
Abstract
In recent years, the emergence of mobile-internet-based crowdfunding has provided a new way for the poor to obtain emergency relief for medical needs. Despite a number of reported scams, medical crowdfunding has made an important contribution to society. Public opinion and sentiment highlight two practical issues: Are the resources being directed to the people who need them the most? And how can we optimize medical crowdfunding? To tackle these questions, we focus on the issue of how the socioeconomic status (SES) of help-seekers affects their online medical crowdfunding outcomes. We ask three research questions: What is the correlation between the SES of help-seekers and their fundraising outcomes? What are the underlying mechanisms? Is there a possible path for the optimization of medical crowdfunding outcomes? Our dataset includes 1930 fundraising cases from a large medical crowdfunding platform in China. The study finds significant differences in crowdfunding outcomes among different socioeconomic groups. Higher SES brings higher donation amounts, higher proportions of fundraising targets reached, a higher number of donations received, and more shares on social media. This socioeconomic gradient in crowdfunding outcomes contradicts the social expectation of prioritizing help to the neediest in medical crowdfunding. Mediation analysis also shows that offline interpersonal networks play an important intermediary role. While appealing case narratives are helpful, they are not an intermediary mechanism that links family SES with crowdfunding outcomes. Further analysis also finds that such a socioeconomic gradient seems to weaken when crowdfunding that begins within a private network of offline acquaintances on WeChat moves to public platforms.
With the rapid development and popularization of the mobile internet in China, social and economic systems have drastically changed, deeply affecting the life chances of members of different classes (Wang and Wang, 2016). Medical crowdfunding platforms (e.g. Easy Crowdfunding, https://qschou.com/; Waterdrop Crowdfunding, https://www.shuidichou.com/) relying on the mobile internet have reshaped the traditional social assistance system for healthcare. Government and social welfare organizations are no longer the sole initiators of medical assistance campaigns. Millions of individuals are now able to speak out for themselves and launch a crowdfunding campaign to help themselves, instead of being screened by a third party before asking for help. China, as the largest developing country in the world, still has a social security system that is far from sound and satisfactory. Therefore, how to make the most use of informal forces for medical relief is particularly significant. Medical crowdfunding, as a crucial supplement to healthcare, provides a feasible alternative for many families suffering critical illnesses and struggling with attendant financial burdens to return to a normal life.
Public opinion and sentiment highlight the need for helping the weak and poor. That is, financial relief for medical care should be directed to the patients with the most serious illnesses and worst financial conditions in a timely manner. In a recent survey, we asked the respondents about what influences their donation decision and donation amount on medical crowdfunding platforms such as Waterdrop Crowdfunding and Easy Crowdfunding. The results show that the trustworthiness of the help-seekers’ information, their financial status, and the severity of the patient's illness are the top three factors. 1 But are public expectations in this regard realized? In other words, do the families of patients with lower socioeconomic status (SES) raise more money and get timely treatment?
Scholars trained in social stratification and mobility may have reservations. Social resources are unevenly distributed in a pyramid shape. That is, an individual with a higher SES has greater power to acquire resources. This is also true in education, housing, health, and other domains concerning individuals’ livelihoods. Is stratification theory still highly predictive in medical crowdfunding? In fact, social stratification studies mostly center on routine events, such as career attainment and promotion in the labor market. However, critical illness, as a non-routine event that requires special support, has brought new challenges and opportunities to the test the power of stratification theories. First, for such non-routine cases, do the relevant theories still maintain their explanatory power? Second, if groups with different SES have different crowdfunding outcomes, what are the underlying mechanisms? Finally, is there any way to improve medical crowdfunding outcomes in the mobile internet era? To answer these questions, this paper takes a health stratification perspective and explores empirically whether the family SES of help-seekers affects their medical crowdfunding outcomes and the possible mechanisms behind this, using data from a large medical crowdfunding platform in China.
The origins and current situation of medical crowdfunding
For a long time, many families in the grip of serious illness have been faced with two obstacles: high treatment costs and limited social security. Unable to afford huge medical expenses, some patients with serious illness cannot receive adequate high-quality medical care, and as a result, suffer rapid deterioration of health. As a matter of fact, unaffordable medical expenses is a global problem, even in developed countries. For example, 62% of bankruptcy applications in the USA are caused by unaffordable medical expenses after illness or injury (Burtch and Chan, 2014). Disease-induced poverty also prevails in China, and is further aggravated by the aging population (Feng et al., 2015). As of the end of 2018, more than 40% of the 16.6 million rural Chinese living in poverty had fallen into or returned to poverty due to illness (Geng, 2017). In order to relieve the financial burden of critical illness treatment, China launched a medical healthcare program targeting critical illness care in 2012. As an extension to the basic medical insurance, it aims at addressing the challenges posed by low reimbursement rates, high deductibles, and low co-pay caps. However, it still leaves many drugs and medical consumables needed for treating critical illnesses uncovered. Moreover, this program has a single source of funds, offers limited security, and suffers from low efficiency (Wu et al., 2019). Many families have had to forego treatment due to huge medical expenses (Shen and Li, 2013). In general, the availability of healthcare for patients with critical illnesses in China remains limited, despite constant improvements in healthcare insurance programs.
Social assistance for medical care is an important way to ensure patients’ right to life and quality of life, and it is even more significant in underdeveloped countries or regions. Thanks to the rapid development of the mobile internet, medical crowdfunding, a new form of social assistance, has seen opportunities for further development. Medical crowdfunding, as a type of online public welfare crowdfunding, 2 refers to the pooling of funds from donors to pay medical expenses via online crowdfunding platforms (Bassani et al., 2018); more specifically, it is donation-based crowdfunding since patients do not need to provide donors with material benefits in return (Ibrahim and Verliyantina, 2012). Compared with crowdfunding for health initiatives or health science research, medical crowdfunding can meet the emergency needs of seriously ill patients, better compensate for shortcomings in public health provision, and allow for easier access to support (Gustke, 2015).
In recent years, medical crowdfunding has been developing at an alarming rate, and has become a new alternative for patients with critical illnesses to pool medical expenses. On GoFundMe, a large crowdfunding website in the West, 8000 medical crowdfunding campaigns raised up to US$1.6 million in 2011. This quickly increased to more than 600,000 campaigns (raising nearly US$150 million) in 2014, making it the largest individual crowdfunding category on the platform (Nexstar Media, 2015). China's online medical crowdfunding has gone through two stages. The former stage is similar to the that of GoFundMe, in which medical crowdfunding is just one branch of all kinds of crowdfunding online on an integrated crowdfunding platform covering education, environmental protection, culture and art, and so on. With the boom of online social interactions and increasing demand for medical assistance, medical crowdfunding in China entered the second stage in 2014 when specially designed platforms for medical crowdfunding began to appear. Those websites rely on WeChat, China's largest personal social platform, to disseminate the campaigns through personal networks. Since then, medical crowdfunding has undergone rapid development in China as the number of medical crowdfunding platforms, crowdfunding campaigns, donors, and total donations have all been rapidly increasing. Since its establishment in September 2014, Easy Crowdfunding has already attracted 550 million users, helped 2.53 million families with patients suffering critical illnesses, and raised a total of 25.5 billion yuan. 3 Waterdrop Crowdfunding, established in July 2016, has raised a total of 26.5 billion yuan, and a total of 300 million donors have donated more than 800 million times (CASS, 2020: 3).
As a new form of public welfare supported by the mobile internet, medical crowdfunding is easily accessible to the public and is efficient in dissemination. Simplified donation procedures and easy payment and sharing make it easy for donors. Crowdfunding campaigns are disseminated through WeChat. Such campaigns usually last no more than a month. Each time the campaign is shared by a friend in his/her own personal network, a “many-to-one” network of medical assistance is formed. This mobile-internet-based model supersedes the temporal and spatial boundaries that constrain traditional face-to-face fundraising, enables multiple successive donations, and also greatly accelerates the spread and expands the coverage of a given campaign. Moreover, its ease of operation and accessibility weaken the “digital divide” (Li, 2006) by allowing almost all patients to initiate a crowdfunding campaign. In general, mobile-internet-based medical crowdfunding can help relieve financial burden for many families, and further extricate them from severe illness and disease-induced poverty.
However, medical crowdfunding, while offering social support to seriously ill patients, has been the subject of moral concern from all walks of life. The solutions to ethical issues, such as fraud, hype, and privacy issues, are vital to the future development of medical crowdfunding (Zhao et al., 2021). This paper does not intend to discuss such ethical issues, but it is necessary to point out two takeaways. First, certain noteworthy events and ensuing discussions have impelled crowdfunding platforms to make technological innovations to as much as possible ensure the credibility of campaigns. For example, the help-seeking party is asked to submit proof of the family's financial conditions, and provide endorser contacts of third parties, especially medical workers, who can verify the details of the medical condition as well as the financial conditions. These innovations have also created the foundations for this study. 4 Second, criticisms directed against ethical violations convey a social consensus: social assistance should be directed to the poor and the weak, who are in greater need, even in online medical crowdfunding. With this in mind, this paper sets out to exploring how SES influences medical crowdfunding outcomes.
Theoretical framework and research hypotheses
Social stratification and health inequality
Social stratification has been a mainstream interdisciplinary perspective by which to understand medical care and health, producing an abundant literature. In fact, research on health inequality is not confined to the inequality concerning morbidity and mortality rates, but includes early healthcare and differential access to resources that facilitate differential recovery rates by SES (Lutfey and Freese, 2005). Medical crowdfunding on the mobile internet is a new phenomenon, but has become an essential way for individuals to access health services. Therefore, health inequality theories are well suited to understanding the differences in medical crowdfunding outcomes. 5 Medical crowdfunding, rising out of new technologies, also provides a new context for us to revisit and understand the theories of health inequality in the era of the mobile internet.
The release of the Black Report on health inequalities in 1980 aroused widespread concern in the field of social stratification and mobility (Elo, 2009). It reported significant differences in morbidity and mortality among all social strata due to their SES differences, and significantly better health among the upper classes than the lower classes (DHSS, 1980). Even though the prevalence of certain diseases may be higher among the affluent members of certain age groups, the health advantages of high SES repeatedly recur. The Whitehall Study pointed out the socioeconomic gradient in health, which holds true in almost all diseases (Marmot, 2015: 121), the so-called “status syndrome” (Qi, 2020: 1–16). The SES differences are significant in healthcare, with higher SES leading to better health; for example, high-ranking civil servants have been found to have better health than ordinary civil servants (Marmot, 2015). “Root cause theory” further explores the mechanisms between SES and health. This theory can be traced back to the “basic causes” put forward by Lieberson (1985: 188) as a term for those factors imposing a lasting impact on dependent variables. The decline of one mechanism will lead to the emergence of other mechanisms or the role of the original mechanism will become more prominent. House et al. (1990, 1994) subsequently applied this to the field of health, emphasizing that there may be a persistent relationship between SES and mortality. However, the basic cause is a general concept, and few scholars have clearly uncovered which basic causes are still able to exert an influence when intervening mechanisms are eliminated.
In response to this, Link and Phelan (1995) put forward the fundamental cause theory (FCT) in 1995. The basic idea is that social conditions, rather than medical, natural, or biological ones, are the fundamental causes of people's health differentiation. They emphasize the lasting impact of social conditions on healthcare, despite the rapid changes in medical care and the emergence of new technologies. In other words, no matter how the downstream factors for health change, social conditions can always affect the health status of individuals by influencing these downstream factors. Lutfey and Freese (2005) further developed FCT after conducting a one-year ethnographic survey in a diabetes clinic. They identified a number of specific mechanisms that affect patients’ access to high-quality healthcare and services. Most of these mechanisms favor patients with better SES. For example, higher SES patients are more likely to follow doctors’ advice and pool various medical resources needed for treatment. Therefore, they see SES as a meta mechanism for health inequalities (Lutfey and Freese, 2005), making it the fundamental theoretical foundation in health stratification research in China (Hong and Liu, 2019; Jiao, 2014, 2018; Jiao and Bao, 2020; Wang, 2011, 2012, 2017).
On the whole, FCT situates health research within structural social inequality, and shifts the focus to social stratification and inequality. Previous research on SES and disease/health has been dominated by medicine and epidemiology. SES was generally considered an irrelevant and unimportant control variable or moderator. It was merely seen as the starting point of a chain of causality in health and the intervening role of health risk factors, especially high-health-risk behaviors. However, during the past decades, social progress and improved medical technologies have not weakened the persistent association between SES and health. This indicates why the focus only on proximal factors fails to explain the socioeconomic gradient in health: specific intervention mechanisms link SES and differential health outcomes via access to the quantity and quality of healthcare services in a given period.
FCT holds that flexible resources play a central role in health disparities resulting from SES (Phelan et al., 2010). The persistent influence of SES on health over time and changing conditions could be the result of multiple possible mechanisms. “Flexible resources” is one important factor enabling such mechanisms. Specifically, both individuals and groups can take advantage of their knowledge, money, power, prestige, social networks, and other key resources according to situational contexts, so as to minimize health risk exposure and actively adopt health protection strategies. It is precisely because the above critical resources can be transformed into healthcare resources in many forms that, regardless of the type of disease, treatment, protective factors, or even how the system of medical assistance changes, health gradients based on SES are maintained in a stable manner.
Flexible resources indicate that health inequality is not confined to inequalities in morbidity and mortality, but also includes early healthcare and differential access to resources that facilitate recovery by different SES (Lutfey and Freese, 2005). In addition, is it possible for online medical crowdfunding to break the “Matthew effect”? Although FCT holds true in many fields of health, it has not been well researched in this emerging era of medical crowdfunding. A few studies concerning differences in medical crowdfunding outcomes have focused on downstream factors, such as narrative skills (Snyder et al., 2016, 2017; The Lancet Oncology, 2017), and fail to recognize the crucial role of the family SES of help-seekers in affecting their access to health resources. In China, sociologists have paid limited attention to medical crowdfunding. Only a few relevant studies have analyzed the operational modes and characteristics of medical crowdfunding platforms (Zheng and Wang, 2017), the relationships between help-seekers and donors (Zhang and Hou, 2018), or differences in resources embedded in online networks (He and Jing, 2019; Wang and Song, 2016) through case studies. Seen from the perspective of social stratification, most of the help-seekers and their families are in the middle and lower classes, taking up a small section of the SES spectrum. Do FCT and the “status syndrome” still hold true for this subpopulation? This question warrants new empirical testing and engagements with the public's ethical and moral sentiments, so as to better understand the social determinants of medical crowdfunding performance.
Research hypotheses
In view of the health inequality theories mentioned above, this study holds that online medical crowdfunding is a new field in which flexible resources can be utilized, and as such SES will influence access to health resources through certain mechanisms regardless of the context. Individuals with higher SES have better healthcare when confronted with diseases, and this positive association will also hold true in medical crowdfunding. On the mobile internet, especially the social networking app WeChat, the flexible resources of people with higher SES are embodied in cultural capital (better digital literacy) and social capital (better personal networks), among other possibilities.
Flexible resources I: Cultural capital
Cultural capital is an important mechanism of reproducing inequality and can be converted into various resources favorable for status attainment (Bourdieu, 1986: 241–258). As an analytical concept, it is also often used to explain sociological issues such as status attainment, academic performance, parenting styles, and consumption stratification in China (Fang, 2018; Qiu and Xiao, 2011; Tian and Jing, 2018; Zhu, 2018). The existing relevant qualitative studies suggest that cultural capital could also be used to explain crowdfunding outcomes on the mobile internet, because the audience for such platforms mainly obtains information indirectly through visual materials.
The digital divide informs us that medical crowdfunding outcomes could still show a socioeconomic gradient despite the ease of accessibility for people of almost all classes. In other words, the internet access divide might be closing for different social strata, but the gap in digital literacy is hard to bridge. Patients with high SES and their family members are often better educated, better at expressing their difficulties by using phrases that are more appealing and emotional, better at describing their hardships more comprehensively, and better at building up credibility with potential donors by uploading various supporting materials and pictures in a timely manner. Such narrative competency has positive outcomes for crowdfunding according to empirical research (Snyder et al., 2016, 2017; The Lancet Oncology, 2017). Therefore, we hold that cultural capital is the first kind of flexible resource that mediates the influence of SES on medical crowdfunding outcomes. Higher SES patients and family members have more cultural capital and thus can better express their plight, and therefore it is easier for them to gain trust and sympathy from other social actors, so as to get more financial support.
Flexible resources II: Social capital
Social capital is a multi-faceted concept. This paper sees it as the resources embedded in social networks that can be mobilized for instrumental actions (Bian, 2004; Lin, 2001: 19–98). Although most studies on social networks and social capital are concerned with social status attainment (Bian, 2012: 1–18; Chen et al., 2004), more and more studies have realized that social capital is an important mechanism for understanding social inequality (Cheng and Zhang, 2013; Cheng and Bian, 2014; Cheng and Yao, 2014; Cheng et al., 2015; Lin, 2000; Lu et al., 2013; Tian and Fu, 2020), and Wang and Ma (2020) employ it to explain the socioeconomic gradient in health. We argue that offline interpersonal networks and their embedded resources are also determinants for successful online crowdfunding.
First, families with higher SES have more social contacts on WeChat. In addition to relatives, patients with higher SES are more likely to have broader social networks that include co-workers, friends from all walks of life, and classmates from different stages of schooling. These social ties can not only help patients to use social networks, but also could be potential donors. They can also disseminate the appeals of help-seekers within their own social networks, facilitating the message to travel beyond the social networks of help-seekers and into social networks with higher heterogeneity.
Second, the homogeneity of social interaction (McPherson et al., 2001) implies that patients with higher SES tend to have not only larger social networks, but also more network members with higher SES. As a result, first, social network members have better financial situations and more are likely to donate and donate more; second, after requests for help have been shared to more people, second- and third-order contacts (and so on) who get exposed to the donation appeal tend to have higher average SES, and such an advantage in SES and its effect on crowdfunding outcomes can be replicated and amplified.
Third, even if families with lower SES have ties of higher SES, such as well-off relatives, there is no guarantee that they will share or repost the message, because these ties may be concerned about the negative impact doing so might incur on their social reputation (Smith, 2005). For example, high SES relatives and friends may be afraid of losing face by exposing their offline ties who are not well off, and some others may worry about the possible perception that they, as core ties to the help-seekers, were shifting the responsibilities to the public by sharing the campaign. In a society featuring favoritism, in China close social ties are obligated to help each other, and such mutual responsibilities and obligations play a key role in people's routine and important non-routine events (Bian, 2017, 2018). If a person does not fulfill his reciprocal obligations to his friends and relatives, he may receive moral criticism. As such, network members with high SES who are willing to donate are more likely to offer donations offline but not to share or disseminate the campaign online. According to the aforementioned sample survey (see note 1) conducted by the authors, 25.3% of young workers with a monthly income of less than 3000 yuan did not make any donations in online crowdfunding, and this figure was 23.1% when it came to young workers with a monthly income of more than 10,000 yuan. However, when it came to sharing or reposting the donation appeals, 39% and 47.7% of the two groups had never shared a donation appeal, respectively. To sum up, class differences in donation experience are small, but they are more apparent in the sharing of appeals, with those with high SES being more reluctant to forward relevant information. 6
Based on the above analysis, we emphasize that the effect of SES on medical crowdfunding outcomes may be contrary to public sentiment and expectations that needy families should get more donations. People with higher SES are likely to have a higher total amount of funds raised, higher rates of achieving funding goals, more donations, and more shares. Cultural capital is one form of flexible resource that mediates the influence of SES on crowdfunding outcomes, and social capital embedded in personal networks is a second form. As such, this study puts forward the following hypotheses.
If the hypotheses above are true, is there any way to weaken the positive association between SES and crowdfunding outcomes? In other words, is there any way to reduce or even reverse the disadvantages of the underprivileged in medical crowdfunding? There is a debate concerning social capital and social inequality: Is social capital the “capital of the poor” or just another amplifier of social inequality (DiMaggio and Garip, 2011)? One school believes social capital to be mechanism to reproduce or even amplify the inequality (Cheng and Bian, 2014), while the other school insists that social capital can benefit groups with low SES and views it as the capital for the poor (Grootaert, 1999, 2001; Woolcock and Narayan, 2000). Such controversy mainly stems from different definitions of social capital, the former seeing it as personal networks and the latter regarding it as essentially public goods, such as universal trust or community cohesion (Cheng and Yao, 2014). This debate has important implications for our exploration of how to resolve socioeconomic inequality in medical crowdfunding: If the medical crowdfunding campaigns are able to travel beyond personal networks based on particularism and reach a broader public based on universalism, will the socioeconomic gradient in crowdfunding outcomes could be narrowed?
The crowdfunding platform of interest in this study has two forms of campaign promotion, 7 and as such it constitutes a quasi-natural experiment through which we can explore the above issues. One is to launch and diffuse the campaign through WeChat (“single channel”), which is also the mainstream means of donation appeal. Usually, after the campaign is launched, the help-seekers and their core ties would share it in their personal networks online through WeChat and more contacts would see the campaign and further repost it into their own personal networks through WeChat again. The diffusion is continued further but it will stop at some point because the contacts it reaches will have weaker ties as the campaign is being diffused further. It should be noted that crowdfunding campaigns disseminated only through WeChat rely on offline personal ties. People who are willing to donate will only get exposed to a specific help request instead of all the help requests on a platform, and thus they are not able to make a rational decision after a full comparison of all help-seekers.
The second form differs from the first in terms of diffusion. Apart from being diffused on WeChat, the campaigns are randomly selected and recommended on the homepage of the crowdfunding platform (“mixed channel”). The homepage offers an opportunity for the help-seekers to appeal to the general public, whom they do not know, instead of real-life ties. Each day the platform displays 30 ongoing medical crowdfunding campaigns on its homepage. By browsing the homepage, donors can keep track of the campaign updates in real time and donate as they wish.
Single-channel and mixed-channel campaigns attract different donors, thus creating differences in their outcomes. Single channel means the potential donors exposed to the campaign are real-life ties or friends of friends, and the contacts are highly homogeneous. The crowdfunding outcomes are strongly affected by those homogeneous contacts. Critical illnesses are crises for the person who needs help and their contacts feel obligated to help regardless of the severity of the disease or the financial conditions. However, when the campaign is recommended on the platform homepage, it means it gets exposed to the general public, the majority of whom are strangers. In this shift from a private to a public sphere, the donation decision is more likely to be influenced by the severity of the disease and the financial conditions of the family. Higher SES could even be a negative factor, because it contradicts the public expectation that help be directed to the neediest. The public are more likely to donate to families with lower SES. Therefore, this study puts forward a final hypothesis.
The theoretical framework of this research is shown in Figure 1.
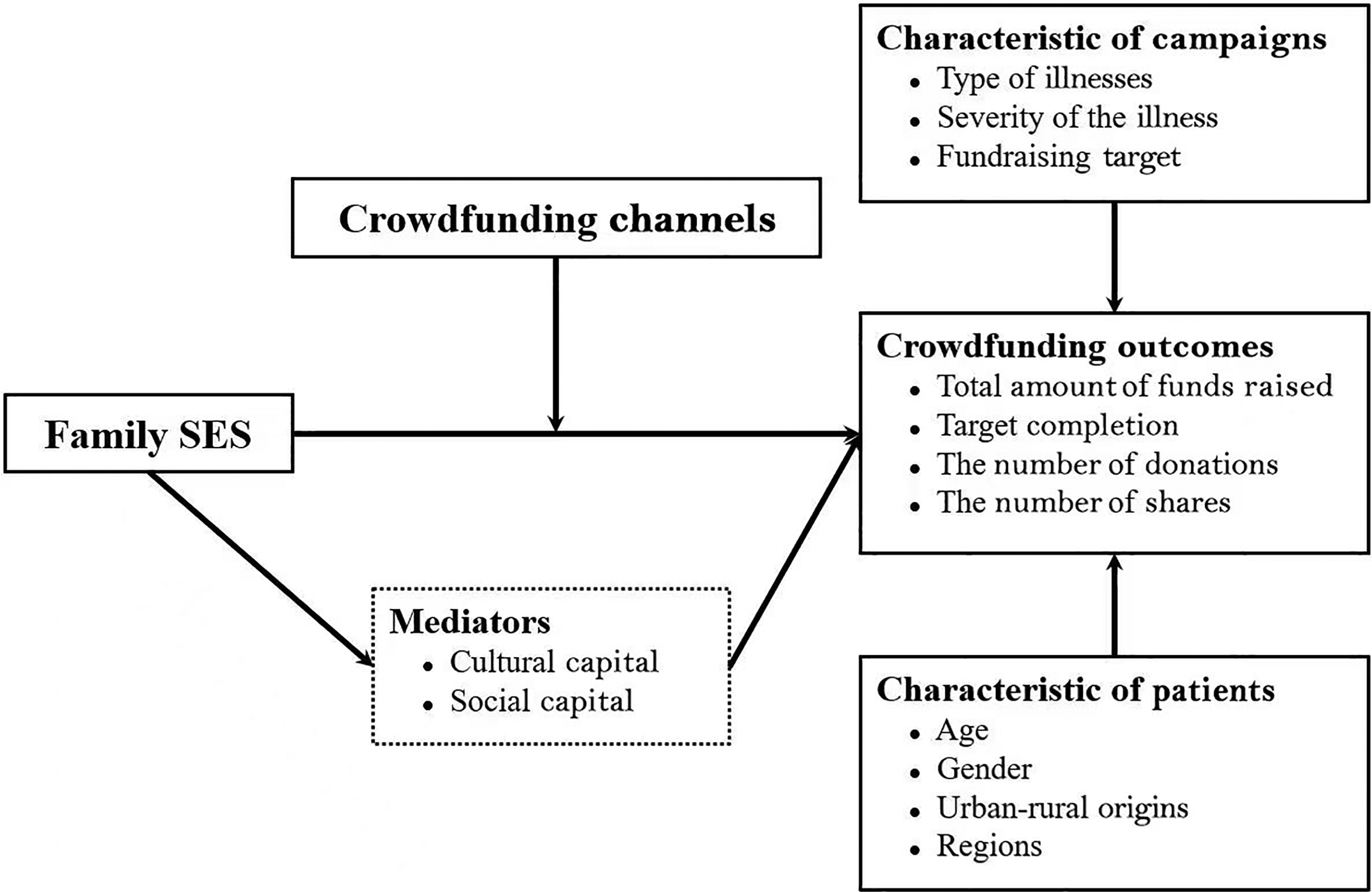
Theoretical framework of this study. SES: Socioeconomic status.
Data and variables
Data
Our data was collected from a large medical crowdfunding platform in China that has raised more than 30 billion yuan from about 1 billion donations; it is the most representative of the Chinese medical crowdfunding platforms. Both individuals and social and charitable organizations can launch medical crowdfunding campaigns on this platform. The campaigns initiated by individuals are of greater social influence and of interest to this study. The crowdfunding campaigns initiated by individuals are usually disseminated among relatives and friends as well as second- and third-order contacts on WeChat. To ensure the authenticity of the campaigns, the platform requires help-seekers to upload personal and family information, especially proof of financial conditions and the medical case. At the same time, endorsers are introduced to verify the authenticity of the campaign, and they are also required to confirm their legal identity before their verification of the campaign. The campaigns on the platform generally do not last more than 30 days and can be closed early. The money raised will be transferred to the patients from the platform in two to three working days. The platform also displays 30 crowdfunding campaigns randomly on its homepage every day, and offers updates from time to time. 8
Our dataset covers cases on the platform from 1 January to 30 May 2019. We collected data from medical crowdfunding campaigns recommended and displayed daily on the homepage and those only diffused on WeChat, and obtained a total of 2058 cases. After excluding the samples with incomplete information, we obtained 1930 valid samples for use in statistical models. The effective sample covers the vast majority of provinces, municipalities, and autonomous regions in China (except for Tibet and Taiwan). Among them, 1603 campaigns were promoted on a mixed-channel basis and 455 campaigns via one channel (only launched and diffused on WeChat).
In addition to data crawling from the platform, we also hired research assistants to manually identify the information of the sample campaigns. They needed to carefully read the contents of all components of the appeals, such as the text, pictures, fundraising updates, and messages left from endorsers to verify information (see Table 1 for details). In order to ensure the data accuracy, the information identification was independently completed by two research assistants, and then a consistency check was carried out. Inconsistent information was corrected, and a consistency check was performed again until there was no difference.
Data crawling and manual identification list.
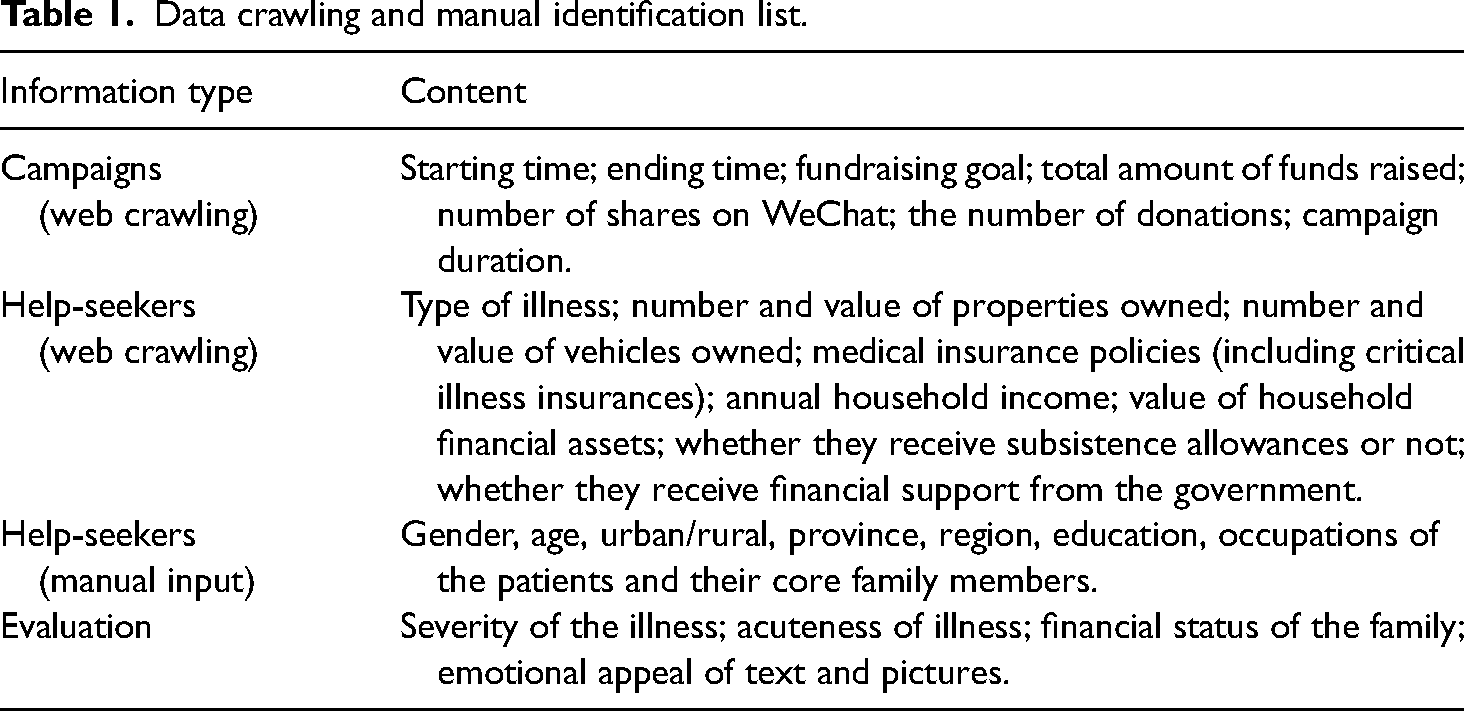
In addition, this study also evaluated each case. Each case was graded and evaluated by two or more research assistants (Table 1). Each assistant needed to evaluate 25–50 medical crowdfunding cases. In order to avoid differences in evaluation standards from different evaluators, we use the following procedures for each case: first, each evaluator scores each feature (e.g. the severity of the disease) of each case separately; then, evaluation scores are standardized within each evaluator to eliminate the differences in evaluation standards of different evaluators; finally, the evaluation scores of different evaluators are summed up and averaged as the final evaluation score of a certain feature of the case.
Variables
Dependent variables
The study focuses on medical crowdfunding outcomes. Hence, the dependent variable includes four indicators: total amount of funds raised, target completion percentage, number of donations, and number of shares. The total amount of funds raised refers to the total amount of money crowdsourced; target completion percentage refers to how close the campaign was to its fundraising goal, and is calculated by dividing the total amount of funds raised by the fundraising goal (in percentage); the number of donations means the total number of donations received by the campaign; the number of shares is the total times the campaign has been shared or reposted on WeChat and reflects the breadth of its diffusion. In order to avoid the influence of outliers, the natural logarithms of the above four variables were taken into the regression model. 9
The average fundraising goal of the crowdfunding cases used in this study was 239,300 yuan, and individual campaigns were shared 2049 times and donated to 1116 times on average. The actual amount of funds raised was 61,000 yuan, and the target completion rate was about 27.2% on average. In fact, a fundraising goal is rarely achieved. Only 34 out of 1930 cases in this study achieved the fundraising goal completely, accounting for 1.8% of the total sample.
Independent variables
(1) Family SES. Social stratification is generally regarded as multidimensional, but since this paper does not address a specific dimension, we adopt family SES as an integrated index (Pampel et al., 2010). We use as many indicators as possible to construct the family SES of help-seekers. At the same time, we also recruited college students to assess the financial status of the families from the donor perspective. After systematic evaluation, 11 indicators reflecting family SES were included. First, this study examines the financial status of the family based on four indicators: the value of any property owned by the family, family annual income, family financial assets, and the ownership of private vehicles. Second, two indicators often used to reflect social class are included: the occupational class and educational level of family members of the fundraisers, which are manually identified by research assistants on the basis of the campaign information. Occupation is classified into 11 categories, namely part-time workers, farmers, the self-employed, the unemployed or homemakers, workers or technicians, college students, enterprise employees, wage earners, civil servants, professional and technical personnel, and managers or bosses. In this study, civil servants, professional and technical personnel, and managers or bosses are coded as 2, employees and wage earners are coded as 1, and the rest are coded as 0. Having a university degree or above is coded as 1, while the rest are coded as 0. Third, several other objective indicators are included to construct SES: the number of health insurance policies they have, whether they receive low-income insurance (dibao), whether they receive subsistence allowances (jiandang lika pinkunhu), and whether they receive financial support from the government. Lastly, the evaluators also assessed the financial status of the family from the perspective of donors, as an indicator of their subjective SES (1 = particularly poor, 2 = relatively poor, 3 = average, 4 = well off, 5 = very well off). The scores were standardized and then summed and averaged. The distributions of the above 11 indicators are different, so they are not suitable to be directly aggregated into a family SES index. To counteract this effect, we first normalize all the indicators (converting them to a variable with a mean of 0 and a standard deviation of 1) and then sum them into the SES index of the family. In addition, in descriptive analysis, we divide help-seekers of different SES into 10 different groups to describe the characteristics of each group of families. In order to better present the profiles in graphs, the 10 groups are grouped into three, with the top 30% as the “high SES” group, the bottom 30% as the “low SES” group, and the rest as the “middle SES” group. (2) Crowdfunding channels. As discussed previously, there are two ways to promote campaigns. One is the single channel only, with the campaigns launched and diffused only to real-life ties on WeChat; the other is the mixed-channel mode, which means that the campaign will also be displayed on the platform homepage to reach strangers, in addition to being promoted on WeChat. In the moderation analysis, we treat the former as the reference group, and explore the moderating effect of mixed channels on how SES influences medical crowdfunding outcomes.
Mediators
The cultural capital of help-seekers and their families is the first mediating variable in the study. We employ four indicators of both subjective and objective measurements. The objective indicators include the text length of the help-seeking narration and the number of pictures displayed in it. In most cases, a longer story means more comprehensive information provided and more adjectives used, and thus it has greater appeal. The more pictures provided (such as photos of patients in hospital, medical bills, and family housing information), the richer, more credible, and more emotionally appealing the information is. Subjective indicators include how emotionally appealing the text and pictures are, which was assessed by college student assistants.
The second mediating variable is the activated social capital of the fundraisers and their families, which comprises two dimensions: social network structure and social network resources. To ensure the reliability of the medical crowdfunding campaigns and facilitate the public to further understand the social and economic status of help-seekers, the platform provides an endorser module. Endorsers need to upload legal authentication, disclose their relations with the patient, and leave messages of attestation. There are nine relationship types, including relatives, friends, colleagues, classmates, neighbors, ward mates (medical ward), doctors and nurses, and teacher–student relationships. In this study, the total number of endorsers of each type was added together for the “network size”, and the total number of types of endorsers was added to represent “network diversity”. We also adopt the amount of funds raised as an indicator of “network resources”. To construct this indicator, we use the first 30 donations of each campaign and summed the total average. 10
Control variables
Considering the association between certain illnesses and age, the study divides help-seekers into seven age groups: 0–5 years old, 6–18 years old, 19–29 years old, 30–40 years old, 41–50 years old, 51–60 years old, and 61 years old and above. The 41–50-year-old group, where the mode of all ages in the sample lies, is set as the reference group. Another very critical control variable is the (monetary) fundraising goal. The fundraising thresholds of different SES groups are obviously different, which may lead to a false correlation between SES and fundraising outcomes, while controlling the fundraising goal can reduce such confounding bias. This variable is a continuous variable of right skew, and we take its logarithm into the model.
Other control variables include gender, urban/rural origin, region, type of disease, and severity and acuteness of the illness. For the gender of the help-seeker, we take women as the reference group; for urban/rural origin, we take urban as the reference group. Region is divided into the eastern, central, northwest, southwest, and northeast regions, with the central region as the reference group. The disease type is a categorical variable, including leukemia, malignant tumor, pneumonia, fracture, brain injury, severe burns, severe nephropathy, neonatal diseases, cardiovascular diseases, severe anemia, multiple conditions, and other conditions, with malignant tumor, which accounts for the highest proportion, as the reference group. The severity and acuteness of the illness was scored subjectively by evaluators after they had read relevant materials, 11 after which it is treated the same way as the other evaluation variables. See Table 2 for descriptive statistics.
Descriptive statistics (n = 1930).
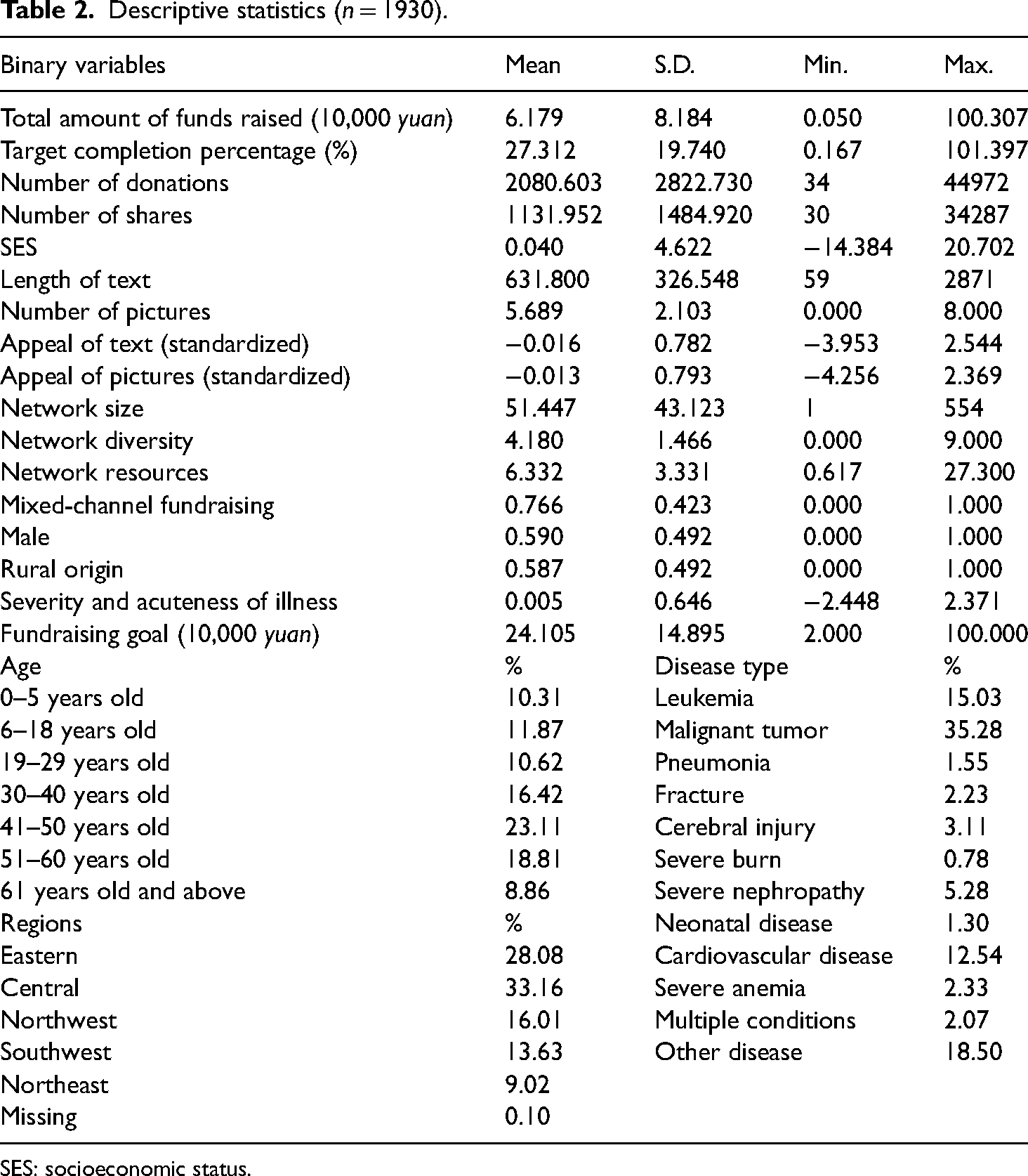
SES: socioeconomic status.
Empirical results
Medical crowdfunding outcomes: A static description
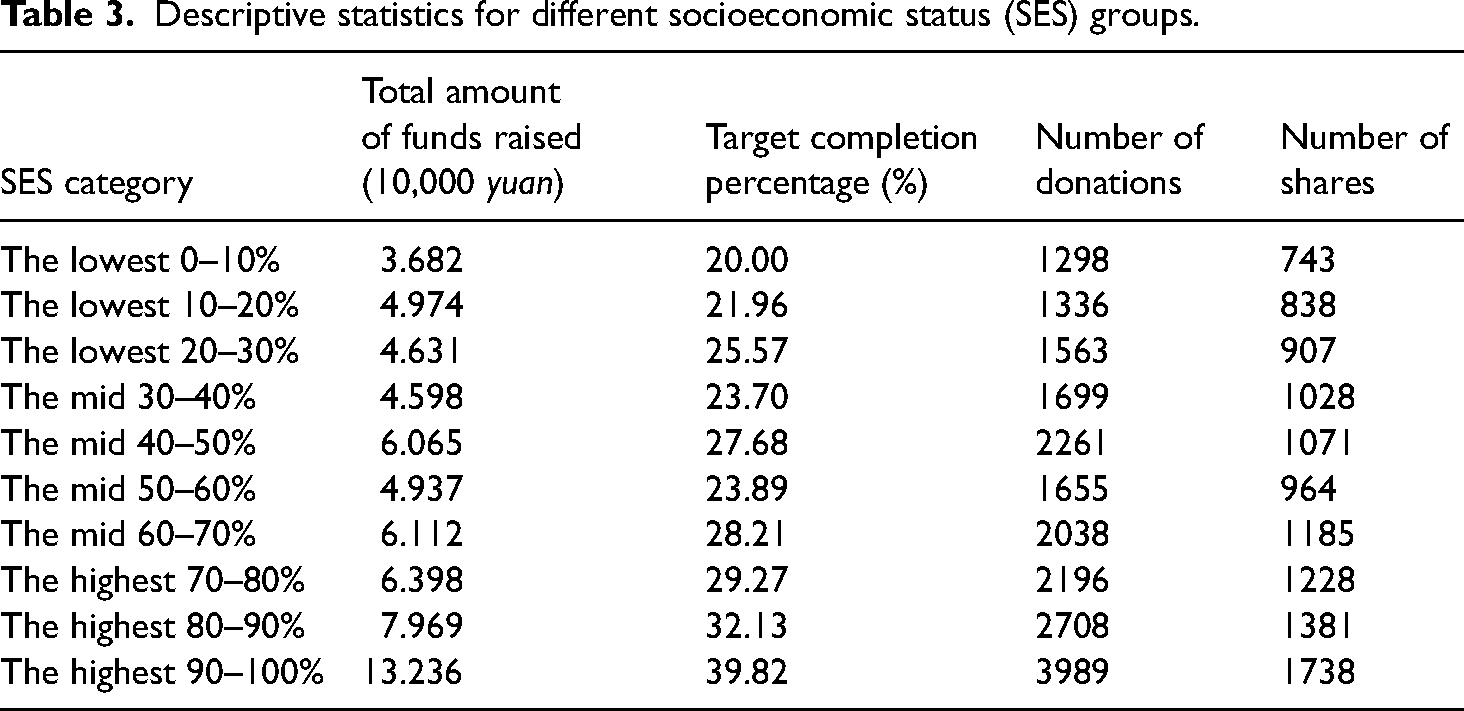
Table 3 shows the differences in total amount of funds raised, target completion percentage, number of donations, and shares among help-seekers of different SES. All the indicators increase with increasing SES, that is, the higher the SES, the better the fundraising outcomes. The average gap in funds raised between the lowest 10% and the highest 10% in terms of SES was 95,540 yuan. Campaigns initiated by the lowest 10% of help-seekers in terms of SES raised only 20% of their fundraising goal on average, which is only half that of the top 10% of help-seekers in terms of SES. There is also a significant socioeconomic gradient in the number of donations and shares, with the figures for the high SES group being 2.07 times and 1.34 times higher compared to those for the low SES group, respectively.
Descriptive statistics for different socioeconomic status (SES) groups.
Medical crowdfunding outcomes: A dynamic description
Figure 2 shows the campaign survival rate (Figure 2(a)) and the average donation amount (Figure 2(b)) among the three SES groups as the number of donations increases, which respectively reflect the quantitative and qualitative advantages of higher SES for medical crowdfunding.
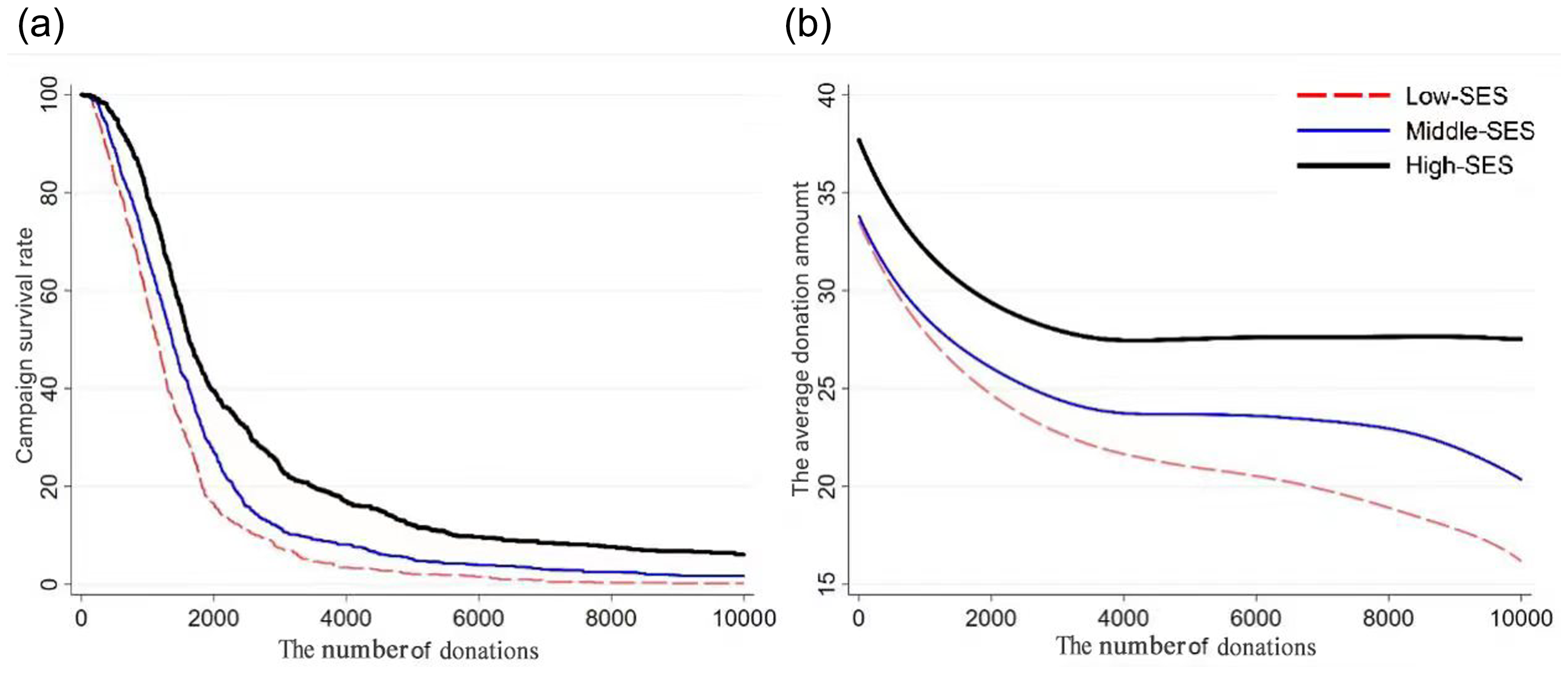
A dynamic depiction of the socioeconomic status (SES) inequality of medical crowdfunding outcomes.
Figure 2(a) shows that the campaign survival rate declines rapidly for all three groups as the number of donations increases, but is consistently higher in the high SES group than in the other two groups. At the threshold of 2000 donations, the campaign survival rate was 39.9% for the higher SES group and only 16.4% for the lower SES group. 12 At the 10,000 donation threshold, the campaign survival rate of the high SES group was 6.1%, while that of the low SES group was close to zero (0.2%, 35 times less than that of the high SES group). Clearly, the lower the SES, the shorter the campaign survival and the greater the gap with those of the higher SES group over time.
More importantly, there is a consistent trend of socioeconomic inequality in medical crowdfunding both in terms of quality of and quantity of donations. Figure 2(b) shows that in the initial stage of fundraising, there is little difference between the average fundraising amount of the middle SES and the lower SES groups, both of which are around 34 yuan, while the high SES group has a higher average of about 37 yuan. Over time, the average donation becomes increasingly lower, but the gap between SES groups begins to widen. The average donation stabilizes at 28 yuan per donation after 3800 donations for the higher SES group, but that of the middle and lower SES groups continues to fall, with the decline being even greater for the lower SES group. In the lower SES group, the average donation drops to 20 yuan at the 6000th donation, and to about 17 yuan at the 10,000th donation. At these two points, the higher SES group's average donation amounts are 8 and 11 yuan higher, respectively. Therefore, both the static and dynamic descriptions support Hypothesis 1, that is, the higher the SES of fundraisers and their families, the better the outcomes of their medical crowdfunding.
SES differences in medical crowdfunding outcomes: Regression analyses
To further explore the socioeconomic inequality in medical crowdfunding, we conduct multiple regression analyses of four indicators: total amount of funds raised, target completion percentage, number of donations, and number of shares. Table 4 displays the results of the four regression models. Model 1 shows that the SES of the help-seeker has a significant positive effect on the total amount of funds raised (p < 0.001, t > 10). To be specific, when other variables are controlled, an increase of one standard deviation in SES results in a 31.1% increase in the total amount raised, 13 fully supporting Hypothesis 1. Model 2 also reveals a significant effect of SES on target completion percentage (p < 0.001). That is, for every standard deviation increase of SES, the target completion increases by 31.9%. Models 3 and 4 respectively show the significant effect of SES on the number of donations received and the shares, and also show a significant positive correlation (p < 0.001). Every standard deviation increase in SES leads to a 22.8% and 17.1% increase, respectively, in the number of donations and shares.
Multiple linear regressions of medical crowdfunding outcomes (n = 1930).
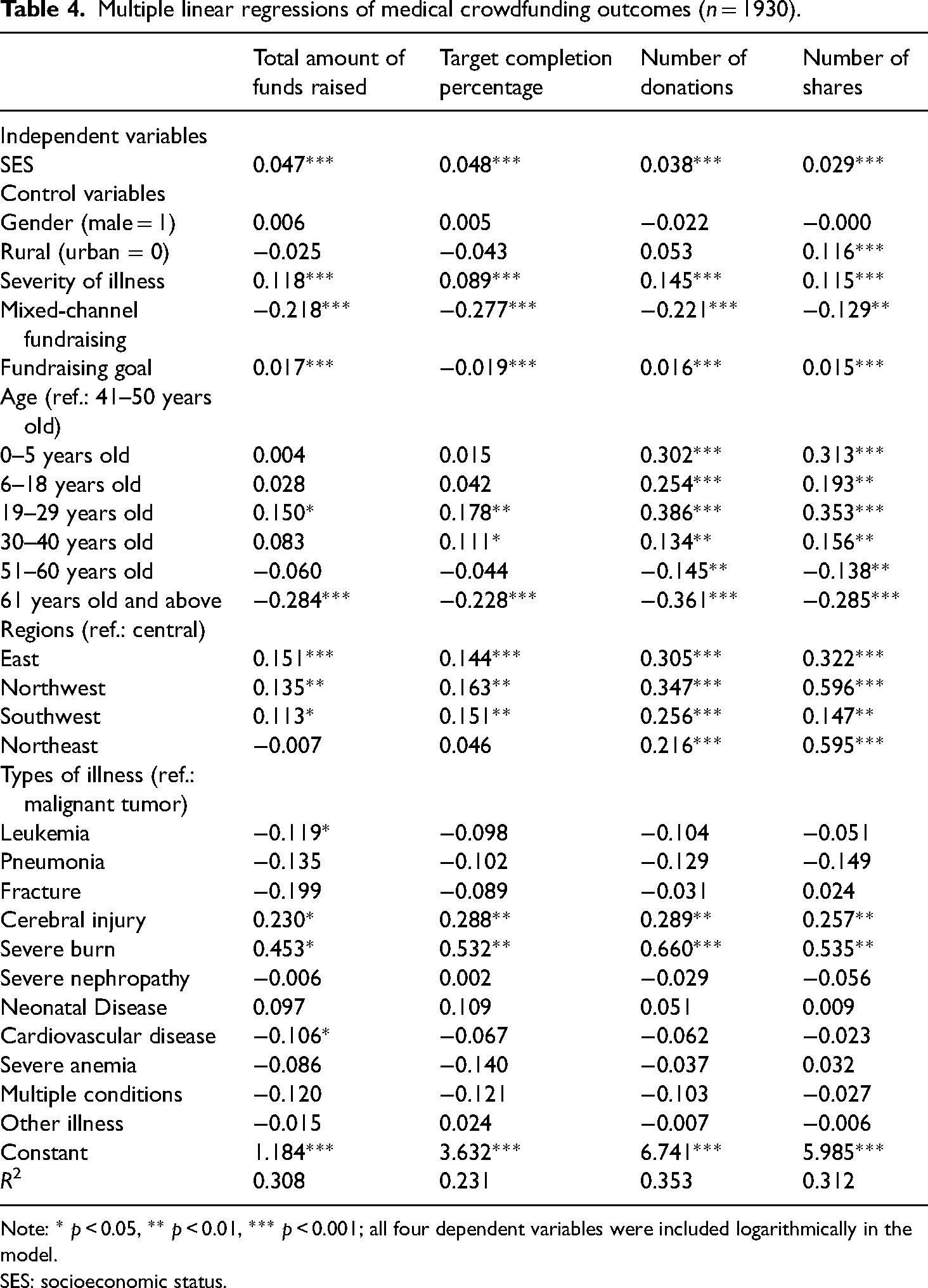
Note: * p < 0.05, ** p < 0.01, *** p < 0.001; all four dependent variables were included logarithmically in the model.
SES: socioeconomic status.
To sum up, the four models in Table 4 show that the SES of the fundraisers and their families has a significant positive effect on the total amount of funds received, target completion percentage, number of donations, and number of shares, meaning Hypothesis 1 is supported.
In terms of the control variables, the more severe and acute the disease, the better the outcome of the crowdfunding campaign. The amount of the fundraising goal has a significant positive impact on the total amount of funds raised, the number of donations, and the number of shares. However, Model 2 also shows that the higher the monetary fundraising goal, the less likely it is that the campaign will achieve it, which is in line with common sense. In terms of the urban/rural divide, campaigns from rural areas have lower target completion percentage target completion, but more shares; there are no significant differences in donations and total amount of money raised across urban and rural campaigns. This means that rural patients receive less money on average than urban patients. Notably, gender was not significant in any of the four models, suggesting that people contribute regardless of the sex of the patient and that women have the same opportunities as men. However, what is alarming is that male help-seekers accounted for nearly 60% of the around 2000 campaigns collected and they are evenly distributed over all age groups, which means that women are less likely to raise money on the internet if they are seriously ill. In addition, fundraising outcomes differ for different ages, regions, and disease types.
To sum up, according to the static and dynamic descriptions and multiple regression analyses, we observed a clear and stable pattern: the higher the family SES of the patient, the better the crowdfunding outcome, and such advantages are embodied in the total amount of funds raised, target completion percentage, number of donations, and number of shares. Therefore, Hypothesis 1 is firmly supported.
Family SES is constructed with multiple indicators, so does each indicator have a consistent impact on crowdfunding outcomes? As a robustness test, we replaced the family SES index with the specific 11 indicators and estimated their effects separately (see Table 5). In the first two columns in Table 5, the 11 indicators are positively significant, consistently indicating that the higher the SES of the patients and their families, the greater the total funds received and the higher the target completion percentage. In addition, the 11 indicators were significantly positive for the number of donations (with two indicators significant at the 0.10 level), showing that the higher the SES of patients and their families, the more donations were received. In terms of the number of shares, seven indicators pass the statistical significance tests with a significance level of 0.05, three indicators pass the statistical test at the 0.10 level, and only one indicator fails the statistical test. Therefore, the robustness tests also support Hypothesis 1.
Robustness tests of medical crowdfunding outcomes (n = 1930).
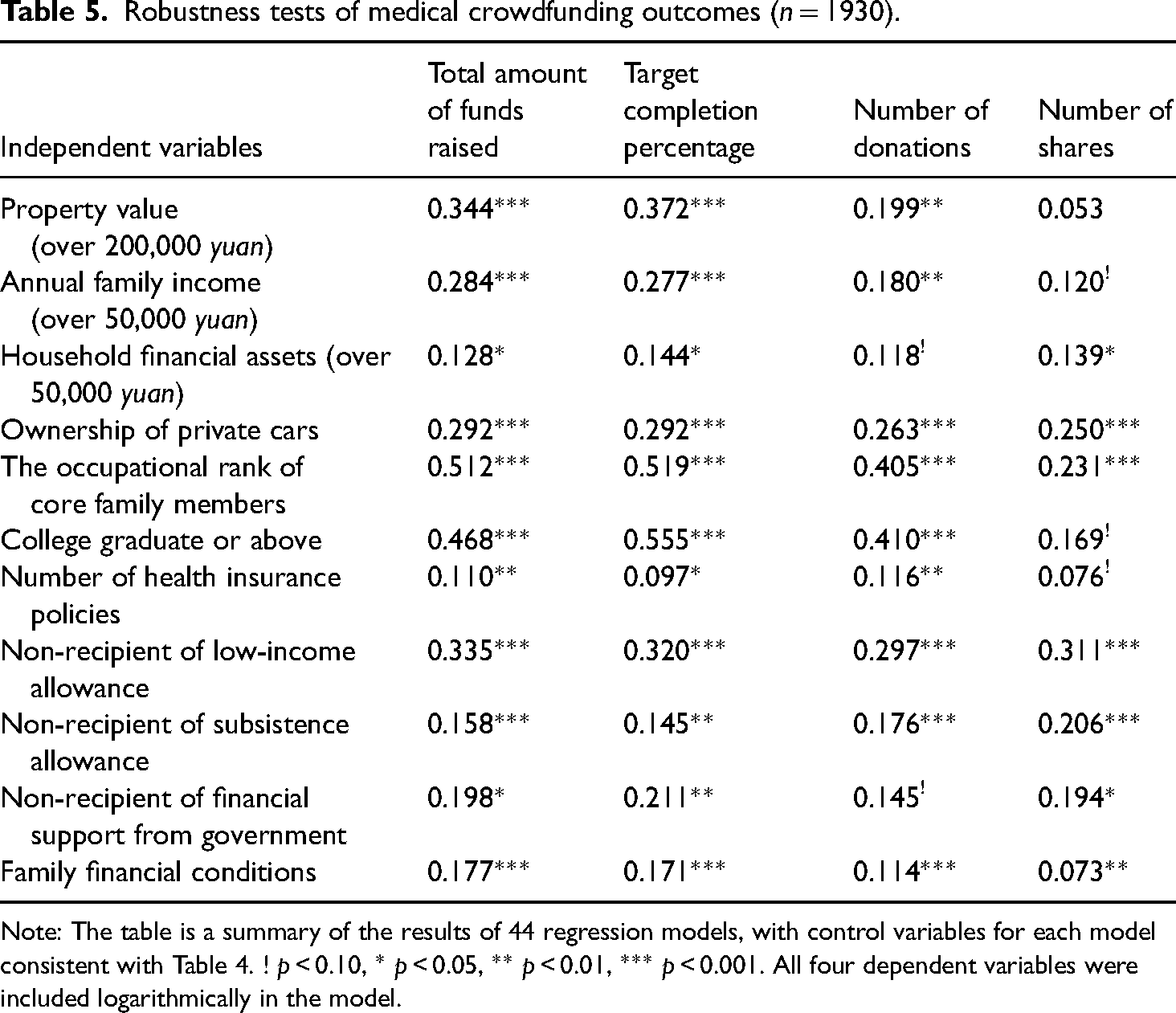
Note: The table is a summary of the results of 44 regression models, with control variables for each model consistent with Table 4. ! p < 0.10, * p < 0.05, ** p < 0.01, *** p < 0.001. All four dependent variables were included logarithmically in the model.
SES differences in medical crowdfunding outcomes: Mediating effects
In order to understand the mechanisms behind the SES differences in medical crowdfunding outcomes, this study then now explores its mediation. Reprising Table 4, Table 6 adds seven mediating variables covering cultural capital and social capital. The results deliver three important conclusions.
Mediation analysis of the effect of socioeconomic status (SES) on medical crowdfunding outcomes (n = 1930).
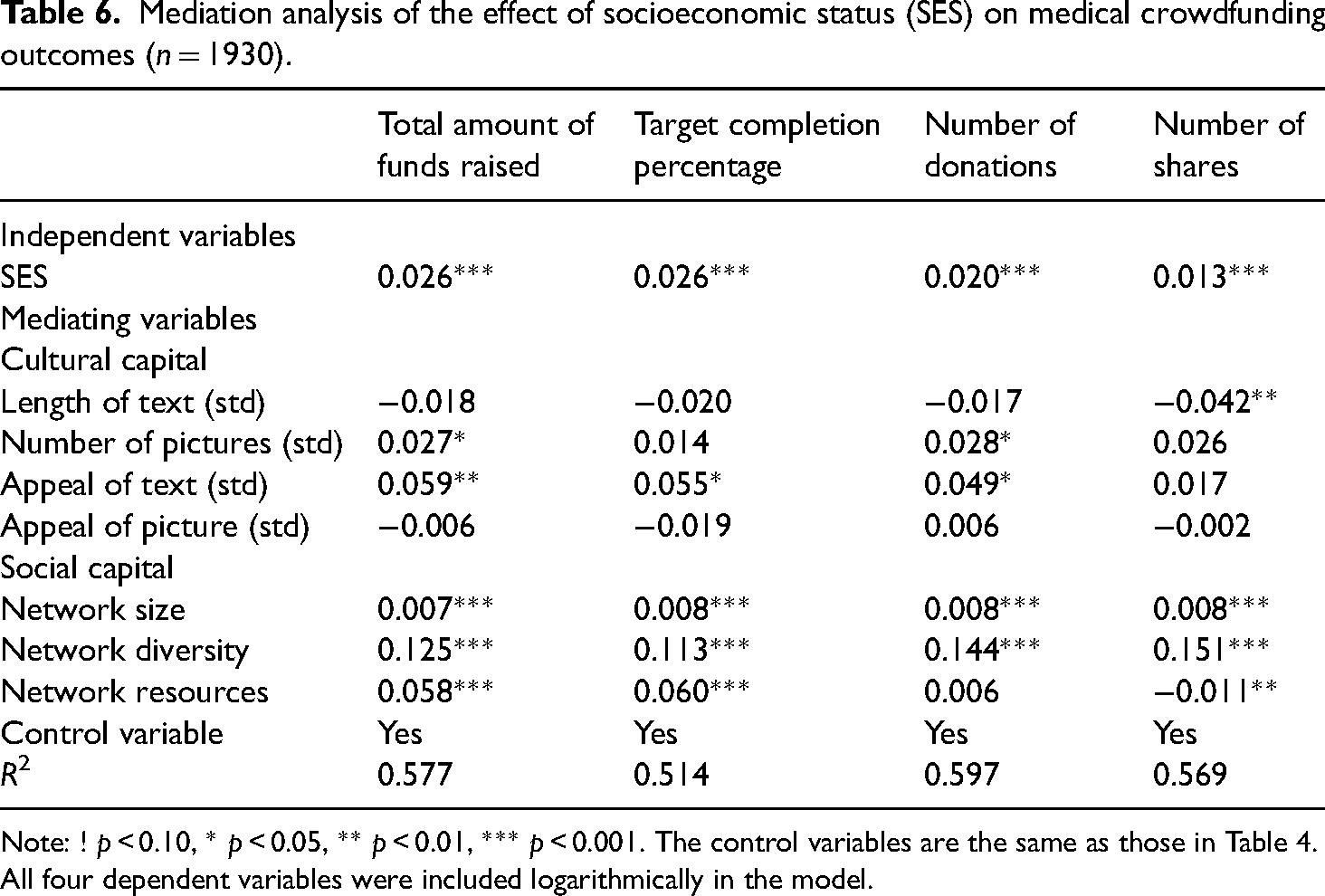
Note: ! p < 0.10, * p < 0.05, ** p < 0.01, *** p < 0.001. The control variables are the same as those in Table 4. All four dependent variables were included logarithmically in the model.
First, with the inclusion of the seven mediating variables into the model, the coefficients of SES, despite still being significant, drop drastically. Taking the total amount of funds raised as an example, the coefficient of family SES decreases from 0.047 to 0.026, which suggests possible mediating mechanisms underlying its effect on medical crowdfunding outcomes.
Second, narrative competency, an indication of cultural capital, has a moderate positive effect on fundraising outcomes. The more images offered, the more donations a campaign receives, and the more funds it receives. The more emotionally appealing the text is, the more donations the campaign receives; the more funds are raised; and the higher the proportion of target fundraising amount reached. However, a positive influence of text length and image appeal was not observed under the mutual control condition; in contrast, the longer the text was, the less likely it was to be forwarded.
Third, the offline social capital has a strong impact on fundraising outcomes. The larger and more diverse in terms of the WeChat networks of the help-seekers and their families, the larger and the more diverse the network is, the more donations and shares a campaign gets, the higher the total amount of money received, and the higher the target completion percentage. The more abundant the network resources of the help-seekers and their families, the more money they receive and the higher the target completion percentage is. However, network resources are not positively correlated with the number of donations, and can even have a negative impact on the number of shares. This indicates that with other variables controlled, network resources affect the total amount of funds raised and the target completion percentage, that is, the quality of crowdfunding instead of its quantity. Conversely, the diversity of the network can affect both its quality and the quantity.
In order to decompose the mediating effects of these variables, bootstrapping is introduced, as listed in Table 7. It can be seen that the total effect is consistent with the regression coefficients of family SES in Table 4, while the direct effect is consistent with that in Table 6. The indirect effect of the seven mediators has an overall explanatory power of around 40–50% (seen from the last row), but they differ in the size of effect.
Bootstrap test of mediating effects on medical crowdfunding outcomes (n = 1930).
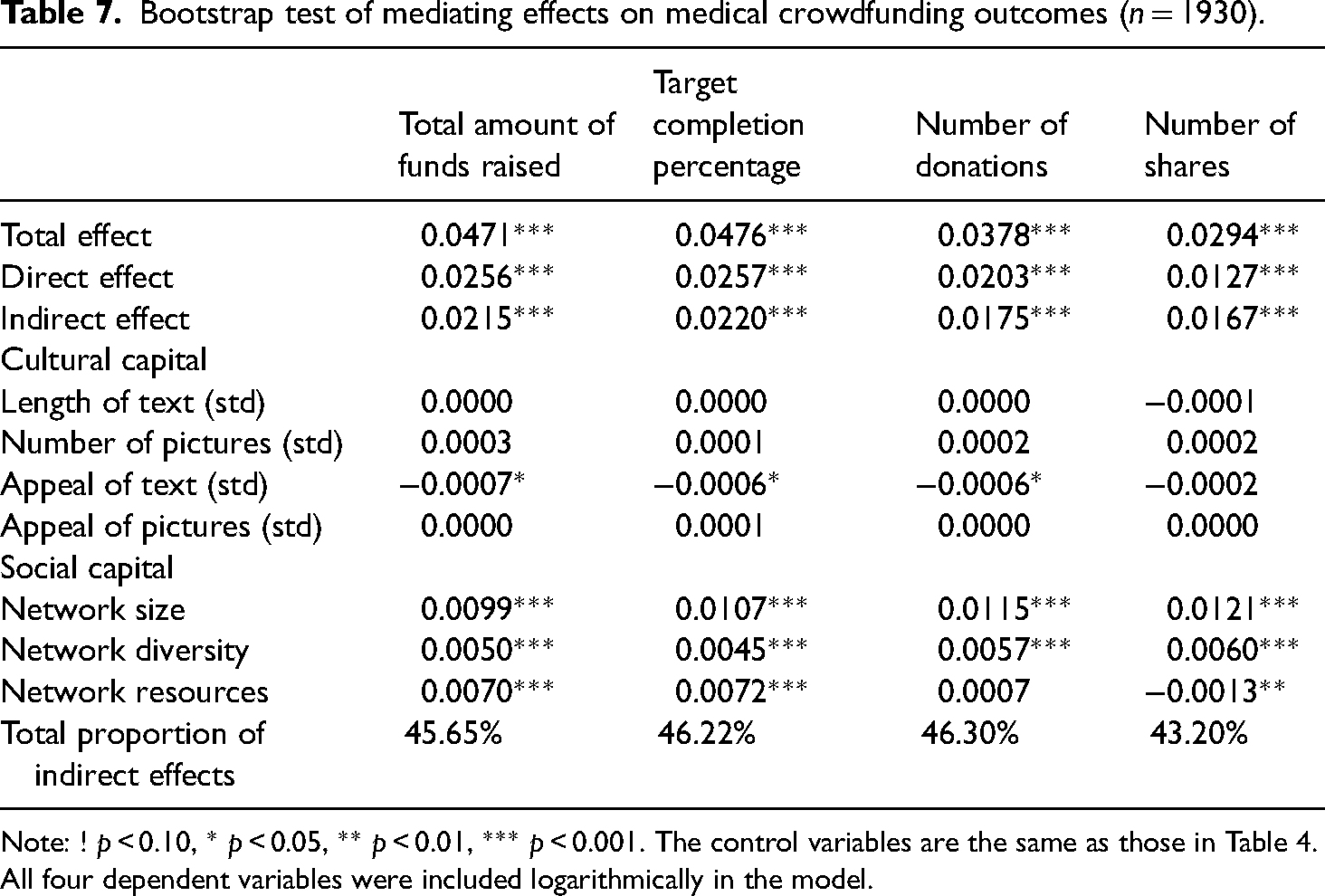
Note: ! p < 0.10, * p < 0.05, ** p < 0.01, *** p < 0.001. The control variables are the same as those in Table 4. All four dependent variables were included logarithmically in the model.
First of all, in terms of the total amount of funds raised and how close it is to the fundraising goal, network size is found to be the most influential mediator, followed by network resources, and then network diversity.
Second, the appeal of the fundraising text, as one of the four indicators for cultural capital, is the only significant mediator, yet it is negative. This is contrary to the theoretical expectation that appealing texts could contribute to fundraising.
However, also contrary to our expectations, such more appealing texts do not come from families with higher SES, but from those with lower SES, which means that the influence of rhetorical appeal gives way to the emotional appeal of the event itself in medical crowdfunding.
Finally, it is worth mentioning that more network resources lead to significantly fewer shares with other variables controlled. There are two reasons for this: first, diverse network resources help facilitate a successful fundraising within a small number of shares; second, some contacts with high SES could be inclined to donate more instead of sharing the campaign in their social networks out of a concern for personal reputation and image management, as discussed above. Considering that even campaigns of those in the top 10% of in terms of SES spectrum in our sample achieve less than 40% of their fundraising goals, we prefer the second explanation.
How to optimize the outcomes of medical crowdfunding
To further explore the role of fundraising channels in reducing or even reversing the disadvantages of the more underprivileged groups in crowdfunding, this study compares the fundraising outcomes of the two types of campaign, those promoted only on WeChat (“single channel”) and those being promoted on WeChat and also on the homepage of the crowdfunding platform (“mixed channel”; Table 8). The main effects and interaction effects of family SES and channel type in Models 1–4 are statistically significant, indicating that the effect of the family SES is more significant for single-channel campaigns than for mixed-channel campaigns. For example, in Model 1, the regression coefficient for family SES decreases from 0.095 for single-channel campaigns to 0.033 for mixed-channel campaigns, 14 a decrease of 65.3%. Models 2–4 show the same trend, with declines of 68.6%, 66.7%, and 52.0%, respectively. Thus, Hypothesis 3 is supported: the socioeconomic inequality in medical crowdfunding depends on the channels used to promote the crowdfunding campaign. As opposed to a single channel, the mixed-channel model can reduce, even if not reverse, the socioeconomic inequality of crowdfunding outcomes.
Multiple linear regressions of medical crowdfunding outcomes (n = 1930).
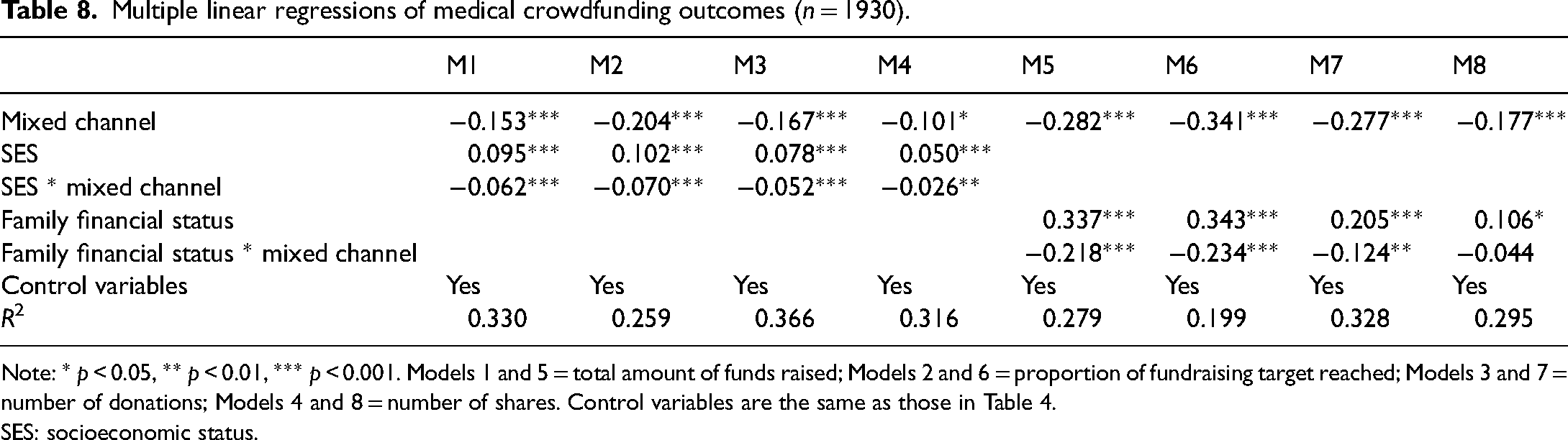
Note: * p < 0.05, ** p < 0.01, *** p < 0.001. Models 1 and 5 = total amount of funds raised; Models 2 and 6 = proportion of fundraising target reached; Models 3 and 7 = number of donations; Models 4 and 8 = number of shares. Control variables are the same as those in Table 4.
SES: socioeconomic status.
To further support Hypothesis 2, this study performs a robustness check (Models 5–8 in Table 8). We use family financial status to replace family SES. The results are consistent with the first four models: the effect of family financial status on fundraising outcomes is greater with the single channel, but significantly reduced with the mixed-channel model. The declines in Models 5–8 range from 41.5% to 68.2%. Therefore, Hypothesis 3 is supported in the robustness test. 15 It is important to emphasize that SES still has a significant positive effect on fundraising outcomes in the single- and mixed-channel models. Even when fundraising campaigns are displayed on public websites, the SES effect cannot be reversed but only be weakened to a certain extent. Therefore, social welfare still has a long way to go, considering that public websites are far less influential than private networks in medical crowdfunding.
Conclusion and discussion
In recent years, mobile-internet-based medical crowdfunding has provided a new means for the underclass to get emergency assistance. While crowdfunding scandals have emerged through the media, these events cannot erase the social contribution of medical crowdfunding platforms. Public opinion and sentiment highlight the issues of significance: are resources being directed to those in the greatest need and how can this be optimized? Therefore, the possible socioeconomic gradient in medical crowdfunding outcomes is our primary interest in this study. It is interpreted via three questions: To what extent is the SES of the patients and their families associated with medical crowdfunding outcomes? What are the underlying mechanisms? Is there a way to optimize this?
Our quantitative analysis of large-scale empirical data reveals a significant socioeconomic gradient in medical crowdfunding outcomes, with SES having a significant positive effect. Groups with relatively higher SES have more flexible resources and thus they are able to raise more funds, get closer to their fundraising goals, get more donations, and get more shares than other groups. Contrary to the social expectation that the poor and needy are helped the most, differences in medical crowdfunding outcomes embody the disparities in access to healthcare based on SES.
Why do patients with higher SES have better outcomes? Our mediation analysis shows that offline interpersonal networks play an important mediating role in the effect of SES on crowdfunding performance. That is, the higher the SES of the help-seekers and their families, the larger their network sizes, the more diverse their networks are, and the more network resources they have. Social capital, as manifested in network quality, promotes the diffusion of donation request and effective mobilization of ties, and thus improves the outcomes of crowdfunding campaigns. In addition, although cultural capital, embodied in narrative competency, contributes to the effectiveness of crowdfunding, its correlation with family SES is weak and does not constitute an intermediary mechanism connecting family SES and crowdfunding effectiveness.
In addition, this paper also focuses on ways to weaken the socioeconomic inequality in online medical crowdfunding outcomes. The paradox of seeking help lies in the channel where the campaign is promoted. Compared with campaigns that are only shared through personal networks, campaigns displayed on the platform homepage are less negatively impacted by the lower SES of help-seekers. As crowdfunding campaigns move from within private social networks to public platforms, they reach a broader audience who do not know the family, and this can help families with lower SES to raise more money. Unfortunately, our results also show that while being displayed on the homepage can greatly reduce the adversity of disadvantaged groups, it cannot entirely reverse SES disparities in outcomes.
The study also describes the socioeconomic inequalities in crowdfunding outcomes from the dynamic perspective of campaign development, finding that the campaigns of lower SES people have shorter survival time and a lower average amount of money raised, and with the passage of time, these two disadvantages worsen, which is worthy of reflection. It is generally believed that, over time, the spread of help-seeking campaigns from networks of acquaintances to public networks can not only break the influence of status homogeneity, but also strengthen the ethics by which help is directed to first and foremost supporting the poor and the weak, thereby closing the fundraising gap. In contrast, our results reveal that groups with lower SES have a harder time getting their message out, and even when their message does get out, it tends to be restricted to members of society who are less able or willing to donate.
Although the “paradox of seeking help” is empirically supported, the vast majority of people who seek help via medical crowdfunding campaigns and their families are still those with lower SES compared with the whole society, or at least are “temporarily vulnerable”. This is because families in the upper and middle classes can pay their own medical bills for critical illnesses without having to initiate crowdfunding campaigns. Therefore, the paradox of seeking help in this study has only been supported in the context of the online medical crowdfunding campaigns. In other words, medical crowdfunding based on WeChat still opens up entirely new ways for the underprivileged to seek help, even if the results are less than ideal. On the one hand, only 1.65% of the fundraisers achieved their fundraising goals; on the other hand, out of the 1930 campaigns we observed, none of the bottom 10% in terms of SES achieved their fundraising goals, while 7% of the top 10% in terms of SES fully achieved their targets. In other words, when higher SES groups try to get a piece of the philanthropic crowdfunding, they get a larger piece of it than expected. Therefore, how to effectively use ethics and regulations to contain speculators, how to break the paradox of seeking help through technology, and how to allocate social resources to those who need them the most, is a practical issue worthy of discussion by people from all walks of life.
This study also helps social scientists understand the relationship among the mobile internet, social capital, and inequality. The digital divide has been a subject of extensive academic discussion in recent years, but most researchers are concerned with inequality in internet access (Li, 2006; Qiu et al., 2016) and rarely attend to another important issue: Does the internet reduce, reproduce, or even widen social inequality? This study shows that families with higher SES are more likely to access medical crowdfunding platforms, which implies that mobile internet technology, at least in some cases, plays a major role in reinforcing inequalities in resource attainment. It is worth noting the following. First, this paper does not take into account unequal internet access. It is possible that groups with particularly low SES do not use the necessary technology and thus are not covered by this study, or high SES groups do not use this approach to access resources. The former will lead us to underestimate the role of the internet in widening/reproducing inequality, while the latter will cause us to overestimate it. Second, researchers also need to be aware of the channels used to promote medical crowdfunding campaigns, which may have a decisive impact on whether crowdfunding reproduces inequalities or not. The paradox of seeking help in this study is observed on the mobile internet application WeChat, on which social networks are online extensions of offline interpersonal networks. Therefore, it is another manifestation that individual social capital reproduces inequality. If the person seeking help can surpass their homogeneous private circles and enter the public internet space, and gain a share of the social capital of more diverse groups, socioeconomic inequality in fundraising outcomes may be significantly reduced. This means that internet platforms with other modes of operation, such as Tiktok (Tu and Zhou, 2019) and the microblogging platform Weibo (like Twitter) (Yin, 2018), may help reduce inequality. Therefore, researchers should avoid a general conclusion as to whether the internet can reduce social inequality or not, and rather need to place it in the context of the specific institutional rules of different online arenas.
Understanding the SES inequality of medical crowdfunding has some policy implications concerning how to better protect poor families during difficult times and help them avoid falling into the poverty. First, the government should pay attention to inequality in medical crowdfunding, and provide more safeguard measures for poor families, in particular through precise poverty alleviation to reduce disease-induced poverty and prevent smaller medical conditions from developing into more serious ones. Second, public medical crowdfunding platforms can continuously optimize their mode of dissemination, helping the campaigns of more disadvantaged individuals to reach the general public. Social platforms need to focus not only on displaying campaigns on their own platforms, but also on finding ways to work with other platforms to help patients make their voices heard on larger media or social platforms. Finally, while optimizing the medical crowdfunding system, the government should also continue to improve the existing public healthcare system so that major disease insurance could play a greater role in supporting poor families with serious diseases.
Due to the lack of survey data, we have only analyzed online fundraising but not offline donations, so the SES differences in medical crowdfunding could be underestimated in this paper. Of the 1930 cases, there is one case worthy of special attention in this regard. Dong Wang (alias), a 40-year-old male who graduated from college in 2001, was a high school teacher in a provincial capital city, with a spouse who was also a teacher in a public school. Their family SES was relatively high among the cases collected. Wang, who suffered from amyotrophic lateral sclerosis (ALS), launched a campaign on the medical crowdfunding platform with a target of 600,000 yuan, and reached his fundraising goal in just four days. It was alarmingly fast. One quote from Dong Wang's thank-you note is worth quoting: The headmaster of our junior high school … and other leaders and colleagues came to visit with sincere greetings and the first donation of 50,000 yuan …, after that, the General Party Branch of the Communist Party of China (CPC) and all the CPC Party branch, trade union, and other faculty of the school also took action to start charity donations for us and raised 188,100 yuan for us.
It is unfortunate that Dong Wang was ill, but he was also lucky to have quickly and successfully raised enough money online and also to have received more than 200,000 yuan in offline donations thanks to his employer and the CPC Party branch, which is beyond the reach of most patients without jobs in state-owned/funded institutions. Therefore, if we take offline donations into account, the socioeconomic inequality of medical crowdfunding may be even worse.
Footnotes
Acknowledgements
The authors thank Yang Shen and the anonymous reviewers for the helpful comments and suggestions. The ideas expressed herein are those of the authors.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Contributorship
Cheng Cheng is responsible for conceptualization, investigation, data curation, project administration, and acquiring funding. Yifei Ren is responsible for data curation and visualization. Both authors collaborate on writing, editing, and reviewing the manuscript.
Funding
This work was supported by the Key Project of the Jiangsu Social Science Fund of China (grant no.: 23SHA003).