
Abstract
Introduction
The purpose of this study was to test a novel activity monitor that tracks the time a prosthesis is worn, and the nature of the ambulatory activity conducted with the prosthesis. These capabilities allow prosthesis users’ wear and accommodation practices (e.g., temporary doffing) to be monitored, and the intensity of their activities to be assessed.
Methods
A portable limb-socket motion sensing system was used to monitor doffs, walk bouts (≥5 steps), low locomotion (2–4 steps), stationary positions, and weight shifts in a group of transtibial prosthesis users. The relationship between doff time and active motion time was investigated, and durations of low and high intensity active motions were compared.
Results
For the 14 participants tested, the median prosthesis day duration ranged from 12.8–18.8 h. Eleven participants typically doffed five or fewer times per day, and three participants typically doffed 10 or more times per day. Nine participants demonstrated a positive correlation between daily doff duration and active motion duration. Six participants spent more time in weight shifts than walk bouts, while eight participants spent more time in walk bouts than weight shifts.
Conclusion
Capturing don time and temporary doffs and distinguishing weight shifts from walks may provide insight relevant to patient care. Longer-term monitoring studies should be conducted, and the clinical utility of the data evaluated.
Keywords
Introduction
Step count is a metric commonly used to assess activity in people with lower-limb amputation. An accelerometer and data storage unit are mounted to the prosthesis, thigh, waist, or wrist to record how many steps the person takes over a period of time. 1 Processing strategies are executed to calculate various activity-related metrics, including steps/day, cadence, fitness and intensity of activity, type of activity and body posture, commercial scores, and gait quality. 2 Data may be communicated to users via a personal device, such as a watch or phone, to help them achieve activity targets. More recently, inertial measurement units (IMUs) that add a 3-axis gyroscope and magnetometer to the accelerometer have been introduced. Data from IMUs have been used to identify turning 3 and to compare in-home and out-of-home ambulation.4,5 Computational learning algorithms operating on IMU data have been developed to characterize terrain stiffness, surface angle, and presence of stairs, 6 as well as activity and bodily position.7,8 A load cell positioned underneath an osseointegrated implant was claimed to improve upon accelerometer-based methods for activity characterization by providing the true load delivered to the prosthesis. 9 However, commercial devices using load data for the purpose of studying activity have not experienced widespread use in the prosthetics industry.
Though available technologies like IMUs, step activity monitors, and load cells can be used to quantify activity, they do not provide an assessment of how much people with limb amputation wear their prosthesis each day since limb presence in the socket is not detected. This limitation makes it difficult to identify prosthetic socket accommodation practices like temporary doffing. Temporary full or partial doffing of the prosthesis for 10 min or more has been shown to facilitate limb fluid volume recovery and may be used to help stabilize limb fluid volume.10–13 In a study on 29 participants with transtibial amputation, participants who did not change sock ply during the day (non-accommodators) spent more time with their prosthesis doffed and reported better outcomes than participants who did change sock ply during the day (accommodators), 14 suggesting that temporary doffing may be beneficial. Possibly, users increase their daily activity with more temporary doffs. In a different study, an inductive sensor worn by a group of 21 participants with transtibial amputation for about 2 weeks showed that only about 12% of the temporary doffs during the day were done to change sock ply. 15 This result suggests that temporary doffing may already be used as an accommodation method by some prosthesis users. The primary purpose of the present study was to use a sensing system that simultaneously monitored both limb presence in the socket and active motion to investigate new prosthesis use categories, including temporary doffs and weight shifts, in a group of participants with transtibial amputation. The results were intended to provide insight into new variables potentially useful for characterizing prosthesis users’ activity.
A secondary purpose of this study was to delineate the type of activity being performed by a prosthesis user. Several researchers have pursued this type of investigation, most of them delineating sitting, standing, lying, and stepping. 2 Others extended from these types of activities to delineate the time-of-day steps were taken, 16 durations of activities, 17 or the direction of movement.3,9 In the present study, we sought to extend from those efforts by developing a sensor capable of measuring weight shifts. Weight shifts are active movement within a confined space. Weight shifts are at the lower end of the activity intensity spectrum while bouts of walking and running are at the higher end. We sought to identify to what degree this delineation, weight shifts versus steps, differentiated prosthesis users’ active motion, i.e., what percentage of active motion was included within these two types of movement, in a group of participants with transtibial amputation. A wide range in the ratio of percentage time weight shifting to percentage time walking measured in this pilot study would suggest that further exploration of this metric to characterize user activity intensity would be warranted.
In this study we used a compact version of a portable limb-socket interface motion sensing system developed in previous work 18 to characterize doffs, walk bouts, low locomotion, stationary positions, and weight shifts in a group of transtibial prosthesis users. The small lightweight system was added to participants’ existing prosthetic sockets and used to measure their activity. The following questions were addressed: (1) Does active motion time increase with doff time? (2) Which active motion – walk bouts or weight shifts – dominates the total time of active use, and how do results vary across participants? (3) Do participants show common patterns of prosthesis use over the day, e.g., active motion focused over a certain time range? (4) Is the portable sensing system durable and thus potentially appropriate for long-term activity monitoring?
Methods
Participants
Potential participants were included in this study if they were at least 18 years old, had a transtibial amputation (unilateral or bilateral) at least 6 months prior, and used a definitive prosthesis regularly. They needed to be wearing or be capable of wearing a silicone elastomer liner. They also needed to be capable of walking with a variable cadence and traversing most environmental barriers such as curbs, stairs or uneven surfaces, activity typical of a Medicare Functional Classification Level (MFCL) K-3 or higher community ambulator. Participants were excluded if they had an open wound on their residual limb. Institutional review board approval was obtained, and all individuals gave written informed consent before any test procedures were initiated (STUDY00000497 (in lab), STUDY00001779 (out of lab)). Participants were recruited from our registry of prior studies and from flyers placed in clinical settings such as a medical center, outpatient waiting rooms, and prosthetics clinics.
Sensing system
The custom-designed sensing system included two sensor antennae, a “target” material embedded in the liner, and electronic circuitry mounted within a box that was fastened to the participant’s socket or pylon. Inductive sensor antennae (32 mm diameter, <0.2 mm thickness) were fastened to the inside of the socket with double-sided adhesive tape (SpeedTape, Fastcap, Ferndale, Washington) at two posterior mid-limb locations (lateral and medial), and covered with an ultra-low friction film with a durable self-adhesive backing (ShearBan™, Tamarack, Blaine, Minnesota) (Figure 1). Our experience is that the two posterior mid-limb sensors typically show comparable results, thus use of two sensors provided a backup in the event one sensor did not function. Sensors positioned at proximal locations were prone to mechanical failure,
18
thus those locations were not included in the present study. The two sensors were placed equidistant from the posterior midline and equidistant between the posterior proximal trimline and the distal end of the socket. Placement of the sensors in participants’ sockets required less than 30 min. Each antenna had a capacitor soldered to its terminals to form an inductor-capacitor (L-C) unit. The target was a trace amount of iron powder embedded in the participant’s liner. The powder was placed within a thin layer of the elastomer, close to the fabric backing. The test liners used in this study were fabricated by a prosthetic liner manufacturer (WillowWood, Mt. Sterling, Ohio) for research purposes. When the L-C unit was powered by an inductive sensing chip (LDC1614, Texas Instruments, Dallas, Texas), the presence of the magnetically permeable iron local to the antenna reinforced the inductor and lowered the sensor’s oscillation frequency in a distance-dependent manner. The change in frequency measured by the inductive sensing chip was a sensitive measure of distance between the target and sensor. In addition to the inductive sensing circuit, the electronics board included a data logger.
18
A 2,000 mA∙h battery (LP-803860 3.7V) with protection circuit module (PKCELL, Shenzhen, China) within the housing powered the circuit. Instrumented prosthetic socket. Left: Sensor antenna positioned at a posterior medial mid-limb location with the tail exiting over the socket brim. The antenna is covered with a low friction adhesive material (white). Right: Participant wearing his instrumented socket ready to leave the lab for take-home use. Wires from the sensor tails plug into a data acquisition unit fastened to the pylon. The soft wrap over the data acquisition unit is removed.
The sensors were calibrated using a two-step procedure as described in a prior clinical study. 19 First, a flat benchtop testing jig was used to displace the sensor away from the target in small increments. The data were used to generate a calibration curve. Then the liner was rolled onto an elastomeric, conical, inflatable silicone balloon. The liner assembly was then placed in the prosthetic socket. Data were collected with the balloon inflated to 34.5 kPa so that the liner was pushed flush with the inside socket surface. The balloon calibration established a zero position for each sensor. A thermistor was soldered to each antenna’s terminals. A thermal calibration procedure was conducted by placing the socket into an oven and then slowly raising and then decreasing the temperature. The thermal calibration curve was used during post-processing to thermally compensate the collected data.
Protocol
Upon arrival to the lab, the research practitioner first inspected the participant’s residual limb and gait to verify the person had a well-fitting socket. Basic demographic data were collected, including age, weight, height, time since amputation, etiology, health history, limb length and mid-limb circumference. The type of socket, suspension, foot and ankle componentry, and participant-reported sock use were documented. Participants doffed their prosthesis so that the researcher could add the instrumentation to the socket as described above.
Once the socket was instrumented, the participant donned the prosthesis. The person walked in the lab and on the treadmill while the research prosthetist assessed the gait and socket fit. Minor adjustments were made if necessary (e.g., alignment, sock ply adjustment). The scripted protocol included sits, stands, and walks on flat, inclined and declined surfaces. After the activity protocol was completed, participants were instructed to leave the lab and wear the socket for approximately 1 week, performing their normal activities with the instrumented prosthesis. When participants returned to the lab, the researcher removed the instrumentation.
Data analysis
The data were downloaded, converted to distance units (millimeters), and thermally compensated. For 13 of the 14 participants, the mean of the two sensor channels was used for data analysis. For the other participant (P13), only the lateral mid-limb channel was used because of inconsistent performance in the medial channel.
To parse the data into days, a don/doff threshold value in the sensed distance signal was selected from visual inspection of the first day of data. A sensed distance threshold of approximately 10 mm was used for all participants. Doffs were sections where the data were above the threshold for more than 5 s continuously. The remaining data were dons. The start of a prosthesis day was defined as the first data section where the socket was donned for more than 30 min. If there was a data section shorter than 30 min within 1 h prior to this timepoint then that data section was used instead to define the start of a prosthesis day. The end of a prosthesis day was the start of a doff longer than 60 min with no dons longer than 30 min between that point and the start of the next day.
Data within each prosthesis day were delineated into five activities: doff; walk bout; low locomotion; stationary position; and weight shift. During walking, amplitude peaks occurred during swing phase, and amplitude troughs occurred during stance phase. An amplitude threshold for walk detection, expressed as a percentage of the peak-to-trough sensed distance, was selected by the researchers from visual inspection of the first day of data. The amplitude threshold was approximately
For each participant, durations of the activities were assembled into bar charts for each day and pie charts for the entire test duration. Steps during walk bouts and low locomotion were tabulated for each day and for each hour of the day and plotted as bar graphs. The percentage of time spent at each of the three active motions (walk bout; low locomotion; weight shift) was calculated and plotted as bar graphs. Plots were generated to visualize relationships between temporary doff time and active use time, but no inferential statistical analyses were conducted to compare participants or categories. This strategy was justified because the group size was small, the number of monitored days differed among participants, and the intent of this investigation was exploratory, to determine if the sensing system and data warranted further investigation.
Results
There were 13 males and one female in the study. Thirteen participants had their amputation as a result of trauma, and one as a result of infection. Median participant age was 56 years (range 34–73), and median time since amputation was 16 years (range 2–50). Median participant body mass index (BMI) 20 was 30.5 (range 23.7–36.0). Twelve participants regularly used a patellar tendon bearing socket (PTB) with locking pin suspension, and two used a total surface bearing (TSB) socket with vacuum suspension. Participant demographics and prosthesis characteristics are summarized in the Appendix (Table A1). Data were collected on each participant for between 3 and 8 days (Appendix (Table A2)). When data was collected for less than 7 days, it was because there was an antenna mechanical failure. Thermal compensation data were available for 40 of the 76 days of data collection. The thermal compensation algorithm tended to shift the sensed distance data v. time plots up or down the y-axis a short distance but did not modify the shape of the curve. Thus, in this study since activity classification relied on relative rather than absolute data, not executing the thermal compensation algorithm had minimal impact on prosthesis use classification results.
Prosthesis day duration (not including first and last day of wear, i.e., days the participant started to wear or stopped wearing the monitor) was between 10 and 20 h for all but 4 days of data collection: participant number 12 day 4 (29.3 h); participant 14 day 7 (5.6 h); participant 3 day 4 (8.7 h); and participant 5 day 3 (8.2 h). The median prosthesis day duration (first and last day excluded) for all participants was between 12.8 and 18.8 h (median 15.3 h) (Appendix ((Figure A1))). The median number of steps/day was 3213 (range 574 to 11,088).
The number of temporary doffs each day for each of the 14 participants is shown in Figure 2. Eleven of the 14 participants doffed their socket a median of five or less times per day, while three participants doffed a median of more than 10 times per day. In Figure 2, the median duration per doff (min/doff) and the interquartile range (min/doff) are shown above the bars for each participant. Number of temporary doffs each day of wear. Results for all participants are shown. Each participant’s results are a different color. Data are shown for all test days. The first and last day were shorter in duration than the other days because the participant came to or left the lab. Med, median minutes/doff; IQR, inter-quartile range of minutes/doff.
The distribution of prosthesis use across all categories for each participant’s prosthesis day time (the sum of all prosthesis days) is shown in Figure 3, and results for all single full days of data collection are summarized in Table 1. Participants spent between 3% and 39% (median 21%) of their total prosthesis day time in active use (i.e., in walk bouts, low locomotion, and weight shifts). Out of these three active conditions, they spent the least percentage of active use time in low locomotion (between 3 and 29% (median 16%) of the active use time). Walk bouts were between 31% and 62% (median 41%) of the active use time, and weight shifts were between 12% and 60% (median 39%) of the active use time. Six of the 14 participants (numbers 4, 5, 9, 12, 13, and 14) spent more time in weight shifts than in walk bouts, while eight participants (1, 2, 3, 6, 7, 8, 10, and 11) spent more time in walk bouts than weight shifts. When considering all full days of monitoring (48 days total), the data varied considerably across the study as to the time spent stationary, i.e., wearing the prosthesis but not in active use, ranging from 18% to 95% (median 68%) (Table 1). Percentage time participants spent at each activity. Duration of doffs, stationary positions, weight shifts, low locomotion, and walk bouts for all days. Data in the pie charts were calculated across the entire data collection period as the sum for the activity expressed as a percentage of the sum of prosthesis day durations. Participants are grouped by the categories illustrated in Figure 4. Red= Category 1; Blue= Category 2; Yellow= Category 3. Minimum, maximum, and median for all full days of data collection - time spent in different activities. pr, prosthesis, min, minutes. *The sum minutes for the prosthesis use category divided by the average prosthesis day duration (min/day).

We conducted an exploratory analysis to investigate how participants distributed their walking activity over the course of a day. Six of the 14 participants (2, 4, 5, 10, 12, and 14) walked most (i.e., had the highest per hour sum of walk bout and low locomotion time) at the beginning of the day then abruptly reduced their per hour walk activity and stayed at a minimum for the rest of the day (Category 1) (Figure 4(a)). Six participants (3, 6, 7, 8, 11, and 13) gradually increased their per hour walk activity, plateaued, and then gradually decreased their activity over the rest of the day (Category 2) (Figure 4(b)). The remaining two participants (1, 9) did not show a consistent pattern in their activity (Category 3) (Figure 4(c)). The median number of steps per hour of prosthesis use was highest for Category 1 (251, range 70–544), following by Category 2 (237, range 80–958), followed by Category 3 (120, range 40–225). Steps per clock hour for all days combined. Example results from one person for each participant group. (a) Category 1: initiated and maintained highest steps/h in the first part of the day then abruptly reduced activity and stay at a minimum the rest of the day; (b) Category 2: increased activity, maximized, and then decreased activity over the rest of the day; and (c) Category 3: no consistent pattern.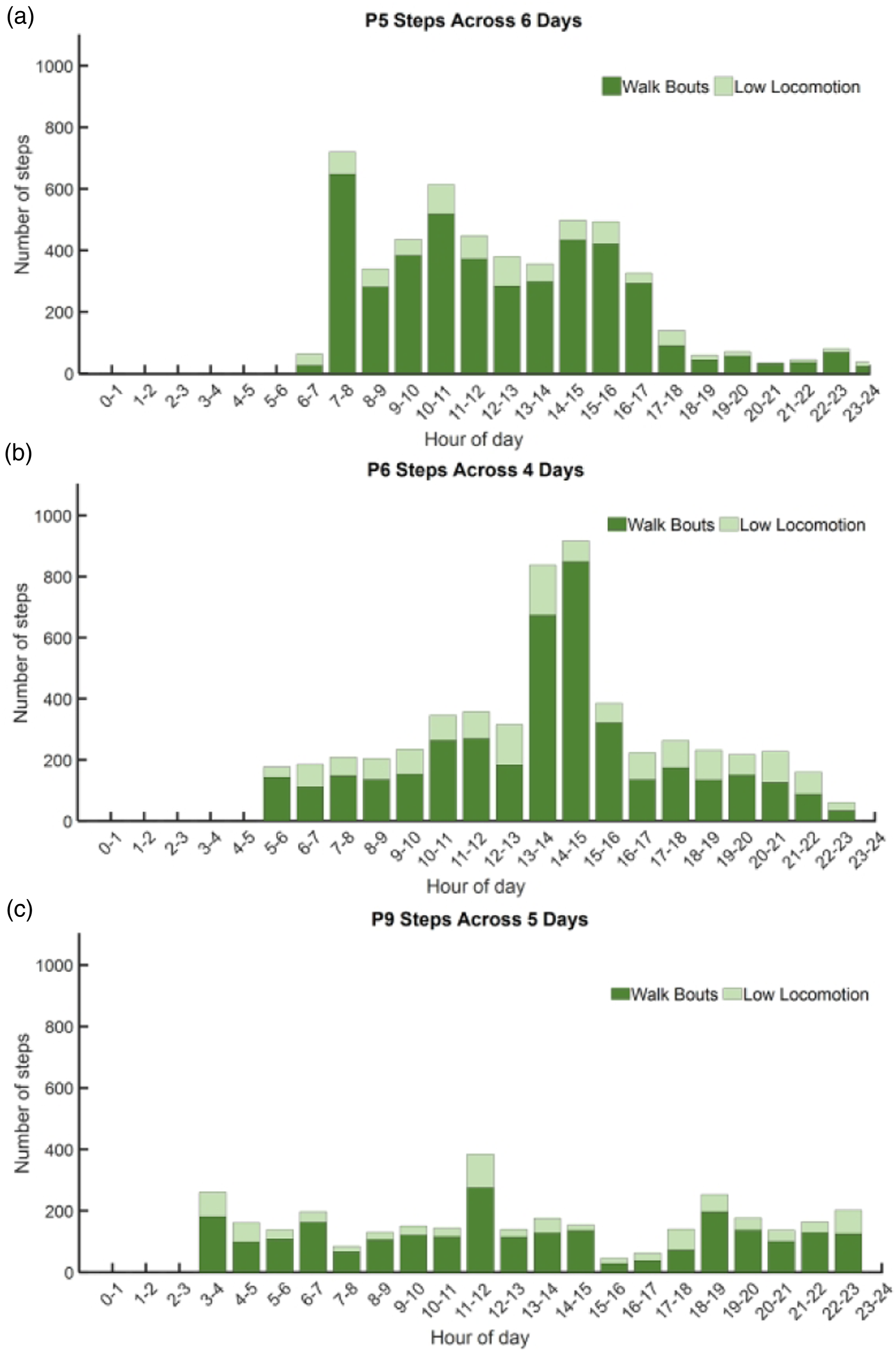
Visual inspection of the plots comparing the duration participants temporarily doffed their prosthesis per day and their active motion time per day (sum of walk bout, low locomotion, and weight shift times) revealed that nine of the 14 participants demonstrated a positive correlation between doff time active motion time (Figure 5). However, some participants had very few days of data collection, causing outliers to markedly affect the correlation results. Doff time and active motion time. Doff time is the x-axis, and active motion time is the y-axis. Data are normalized to the maximum for each axis for each participant so that the direction of the least-squares linear fit line can be clearly visualized. Each circle indicates a day of prosthesis use. Active motion time is the sum of time spent in walk bouts, low locomotion, and weight shifts.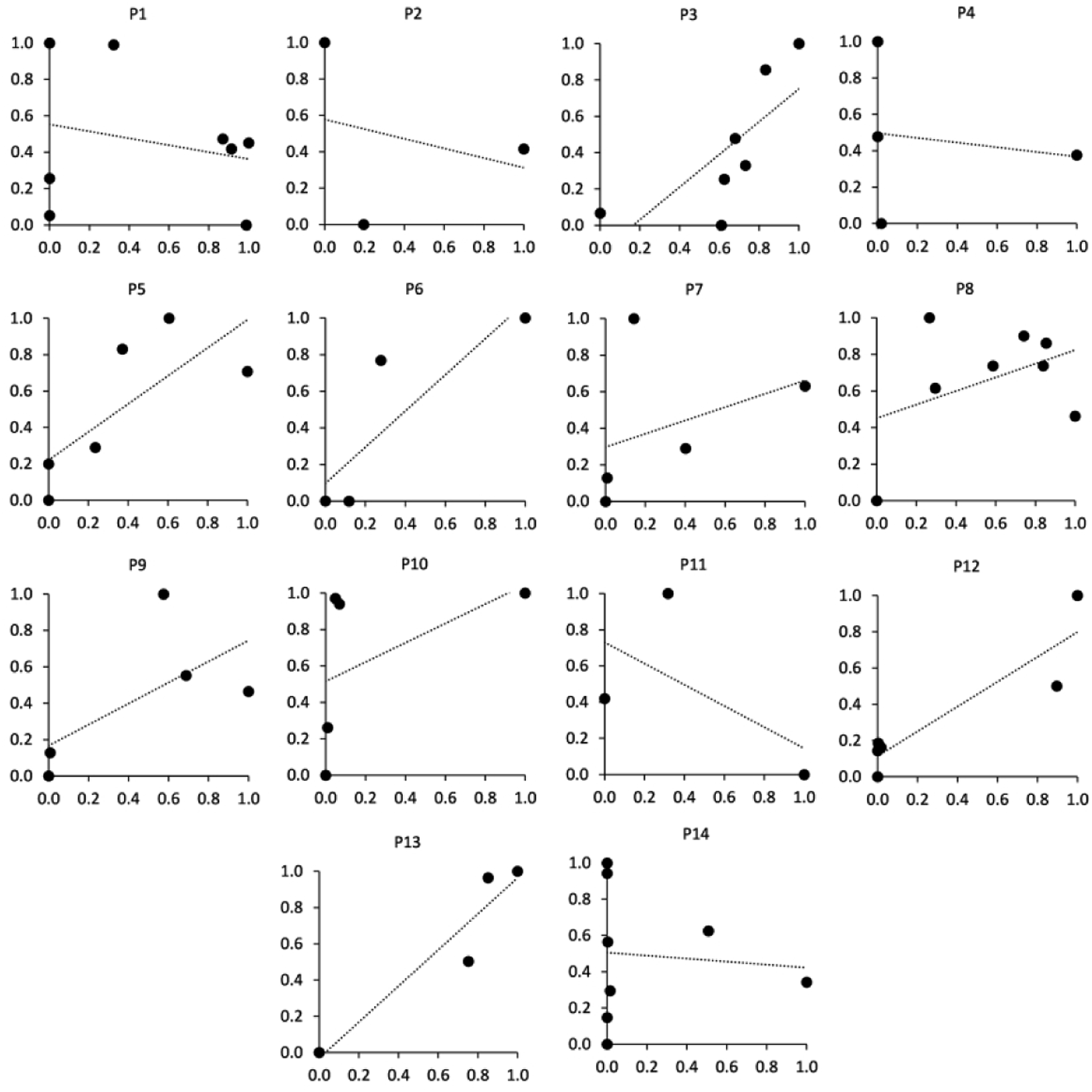
We calculated the percentage of active use time for each of the three categories (walk bouts, low locomotion, weight shifts) and then sorted the participants by highest to lowest walk bout percentage (Figure 6). Walk bout percentage and weight shift percentage were both greater than low locomotion percentage for all participants but one (participant 1). Participants with a high bout percentage generally had a low weight shift percentage. Five of the six participants in Category 1 were in the left half of the bar graph (Figure 6), and five of the six participants in Category 2 were in the right half. Percentage of all active motion time spent in weight shifts (wt shfts), low locomotion (low locom), and walk bouts (bouts) for each participant. Beneath the bar graph, participant membership in one of the three groups from the activity distribution over the day classification (Figures 4(a)–(c)) is shown. Five of the six participants in Category 1 (red participant numbers) were in the right half of the bar graph, and five of the six participants in Category 2 (blue participant numbers) were in the left half.
Discussion
Improvements in activity monitoring technology are advancing the characterization of prosthesis use in people with lower-limb amputation, allowing researchers to extend beyond the traditional measurements of step count and cadence to more fully characterize prosthesis users' clinical outcomes. 2 Activities such as working at a counter or moving items around while sitting at a desk may soon be detectable, for example. Providing body support to enable these actions is a key function of the prosthesis from the user’s perspective, but one that is rarely measured using traditional step counting technologies. As a more detailed characterization of activity becomes available, limb presence or absence within the socket becomes more important to detect. Without it, a stationary body position cannot be delineated from not wearing the prosthesis at all. Further, the duration of temporary doffs, relevant to the stabilization of limb fluid volume, 13 cannot be accurately quantified. The purpose of this study was to investigate new prosthesis use categories, including temporary doffs and weight shifts, in a group of participants with transtibial amputation. The results were intended to provide insight into new variables potentially useful for characterizing participants’ activity.
We found that all participants implemented temporary doffing as an accommodation method or to change socks. Though we did not query participants as to why they temporarily doffed their prosthesis, two participants (3 and 6) volunteered information that intermittent doffing extended the duration they comfortably wore the prosthesis during the day, i.e., their prosthesis day duration. The median temporary doff duration for 10 of the 14 participants in the present study ranged from 0.6 min to 13.3 min (Figure 2), suggesting that relatively short doffs effectively met their needs. Further investigation using a consistent number of monitored days across participants and a larger group of participants would be needed to make interpretations applicable for clinical care recommendation. In a prior study where participants recorded their sock use during about a 2-week period, 15 we found that doff durations for socket release ranged from 4.7 min to 80.6 min. In that study, 12% of the temporary doffs were to change sock ply while the rest were for temporary socket release.
In this small group of participants, we did not compute a correlation between doff time and active motion time since there were too few days of data collection to conduct a valid statistical analysis, but instead only considered if the slope was positive or negative. The positive slope for nine of the 14 participants is interesting (Figure 5) and suggests that further investigation of this relationship should be pursued. We note that in the present study the monitoring period was short, i.e., from 3 to 8 days, and sitting weight shift data were included within the active motion category. Sitting weight shifts are relevant to prosthesis use because during these times the prosthesis provides essential mechanical support to use the upper body to accomplish the task at hand. Additional research is needed to determine how these features of the study (number of days, inclusion of sitting weight shifts within the active motion category) data analysis affected the results. In addition, it needs to be determined if the relationship between doff time and active motion applies only to a subset of prosthesis users, i.e., those with certain physical, physiological, or other personal qualities.
Participants in this study spent between 18% and 95% of their total prosthesis day time stationary (Figure 3), either sitting down or standing. They spent between 2% to 24% of their prosthesis day time in walk bouts, consistent with reports in the literature characterizing activity and bodily position in participants with transtibial amputation.21–24 The range of the time spent in weight shifts was <1%–18%, similar to the range of the time spent in walk bouts (2%–24%), demonstrating that weight shifts are a meaningful part of prosthesis use activity. As shown in Figure 6, participants varied as to whether they spent more time in walk bouts or weight shifts.
Delineating weight shifting from walk bouts may facilitate understanding of a person’s prosthesis use and their componentry needs. Weight shifts are at the opposite end of the activity intensity spectrum from bouts of walking. They are less demanding in terms of energy expenditure and potential trauma to the residual limb. Practitioners may interpret weight shifts as moving within a confined space such as within a room or building, making frequent side motions and turns, or shifting while sitting at a desk. Presentation of weight shift data to practitioners may help them determine and justify componentry needs, for example, an ankle that facilities stability during multidirectional motions. Participants who spend little time weight shifting but a high percentage of their active motion time conducting walk bouts might benefit instead from componentry that facilitates efficient energy transfer during gait at the expense of less lateral stability. These suggestions are conjecture and would need to be tested through rigorous scientific investigation. Clinical investigations comparing weight shift and walk bout durations while participants use different types of componentry may help delineate to what degree active motion depends on the person’s lifestyle compared to the stability and energy return qualities of the prosthetic foot/ankle system.
The behavior of participants in Category 1 (Figure 4(a)) who abruptly reduced their walking each day at about the same time may reflect one type of prosthesis use pattern. Participants who ramped up their activity and then ramped down later in the data may reflect a different prosthesis use pattern. However, two participants told us that they knew that they could only conduct a certain amount of activity each day before they reached their limit, because of fatigue or soreness in their residual limb. The type of active motion users perform may affect their daily prosthesis use limit. We would expect, for example, that long durations of walk bouts would reduce the time-to-limit because walk bouts are more strenuous and deliver more energy to the residual limb than low locomotion or weight shifts. It may be possible to develop computational models to predict prosthesis users’ time-to-limit based on the durations of their different active motion levels to that point in the day. These models would have implications for patient training, componentry selection and justification. Further, delineating active motion in this manner may provide a quantitative outcome assessment to compare what actions people with limb amputation chose to do given different componentry choices.
Because dons and doffs were clearly identified using the sensing elements in this study, we were able to well define the beginning and end of a prosthesis day. Excluding bathroom, snack, or other breaks in the late evening (i.e., ≤30 min temporary don) was important towards characterization of prosthesis use because long periods of non-use between the prior active motion and the temporary don would have been added to the prosthesis day duration (Figure 3). In our view, temporary dons near the start of the day, like going from the bedroom to the bathroom to take a shower in the morning, however, were important to include within the prosthesis day duration because they were part of the preparation for the day. A future research need is to quantify if and to what degree using these strategies compared to accelerometer derived thresholds 1 affect clinical interpretation of the data.
Accurate and consistent quantification of prosthesis use and prosthesis day duration are relevant because they provide a means for comparing an individual to a group of people with the same disabilities or other characteristics. We noticed in this study that five of the six participants in Category 1 had higher durations of weight shifts than walk bouts, and four of the six participants in Category 2 had higher durations of walk bouts than weight shifts. In other words, participants who focused their high walk intensity (high number of steps/h) during a couple of hours during the day and walked with a lower walk intensity (lower number of steps/h) the rest of the time, tended to walk in bouts more than in weight shifts compared with participants who executed a consistent moderate walk intensity over the day. Participants 10 and 13, however, did not follow this pattern. Further investigation is needed to determine if the observed pattern was coincidence. The results suggest that prosthesis use monitoring may help practitioners to identify each patient’s prosthesis use pattern, information useful for planning treatment of the individual patient.
After days of use some participants’ sensing system experienced antenna mechanical failures, but this problem was less frequent compared with our previous efforts using the portable monitor. 18 This was in part because the antennae were not placed near the brim nor near bony sites on the residual limb. Shear stresses tend to be lower in the posterior mid-limb region than at the brim or bony locations, 25 which may have contributed to this result. Since antenna failures still occurred, sometimes after just a few days, we believe that in future investigations the antennae should be embedded within the socket wall during fabrication. 26 This change makes it impossible for practitioners to use the system on participants who already have well-fitting sockets – a duplicate socket, but with embedded sensors, must be made. Embedded sensors do not degrade even over months of socket use thus can be left in the socket permanently and plugged in when it is of interest to acquire data. Making users’ regular sockets with embedded sensors may be a reasonable practical strategy to avoid mechanical failures like those experienced by some participants in the present study.
Conclusion
The sensing system and analysis methods used in this investigation may have application to clinical care in prosthetics. The percentage time of walk bouts compared to weight shifts, which varied across participants in the present study, may provide insight into the intensity of users’ active motion and facilitate prescription selection. Characterizing doff durations rather than the total time a user spends doffed may help delineate brief socket releases, which may benefit limb volume stabilization,10–13 from long doffs, which may signify an issue wearing the prosthesis such as pain or fatigue. A next step is to embed the sensing elements in sockets during fabrication and implement the technology in long-term investigations to assess these hypotheses and the diagnostic and prognostic utility of the system.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Prosthesis day duration for all participants. The blue boxes indicate the range of the prosthesis day duration across all days (not including the first and last day when the participant visited the lab), and the yellow lines across the boxes indicate the median. There are no blue boxes for P2 and P11 because there was only one complete day of data for each of them. The data from P12 showed 1 day that was longer than 24 h because the participant worked a long overnight shift.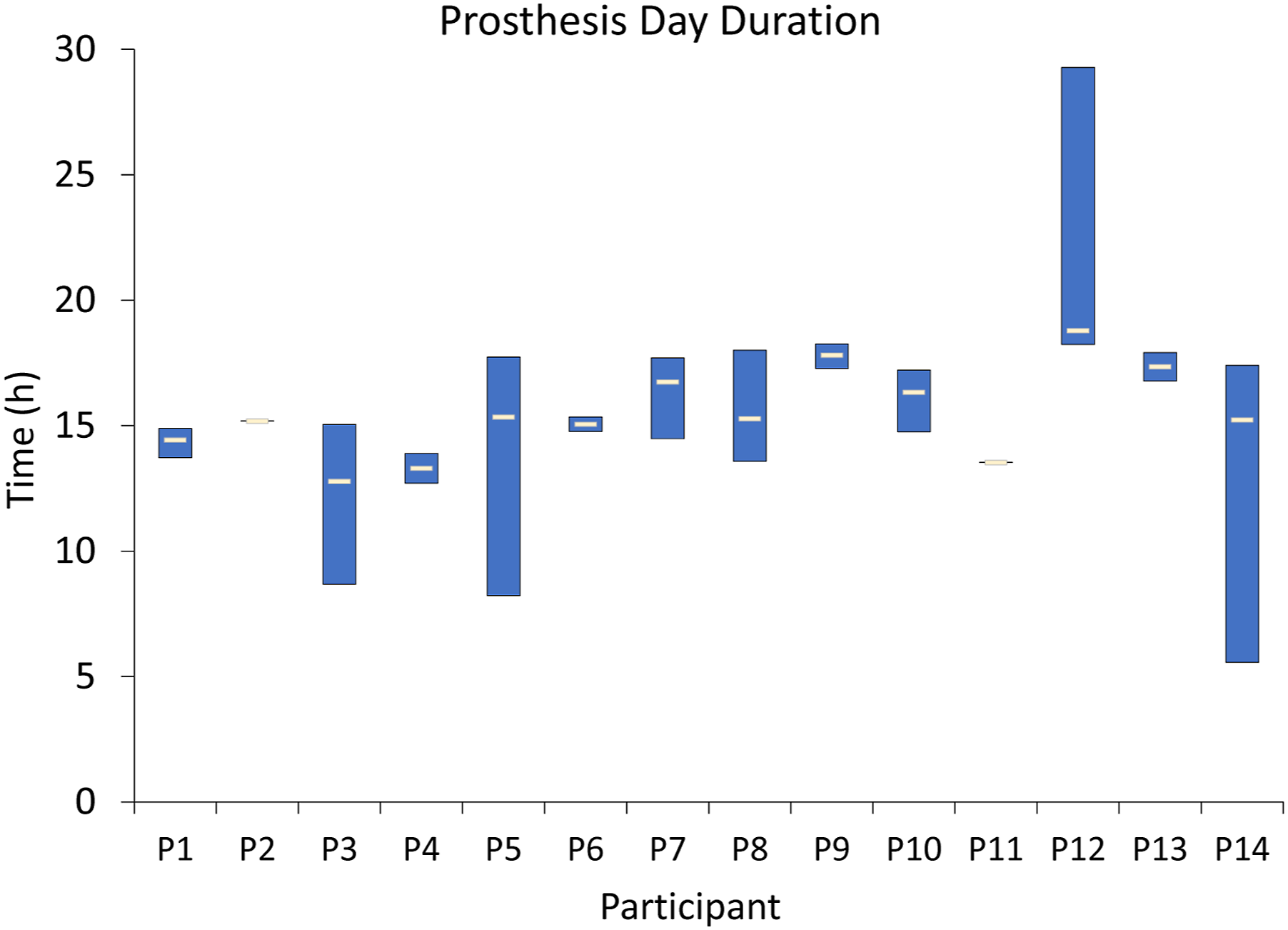
Participant demographics and prosthesis characteristics. Partic, participant; Gend, gender; BMI, body mass index; Amp, amputation; M, male; F, female; HBP, high blood pressure; MS, multiple sclerosis; DM, diabetes mellitus; chol, cholesterol
Partic
Gend
Age (y)
K-Level
BMI (kg/m2)
Time since Amp (y)
Etiology
Limb shape
Tobacco/Smoker
Co-Morbidities
P1
M
70
3
32.7
17
Trauma
Cylindrical
—
HBP
P2
M
56
3
30.7
11
Trauma
Conical
Tobacco
HBP, gout
P3
M
55
3
30.7
28
Trauma
Cylindrical
—
HBP
P4
M
73
3
29.5
50
Trauma
Conical
—
HBP, congestive heart failure
P5
M
34
3
36.0
14
Trauma
Cylindrical
Smoker
HBP
P6
M
38
4
25.0
16
Trauma
Conical
—
MS
P7
M
58
3
23.7
34
Trauma
Conical
—
—
P8
F
61
3
23.7
41
Trauma
Conical
Smoker
DM, stroke, HBP, high chol., thyroid disease
P9
M
42
4
25.1
2
Trauma
Cylindrical
Smoker
HBP
P10
M
72
3
27.6
44
Trauma
Conical
—
HBP
P11
M
47
4
30.2
5
Trauma
Cylindrical
—
—
P12
M
58
3
35.0
15
Infection
Conical
—
DM HBP
P13
M
53
3
35.8
12
Trauma
Conical
Smoker
HBP, high chol, kidney stones/function
P14
M
44
3
31.6
5
Trauma
Cylindrical
Smoker
HBP
Days of data collection on each participant.
Participant
Days
P1
8
P2
3
P3
7
P4
4
P5
6
P6
4
P7
5
P8
8
P9
5
P10
5
P11
3
P12
7
P13
4
P14
8
TOTAL
76