
Abstract
Introduction
No previous study has explored the effectiveness of current prescription standards for evaluating power mobility device (PMD) maneuverability. To verify the current prescription standards for PMDs using a virtual reality (VR)-based PMD simulator and to present the possibility of using a VR-based PMD simulator as an alternative to current evaluation standards.
Methods
A total of 52 patients with brain diseases were enrolled. All participants were over 18 years old and had gait disturbance or limited outdoor walking ability. Participants performed a driving ability test using a VR PMD simulator.
Results
The driving ability test using the VR PMD simulator indicated that cognitive impairment, measured by the K-MMSE (p = 0.017), and unilateral neglect, measured by line bisection (p = 0.031), led to reduced driving ability and safety. In addition, patients with cognitive impairment or neglect presented driving stability problems, which were observed in the driving trajectory. There was also no correlation between driving scores and MBI subitems.
Conclusion
In patients with brain lesions, a driving ability test using a VR PMD simulator can be a safe, objective method for comprehensively evaluating a driver’s capacity, offering an alternative to the current prescription standards for PMDs.
Introduction
Mobility impairment is a common sequela of brain diseases such as cerebral stroke, traumatic brain injury, and cerebral palsy.1–3 It can restrict an individual’s social participation and quality of life. Many individuals with mobility impairment use assistive devices such as walking sticks, anterior walkers, or manual wheelchairs. People with more significant physical disabilities who cannot independently operate manual assistive devices and those who wish to cover longer distances need power mobility devices (PMDs) such as power wheelchairs (PWCs) and scooters. 4 PMDs can improve the quality of life of people with disabilities by helping them participate in the community.4–7
In 2019, around 2,619,000 people were registered with the National Disability Registration System (NDRS) of the Republic of Korea. This is about 2.7 times more than in 2000 and accounts for about 5.1% of the country’s total population of 51,849,861. 8 The Korean Ministry of Health and Welfare expanded health insurance coverage for PMDs in February 2008. 9 Since then, the supply of PMDs has steadily increased every year; About 130,000 units were distributed from 2008 to 2016, and 14,566 units were distributed in 2016 alone. 9 Considering the expansion of disability categories and the increase in the number of registered persons in the National Disability Registration System due to various national policies to support the disabled, along with the higher aging rate of this population, the demand for PMDs is likely to continue to increase in the near future. As a result, there is a risk of increasing socioeconomic costs associated with providing PMDs to the disabled.
The current PMD prescription standards (Supplementary Table 1) include an assessment of independent walking ability or distance, the upper limb manual muscle test (MMT), the Korean-Mini Mental Status Examination (K-MMSE), and the modified Barthel Index (MBI). Although visual perception is also important for operating a PMD, 10 evaluations of visual field defects and neglect have not been included in the prescription standards. The current criteria (Supplementary Table 1) stipulate that “the minimum traffic rules must be understood,” “the devices can be operated smoothly,” and “PMD can be prescribed in the case of being judged suitable through MBI evaluation.” Apart from a K-MMSE score of at least 24 points and possession of a driver’s license, there are no cut-off values that connect upper extremity function or MBI scores to the ability to operate a PMD. Furthermore, no previous study has evaluated whether the current criteria effectively measure a person’s ability to maneuver a PMD. For patients who obtained a driver’s license before the onset of brain disease, possession of the license may not reflect their current driving ability because brain diseases can impact cognitive function. In addition, an electric wheelchair can be prescribed for patients with MMT grade 3 or lower according to the Medical Research Council (MRC) standards, and an electric scooter can be prescribed for those with a grade of 4 or higher. There have been conflicts between physicians and their patients who want specific types of PMDs because the same individual may be assessed as grade 3 or grade 4 by different testers.
Therefore, a more objective, systematic patient assessment system for PMD prescriptions is needed. A virtual reality (VR) computer simulation can be used to perform assessments in a relatively safe environment. Such a simulator can create various driving environments and enable a quantitative evaluation of a patient’s driving skills.1,11–16 In this study, we hypothesized that the ability to operate a VR-based PMD simulator reflects the participant’s real ability to operate a PMD. By comparing current PMD prescription standards with participants’ ability to operate the VR PMD simulator, we aimed to verify the current PMD prescription standards and to present the possibility of a VR PMD simulator as an alternative to current evaluation methods.
Methods
Participants
We enrolled participants who met the inclusion criteria from patients who visited the outpatient clinic of the rehabilitation department of our medical training center or who received inpatient rehabilitation treatment at our hospital from March to October 2021. A total of 52 participants with brain diseases including stroke, traumatic brain injury (TBI), and cerebral palsy were enrolled. All participants took part in a simulator driving test. All included patients (1) were over 18 years old and diagnosed with brain diseases, (2) had gait disturbance or limited outdoor walking ability, (3) understood the aim of this study and were able to agree to participate. This study was approved by the Institutional Review Boards of the National Health Insurance Service, Ilsan Hospital. All participants provided informed consent.
Equipment
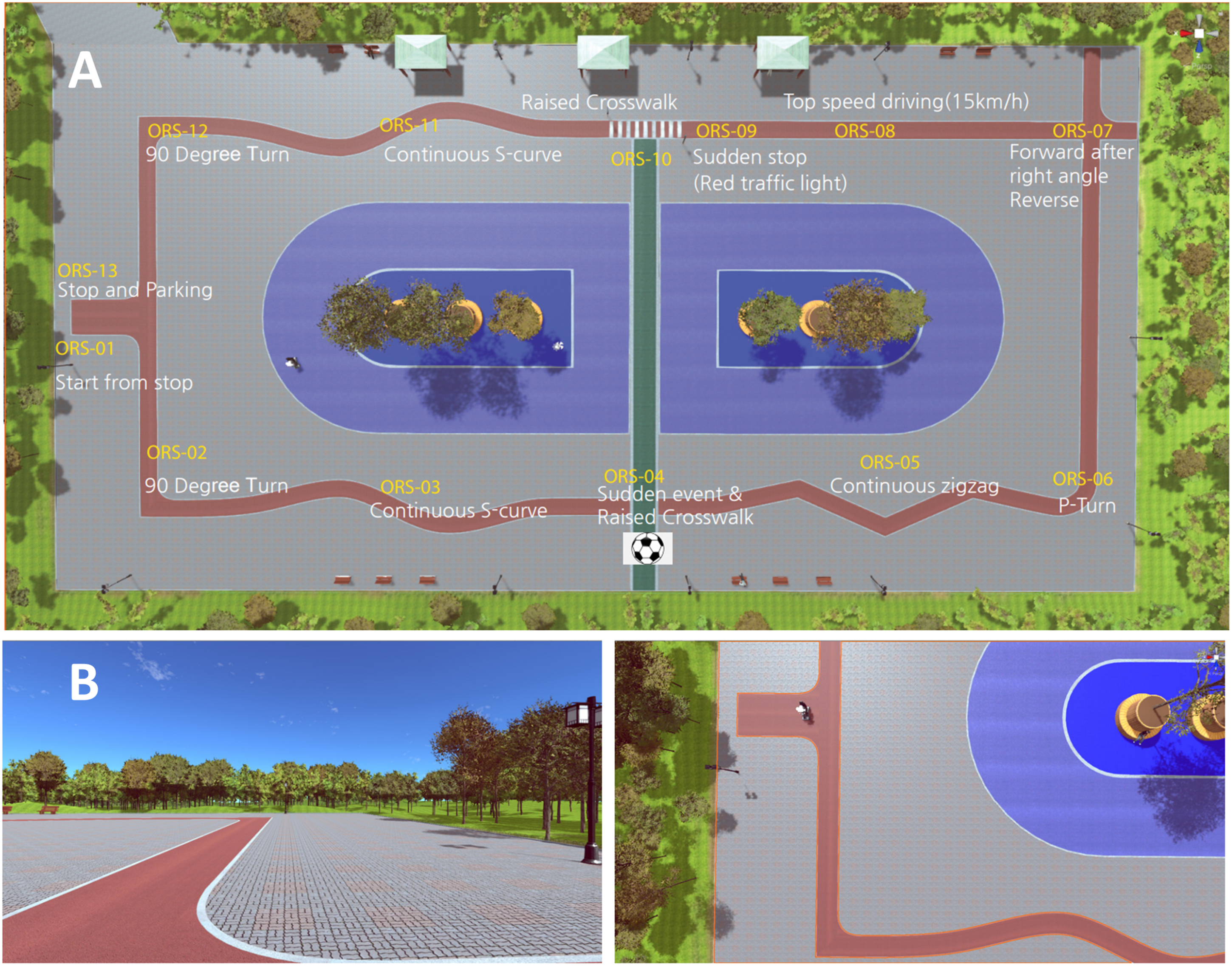
The VR PMD simulator is a device that can simulate the driving environment of a PWC or a scooter (Figure 1). Electric scooters are operated via handlebars; PWCs are operated with a joystick. The handlebar for scooter mode in the simulator includes a grip force sensor, a haptic device, a horn, an ignition key, a speed programmer, a turn indicator, a headlight switch, and a forward/reverse/acceleration/deceleration lever. The joystick controller for PWC mode includes a four-way joystick controller, a power switch, and an acceleration/deceleration control button. It can be adjusted for left-handed or right-handed use. The grip force sensor on the handlebar can measure hand grip strength and the difference in grip strength between the user’s hands (Figure 1). Two VR driving course scenarios were developed: an indoor virtual driving course (practice version) (Supplementary fig. 1) and an outdoor virtual driving course (test version). The outdoor course includes a range of obstacles and situations to assess the user’s ability to operate the PMD. The test road is 1.8 m wide, and the test consists of a total of 13 sections. The user must start the device, execute a 90-degree turn, navigate an S-shaped continuous curve, cross a highland crosswalk (a crosswalk with a speed bump), execute a zigzag, execute a P-turn, navigate a T-shape, and stop quickly from maximum speed (sudden stop at a red traffic light while driving at full speed). These tasks must be accomplished on various types of paved road surfaces (Figure 2). A total score of 100 points is possible; two points are deducted for each negative event, including course deviation, sudden acceleration/deceleration, sudden yawing, and overrunning the allotted time to complete the course (Supplementary Figure 2). To quantitatively and qualitatively evaluate each driver’s skill, both the results of the test and actual driving trajectory were automatically stored and analyzed for driving stability, including straightness, degree of left–right deflection, and course deviation. (A) System configuration and (B) operating modules of power mobility device simulator. (B) Handlebar for electric scooter mode and joystick controller for power wheelchair mode. Virtual reality driving course. (A) Top view. (B) Section 1 (start from standstill) and section 2 (90-degree turn).
Procedure
We collected data related used to current PMD prescription evaluation tools from all participants. These data included MMT, range of motion of the upper limbs, MBI, K-MMSE, walking ability, and possession of a driver’s license. We defined K-MMSE scores of 24 or higher to indicate almost no cognitive impairment; a score of 17 or lower indicated severe cognitive impairment. 17 The severity of unilateral neglect was assessed using the line bisection test; participants were then categorized as having normal, mild, or severe neglect. 18 The Korean version of the Western Aphasia Battery (K-WAB) was used to measure the aphasia quotient (AQ) in participants with suspected aphasia. 19 After a physical and neurological evaluation, participants’ driving performance skills were evaluated using the VR PMD simulator. Participants without severe muscle weakness in the upper limbs (MRC grade 3 or higher) and without a severe difference in strength between sides first attempted the driving test with the electric scooter (handlebar interface). Participants who could not operate the handlebars due to severe weakness in the upper limbs (below MRC grade 3) or to a severe difference in muscle strength between sides performed the test using a PWC (four-way joystick). The test included operating the handlebar, turning the headlights on and off, using the turn indicator, and using the forward/backward levers in response to auditory and visual instructions. Participants were then asked to complete a virtual outdoor driving course (test version). To evaluate the effectiveness of the current prescription standards, we compared the current PMD prescription standards to the results of VR PMD simulator driving test.
Statistical Analyses
Statistical analyses were performed using SPSS software (version 23.0, SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to examine quantitative continuous variables, including mean ± standard deviation and median (interquartile range). For data that were not distributed normally, the Mann-Whitney U test was used to confirm the differences in the driving test results of between groups, classified according to each variable. Among-group comparisons were made using the Kruskal-Wallis test. Post-hoc analyses were performed when the main effects were significant. Correlations between MBI subitems and driving test scores were explored using the Spearman test. For all analyses, a p-value of <.05 was considered statistically significant.
Results
A total of 52 patients completed the VR PMD simulator driving test. Thirty-two of the participants had hemiparesis (61.5%), and 20 (38.5%) had quadriparesis. The causative disease analysis showed that 28 (53.8%) participants had suffered a hemorrhagic stroke, 17 (32.7%) had suffered an ischemic infarction, three (5.8%) had TBI, and four (7.6%) had cerebral palsy or another cause. Forty-one participants (78.8%) performed the driving test using the PWC mode; the remaining 11 subjects used the electric scooter mode. According to the Korean National Disability registration criteria (Supplementary Table 2), 11 participants had mild disabilities (grades 4 5), 33 participants had severe disabilities (grades 1–3), and eight participants had not yet been registered as disabled.
Differences in driving test scores between groups according to gender, age, driver’s license, K-MMSE, neglect, and K-WAB.

Note: Values are median (IQR), mean ± SD, or as otherwise indicated. IQR = Interquartile Range; SD = Standard Deviation; K-MMSE = Korean Mini-Mental State Examination; AQ = Aphasia Quotient, MBI = modified Barthel Index.
All post-hoc analyses were done using the Dunn procedure. *, † indicate statistical significance in the post-hoc analysis.
Correlation of MBI subitems with driving test scores.

Values are median (IQR) or as otherwise indicated. IQR = Interquartile Range; MBI = modified Barthel Index.
Driving test results for groups according to K-MMSE and unilateral neglect.

Note: Values are median (IQR), mean ± SD, or as otherwise indicated. A p-value <0.05 indicates statistical significance. All post-hoc analyses were done using the Dunn procedure. *, † indicate statistical significance in the post-hoc analysis. N = Number; IQR = Interquartile Range; SD = Standard Deviation; K-MMSE = Korean Mini-Mental State Examination.
Discussion
The guidelines for prescribing wheelchairs and scooters identify items that can confirm user capacity and performance requirements as criteria. These include psychosocial and behavioral status, cognitive and perceptual skills (judgment, attention, decision-making, speed of information processing, planning, and problem solving), sensory impairments (vision, hearing, and the ability to identify obstacles and avoid collisions, judge speed and distance, and react quickly), upper limb capacity and risk of injury, prescribed medications, illicit drug use, long-term need, and cardiopulmonary functions. 20
Cognitive impairment limits the use of electric mobility devices.21,22 This study confirms that MMSE scores are related to PMD driving skills. Participants with cognitive impairment, that is, those with an MMSE score under 24, had lower driving scores than participants in the normal group (Table 3). For participants with cognitive impairment, more points were deducted due to driving time overrun and course deviation, and the total driving time was longer (Table 3). In addition, these participants had poorer driving stability, as shown on the driving trajectory graph (Figure 3). The MMSE can evaluate cognitive function relatively simply, but it also has some disadvantages; its evaluative accuracy varies depending on factors such as the patient’s educational background, age, and aphasia. Because this study included only a small number of participants, these findings may not indicate the appropriate MMSE cut-off value for PMD use. Driving trajectory of participants with and without cognitive impairment and neglect. (A) Neither cognitive impairment nor unilateral neglect. (B) Cognitive impairment without unilateral neglect. (C) Unilateral neglect without cognitive impairment. (D) Both cognitive impairment and unilateral neglect.
Along with motor skills and cognitive function, visuospatial function impacts a patient’s ability to smoothly operate a PMD. 10 The neglect group received lower driving test scores, and significantly more points were deducted due to driving time overrun for this group than for the normal group (Table 3). Furthermore, although these differences were not statistically significant, the neglect group had more deductions due to course deviation, sudden acceleration/deceleration, and yawing; these participants also had longer driving times (Table 3). In general, a higher number of course deviations and sudden movements correlate with lower driving stability. Therefore, the neglect group had more unstable characteristics than the normal group in terms of driving stability and safety. These characteristics can also be observed on the driving trajectory graph (Figure 3). If an inappropriate prescription is given to patients whose driving is unstable, the risk of PMD-related accidents may increase.
In this study, there was no correlation between aphasia and driving assessment results (Table 1). However, aphasia may limit patients’ ability to understand the traffic rules that impact PMD operation. 23 Of the 14 total subjects, five had severe aphasia with an AQ of 62 or lower. All but one of these scored over 90 points in the driving test, and all of them had Broca’s aphasia, measured using Kertesz’s method. 24 The participant with the lowest AQ score had global aphasia and a low driving test score of 66 points. Therefore, the possible influence of aphasia subtype on driving score cannot be excluded. However, as our sample size was too small to allow statistical analyses by aphasia subtype, further research is needed.
Currently, there is only a vague statement of eligibility for MBI assessment, and there are no objective specifications in the prescription criteria (Supplementary Table 1). However, our analysis showed no correlation between driving score and MBI subitems (Table 2).
Our test with the VR-based PMD simulator was related to cognitive and visuospatial function, but not by ambiguous criteria such as MBI. Therefore, newer prescription standards based on VR-based PMD simulator results would save time by eliminating the need for tests that are not related to a patient’s ability to operate a PMD.
One of the most important aspects of PMD is safety.25,26 Currently, patients do not receive proper driver training or safety education before or after receiving a prescription for a PMD. A recent survey found that only 28% of PMD users had received driving safety education and training. 9
According to a 2015 survey by the Korea Consumer Agency on the use of PMDs, 35.3% of patients who used a PMD fewer than four times a week said that they did not use their PMD often due to problems related to the ability to operate the PMD, and 29.4% said they did not use their PMD due to problems related to driving safety. 27 Of 77 electric wheelchair users in that study, 31 (40.3%) had experienced wheelchair-related accidents, and among 210 electric scooter users, 71 (33.8%) had experienced an accident. 27 The report adds that patients do not receive basic safety education or driver training, which increases the risk of accidents.
Our VR PMD simulator can be used for PMD driving training as well as for evaluating patients for PMD prescriptions. Sufficient driver training with the PMD simulator could prevent wheelchair-related accidents.15, 28 Furthermore, a simulator could provide more opportunities to disabled people who are currently ineligible for PMD prescriptions due to a lack of driving experience, thereby broadening the population of eligible patients.
This study has several limitations. First, the sample size was relatively small. Second, many participants had no previous experience with driving a PMD. This could lead to some bias in the findings, especially when our participants’ results are compared to the driving skills of experienced PMD users. Third, the results with the simulator used in this study have not yet been compared to similar tests using a real PMD. Therefore, further research is needed to validate the comparability of VR PMD simulator operation to actual PMD operation. Finally, the reliability of our data could not be confirmed as each participant completed only a single driving test; no repeated tests were performed. This was because of the practical challenges of conducting repeated tests with outpatient participants.
The driving ability test using the VR-based PMD simulator indicated that driving ability and safety differed based on cognitive impairment and unilateral neglect. No differences were observed based on gender, age, possession of a driver’s license, MBI subitems, or aphasia. In patients with brain injuries, a driving ability test using a VR PMD simulator can be an objective and safe method for comprehensively evaluating patients’ PMD driving skills, offering an alternative to the current standards for PMD prescriptions.
Supplemental Material
Supplemental Material - Using a virtual reality power mobility device simulator to assess the driving skills of people with brain diseases
Supplemental Material for Using a virtual reality power mobility device simulator to assess the driving skills of people with brain diseases by Namwoo Kwon, Myung Joon Lim, Ilki Hong and Hyoung Seop Kim in Journal of Rehabilitation and Assistive Technologies Engineering.
Footnotes
Acknowledgements
Min-A Kim is a certified occupation therapist and a research assistant in this study. All evaluations and data were collected by her. We appreciate her efforts.
Author contributions
Conceptualization: Kim HS, Hong IK, Lim MJ. Data curation: Kwon NW, Hong IK, Kim HS. Data analysis: Kwon NW, Hong IK. Funding acquisition: Kim HS, Lim MJ. Investigation: Kwon NW, Kim HS. Methodology: Kwon NW, Kim HS. Suppliers: Hong IK. Writing - original draft: Kwon NW. Writing -review & editing: Kim HS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Rehabilitation Research and Development Support Program (#NRCRSP-EX20006) of the National Rehabilitation Center, Ministry of Health and Welfare, Korea.
Disclosure
Unipolar Inc. was responsible for the development of the virtual reality-based PMD simulator and the content of the virtual reality simulation. The authors declare that they have no competing interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.