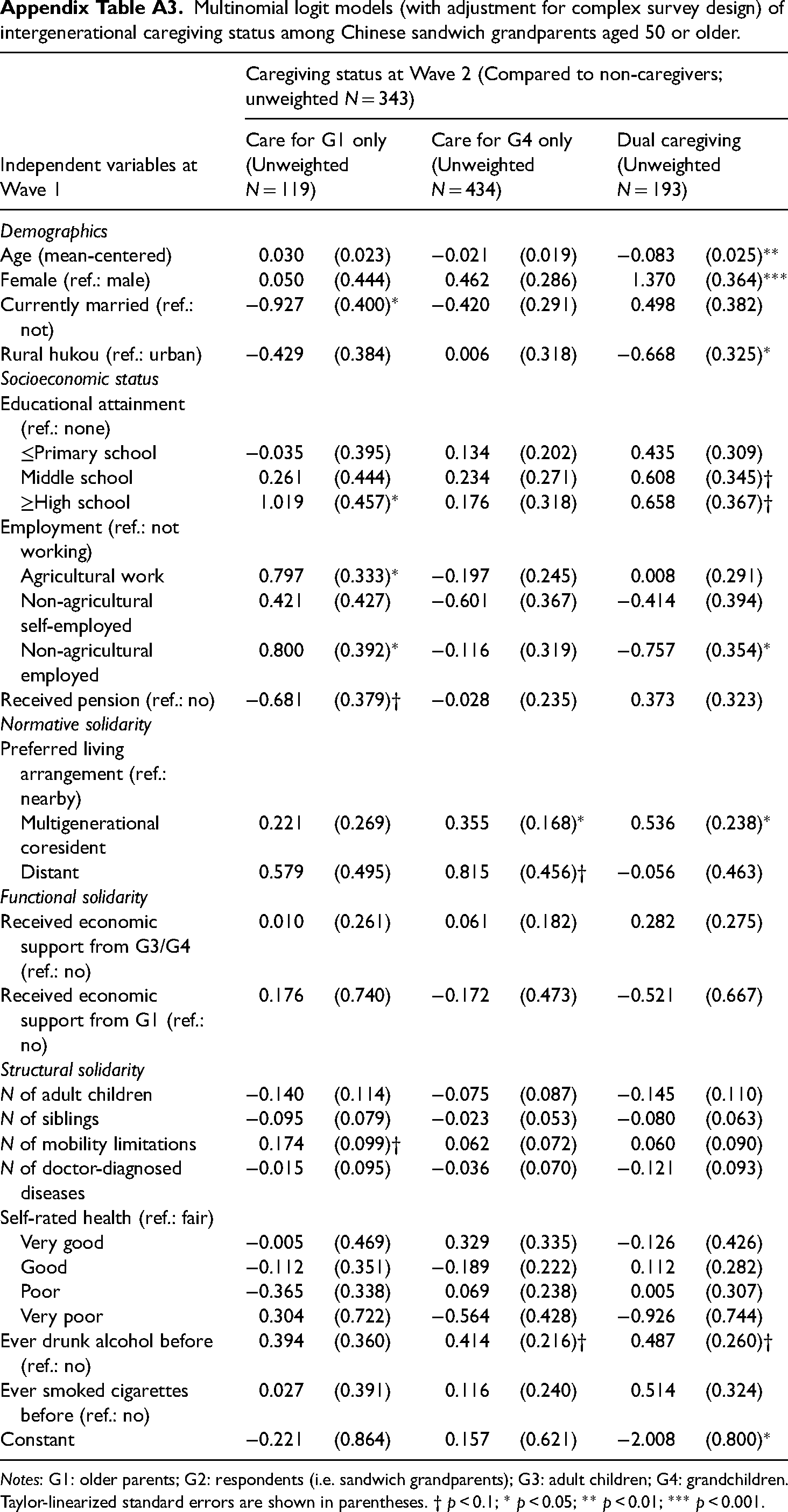
The last robustness check changed the age range of the sample from 45 or older to 50 or older. Under these conditions, intergenerational transfer was still not associated with intergenerational caregiving (see Appendix Table A3) and the number of adult children was no longer associated with intergenerational caregiving. As for health selection, smoking cigarettes was no longer associated with dual caregiving. However, drinking alcohol had marginally significant positive associations with caring for grandchildren and dual caregiving. Preferring multigenerational coresidence was no longer associated with caring for older parents, but it remained a significant and positive predictor of caring for grandchildren and dual caregiving.
Discussions and conclusions
As population aging accelerates, a new sandwich generation is on the rise. Grandparents are faced with competing demands for intergenerational caregiving from their grandchildren and their own older parents (i.e. great-grandparents) in the USA (Grundy and Henretta, 2006), Europe (Silverstein et al., 2020), and China (Xu, 2019a). Using demographic microsimulation, one recent study estimated that about 46% of the global population born between 1970 and 2040 would at some point become sandwich grandparents (Alburez-Gutierrez et al., 2021). Drawing on nationally representative data, this study contributes to the literature by estimating the trends in intergenerational caregiving of sandwich grandparents in China between 2011 and 2018.
More than 150 million Chinese adults aged 45 and older were estimated to be sandwich grandparents in 2011. Among them, more than 17 million were dual caregivers who provided care to their own older parents and young grandchildren simultaneously. These numbers fluctuated considerably between 2011 and 2018. Nevertheless, they suggest that millions of Chinese grandparents have extended families with four generations and are subject to competing demands for caregiving from multiple generations.
Furthermore, this study tested several hypotheses of intergenerational solidarity to examine correlates of intergenerational caregiving patterns among the Chinese sandwich grandparents. There was little or no evidence of functional or structural solidarity associated with providing care to older parents, young grandchildren, or both. This is not necessarily bad news for research on sandwich grandparents. For example, researchers who study the health implications of being a caregiver for sandwich grandparents are often concerned about the potential mediating effects of time-for-money exchange and health-related selection bias (Liu and Chen, 2022; Xu, 2019a; Xu et al., 2022). The lack of significant findings from this study may help alleviate these methodological challenges, at least in the Chinese context.
This study found evidence of normative solidarity at work. Sandwich grandparents who held more traditional family values, as measured by a stronger preference for multigenerational coresidence, were more likely to provide care to their own older parents, young grandchildren, or both. This finding was robust to several sensitivity analyses. Overall, the cultural mandates of filial piety, mutual aid, and interdependence across generations still persist in many Chinese families (Silverstein et al., 2006). Chinese sandwich grandparents place a stronger emphasis on the collective well-being of their extended families and value family solidarity, harmony, and continuity more than their peers in Western cultures (Burnette et al., 2013). They fulfill their culturally prescribed family obligations by providing care to both older and younger family members, which in turn could be emotionally rewarding and enhance their health and well-being.
There was some nuanced between-group variation in the association between normative solidarity and intergenerational caregiving. The estimated log relative risk ratios for preferring multigenerational coresidence were larger for providing care to older parents alone and providing dual care than for providing care to grandchildren only (see Table 3). After adjusting for baseline caregiving activities, this coefficient became statistically insignificant for providing care to grandchildren only (see Table 4). Despite evolving views on and values regarding filial piety in contemporary China (Liu, 2021; Xu and Peng, 2021), taking care of older parents remains one of the core tenets, while looking after grandchildren is a new practice that has emerged in response to social and demographic changes. Therefore, it is not entirely surprising that the preference for traditional multigenerational coresidence has stronger predictive power for intergenerational caregiving activities that involve older parents than grandchildren.
There were several findings that ran counter to certain research hypotheses. For example, having more mobility limitations was associated with a higher likelihood of caring for older parents. This might reflect reverse causality, but further research is needed. In addition, sandwich grandparents who had smoked were more likely to provide care to both older parents and grandchildren than non-smokers. In the context of contemporary China where smokers are predominantly male, this seemingly counterintuitive finding may reflect health selection bias. Several studies have shown that Chinese adults who smoke cigarettes have better self-reported health (Yen et al., 2010) and lower levels of physiological dysfunction in cardiovascular, metabolic, inflammation, and urinary systems (Xu, 2018). Therefore, it is possible that grandparents who had smoked cigarettes (most likely grandfathers) are relatively healthy and thus are more able to be caregivers.
The findings from this study should be interpreted with caution because of several limitations. Firstly, the CHARLS data are longitudinal in nature and therefore may not be nationally representative after sample attrition over time. Methodologically speaking, data from repeated cross-sectional surveys allow more accurate estimates of the trends in sandwich grandparenting, but such data remain absent in contemporary China. Furthermore, using lagged predictors with longitudinal data alone does not fully address the concern of endogeneity. For example, normative solidarity measured by the vignette question about multigenerational living arrangements in 2011 might be affected by respondents’ experience of intergenerational caregiving in prior years. Hence, the regression estimates based on lagged predictors may partly reflect the reverse causal effect of intergenerational caregiving on normative solidarity.
Secondly, each domain of intergenerational solidarity is multifaceted and should be measured by multiple indicators (Bengtson and Roberts, 1991). CHARLS collected relatively more data on functional solidarity and structural solidarity than on normative solidarity, limiting the capacity of this study to fully examine every aspect of intergenerational solidarity. It would also be important to account for older parents’ age and grandchildren's age because the older the parents are and the younger the grandchildren are, the more demanding intergenerational caregiving would be. However, CHARLS only collected ages of other family members who lived with the main respondents, making it impossible to identify the age of any older parent or grandchild who was taken care of by the sandwich grandparents but who did not live together with the latter.
Thirdly, this study measured patterns of intergenerational caregiving in a crude way. CHARLS did not collect details about specific caregiving activities. Certain caregiving activities, such as reading books with grandchildren and taking a walk with older parents, can be emotionally rewarding and provide health benefits to sandwich grandparents, while others, such as bathing young grandchildren or disabled older parents, can be physically and mentally demanding. Future research is needed to differentiate caregiving activities in terms of potential burdens and benefits to better understand sandwich grandparents’ involvement in intergenerational caregiving.
Sandwich grandparents are not randomly selected as caregivers for their older parents or grandchildren, or both. This study has revealed several demographic, socioeconomic, and cultural factors associated with Chinese sandwich grandparents’ involvement in intergenerational caregiving. These findings can inform policy designs that assist sandwich grandparents in achieving healthy aging for themselves while being caregivers in old age. Future research in other societies is needed to examine whether findings from this study can been generalized to culturally different settings.
Footnotes
Acknowledgments
This study uses data or information from the Harmonized CHARLS dataset and Codebook, Version D as of June 2021 developed by the Gateway to Global Aging Data. The development of the Harmonized CHARLS was funded by the National Institute on Aging of USA(R01 AG030153, RC2 AG036619, R03 AG043052). For more information, please refer to ![]() .
.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation of The City University of New York (grant no.: TRADA-50-116), National Institute on Aging of USA (grant no.: R01 AG030153, R03 AG043052, RC2 AG036619).
Appendix
Multinomial logit models (with adjustment for complex survey design) of intergenerational caregiving status among Chinese sandwich grandparents aged 50 or older.
| Caregiving status at Wave 2 (Compared to non-caregivers; unweighted N = 343) | ||||||
|---|---|---|---|---|---|---|
| Independent variables at Wave 1 | Care for G1 only (Unweighted N = 119) | Care for G4 only (Unweighted N = 434) | Dual caregiving (Unweighted N = 193) | |||
| Demographics | ||||||
| Age (mean-centered) | 0.030 | (0.023) | −0.021 | (0.019) | −0.083 | (0.025)** |
| Female (ref.: male) | 0.050 | (0.444) | 0.462 | (0.286) | 1.370 | (0.364)*** |
| Currently married (ref.: not) | −0.927 | (0.400)* | −0.420 | (0.291) | 0.498 | (0.382) |
| Rural hukou (ref.: urban) | −0.429 | (0.384) | 0.006 | (0.318) | −0.668 | (0.325)* |
| Socioeconomic status | ||||||
| Educational attainment (ref.: none) | ||||||
| ≤Primary school | −0.035 | (0.395) | 0.134 | (0.202) | 0.435 | (0.309) |
| Middle school | 0.261 | (0.444) | 0.234 | (0.271) | 0.608 | (0.345)† |
| ≥High school | 1.019 | (0.457)* | 0.176 | (0.318) | 0.658 | (0.367)† |
| Employment (ref.: not working) | ||||||
| Agricultural work | 0.797 | (0.333)* | −0.197 | (0.245) | 0.008 | (0.291) |
| Non-agricultural self-employed | 0.421 | (0.427) | −0.601 | (0.367) | −0.414 | (0.394) |
| Non-agricultural employed | 0.800 | (0.392)* | −0.116 | (0.319) | −0.757 | (0.354)* |
| Received pension (ref.: no) | −0.681 | (0.379)† | −0.028 | (0.235) | 0.373 | (0.323) |
| Normative solidarity | ||||||
| Preferred living arrangement (ref.: nearby) | ||||||
| Multigenerational coresident | 0.221 | (0.269) | 0.355 | (0.168)* | 0.536 | (0.238)* |
| Distant | 0.579 | (0.495) | 0.815 | (0.456)† | −0.056 | (0.463) |
| Functional solidarity | ||||||
| Received economic support from G3/G4 (ref.: no) | 0.010 | (0.261) | 0.061 | (0.182) | 0.282 | (0.275) |
| Received economic support from G1 (ref.: no) | 0.176 | (0.740) | −0.172 | (0.473) | −0.521 | (0.667) |
| Structural solidarity | ||||||
| N of adult children | −0.140 | (0.114) | −0.075 | (0.087) | −0.145 | (0.110) |
| N of siblings | −0.095 | (0.079) | −0.023 | (0.053) | −0.080 | (0.063) |
| N of mobility limitations | 0.174 | (0.099)† | 0.062 | (0.072) | 0.060 | (0.090) |
| N of doctor-diagnosed diseases | −0.015 | (0.095) | −0.036 | (0.070) | −0.121 | (0.093) |
| Self-rated health (ref.: fair) | ||||||
| Very good | −0.005 | (0.469) | 0.329 | (0.335) | −0.126 | (0.426) |
| Good | −0.112 | (0.351) | −0.189 | (0.222) | 0.112 | (0.282) |
| Poor | −0.365 | (0.338) | 0.069 | (0.238) | 0.005 | (0.307) |
| Very poor | 0.304 | (0.722) | −0.564 | (0.428) | −0.926 | (0.744) |
| Ever drunk alcohol before (ref.: no) | 0.394 | (0.360) | 0.414 | (0.216)† | 0.487 | (0.260)† |
| Ever smoked cigarettes before (ref.: no) | 0.027 | (0.391) | 0.116 | (0.240) | 0.514 | (0.324) |
| Constant | −0.221 | (0.864) | 0.157 | (0.621) | −2.008 | (0.800)* |
Notes: G1: older parents; G2: respondents (i.e. sandwich grandparents); G3: adult children; G4: grandchildren. Taylor-linearized standard errors are shown in parentheses. † p < 0.1; * p < 0.05; ** p < 0.01; *** p < 0.001.