
Abstract
Keywords
Introduction
Microprocessor regulation of prosthetic ankle position and resistance to movement was introduced commercially in 2006. Since that time, a number of distinct approaches to such regulation have been introduced to the field and explored in the literature. Emerging benefits associated with such microprocessor feet (MPFs) include improved biomechanical performance during the negotiation of ramps and stairs1–6 increased toe clearance in swing,4,6 reduced peak pressures against the residual limb within the socket1,2 and increased prosthetic mobility.7,8 However, much of the literature supporting the use of MPF’s has been supported by product manufacturers1–5,7,9 and derived from measurements taken in controlled laboratory environments.1–6,9,10 Independent analyses of such feet in community settings have been limited.
Prosthetic mobility, often measured with instruments such as Prosthesis Evaluation Questionnaire (PEQ) 11 or Prosthetic Limb Users Survey of Mobility (PLUS-M), 12 is closely related to the overarching construct of physical function. Physical function has been described as one of many health indicators that can be used to monitor self-reported health and track rehabilitation goals among prosthesis users. 13 The domain of physical function plays a pivotal role in prosthetic rehabilitation. Prior studies have shown that poor physical function when assessed with performance measures is associated with increased risk of falls, mortality and morbidity among lower limb prosthesis users.14–17 However, very limited evidence exists examining the relationship of MPFs to improved physical function when measured with instruments such as the PROMIS-PF (Patient-Reported Outcomes Measurement Information system -Physical Function) or PEQ. The PROMIS-PF was recently developed to evaluate one’s capacity to complete various physical tasks, and was designed to overcome psychometric limitations such as floor/ceiling effects, responder burden, and lack of responsiveness 18
The PEQ is a well-validated population-specific patient reported instrument outcome assessing several constructs related to quality of life among users of lower limb prostheses including prosthesis function, mobility, psychosocial considerations and well-being. 11 While the individual items of the PEQ have not been validated for independent use, the breadth of the measure provides a number of individual test items spanning a diverse range of specific activities, environments and considerations that have received some measure of psychometric validation.
The primary purpose of this study was to determine the impact of MPF upon physical function as measured with the PROMIS-PF among transtibial prosthesis users as they transitioned to the use of a number of commercially available MPFs while maintaining their original socket fit. The secondary aim of this study was to provide preliminary findings on the impact of MPF upon back pain, residual limb pain, and hill ascent and descent using single-item questions from the Prosthesis Evaluation Questionnaire (PEQ). It was hypothesized that the transition from a non-MPF to an MPF would be associated with improvements in physical function as measured by a custom short form of the PROMIS-PF.
Methods
Study design
Records beginning in July 2019 through February 2021 from cases within a national provider of lower limb prostheses were assessed for eligibility. Patient cases were eligible if the patient was an established non-MPF transtibial prosthesis user and had a written prescription from a physician on file to transition into an MPF. In order to limit fit confounders, individuals were excluded if their socket was also replaced. To address the current hypothesis, patient reported outcomes collected as part of the patient’s evaluation (i.e. prior to receipt of MPF) and at a subsequent follow-up appointment (i.e. after patient had acclimated to the new MPF) were extracted for analysis. After the delivery of the MPF, board-certified prosthetists ensured that the patient's foot was properly fitted, aligned and adjusted for comfort. Since there were not onsite physical therapists present at the clinic...certified prosthetists provided training to patients on how to ambulate with the MPF. The current retrospective analysis of patient outcomes was approved by the Western Copernicus Group Investigational Review Board (Protocol # 20170059). Patients were exempt from informed consent. This study conforms with the STROBE guidelines.
Participants
Individuals included in this analysis were adults 18 years and older with lower limb amputation. There were no exclusions based on amputation etiology.
Endpoint measures
The endpoint measures in this analysis primarily focused on the results from a custom PROMIS Physical Function (PROMIS-PF) patient reported outcomes questionnaire. A secondary focus included the combination of independent item questions from the PEQ. The PROMIS-PF is a psychometrically validated instrument designed for the general population which can be customized to a targeted sub-population by selecting relevant and appropriate items. An eight-item PROMIS-PF short form was used in this study with items selected that were tailored towards lower limb prosthesis users. This approach of using a customized PROMIS short form is well documented in previous studies.19–21 Scores obtained can be compared to scores derived from other PROMIS physical function questionnaires when using the same item bank (v2.0). The eight items (i.e., PFA9, PFA21, PFA23, PFC6r1, PFA42, PFC41, PFC45r1, PFA56) taken from the PROMIS v2.0 PF item bank included assessments of bending down to retrieve clothing from the floor, going up and down stairs at a normal pace, going for a walk of at least 15 min, walking a block, carrying a laundry basket up a flight of stairs, transferring in and out of a low, soft couch, transferring off and onto the toilet and getting in and out of a car. Responses to the questions range on a 5-point ordinal scale ranging from “without any difficulty” to “unable to do”. Each response is assigned a 1-5 value, and then all responses are subsequently summed. This raw score is then converted to a normally distributed T-score for subsequent analysis and comparison using the HealthMeasures.net scoring service.
Items taken from the PEQ included assessments of prosthesis fit, prosthesis weight, sitting comfort, residual limb pain, back pain, and the respective abilities to walk both up and down a steep hill. Each item was individually graded on a 5-point ordinal scale with 5 representing a positive response option. Notably, while the original PEQ was comprised of continuous visual analog scales, there have been previous examples of effective use of PEQ questions administered with discrete, ordinal scale responses. 22
Independent variables
The main independent variable used was foot type (i.e., non-MPF and MPF). Other demographic variables used to describe the study population included age, sex, cause of amputation, height, weight, time between assessments, and employment status. For time between assessments, outcome pairs were retained for those patients who had experienced between 13 and 120 days between their two assessments. This time window was selected to ensure adequate acclimation to the new prosthetic foot without allowing so much time that changes might be reasonably attributed to factors outside of the prosthesis. Employment status was defined as being currently employed (or student status) or not.
Statistical analysis
Demographic and amputation-related factors were presented at the patient-level for this analysis. Prior to inferential analysis, the final sample was assessed for normality, homoscedasticity, absence of muticollinearity, and outliers. A paired t-test was used to assess the unadjusted differences in PROMIS-PF scores among the non-MPF and MPF. To adjust for the confounding effect that certain demographic and clinical variables may have on this relationship, a linear mixed effect regression model was conducted using the lme4 r package. 23 For the linear mixed effects analysis, MPF technology, gender, age, time between assessment, and etiology (collapsed to vascular disease/diabetes or not) were entered as fixed effects, while the intercept for subjects was entered as a random effect. The likelihood ratio test was used to obtain the p-values for the full model with the main independent variable versus a null model without the main independent variable. 24 Adjusted analyses were not conducted for the relationships between the use of MPF and PEQ items. All statistical analyses were performed using R (R Core Team, 2012).
Results
There were 23 patient cases that were found for analysis. Three of the patient cases had follow-up measures outside the inclusion window and were excluded. The remaining 20 patients presented with an average age of 56.65 years with an average of 31.85 days between baseline and follow-up assessments (Table 1). Over 60% of the sample were male (13/20), and the most frequent cause of amputation was vascular disease/diabetes. Subjects used a range of legacy non-MPFs, most of which were consistent with the community ambulation standards of the K3 Medicare Functional Classification Level. The Blatchford Elan was the most frequently utilized MPF (n = 12), but the Proteor Kinnex, Otto Bock Meridium, and Ossur Proprio were also utilized. While all MPF’s were fitted and aligned by board-certified prosthetists, there was no standardized physical therapy associated with the receipt of the new prosthetic feet.
Physical Function
Univariate analysis
Using a paired t-test for analysis, there was a significant increase in PROMIS-PF scores with the use of a MPF compared to those observed with the non-MPF (MPF - non-MPF mean difference: 5.40 ± 1.25; t(19) = 4.31 (p = 0.0004) (Figure 1). PROMIS-PF T-scores significantly improved for patients when using MPFs compared to their non-MPFs (p = .0004). MPF = microprocessor foot.
Multivariate analysis
Sample Demographics.

Linear mixed effect model for PROMIS-PF.
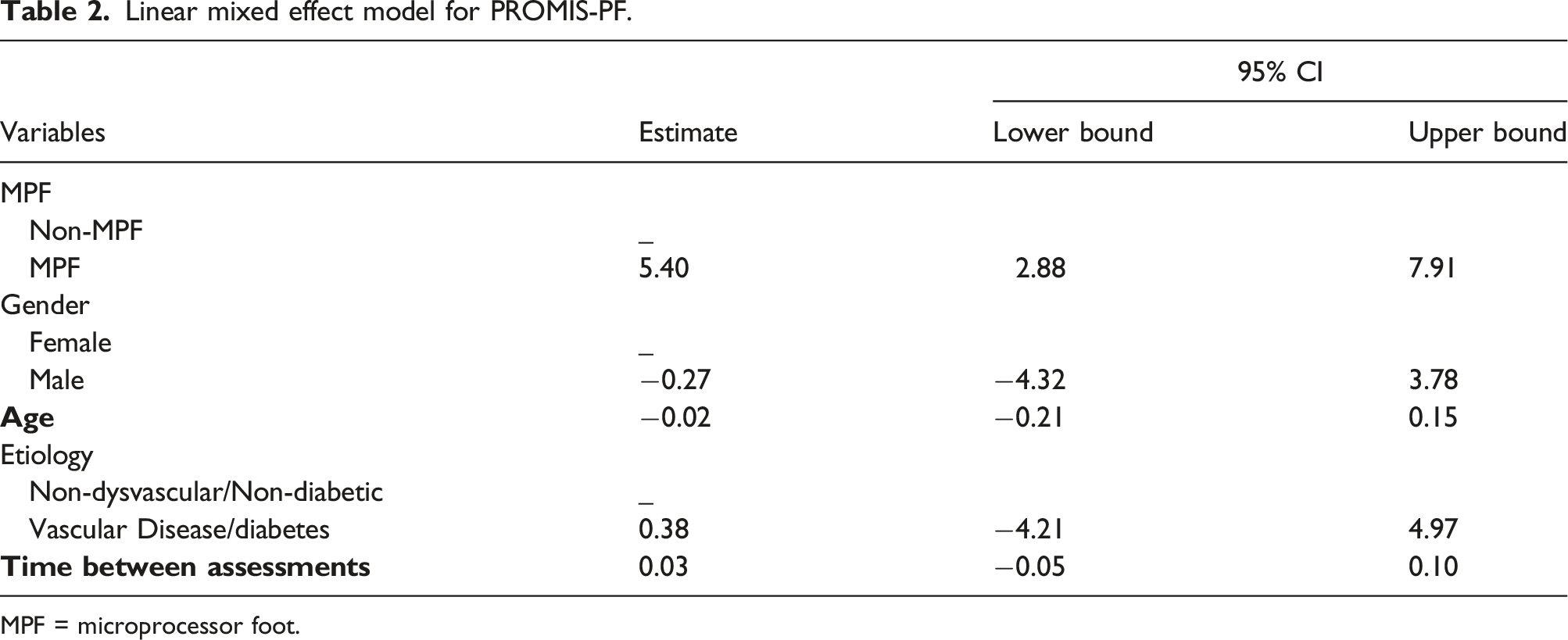
MPF = microprocessor foot.
Prosthesis evaluation questionnaire
Back pain, residual limb pain, and hill ascent and descent
Mean differences among PEQ items with Non-MPF and MPF.

Individual items from the PEQ; PEQ = Prosthesis Evaluation Questionnaire; MPF = microprocessor foot; Non-MPF = non-microprocessor foot; SD = standard deviation; CI = confidence interval; * = significant at p < 0.05.
Discussion
A Cochrane Review on the prescription of prosthetic ankle-foot mechanisms after lower limb amputation observed that most clinical trials on prosthetic ankle foot mechanisms were informed by laboratory data collected in controlled walking environments. 25 They encouraged the use of outcome measures with more ecological validity that took a broader view of mobility including transfers, maintaining balance, the negotiation of stairs and inclines, and walking over environmental obstacles. The data collected in this convenience sample of prosthesis users maintaining their transtibial socket while transitioning from a non-MPF to an MPF provides additional insights beyond the controlled laboratory environments from which much of the evidence to date has relied upon.
Transtibial prosthesis users who transitioned from non-MPFs to MPFs experienced a significant improvement in their physical function score as measured using the PROMIS-PF. The five-point improvement in the PROMIS-PF score far exceeded the recommended range (1.9-2.2) noted as a minimally important difference for improvement found in other sub-populations, 26 suggesting that the transition from a non-MPF to a MPF technology was not only statistically significant but also clinically meaningful. Upon detailed analysis, those items with the greatest improvements in physical function included items reflective of sit–to-stand transfers and stair negotiation followed by bending down to retrieve something from the floor. More modest benefits were also observed with level ground ambulation over sustained times and distances.
The benefits of MPF in stair ascent have been established in several laboratory based clinical trials. The Ossur Proprio MPF has been associated with increased dorsiflexion in stance, improving the positioning of the ipsilateral knee into relative stance flexion to maintain upward and forward momentum. 2 The latter adaptation yields a more even distribution of peak pressures in the socket such that pressure values associated with stair ascent with an MPF better approximate those observed in level ground walking. 10 These biomechanical observations, coupled with increased swing phase dorsiflexion reducing the risk of a stumble on the stair landing, may partially explain the observed improvements to the PROMIS questions, “Are you able to carry a laundry basket up a flight of stairs,” and “Are you able to go up and down stairs at a normal pace.”
The benefits of MPF relative to sit-to-stand transfers from either a low, soft couch or a toilet have not been previously reported. The added ankle dorsiflexion likely permits the users to bring their ipsilateral knee and body center of mass further anterior over their feet to execute such stand-to-sit and sit-to-stand transfers with easier mechanics. This same benefit would appear to assist the retrieval of a dropped item from the floor as the augmented stance dorsiflexion would allow the user to sustain their center of mass over a larger plantar surface area.
Improvements were observed but less pronounced with PROMIS questions related to sustained ambulation on level ground. This is consistent with the observations of Hahn et al with the Ottobock Meridium MPF where improvements were observed with greater frequency during complex gait tasks such as negotiating ramps and uneven terrains (82%-97%) than the more subdued task of level ground ambulation (54%). 27 Delussi et al observed significant reductions in the measured energy costs of ambulation after 90°days with the Proprio MPF. 9 Reductions in energy cost may partially explain the mean improvements associated with the questions related to sustained ambulation of at least 15 min in duration, or a block (100 m) in length.
With respect to the items taken from the PEQ, the constructs associated with the greatest improvement were the navigation of steep hills. Significant improvements were also observed with respect to socket comfort. Both of these are in alignment with the PROMIS-PF findings related to stair ascent and descent, movements that require the ankle joint to operate in a different range to dissipate excessive forces rather than translating to the limb-socket interface and proximal joint structures.
The improved ability to walk both up a steep hill and down a steep hill with an MPF may be tied to the biomechanics of the MPF. Specifically, the biomechanics of MPF during ramp negotiation have been studied extensively. During ramp ascent, the additional stance phase dorsiflexion of the Ossur Proprio MPF reduces the knee hyperextension associated with non-articulating feet, leading to a more favorable knee position to maintain momentum forward and up. 3 In addition, minimum toe clearance values increase 53%-100% in swing phase with the greatest increases associated with increased walking velocities. 4 During ramp descent, the additional ankle plantarflexion reduces the flexion moment acting upon the ipsilateral knee, increasing the perceived safety associated with that ambulation environment. 3 With the Blatchford Elan MPF, ramp descent is associated with a relatively quick foot flat followed by a more measured forward shank rotation, reducing the flexion moment acting upon the knee and affording a controlled forward shank progression. 5 Increased minimum toe clearance values have been observed with the Endolite Elan MPF during both ramp ascent and descent. 6 The Proteor Kinnex MPF has been associated with improved socket comfort scores in both standing and walking on both inclined and declined slopes. 7 These cumulative, largely laboratory-based findings may begin to explain why our subjects reported significant reductions in difficulty with their ability to walk both up a steep hill and down a steep hill with their MPF.
Another interesting finding is the improvement in assessment of fit of the prosthesis. All subjects maintained their same socket during the transition to their MPF, yet they reported a significant improvement in their assessment of the fit of their prosthesis once they walked with their MPF. This may be due to a reduction in localized socket pressures described above during slope and stair negotiation and further reported with hydraulic ankle-feet during level ground ambulation. 28 Subjects also reported significant improvement in sitting comfort. This may reflect the ability of MPF options to yield into both dorsiflexion and plantarflexion to accommodate a range of knee angles with an associated reduction in localized force couples within the socket. While seven of twenty subjects reported a mean decrease in residual limb pain compared to only four reporting a mean increase in limb pain, the mean improvement of the cohort failed to reach statistical significance. This may suggest that socket discomfort is not always perceived as intense residual limb pain.
Somewhat surprisingly, improvements related to pain intensity were less pronounced and failed to reach statistical significance. Statistical improvements were, however, noted with respect to sitting comfort. This may suggest that there is increased discomfort with non-MPF, but it does not cross into the threshold of being considered painful. Counter to our hypothesis, the transition to the use of heavier MPFs was not perceived as increasing the weight of the prostheses. Rather, the weight of the device with the MPF was viewed more favorably than that associated with the legacy foot, though this difference failed to reach significance. This trend in reduced perceived weight may reflect increased minimum toe clearance values associated with MPF 4 and the decreased need for compensatory gait mechanisms to achieve adequate swing phase clearance in the presence of augmented swing phase dorsiflexion. Our findings conflict with the reports of Kaluf et al where subjects identified the increased weight of the Proteor Kinnex MPF as one of their primary “dislikes” relative to the non-MPF. 7 However, it should be noted that the most commonly utilized MPF in our sample, the Elan, weighs 20% less than the Proteor Kinnex.
The significant improvement in back pain intensity associated with the transition to an MPF was not anticipated. The biomechanical rationale for this observation is unclear, but may be related to the improved swing phase clearance associated with MPFs and a reduced need to utilize compensatory gait strategies at the hips and low back. This apparent relationship between MPFs and low back pain warrants further investigation and research.
There are a number of limitations associated with this research. While patient-reported feedback was collected from users of four commonly utilized and commercially available MPFs, the sample sizes were insufficient to draw meaningful conclusions related to the comparative effectiveness of different MPF models, and therefore further sub-analysis comparing groups were not performed. Future work should consider exploring the impact of MPF models on patient outcomes. As a retrospective analysis of clinical data, it is challenging to control the quality of alignment or settings of the MPFs used in this study. Rather, this study represents an analysis of patient reported outcomes in an ecologically representative sample of patients receiving care from a number of different clinicians across the United States. Notably, all clinicians are required to take a minimum level of continuing education to maintain their status, as well as targeted courses for providing the care associated with these MPFs. While refinements in alignment and settings may have led to additional improvements in certain metrics, our findings represent the realities of the alignments and settings observed in a cross-sectional analysis of patient fittings as they occurred in traditional patient care environments rather than controlled laboratory settings. Subsequently, stronger benefits may be possible with enhanced clinician training.
Another limitation to this study is that the domains of pain, stair ascent and decent were measured using single-item questions extracted from the PEQ in an approach that has not been validated. Nevertheless, the intention of our secondary aim was to provide a preliminary assessment of the impact of MPF to improve back pain. Future studies should explore this relationship using standardized, validated instruments that may be able to reinforce the current findings. Finally, while patients are known to occasionally reject new components, our retrospective screening efforts did not identify any individuals who rejected their MPF at delivery. This may represent a possible sampling bias within our retrospective screening methodology.
Conclusion
This study supports previous findings conducted in controlled laboratory walking environments showing benefits associated with microprocessor feet (MPFs). These known benefits include: improved biomechanical performance during the negotiation of ramps and stairs, increased toe clearance in swing, reduced peak pressures against the residual limb within the socket and increased prosthetic mobility. Additionally, this study demonstrates how MPFs interact outside of the laboratory when the only prosthetic variable was the transition from non-MPF to MPF. Transtibial prosthesis users who transitioned from non-MPFs to MPFs experienced a significant improvement in their physical function score as measured by the PROMIS-PF. In addition, back pain, residual limb pain, and hill ascent and descent showed improved scores from the independent items taken from the PEQ. Observations from this study can inform clinical decision making surrounding known clinical benefits of MPF technology.
Footnotes
Contributorship
PS and EW design and conceived the study. PS conducted the literature review and wrote the first draft. DE and SW were involved in gaining ethical approval and data analysis. DE and VS were involved in data reduction. All authors critically revised, edited, and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
PS.