
Abstract
Limb difference affects millions worldwide, with prevalence expected to rise due to increasing rates of diabetes and vascular disease. Despite the need for high-quality, functional prostheses, many individuals, particularly in low- and middle-income countries, lack access to affordable, customized prostheses. 3D printing offers a promising approach to address these gaps by enabling lower-cost, highly personalized prosthetic fabrication. This narrative review examines the current state of 3D printing in prosthetics, with a focus on upper limb prostheses, socket design, and terminal attachments. Although 3D printing has been used to produce functional prostheses, particularly in non-regulated settings, clinical adoption remains limited due to concerns regarding safety, durability, and a lack of high-quality evidence. This review highlights the advantages of 3D printing, including cost-effectiveness, customization, and accessibility, while also addressing key limitations such as material performance, regulatory challenges, and insufficient clinical validation. Future research priorities include rigorous clinical trials and performance testing to establish non-inferiority compared with conventional prostheses and to support broader clinical integration.
Introduction
Limb difference, whether acquired or congenital, can be debilitating. The prevalence of limb difference in the United States was estimated to be 2.3 million people in 2019, increased from 1.6 million people in 2005, and may rise to five million by 2060.1–3 Acquired upper extremity amputations, which are thought to have a prevalence of roughly 11.6 per 100,000 adults, 4 are much less common than acquired lower extremity amputations. In low- and middle-income countries, where trauma is the leading cause of amputation, the prevalence of limb loss was estimated to be 57.7 million as of 2017.5,6 Additionally, roughly four in 10,000 babies each year are born with at least partial limb difference, ranging from a missing digit to full agenesis of one or more limbs.7,8 Unfortunately, many individuals with limb difference worldwide do not have reliable access to high-quality, functional, and comfortable prostheses, often due to limited funding or because there are not enough prosthetists to service the number of patients in a given area.5,6,9,10 Given this need for greater prosthesis access, clinicians, prosthetists, and medical device companies have put considerable time and effort into finding ways to streamline the manufacturing and distribution of prostheses.
In the 21st century, additive manufacturing (AM) processes, more commonly known as 3D printing, have exploded in popularity and accessibility. 11 3D printing has become particularly widespread as an increasing number of manufacturers have developed small, low-cost printers for the consumer market.11,12 Cases abound of individuals with access to 3D printing technologies creating customized solutions for people with limb difference.13,14 3D-printed prostheses designed or printed by laypeople, often prosthesis users themselves, are most commonly designed for upper limb differences. However, 3D printing has also been used in lower extremity and in clinically fabricated prostheses, particularly in the areas of socket fitting 15 and proprietary component designs.13,16,17
However, there are clinicians who remain skeptical about the utility of 3D printing in creating robust prostheses. While media reports highlight the advantages of 3D printing, there is an unfortunate dearth of rigorous clinical trials and high-quality evidence in support of 3D-printed extremity prostheses, sockets, and prosthetic components.18,19 Hesitancy to implement 3D printing in prosthesis manufacturing may also be due to misconceptions about the capabilities of AM and a lack of training about how 3D printing can be incorporated into a prosthetist’s workflow. 13 By examining the existing literature regarding 3D printing in prosthetic fabrication, general trends including advantages, challenges, and future opportunities for AM in prosthetic development can be identified.
In this review, we therefore seek to address the following questions: What is the current state of 3D printing in prosthetic manufacturing? What are the advantages and limitations of using this technology to fabricate prostheses? What areas require further research and development to make 3D printing a truly viable tool for the prosthetist?
Overview of the standard prosthetic fabrication process
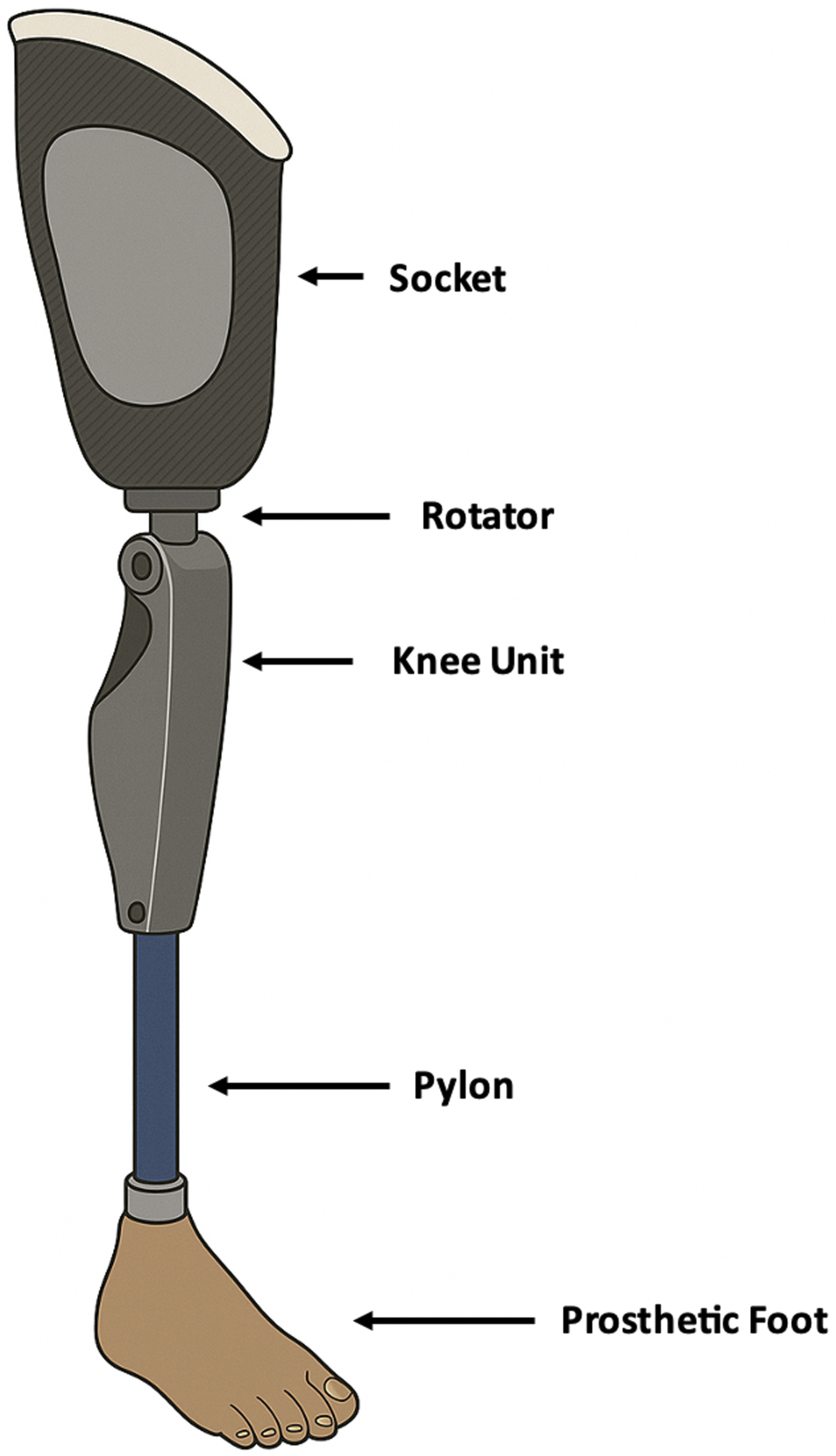
The standard approach to managing limb difference, originally conceived in the 1500s, is to replace the function of the missing limb with a prosthesis (see Figure 1 and Figure 2 for representative upper limb and lower limb prostheses).
20
Transradial upper limb prosthesis. Transfemoral lower limb prosthesis.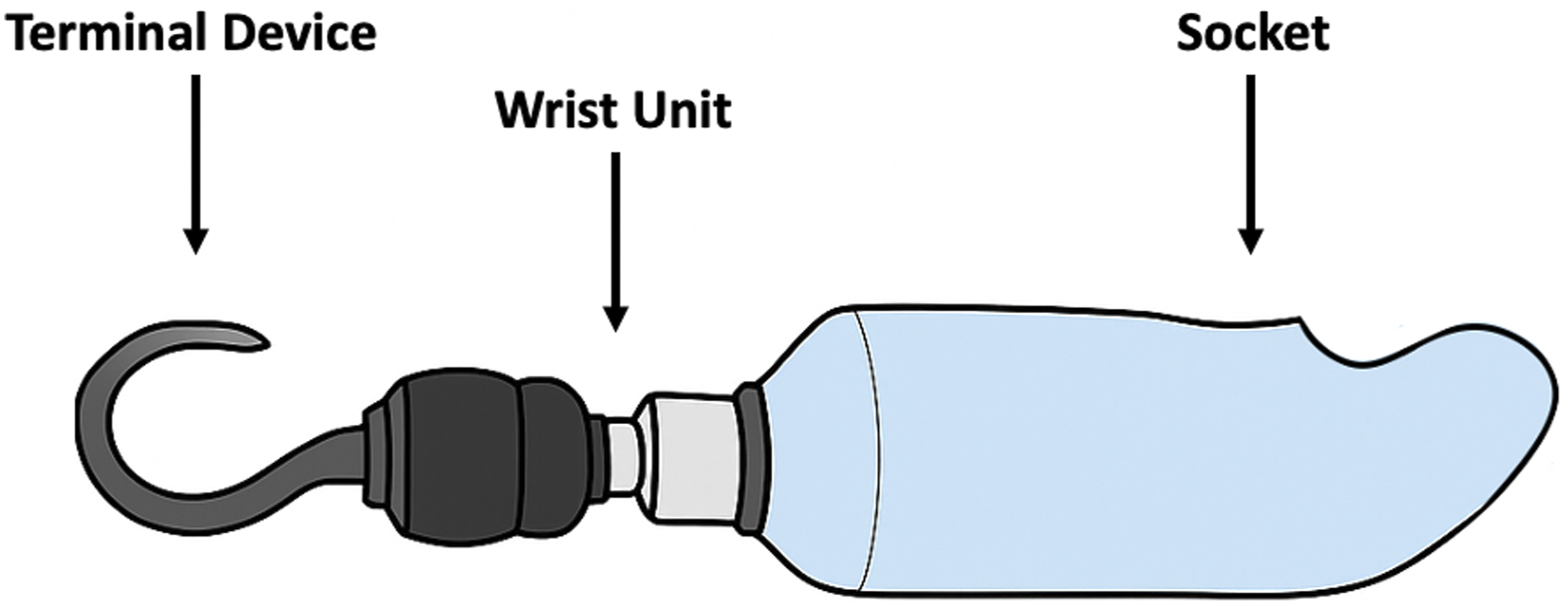
Traditionally, obtaining a prosthesis involved engaging a local prosthetist who would produce a custom socket based on the shape of the user’s residual limb.
21
The iterative fabrication and assembly process (Figure 3(a)) (see Chapter 6 of Orthotics and Prosthetics in Rehabilitation
22
for a comprehensive overview) is time-intensive: the residual limb shape is first captured via casting to make a mold which is filled with plaster to create a positive cast to approximate the residual limb.13,21–23 The positive cast is further modified through a combination of automated and hands-on refinements to achieve a final cast from which the user’s new prosthetic socket is fabricated.22,23 The process of iteratively refining the physical cast to achieve a comfortable and secure fit for the user can take weeks to months and requires skilled manual labor by highly-trained technicians. While this stepwise process allows for serial refinements, it also typically results in data loss, as each subsequent component used in casting is either modified or destroyed through the fitting process.19,24 The iterative processes of limb measurement, socket prototyping, and socket manufacturing and use for both (a) traditional prosthesis fabrication and (b) digital scanning workflows, including those that utilize 3D printing. As shown, the digital workflow can streamline the socket prototyping process, eliminating intermediary steps and material waste.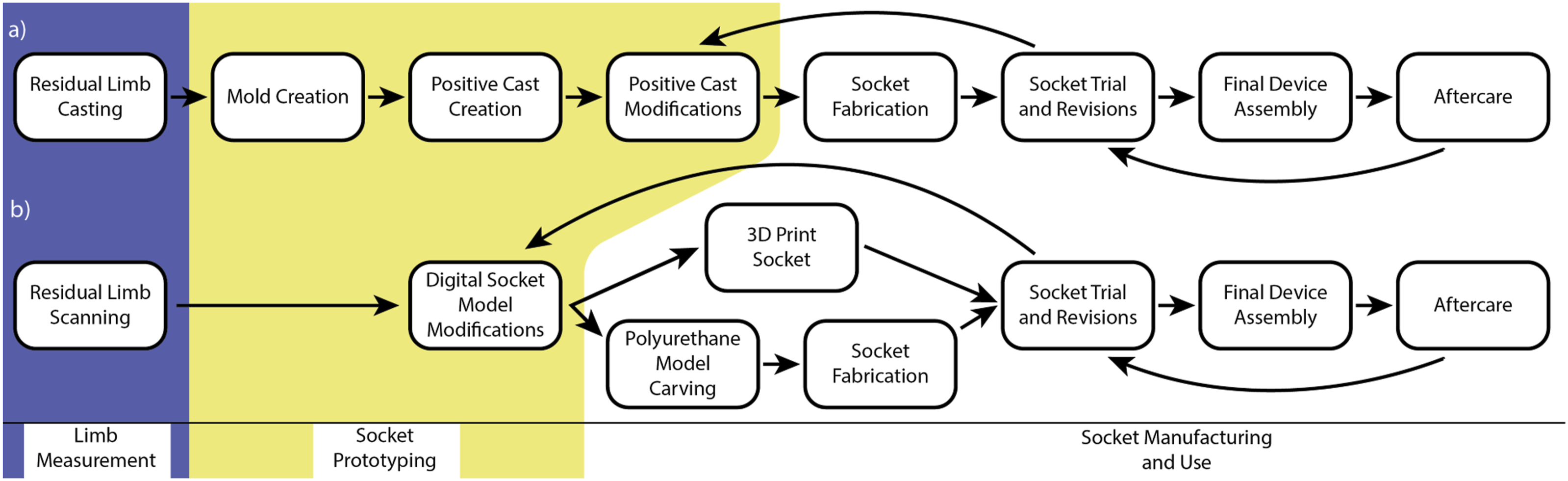
In response to some of the challenges with this highly manual process, since the 1980s, digitization of certain steps of the workflow has become increasingly viable. 25 For instance, the residual limb shape capture may be performed with digital scanning, and the positive cast may be produced and modified with Computer Numerical Control (CNC) carving21,25 (see Sockets section below for further discussion, and Figure 3(b) for a schematic of a digitized workflow). CNC carving eliminates some of the hands-on time required for positive cast production in the traditional process, but still introduces an additional step and materials. 25
Once a prosthesis user has a customized socket that fits well, it is assembled with industrially manufactured prosthetic components according to the user’s needs and preferences. 22 For instance, lower limb prostheses will require components to simulate the foot, ankle, lower leg, knee, thigh, and/or hip depending on the level of amputation; upper extremity prostheses may similarly require components to replicate the function or form of the hand and fingers, wrist, forearm, elbow, and/or shoulder.8,26,27 Decisions about the components included in a prosthesis are based on the user’s anticipated needs and are also constrained by cost, overall device weight, and the availability of insurance coverage. 8 As a result, prostheses are customized not only by socket fit, but also by the components that are assembled to create the final device.
The determination of the desired functions of the prosthesis guides its design and fabrication. A discussion of the myriad considerations for prosthetic componentry is beyond the scope of this review (for a good overview, see Braddom’s Physical Medicine and Rehabilitation Seventh Edition Chapters 10 and 11 for upper and lower extremity prostheses),8,26 however, broadly, prostheses can vary widely in complexity, and may contain any combination of passive or simple mechanical components as well as electronics, microprocessors, or hydraulic mechanisms. 28 The cost of prostheses correspondingly can vary significantly depending on the sophistication of the components; generally speaking, an assembled prosthetic device will cost the payer tens of thousands of dollars.6,7,29,30
Challenges with the standard prosthesis fabrication process
Given the time, labor, and cost required to produce a prosthesis, even the most basic devices may be inaccessible for many individuals with limb difference, especially those who live in areas with few prosthetists to service many potential users.7,30–33 Furthermore, many individuals with limb difference abandon their prosthesis due to uncomfortable fit, cumbersome components, or poor durability; lower rates of prosthesis use are more common in users with upper extremity limb difference and those with more proximal amputations of either the upper or lower limb.28,33–38 Additionally, because the socket fabrication process is so labor-intensive and user-specific, it is difficult to replicate designs when they need to be replaced or modified. Residual limb molds are rarely saved, so when a prosthesis user needs a new socket (typically because an improved fit is required or because of regular wear-and-tear), if the current socket cannot be acceptably modified, the entire fitting and fabrication process must be repeated.19,24
Overview of 3D printing materials and methods
To understand how 3D printing could be used in prosthesis manufacturing, it is important to first understand AM (for a comprehensive overview of AM, refer to the International Organization for Standardization [ISO] and American Society for Testing and Materials [ASTM] document ISO/ASTM 52900:2021 Annex B). 39 There are multiple types of 3D printing including fused deposition modeling (FDM), selective laser sintering (SLS), and stereolithography (SLA), along with other variations like selective laser melting (SLM) and direct metal printing (DMP) that allow for the printing of metals.40–42 FDM printing relies on a heated nozzle to melt thermoplastics which are then extruded into the intended designs, while SLA uses ultraviolet (UV) light to precisely harden shapes out of a liquid resin solution, and SLS uses a laser to sinter powder to create the geometries of the final model.41,43 FDM is the most familiar technology used in hobbyist 3D printing and is widely used even in research and industrial settings. SLA, SLS, and metal 3D printing are more commonly seen in industrial applications and offer printing of materials and geometries that are not possible with consumer-grade FDM printers.
Despite the technical differences, all 3D printing techniques require a computer-aided design (CAD) file (i.e., digital model), which is then converted into a layer-by-layer plan that can be implemented by the 3D printer. For instance, FDM printing works by depositing melted strands of plastic first onto the print bed as a base layer before depositing subsequent layers to construct the design; once deposited, the plastic cools and fuses to the layer below while additional layers are added on top.43,44 In FDM printing, it is necessary for the designer to specify the way in which a part is filled, both the pattern of the inner material (e.g., honeycomb, grid, concentric, etc.) and percentage of solid material used (where 90% infill would represent nearly solid, and 20% is less dense). Increasing the infill exponentially increases the time and material needed to produce the part. Both the infill percentage and pattern affect the strength and weight of the final printed part.44,45
Just as there are multiple types of 3D printing technologies, there are many materials that can be 3D printed. Common and readily available materials for hobbyist FDM 3D printers are polylactic acid (PLA) and polyethylene terephthalate glycol (PETG); historically, acrylonitrile butadiene styrene (ABS) filament was also commonly used, though in many instances has been superseded by PETG as ABS can be more technically challenging to print. PLA is still often used with hobbyist printers, especially in low-resource settings, because of its affordability, availability, and relative ease-of-use as it does not require a heated print bed. 41 For high quality prints, PETG needs to be dried before printing and requires a heated bed for optimal adhesion, but offers improved strength, durability, and heat and ultraviolet tolerance at only slighter higher cost than PLA, and thus has become a compelling option for both hobbyist and professional printers. 41
Materials with a wider variety of mechanical properties, such as thermoplastic elastomers (TPE) and thermoplastic polyurethane (TPU), polyamide (PA, also known as nylon), polycarbonate (PC), and reinforced plastics are also becoming more readily available to consumers.15,21,22,43,44 Flexible materials like TPEs are useful for parts that need to be able to bend or temporarily deform, PA and PC possess chemical and thermal resistance and dimensional stability, and reinforced materials (e.g., with carbon fiber, glass, or even wood) increase the strength and durability of plastic filaments.22,41 Industrial FDM printers often add the ability to print high-performance polymers like polyether ether ketone (PEEK). 46 In SLS printing, powders are often nylon-based, though additives such as glass, carbon fiber, or graphene are frequently added, whereas SLA processes utilize photosensitive thermoset polymers. 46 As with any manufacturing technology, the designer must weigh the cost of the material against the desired material properties for the application.
Current use cases for 3D printing in prosthetic manufacturing
Upper extremity prostheses
Upper limb prosthesis manufacturing is arguably the sub-discipline of prosthetics that has been most impacted by 3D printing.35,45,47 Compared to lower limb prostheses, these devices are smaller in size, and structural strength is less critical since they are not expected to be continuously load bearing. As such, upper limb prostheses are conducive to experimentation, and numerous community and industry organizations have developed 3D-printed designs. Additionally, the various levels of sophistication of upper extremity prostheses make them amenable to AM techniques. For example, passive or body-powered prostheses can be almost entirely 3D printed, 48 while more advanced myoelectric prostheses can still benefit from the 3D printing of certain components such as fingers and electronics housings.29,49,50
Body-powered prostheses are the most common type of upper extremity prostheses in clinical use today due to their simplicity and relative affordability. To actuate a body-powered prosthesis, the user moves their shoulder, back, or another part of the body to pull cables or pulleys which then move the mechanical joints of the prosthesis.8,47 Body-powered prostheses are preferred by many clinicians and individuals with limb difference because they are simple, robust, and highly functional. 20 They also have an added benefit in that tension on the cable or harness provides some sensory feedback to the user. 8 Their ease-of-use and lack of electric components are conducive to 3D printing, as AM techniques can produce lightweight components which can be easily assembled ad hoc to tailor the device to the end user. 51 Some of the most well-circulated 3D-printed prosthetic designs45,49 fall into this category and include the Robohand, 52 Cyborg Beast, 53 and e-NABLE devices. 54 Online repositories have allowed these designs to be shared and refined by hobbyists and prosthesis users. 55
In contrast to body-powered prostheses, myoelectric prostheses are controlled by the electrical activity of the muscles in the residual limb of the user. These electrical signals are converted into a command to actuate electric motors in the joints of the prosthesis. Myoelectric prostheses typically have more sophisticated components, allowing for greater dexterity and more degrees of freedom of movement than body-powered devices, however, often at the expense of durability and intuitiveness. 47 These prostheses have undergone substantial engineering development over the last few decades, with modern devices capable of electrically powered actuation of the shoulder, elbow, wrist, and individual fingers. 18 Despite their relative complexity, 3D printing can still be used in the creation of these devices, both in research and development as well as production. One common example of a 3D-printed myoelectric device is the Open Bionics Hero Arm. 50 3D printing plays a role in the fabrication of proprietary myoelectric components, some of which require complex geometries that can only be achieved via AM, and offers a cost-effective alternative to injection molding for small-batch manufacturing.29,35,47,56
Nonprofit distribution
3D-printed prostheses are typically distributed through non-profit organizations such as e-NABLE, 54 Limbitless Solutions, 57 LifeNabled, 58 Team UnLimbited, 59 and Form 5 Prosthetics 60 ; many of these organizations focus on upper limb devices while others produce customized sockets or lower limb prostheses. Non-profit organizations can fundraise for the cost of materials and give the prostheses to people in need at little or no cost to the user. Many of these organizations publish their designs online, leading to iterative, crowd-sourced improvements and making the devices available to anyone with access to a 3D printer.61,62 These prostheses are not as robust as commercially manufactured devices and should not be thought of as a direct replacement for professionally fitted prostheses, but they do offer a functional stopgap for people who cannot access commercial devices. 30
Because of their relative affordability and lower initial capital investment in machinery and training, 3D-printed prostheses have been proposed as a solution to the inaccessibility of prostheses in developing countries.13,30 Compared to the alternative limited access to prosthetic care in under-resourced areas, 3D printing can provide a means for access to prostheses until an effective health care infrastructure is in place and more funding is available for professional training and reimbursement.9,30,63 As trauma remains the leading cause of acquired limb difference in developing countries, a 3D-printed prosthesis may allow a user to return to their occupation more quickly than if they had to wait to receive a commercially available device. 6
Pediatrics
Fitting pediatric users with traditional prostheses can be challenging for several reasons. Children grow quickly and so their prostheses require frequent size adjustments which incurs ongoing costs for the child and their family. 53 Children may also be more active and more likely to cause unintentional damage to the components of their prostheses. 64 When considering upper extremity prostheses specifically, it can be challenging to help a child incorporate a prosthesis into their daily activities, as children often naturally adapt to using their residual limb without a prosthesis.65,66
Despite these challenges, the use of an upper extremity prosthesis for children with upper limb difference can improve their functional outcomes,65–67 help them achieve critical developmental milestones, 66 and reduce the incidence of overuse injuries proximal to their limb deficiency or in their contralateral intact limb. 68 3D-printed prostheses can help meet the prosthetic needs of children by providing a more cost-effective solution for these young users who quickly outgrow their devices. 64 3D printing may reduce the weight of the prosthesis (though at the cost of strength and durability); the unwieldy nature of traditional prostheses can be a barrier to adoption for young children whose bodies cannot support the unbalanced weight of heavier devices.49,69 If part of the prosthesis does break, modular prostheses enable damaged or outgrown components to be swapped out, reducing the cost of repairs and decreasing the need for a full replacement device. 63 Finally, 3D-printed prostheses allow for a broad range of cosmetic appearances (e.g., color combinations) that can help a child more readily identify with and accept their prosthesis.35,49,63
Customized components and terminal attachments
There are many types of attachments, or terminal devices, that can be added to the end of a prosthesis to confer a desired function. These terminal devices may or may not resemble anthropomorphic structures; for instance, an upper extremity prosthesis can end in a hand or in a hook, while a lower extremity prosthesis can end in a solid foot or a blade for running.8,26,27 Terminal devices can be highly specialized to provide narrow functionality for particular applications like occupations or hobbies, and 3D printing has been used in the manufacturing of many of these attachments as the technology is capable of creating structures that would be difficult or impossible to build using traditional manufacturing techniques.16,70 Durability is an oft-cited limitation of 3D-printed prostheses, but is less of a concern for an activity-specific terminal device, which is often not used daily and thus does not undergo frequent repetitive loading. The relative affordability of 3D-printed components may make 3D-printed terminal devices more obtainable and more easily replaced if broken.
3D printing also confers benefits in the creation of water-friendly devices. Many traditional passive prosthetic components are themselves water-resistant; however, for prostheses containing electronics without adequate waterproofing (i.e., without IPX7 or equivalent rating), most insurers will not pay for a second device specifically for use in water. 3D printing offers a cost-effective solution to allow individuals with limb difference to have an alternative prosthesis specifically for use in wet environments which can encourage exercise and wellness through participation in water sports, aqua therapy, and all-weather leisure activities. 71 Commercial solutions such as the Limber Unileg demonstrate the viability of purpose-designed waterproof prostheses. 72
Sockets
The socket is arguably the most crucial component of a prosthesis because it is the junction between the user’s residual limb and the rest of the prosthesis, and discomfort at the socket is the most cited reason for prosthesis abandonment.28,36,61,73 An ill-fitting socket is not only uncomfortable but can also be dangerous, as a poorly fit socket can put increased pressure on the residual limb leading to skin breakdown.61,73,74 3D printing, oftentimes in conjunction with 3D scanning, can expedite and enhance socket fitting and manufacturing.
Rather than being formed from physical molds, 3D-printed sockets rely on digital models which are generated from residual limb images. While research studies have shown the promise of obtaining these models from pre-existing imaging data such as x-rays, magnetic resonance imaging (MRI), or computed tomography (CT), 75 digital models are most often generated specifically for socket fabrication via handheld or in-office 3D scanners which rely on touch probes, lasers, or photography.13,19,23,24,63
Manual residual limb casting (as shown in Figure 3(a)) has traditionally been the gold standard for accurate capture of the residual limb. Manual casting allows the prosthetist to not only replicate the limb shape but also detect bony prominences and pressure points as well as manipulate the limb into a functional position (e.g., to improve rotational stability in the socket) 22 ; this direct “feel” of the limb and the corresponding socket can be difficult to replicate with fully digital workflows. However, improvements in 3D scanning technologies along with the use of finite element analysis may allow prosthetists to use 3D models to predict areas of high stress and strain and directly modify the digital socket model prior to fabrication.22,23,56 A completely digital workflow (Figure 3(b)) streamlines the fabrication process and the resulting digital models can be stored for reference, though a new scan will typically be needed when replacement sockets are required due to residual limb volume changes.13,21,23,27,76 Again, it is also worth noting that digital workflows do not preclude non-AM fabrication; as mentioned above and shown in Figure 3(b), CNC carving of positive molds from scan data is an established clinical approach. 21
Regardless of the fabrication pathway, check sockets, temporary sockets that are used to test static and dynamic fit, are a standard component of both traditional and digital prosthetic fitting workflows. 77 The use of 3D printing to create check sockets has been described.77,78 However, traditional check sockets are typically made of thermoplastics, which can be heated and deformed to modify fit, offering a degree of adaptability that typically requires reprinting in AM-based approaches.
In the future, the unique capabilities of AM could lead to improvements in socket fit, as 3D printers that are capable of printing different materials may be used to produce multi-material sockets which can better redistribute pressure in the residual limb. With traditionally manufactured sockets, prosthetists will often manually carve out relief areas or add extra padding if a user endorses discomfort in a particular area of the socket. Sengeh and Herr describe an alternative solution in which MRI data of a residual limb is used to map out bony protuberances and, using a multimaterial printer, a socket is fabricated with materials of varying compliance to offload pressure in critical areas.75,79 With the rise of imaging and scanning technologies to gather robust data about a user’s residual limb, and with advances in 3D printing to accommodate filaments with diverse material properties, it is conceivable that sockets could be produced which are customized not only in appearance and shape, but also in material composition. 63
Reduced materials and production costs
The delivered cost of traditional prostheses, whether covered by insurance, grant funding, or the users themselves, can be quite prohibitive, ranging from anywhere between a few thousand dollars to upwards of $50,000 depending on the complexity of the components.6,7,30 Accordingly, the comparatively low cost to the end user is often cited as a primary advantage of 3D-printed prostheses. These overall cost savings may be the result of both less expensive materials and fabrication equipment as well as reduced labor costs.
Consumer 3D printers are now available for a few thousand dollars or less, whereas industrial-grade FDM printers can cost tens of thousands of dollars; SLS systems represent a substantially higher capital investment, often exceeding $100,000 for industrial units, along with greater operational and maintenance costs.12,30,80 The raw materials needed to print a prosthesis can be acquired for a relatively low price; many 3D-printed prosthetic designs are printed in PLA in hobbyist contexts, and more advanced materials like PETG or reinforced filaments remain cost-effective when compared to commercially manufactured prosthetic materials.30,31,61
Despite advancements in 3D printing technologies for prosthesis manufacturing, reliable cost data remains quite limited, in part due to the myriad types of prostheses being produced as well as variations in design, complexity, and AM materials used, not to mention widely-variable healthcare delivery contexts.9,31,80 As a result, it is difficult to draw general cost comparisons between 3D-printed prostheses and those manufactured via more traditional fabrication pathways; to attempt to do so may also imply that all 3D-printed prostheses are functionally or clinically equivalent to professionally-fabricated prostheses, which is clearly not always the case. Thus, cost analyses across a variety of implementation settings and healthcare contexts 81 are needed to further bolster the body of evidence supporting the expansion of AM in prosthetic manufacturing.
Limitations of 3D-printed prostheses
Despite the advantages that 3D printing provides, there are challenges which have limited the widespread adoption of AM to produce prostheses. Many of these limitations, including device strength, fatigue resistance, surface smoothness, and compatibility with standardized prosthesis parts can be traced back to the fundamental mechanisms of how 3D printing works, and may be mitigated as the technology continues to improve.
Device strength and durability
Although a widely acknowledged limitation of 3D-printed prostheses, there is little research characterizing their durability.45,67 The expected lifespan of a prosthesis is important to quantify to accurately compare the reliability and affordability of 3D-printed devices to traditionally manufactured prostheses, but few studies have examined the life cycle of 3D-printed prostheses. Multiple factors, including materials, printing methods, and overall device assembly play a role in determining the strength and durability of 3D-printed prostheses, and more research is needed to characterize the material properties impacting 3D-printed prostheses which can then inform better designs for increased longevity. 82
In hobbyist and open-source contexts, FDM printing with easily accessible materials such as PLA, PETG, or ABS is common,21,43,44 but these polymers are relatively brittle when compared with more industrial-grade materials, especially if exposed to moisture prior to printing, and may exhibit abrupt failure under loading.83–85 In FDM specifically, the layer-by-layer construction means that parts exhibit anisotropy (direction-dependent material characteristics).35,83,84 PLA and ABS are also susceptible to degradation when exposed to UV light, temperature extremes, or humidity.86–88 This ultimately means that hobbyist-made 3D-printed prostheses produced with FDM printers might withstand daily stresses and strains but can fail irreparably if loaded beyond their upper limit. Furthermore, prostheses fabricated with cheaper materials such as PLA and ABS may not be suitable for repetitive, sustained weight bearing, such as might be required in a lower extremity prosthesis.15,22
Some of these limitations can be mitigated with alternative materials or printing methods. Importantly, anisotropy is primarily a concern for FDM; SLS and SLA generally produce more isotropic parts that are less susceptible to delamination-type failure. 89 Many other more durable filaments, including nylon and carbon-fiber-reinforced composites, are widely available for many types of 3D printers and offer significantly better mechanical performance for structural applications with less degradation due to environmental factors. There are also techniques, such as annealing90,91 or combining 3D-printed pieces with other materials or finishes, that can increase the strength and durability of 3D-printed prostheses.86,92 Of course, these methods add to the overall production time and cost. 61
It is also worth noting that the 3D printing process itself is impacted by many factors including raw material quality, ambient temperature and humidity, printer calibration, and stability/vibration dampening of the printing surface. This means that a prosthesis of the same design, printed with the same type of materials and parameters, and even manufactured with the same printer, can have considerable variability from print to print. 44 Commercial-grade 3D printers are less impacted by these variations than hobbyist-grade models, but it is still worth noting that 3D-printed prostheses can vary significantly in quality. This creates a challenge for scaling production, since quality control is more difficult to achieve, and can hinder testing and regulation since a single design may have varying properties depending on when, where, and how it is printed. 39
Durability and failure modes
The ad-hoc nature of hobbyist 3D-printed prostheses means they are often assembled with readily available components that are not necessarily designed to withstand the demands of everyday use. For example, many hobbyist-printed upper extremity prosthesis designs require “tendons” which connect to each finger to open or close the prosthetic hand, and these “tendons” are often made of off-the-shelf materials like fishing line. Unsurprisingly, these elements are often the first to fail, thus reducing the lifespan of 3D-printed hands. 32 One study 32 examining two open-source 3D-printed hands found that the hands could withstand forces up to 30 Newtons (N) before failing – significantly below the 68 N grip force that is generally regarded as the minimum upper extremity force needed to execute basic tasks of daily living. 45 Load at failure was even lower for pediatric-sized 3D-printed upper extremity prostheses in another study. 30 For practical use of a prosthetic limb, studies have suggested a minimum grip force of 45 N, but open-source 3D-printed upper extremity prostheses have not consistently met this benchmark in previous testing. 69
For lower extremity prostheses, two studies applied ISO standard 10328 93 which specifies testing to determine whether sockets can withstand a minimum static load, and found that 1) PLA 3D-printed sockets could withstand the minimum required 4480 N threshold set by the standard, and 2) 3D-printed sockets had comparable ultimate strength to thermoplastic sockets, but the ultimate strength of 3D-printed sockets was inferior to that of industry-standard carbon fiber sockets.82,94 In one of these studies, the 3D-printed transtibial sockets tended to fail most frequently at the interface between the PLA socket and the pylon, the component that connects the socket to the prosthetic foot. 82 The mismatch in elastic modulus between the rigid metal pylon and the more-deformable socket can induce failure in the transition area between these two materials. 22 Owen and DesJardins hypothesized that this knowledge could be used to preemptively reinforce these high-failure areas with extra thickness or wall material, an example of how a better understanding about the characteristics of the materials used and the interplay between them can be leveraged when designing and building prostheses using AM techniques. 82
Widespread adoption and regulatory issues
The regulation of 3D-printed prostheses presents a major barrier to their wider use. Many of these prostheses – especially upper limb devices – are based on open-source designs, but it is unclear how these should be governed under current U.S. laws. The U.S. Food and Drug Administration (FDA) considers AM a standard production technique and regulates the resulting devices accordingly. However, when devices are customized based on patient-specific anatomical data and fabricated within clinical settings, they may qualify as point-of-care devices, and the FDA’s current guidance on 3D-printed medical devices lacks explicit provisions for point-of-care manufacturing.95,96 As a result, 3D-printed prostheses produced in-house by hospitals or by volunteer makers or end users outside of a clinical setting fall into a regulatory gray zone. These devices are neither fully exempt from oversight nor clearly addressed within existing frameworks.
While some stakeholders view the FDA’s limited intervention as a catalyst for innovation and user-driven design, this regulatory ambiguity poses significant challenges. Health systems and medical device companies may be reluctant to distribute 3D-printed prostheses without formal FDA clearance, due to concerns about liability and patient safety. 61 Consequently, most fully 3D-printed prosthetic devices remain confined to research environments, limiting their clinical availability and broader adoption.
Fortunately, many FDA-approved prosthetic designs do have 3D-printed components, 29 and this may be an avenue to promote further adoption of AM techniques in prosthetic manufacturing. In addition to regulatory approval, widespread adoption of 3D printing in prosthetic fabrication will require buy-in from prosthetists, clinicians, and technicians. While hospitals are increasingly investing in 3D printing equipment, and there are companies working to distribute 3D printers to prosthetist offices for socket fabrication, it will take targeted effort to train prosthetists and technicians on the ways in which AM can benefit their practices.
Future directions
Optimization of the 3D printing process
Many of the limitations of 3D-printed prostheses can be mitigated with improvements in 3D printing processes. One of the largest barriers to widespread adoption of 3D-printed devices is long printing times associated with AM. In addition to recent improvements in 3D printing technology which have greatly increased the speeds of even hobbyist-grade printers, additional techniques can be employed to streamline the manufacturing of 3D-printed devices. For example, King et al. proposed pre-stocking certain components in a range of sizes then combining these elements with customized parts to create user-specific assembled devices. 31 In their proposal regarding an upper extremity prosthesis, injection molded fingers could be attached to a 3D-printed palm, cutting down on production time and costs associated with elements that do not vary much from user to user while focusing customization on components with more variation. One could foresee a modular system where the manufacturing process is highly optimized from a time and cost standpoint to leverage the strengths of multiple manufacturing techniques while still providing user-specific customization of critical components such as the socket and terminal attachments.
Furthermore, as 3D printers become more refined, the types of materials that can be printed economically will increase. Relatively affordable consumer 3D printers can now handle printing multiple materials simultaneously and can print materials with diverse properties including flexible filaments, temperature-resistant plastics, and reinforced filaments.15,41,43 Industrial 3D printers can print an even wider range of materials. Notwithstanding these improvements, multiple reports of innovative manufacturing methods combining 3D-printed and non-3D-printed materials can be found which may offer viable production methods in the future. For example, Leddy et al. used anthropometric data to create 3D-printed finger molds which were then filled with a composite material which was both lighter and stiffer than either aluminum or 3D-printed prosthetic fingers. 97
Improved oversight
While open-source 3D-printed devices bring great promise to individuals with limb loss in less-resourced settings, the lack of design, durability, and manufacturing standards could result in an increased risk of device failure. There is also limited financial data to quantify cost savings for both users and health care systems over a lifetime of using these devices. 98 As mentioned above, the ASTM is at the forefront of standards development for AM processes and materials 39 ; concurrently, there are ISO standards (e.g., 10328, 22675)93,99 that describe how prostheses should be tested from a mechanical standpoint to ensure the rigor of the design and manufacturing process, but few 3D-printed prostheses have undergone this testing.82,86,100 Additionally, variability in the 3D printers and materials used when manufacturing these devices can greatly affect the quality and cost of the final product. Despite this lack of oversight, grassroots efforts to build prostheses for those who cannot receive professional care persist around the globe. To encourage equity in the quality and distribution of all prostheses, a set of manufacturing standards could be created for open-source prosthesis designs, perhaps using ASTM standards 39 as a starting point. Testing of designs can be done using existing ISO standards93,99 for prosthetic components based on a variety of different printing materials and techniques. The results of these tests can inform manufacturing standards (e.g., materials, printing parameters) unique to each design to be published. This will help establish best practices for manufacturers and realistic expectations of users in terms of the quality of these devices.
Rigorous research
Once the materials properties of 3D-printed prostheses have been quantified and tested via ISO standards, research focus should then shift to large-scale clinical trials. Recent scoping reviews21,101 found that clinical outcomes data on prostheses and AM is limited, with most of the existing literature involving proof-of-concept studies which do not closely mimic the intended wear environment; those studies also do not include long-term data. 63 To date, most of the wear tests examining 3D-printed prostheses have enrolled only a few participants (n ≤ 5) who wear the devices to perform specific experimental tasks. In these studies, the total wear time is often only a few hours or at most a few days. 21 To show non-inferiority of 3D-printed prostheses compared to comparable commercially available devices, studies will need to capture regular wear data over months to years. This data will further help quantify the lifespan of prostheses fabricated with AM techniques and will provide evidence-based data to help prescribers feel confident in fitting their patients with the right type of device that best fits their needs.61,63
Education and training
3D printing is a rapidly developing technology which has experienced dramatic growth and development. While there are valid uses of 3D printing in the field of prosthetics, prosthetist training programs may not cover the uses of 3D printing for prostheses in their curriculum. 63 Increased exposure to 3D printing within the field of prosthetics both for trainees and practicing professionals could effectively increase interest in the technology and maximize the benefits this technology has to offer. Thus, in addition to efforts to improve the testing and manufacturing standards of 3D-printed prostheses, efforts and funding should also go toward training more prosthetists and technicians on the myriad manufacturing techniques, including 3D printing, which would ultimately help address the shortage of prosthetic devices for users around the globe.21,61 In developed countries, increasing insurance coverage or reducing out-of-pocket costs for prostheses could help expand access to both 3D-printed and traditionally manufactured devices, while in developing countries, policies that cultivate the infrastructure necessary to receive professional prosthetic care could be effective in combating the excessive need for grassroots care. 33 Either way, 3D-printed devices are just one component of expanded access to prosthetic care, and to be maximally effective, health care policies that facilitate the distribution of safe and reliable prostheses are needed.
Conclusion
3D printing is a promising technology that offers a cost-effective, environmentally sustainable solution for highly customized, small-run manufacturing, and thus is well-positioned to be integrated into the prosthetic fabrication process. However, to date, 3D printing has been largely relegated to open-source upper extremity prostheses which fall outside of FDA oversight. With recent advancements in additive manufacturing technology, 3D printing is becoming increasingly affordable and reliable and has been shown to be a viable solution in the manufacturing of not only upper extremity prostheses but also prosthetic sockets and customized terminal attachments. With future research and testing to quantify the performance of 3D-printed prostheses, the incorporation of 3D printing in prosthetic fabrication could help alleviate current challenges with equitable distribution of affordable yet highly functional prostheses.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.