
Abstract
Although there has been a longstanding curiosity about the socio-political consequences of China’s remarkable urban–rural divide, we have yet to understand the divide’s possible influence on mental health. Using data from the 2016 wave of the China Labor-force Dynamics Survey (CLDS), we find that depressive symptoms of both rural–urban migrants and rural residents are significantly higher than those of urban residents. Consistent with the fundamental-causes-of-disease and stress-exposure perspectives, results from zero-inflated negative binomial regression suggest that such differences in depressive symptoms can be attributed to socioeconomic status and proximate stressors such as unemployment, living alone, and the unaffordability of medical services. In particular, the rural–urban difference in depressive symptoms is explained away by educational attainment. A further investigation using spline Poisson regression suggests that the protective effects of the period of middle school, which vary substantially across demographic groups, are especially relevant to the rural–urban disparity in depression. We argue that hukou is a fundamental cause of disease in China and mental health is an important yet understudied area where China’s salient urban–rural inequality strikes.
Keywords
Introduction
In China, hukou, the household registration system, is an institutional arrangement that categorizes people according to their place of birth and subsequently determines their (unequal) rights, privileges, and access to resources (Chan and Zhang, 1999; Fu and Ren, 2010; Lin and Bian, 1991; Tong and Piotrowski, 2012; Wu and Treiman, 2007). It is widely argued that social inequality in contemporary China results more from institutional arrangements such as hukou or danwei (one’s work unit) than from individual characteristics (Bian and Logan, 1996; Fu and George, 2015; Lin and Bian, 1991; Walder, 1992; Zhou, 2000). Social stratification, or more precisely, unequal access to resources, social support, and health care, is shown to be a key driving force in determining the mental health inequality across societies and political economies (Aneshensel et al., 2013; Miech et al., 1999; Muntaner et al., 2007; Wheaton, 2001). Therefore, it is worthwhile to explore the ramifications of China’s hukou system for mental health across social groups. Although mental health in China has attracted considerable attention in recent years from epidemiologists, demographers, and medical sociologists (Chen et al., 2010; Graham et al., 2017; Shi et al., 2016; Yip et al., 2007), this specific research question has yet to be thoroughly investigated.
To address this question, we analyze data from the most recent wave (2016) of the China Labor-force Dynamics Survey (CLDS). More specifically, we employ zero-inflated negative binomial (ZINB) models and spline Poisson regression models to address the following questions: (a) Does a rural–urban disparity in mental health exist in China? (b) If yes, what socio-economic indicators in contemporary Chinese society may account for such a disparity? and (c) If there were a key variable shaping the rural–urban disparity in mental health, how would it moderate mental health inequality? Next, we discuss the relevance of hukou to mental health in contemporary China.
Does hukou matter for mental health? Stratification and mental health in China
Students of social stratification are often motivated by two major questions: how social inequality comes into being, and what social inequality produces and reproduces (Link and Phelan, 1995; Phelan et al., 2004; Williams and Collins, 1995). Regarding the first question, inequality occurs at both the individual and group levels. For example, significant variations in income occur not only among individuals, but also across social groups defined by, for example, gender, ethnicity, immigration status, or place of origin. While theorists propose several concepts (e.g., categorical inequality, horizontal inequality, and between-group inequality) to understand how social inequality arises among individuals who have similar attributes but are positioned in segmented social groups (Jiang et al., 2012; Stewart, 2016; Tilly, 1998), the link between socio-political segmentation and inequality has attracted significant attention in recent years (Lin, 2000; Massey, 2007; Stewart, 2016).
The extensive impact of the hukou system on social inequality in China has been an important research topic in recent decades (Chan and Zhang, 1999; Fu and Ren, 2010; Wu and Treiman, 2007; Xu and Xie, 2015). Established in the 1950s, hukou divided the Chinese population into agricultural hukou holders in rural areas and non-agricultural hukou holders in cities. Prior to China’s economic reforms starting in the late 1970s, the migration of agricultural hukou holders was severely restricted to prevent a shortage of people and resources devoted to agricultural production. Given that China’s economic reforms developed a strong demand for cheap labor in urban and coastal areas, the hukou’s role in controlling rural–urban migration has gradually been lessened (Chan, 1994; Fu and Ren, 2010). One consequence of the deregulation of rural–urban migration in China is an influx of rural–urban migrants who are neither urbanites according to their de jure registration status, nor villagers based on their de facto work/residence locations. Yet, it is misleading to interpret the trend of massive rural migration as a retreat of hukou in Chinese society; due to their agricultural and nonlocal hukou status, the rural migrants—referred to by demographers as the ‘floating population’—are not entitled to public services, welfare benefits, or local resources such as education and housing in urban China (Chan and Buckingham, 2008; Whyte, 2010). The hukou system continues to play a key role in producing socioeconomic disparities in China because one’s place of birth is inextricably linked with access to social benefits, availability of state resources, and career opportunities (Chan and Zhang, 1999; Fu and Ren, 2010; Wu and Treiman, 2007).
Today, China is probably one of the most unequal societies in the world, and the rural–urban divide has been shown to be a driving force behind China’s social inequality (Wu and Treiman, 2004; Xie et al., 2012; Xie and Zhou, 2014). Despite recent reforms to the hukou system, scholars still view it as a key institutional arrangement shaping social stratification in Chinese society (Rarick et al., 2017; Xie and Zhou, 2014; Zhang and Treiman, 2013). While prior studies on hukou have tended to focus on inequalities in income, wealth, housing, life chances, and physical health (Chan and Zhang, 1999; Kanbur and Zhang, 1999; Liu, 2005; Lu and Qin, 2014; Wu and Treiman, 2007), we argue that the impact of hukou on mental health should not be under-estimated. The existing literature often approaches the socioeconomic gradient in mental health from a micro-level perspective and views the mental health disparity in China as a consequence of individual backgrounds and characteristics (Chen et al., 2010; Graham et al., 2017; Shi et al., 2016). In these studies, the socio-political nature of hukou was not sufficiently developed. For example, Yip et al. (2007) examined the association between social capital and mental health in rural China and found that, at the individual level, trust affects the subjective well-being of rural peasants. Using a survey of 210 unemployed migrant workers in Zhejiang Province, Chen et al. (2012) investigated the effects of the duration of unemployment and related coping strategies on mental health. This research suggested that long-term unemployment and under-developed coping strategies are associated with the mental health problems faced by these unemployed migrant workers. Most recently, Graham et al. (2017) studied the correlations between psychological health and individual traits such as age, education, and income. They found that urban educated Chinese are more likely to report depression than others. Again, hukou was recognized in this study as an individual characteristic rather than as the institutional backdrop against which the mental health of segmented social groups is differentiated.
The focus of these studies, which situated the link between hukou and mental health within the macro context of China’s socio-political transformation, tended to be on specific social groups, such as rural migrants, left-behind children, or rural residents. For instance, using data collected in Beijing in 2004 and 2005, Lin et al. (2011) found that both the experience of discrimination and perceived social inequity were strongly associated with mental illness among rural migrants. Drawing on a panel dataset of more than 19,000 students from 252 rural primary schools in northwestern China, Shi et al. (2016) reported a significant and negative association between parental out-migration and the mental health of left-behind children in rural China. Similarly, a different study by Lu et al. (2012) also suggested that adults in rural households with out-migrants are at a higher risk of depression than those in households without out-migrants, despite the fact that monetary remittances can compensate for the mental cost of out-migration. In a study of rural children, Xu and Xie (2015) found that migrating with their parents had no negative effect on the children’s subjective well-being. While these studies are valuable for understanding the broad impact of a particular institutional arrangement on psychological well-being, we have not thus far developed a more holistic view of how the link between hukou and mental health is differentiated among segmented social groups.
More recently, a few studies have compared differences in physical health (rather than mental health) between social groups defined by hukou, such as between rural migrants and urban residents, or between rural residents and urban residents. In order to test for selective migration in China, Tong and Piotrowski (2012) compared the health status of migrants and non-migrants using data from the 1997–2009 waves of the China Health and Nutrition Survey. They found that migrants were positively selected on the basis of health. Based on a nationally representative survey, the analysis conducted by Niu and Qi (2015) showed that rural migrants in urban areas were generally healthier than urban natives, but residents with non-agricultural hukou were healthier than those with an agricultural hukou. Yet, given this study’s focus on physical health, it remains unclear whether the rural–urban disparity also exists in mental health. In this regard, one study published in The Lancet appeared to support the link between hukou-based segmentation and mental health. Based on an epidemiological survey conducted from 2001 to 2005 in four provinces, Phillips et al. (2009) found that rural residents were more likely than urban residents to have depressive disorders and alcohol dependence. Likewise, a qualitative study conducted in eleven provinces in China suggested that suicide, especially elderly suicide, has increasingly been a critical issue in rural China since the 1980s (Liu and Fu, 2017). In the present study, drawing upon two influential frameworks explaining (mental) health disparities across different socio-cultural contexts—the fundamental-causes-of-disease and stress-exposure perspectives—we further explore the pathways through which the hukou system may affect mental-health conditions of segmented demographic groups.
Hukou and mental health: Exploring possible mechanisms
Sociological research on mental health is informed by two conceptual frameworks, one focused on the fundamental causes, and the other on the proximate determinants of diseases. As posited by the fundamental-causes-of-disease framework (Link and Phelan, 1995; Phelan and Link, 2005), social conditions such as education, income, and social support serve as underlying forces driving inequalities in health. Because the privileged always have more access to health services, better knowledge of risk factors for diseases, and earlier exposure to advances in clinical practices and medical technology, economic growth and social development will not eliminate the socio-economic gradient in health. Rather, health inequality persists in any society in which power and resources are distributed unevenly across social groups. According to this fundamental-causes perspective, policy makers’ focus on risk factors (or proximate causes) of diseases—things such as inactivity, air pollution, and neighborhood disadvantage—is likely to be misplaced. The development of effective interventions is then based on a concrete understanding of what fundamental causes subject people to these risk factors.
The concept of fundamental causes of diseases points to the significance of underlying social conditions in shaping the epidemiology of diseases; however, the stress-exposure framework focuses on proximate causes (or risk factors) and offers a different explanation of mental health inequality within a society (Gee and Payne-Sturges, 2004; George and Lynch, 2003; Lantz et al., 2005). As suggested by this latter framework, the reason why certain socio-demographic groups appear to be more susceptible to mental illness has nothing to do with their intrinsic vulnerability. Similarly, if scholars were able to measure stressors in a more comprehensive way (Lantz et al., 2005) or properly model the impact of stressors on mental illness (George and Lynch 2003), exposure to a wide range of social, economic, or environmental stressors might account for more mental health problems experienced by the disadvantaged groups.
Both conceptual frameworks are useful in exploring the link between hukou and depressive symptoms of segmented demographic groups. According to the fundamental-causes-of-disease theory, inequality in social conditions is a primary vehicle through which the health disparity comes into being and perpetuates itself. In empirical research across different societies, such inequality in social conditions is often operationalized by measures of socioeconomic status. Our first hypothesis is thus formulated as follows: Hypothesis 1: Differences in depressive symptoms among demographic groups segmented by hukou are attributable to inequality in socioeconomic status. Hypothesis 1A: Among the various indicators of socioeconomic status, education (especially the period of compulsory education) is most relevant to the rural–urban disparity in depressive symptoms. Hypothesis 2: Differences in depressive symptoms across segmented demographic groups are related to their differential exposure to proximate (social, economic, or medical) stressors.
Data and methods
Data
This study is based on the latest wave (2016) of the CLDS, which is administered by the Center for Social Surveys at Sun Yat-sen University. As a large-scale nationally representative survey of China’s labor force, the CLDS covers all provinces in mainland China except for Tibet and Hainan. A multistage stratified cluster sampling technique with probability proportionate to size (PPS) was employed by the CLDS to select households from a selected residents committee (RC, or juwei hui) or peasants committee (PC, or cunwei hui). The 2282 counties (xian), county-level cities, or county-level districts served as the primary sampling units. Street offices (jiedao ban) and townships (zhen) within a selected county and then RCs and PCs within a selected street office or township, respectively, were randomly chosen. Face-to-face interviews were conducted by trained interviewees using a Computer Assisted Personal Interviewing (CAPI) system. The response rate for the 2016 wave was 71.0% (81.6% in rural areas and 60.9 % in urban areas). Our analysis is based on 12,555 individuals from the 2016 CLDS project.
Measures
The outcome variable is the Center for Epidemiologic Studies Depression (CES-D) 20-item self-reported depressive symptom scale (Lewinsohn et al., 1997; Radloff, 1977). The CES-D scale asks respondents to assess how often over the last week they experienced any of the 20 depressive scenarios/items, including sleeping, appetite, loss of interest, sadness, and fatigue. The response categories for each item are the same: rarely or none of the time (0 days and coded as zero), some or a little of the time (1–2 days and coded as one), moderately or much of the time (3–4 days and coded as two), and most or almost all the time (5–7 days and coded as three). The Cronbach’s alpha of these 20 items reported by respondents is 0.95, suggesting high internal consistency. The CES-D score, or the sum of scores of the 20 CES-D items, is used as the outcome variable and a higher score indicates that a respondent is more depressed (Ragland et al., 2005).
Because the main thrust of this study is to investigate the mental health conditions of demographic groups segmented by hukou, the overall sample was categorized into three groups: rural residents, rural–urban migrants, and urban residents. These three groups are defined by their de jure hukou status and de facto residence. Rural residents had agricultural hukou status and resided in rural areas; rural–urban migrants also had agricultural hukou status but lived in urban areas at the time of interview; and urban residents held non-agricultural hukou status and resided in urban areas (urban-to-urban migrants are also included in this category). It should be noted, however, that the pattern of internal migration in China is more complex than that revealed by the three demographic groups. For example, the original dataset also included 201 individuals who held non-agricultural hukou but lived in rural regions. Yet, the three categories investigated here allow us to have a general picture of the Chinese population segmented by hukou.
Several socioeconomic indicators are considered. Since the link between hukou and education has been well documented in the existing literature (Chan, 2009; Fu and Ren, 2010; Heckman, 2005), educational attainment is measured by a categorical variable consisting of four categories: primary school, middle school, high school, and college or above. Income is measured by a continuous variable denoting the logarithm of annual per capita household income. For one’s occupation, we consider two dummy variables denoting administrative jobs (e.g., government officials, military officers, and local cadres) and professional jobs (e.g., professors, doctors, and lawyers), respectively, and treat all other jobs as reference. Given the documented impact of work units on one’s (mental) health status (Fu and George, 2015; Lai, 1995), a dichotomous variable, state-sector employment, is included to denote whether respondents work in state sectors (governments, institutes, or state-owned enterprises).
A series of proximate stressors related to mental illness are incorporated into this research (Baker et al., 2013; Dean et al., 1992; Kessler et al., 1987; World Health Organization, 2001). Given that unemployment, living alone, and housing tenancy are possible risk factors for mental illness (Baker et al., 2013; Dean et al., 1992; Evans et al., 2003; Kessler et al., 1987), these stressors are denoted by three dichotomous variables. Stressors pertaining to conditions of physical health and medical services are also considered due to their known consequences on mental health (Phelan et al., 2001; Richardson et al., 2005). In China, the public insurance program (gongfei yiliao) covers the majority of, if not all, medical expenses and is often provided to state employees (Shi, 1993). The absence of such coverage is denoted by a dichotomous variable, unavailability of public medical insurance. In the 2016 CLDS survey, respondents were asked whether cost was the reason they did not see a doctor or visit a clinic when they were sick. A dichotomous variable, unaffordability of medical services, is coded as one if a respondent reported such a scenario. The presence of any self-reported occupational disease is also denoted by a dichotomous variable. Finally, control variables are male (female as reference), age (in years), being married (other marital status as reference), and region (coastal, central, and western areas).
Methods
We consider the outcome variable, the sum of scores of the 20 CES-D items, as a count response. Generalized linear models from the Poisson family of distributions are often used to model count responses (Fu et al., Forthcoming; Fu et al., 2017; Long and Freese, 2006; Powers and Xie, 2008). Since mental disorders are distributed unevenly across socio-demographic groups in China (Parker et al., 2001; Phillips et al., 2009), these Poisson-based models are particularly useful in analyzing skewed counts of depressive symptoms (Cacioppo et al., 2006; Hays et al., 1998; Wade et al., 2002). The Poisson distribution requires that its mean be the same as its variable, which is seldom satisfied in empirical data. In practice, researchers find that the variance of count data tends to be larger than its mean, which is referred to as overdispersion. By and large, two methods have been proposed to account for overdispersion in count data. First, the zero-inflated Poisson approach deals with excessive zeros in count data and suggests that those who are not at risk of the count response (e.g., depressive symptoms) account for the overdispersion issue (Fu et al., 2016). Second, and in contrast, the negative-binomial approach separately models the variance and the mean of count data and thus allows the former to be greater than the latter. Despite a disproportionately large number of respondents (25.4% of the sample) reporting zero depressive symptoms, it remains unclear whether the zero-inflated Poisson approach is preferred over the negative-binomial approach before formal statistical tests are performed. As expected, a mixture of the two approaches—the ZINB model—outperforms either of the two aforementioned approaches in terms of replicating the empirical distribution (see Figure 1). We thus use the ZINB model to analyze depressive symptoms across demographic groups segmented by hukou. According to the ZINB model (Cameron and Trivedi, 1998), the probability mass function of the count variable (i.e., the CES-D depression score) is as follows
Distributions of observed and predicted depressive symptoms.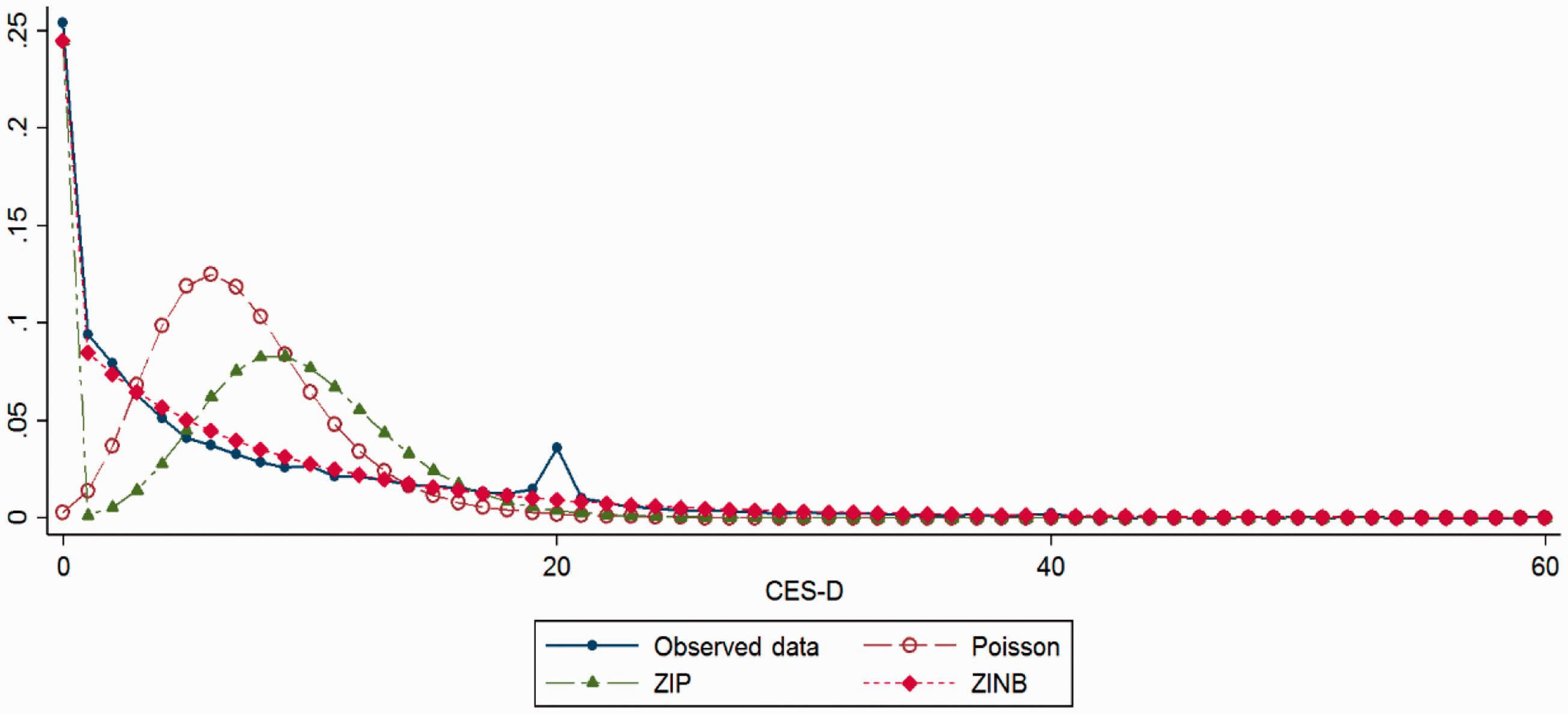

In the equation (1) above, yi is the CES-D depression score and pi is an exposure parameter denoting the probability that a respondent is not at any risk of depression. Here


Equation (1) means that there are two components of the probability that a zero CES-D score (i.e.,
Hypothesis 1A posits that education, especially the period of compulsory education, is most relevant to the rural–urban disparity in mental health. To test this hypothesis across demographic groups, we compare the effects of different stages of educational attainment on depression using spline regression (Fu and Ren, 2010; Marsh and Cormier, 2001). 1 When dummy variables are used to measure educational attainment, the effect of each stage of educational attainment can be understood as a combined effect of the educational attainment being investigated and all lower stages of educational attainment. For example, the effect of high school corresponds to the combination of the effects of high school, middle school, and primary school. Spline regression models are thus used to tease out the separate effects of different stages of educational attainment. To focus on those who are actually at risk of depression, a ZINB model with only control variables (sex, age, marital status, and regional location) was first conducted to identify respondents who are at little risk of depression (defined as probability of zero inflation is greater than 0.9). These respondents who are at little risk of depression were subsequently excluded from the spline Poisson regression analysis. Spline negative binomial regression is also employed in an auxiliary analysis (results not shown here) to assess the association between educational attainment and depressive symptoms, and our key findings remain virtually the same.
Results
A summary of sample characteristics by demographic group (n = 12,555).
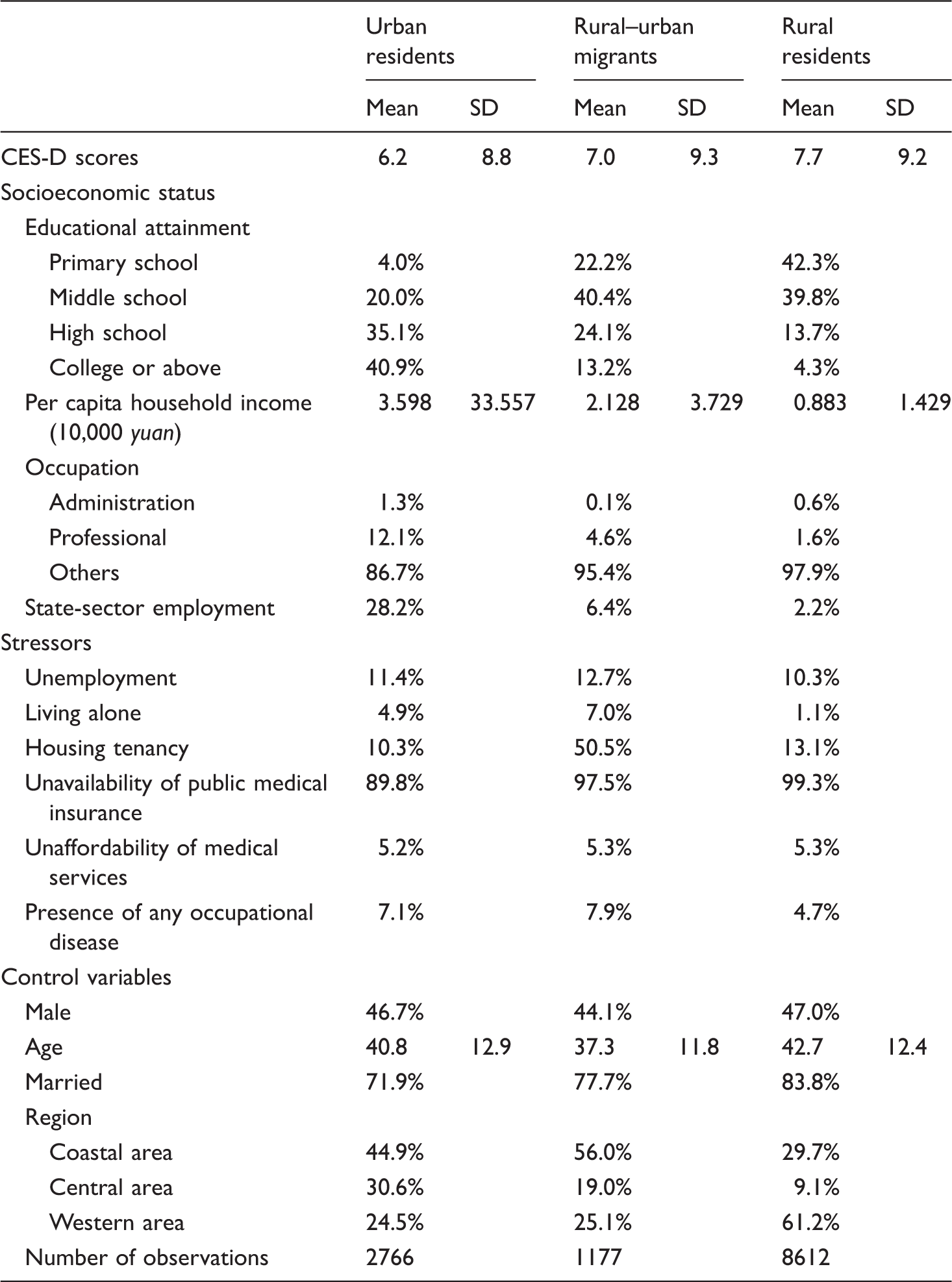
For stressors considered in this research, rural–urban migrants reported the highest level of unemployment (12.7%) among the three demographic groups investigated. As compared to the other two groups, rural–urban migrants were also more likely to live alone (7.0%) and be housing tenants (50.5%). The public (medical) insurance program was essentially unavailable to rural–urban migrants and rural residents (especially the latter). For the three demographic groups, there is little variation in their average proportions of medical services unaffordability. Despite the fact that rural–urban migrants reported the highest prevalence rate of occupational diseases (7.9%), one surprising finding is that rural residents reported the lowest prevalence rate of occupational diseases (4.7%). Given the self-reported nature of this variable, this surprising finding may suggest that rural residents are less aware of their history of diseases (Li et al., 2009). For control variables, rural–urban migrants tend to be female and younger as compared with the other two groups. Respondents who were married account for 83.8% and 77.7% of rural residents and rural–urban migrants, respectively, while the corresponding percentage for urban residents is 71.9%. Over one half of rural–urban migrants (56.0%) were interviewed in coastal areas and most rural residents (61.2%) were interviewed in western areas. Urban residents were distributed more evenly across the three regions.
Results from zero-inflated negative binomial regression: zero inflation of depressive symptoms.
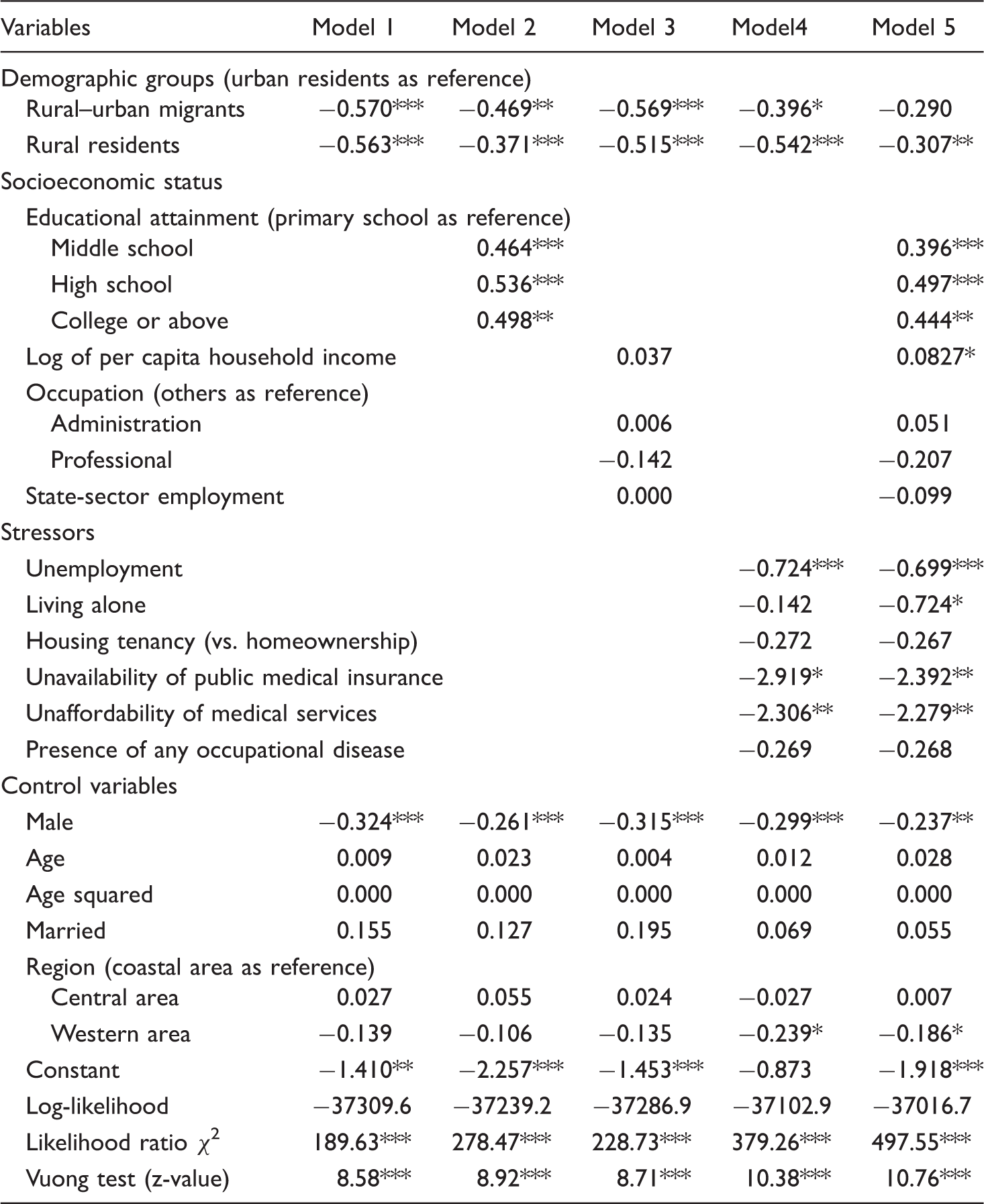
p < .05; ** p < .01;*** p < .001 (two-tailed tests)
Results from zero-inflated negative binomial regression: counts of depressive symptoms.
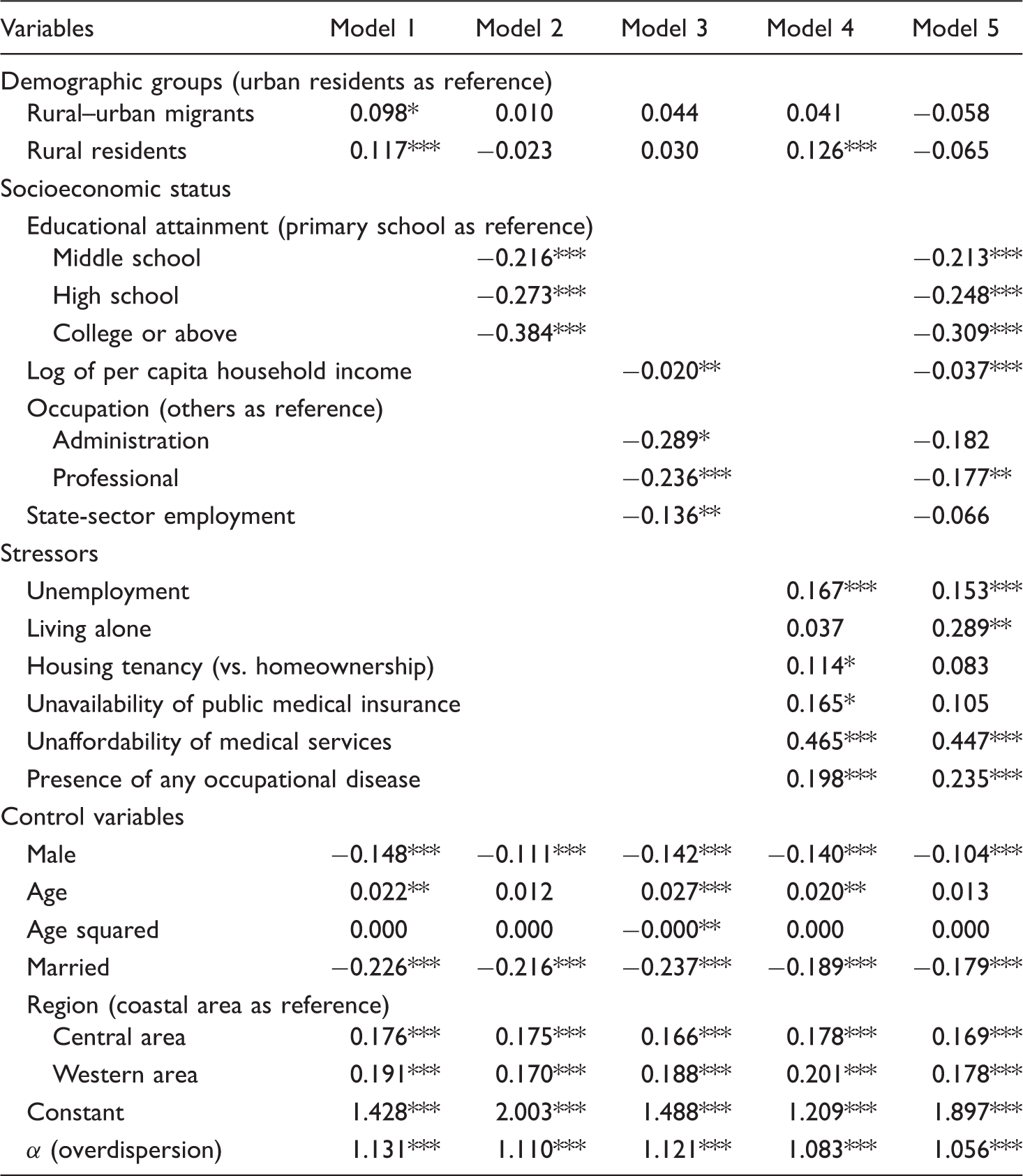
p < .05; **p < .01;***p < .001 (two-tailed tests)
Next, we investigate the depressive symptoms of those who are at risk of depression in order to test our research hypothesis, which is implemented by the negative-binomial component of the ZINB model (see Table 3). As suggested by the significant values of α across the five models, negative binomial models should be employed to address the overdispersion issue. When only control variables are included in Model 1, both rural–urban migrants and rural residents are significantly associated with higher CES-D scores than urban residents with non-agricultural hukou status. Yet, one remarkable finding is that the significantly higher CES-D scores reported by individuals with agricultural hukou status become non-significant once educational attainment is considered in the analysis (see Model 2 in Table 3). Moreover, the association between rural residents and the CES-D score even becomes negative. While other socio-economic variables (income, occupation, and state-sector employment) can also explain away the significant effects of demographic groups on depression, a crossover in the effect of rural migrants is not observed in Model 3. We interpret these findings as support for Hypothesis 1 that the inequality in socioeconomic status plays a key role in shaping different mental health conditions across demographic groups segmented by hukou. Various proximate stressors are then included in the analysis to test Hypothesis 2. In Model 4, rural–urban migrants are no longer significantly associated with higher depressive scores but rural residents are. Hypothesis 2 is thus partially supported. When all measures are incorporated in Model 5, the association between demographic groups and the CES-D score is non-significant. Among socioeconomic variables, education, income, and having a professional job appear to be protective factors in mental health; unemployment, living alone, unaffordability of medical services, and the presence of an occupational disease are risk factors for depression. For control variables, male and married respondents reported significantly lower CES-D scores, while individuals living in western or central areas (coastal areas as reference) reported significantly higher depressive scores.
Spline Poisson regression analysis of depressive symptoms: the effect of educational attainment. a

Those who are at very low risk for depression (probability of exposure to depression is less than 0.10) are excluded from the analysis.
p < .05; **p < .01;***p < .001 (two-tailed tests)
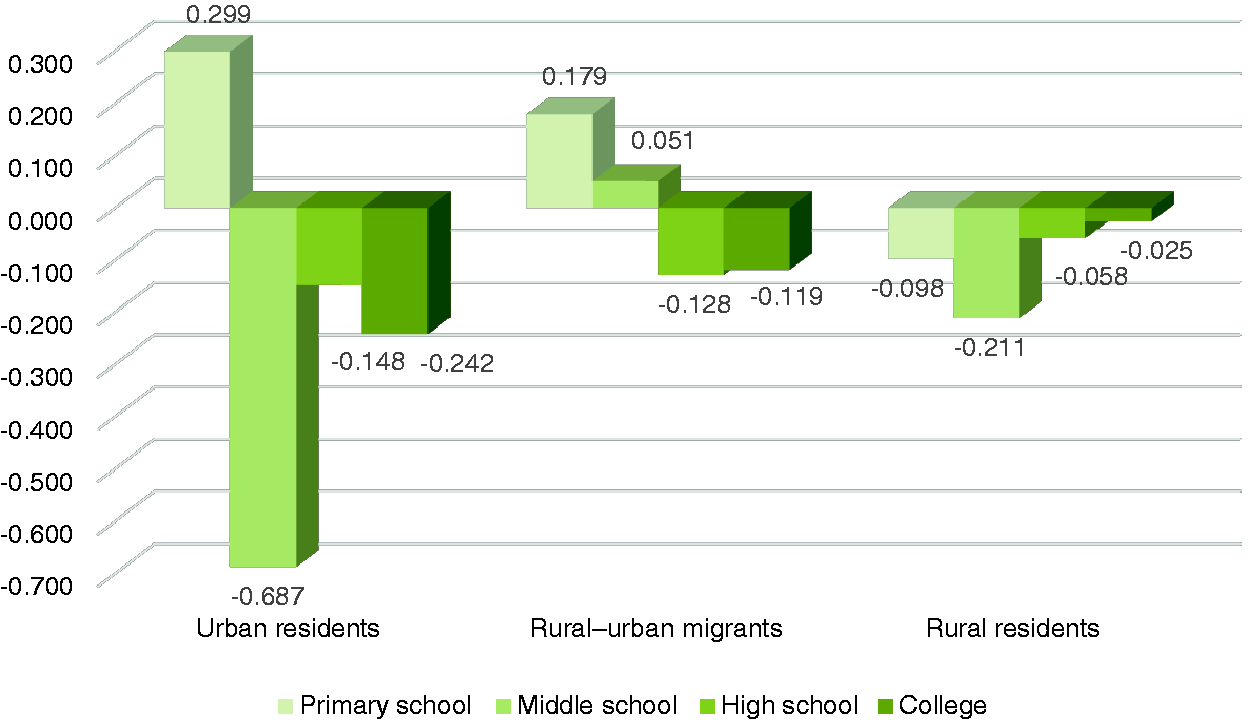
Partial effects of educational attainment on CES-D scores by demographic groups.
Conclusion
Although there has been a longstanding curiosity about the socio-political consequences of China’s remarkable urban–rural divide, we have yet to understand the divide’s possible influence on mental health. Using data from the 2016 wave of the CLDS, we find that depressive symptoms reported by individuals with agricultural hukou status (rural–urban migrants and rural residents) are significantly higher than those reported by urban residents. Results from ZINB regression suggest that this rural–urban difference in depressive symptoms can be attributable to socioeconomic status and proximate stressors such as unemployment, living alone, and unaffordability of medical services. In particular, the rural–urban difference in depressive symptoms is explained away by educational attainment: after controlling for educational attainment there is an urban–rural crossover in depression such that depressive scores reported by rural residents become lower than those reported by urban residents. As suggested by results from spline Poisson regression, the protective effects of the period of middle school, which vary substantially across demographic groups, are especially relevant to the rural–urban disparity in depression. We argue that hukou is a fundamental cause of disease in China and its effects on depression are mediated by various social, economic, and medical factors. Mental health is an important yet under-studied area in which China’s salient urban–rural inequality strikes.
The existing literature suggests that people in China may deny experiencing depression or express it somatically given the low prevalence rates of depression reported in China (Parker et al., 2001). Findings from this study show that a proportion of the Chinese population is actually at little risk of depression, which may contribute to the low prevalence rates of depression in China. Furthermore, socioeconomic, cultural, or cognitive factors shaping the exposure to depression in China deserve attention in future studies. The important role of education in explaining the rural–urban disparity in depression is in line with conclusions from previous studies: educational inequality is a primary mechanism through which the hukou system perpetuates and magnifies social inequality in China. For example, the period of middle school has a salient protective effect against depression among urban residents, whereas such a protective effect appears to be much smaller among rural residents and even disappears among rural–urban migrants. The life-course trajectories of these demographic groups segmented by hukou may shed light on this interesting finding. For urban residents, the middle-school years tend to be a comparatively positive and optimistic period for urban residents as they prepare for high school. In contrast, middle school is a critical period for rural adolescents to see their family hardships and limited career opportunities in relation to China's broader social context. After middle school, a large proportion of them have to leave their families, work in labor-intensive industries and endure difficulties in cities.
The key issue raised by this study is probably not what variable predicts depression across demographic groups. Rather, our findings show that mental health problems experienced by the disadvantaged with rural origins are deeply embedded in the political structuring of their everyday lives. With the persistence of power in reform-era China, scholars cannot fully understand the origin of mental illness among the Chinese unless the role of politics has been carefully addressed (Fu, 2018). Despite the prevailing public outcry against the hukou system and piecemeal hukou reforms implemented at both the national and local levels, this study demonstrates that the system still functions in China as an institutional arrangement creating inequality and injustice. This socialist policy exists, moreover, against the backdrop of institutional arrangements that have been established in other modern societies to correct for inequality and injustice. Despite the country’s rapid economic growth since the 1980s, individuals with rural origins remain at the bottom of China’s social hierarchy. With the poor quality of their education, inadequate investment in infrastructure, unavailability of state resources, and limited life chances, rural residents cannot flourish in an environment where they are institutionally discriminated against. From the social-stratification perspective, our findings do not deviate materially from Hu Feng’s vivid portrayals of Chinese peasants in the 1930s. In his epilogue to Xiao Hong’s novel The Field of Life and Death, Hu Feng wrote: [Peasants in China] live like mosquitoes, pointlessly reproduce themselves, chaotically pass away. [They] use their own blood, sweat and lives to fertilize the land, cultivate crops, raise cattle. [They] creep beneath the power of the tyranny of nature and tyrannies with two legs (Hu, 1991 [1935]: 145).
Footnotes
Acknowledgment
The authors are grateful for comments from Professor Eric Fong, Luying Wang, Erin Williams and two anonymous reviewers.
Funding
The authors gratefully acknowledge financial support from The Chiang Ching-kuo Foundation for International Scholarly Exchange, Hampton Scholar Award at The University of British Columbia and the National Natural Science Foundation in China (grant number 71540031).