
Abstract
Introduction
Parkinsonian tremor has severely impacted the lives of 65% of individuals with Parkinson’s disease, and nearly 25% do not respond to traditional treatments. Although wearable tremor suppression devices (WTSDs) have become a promising alternative approach, this technology is still in the early stages of development, and no studies have reported the stakeholders’ opinions on this technology and their desired design requirements.
Methods
An online survey was distributed to affected Canadians and Canadian movement disorder specialists (MDS) to acquire information on demographics, the current state of treatments, opinions on the WTSDs, and the desired design requirements of future WTSDs.
Results
A total of 101 affected individuals and 24 MDS completed the survey. It was found that both groups are generally open to using WTSDs to manage tremor. The most important design requirement to end users is the adaptability to lifestyle, followed by weight and size, accurate motion, comfort, safety, quick response, and cost. Lastly, most of the participants (65%) think that the device should cost under $500.
Conclusions
The findings from this study can be used as guidelines for the development of future WTSDs, such that the future generations could be evaluated and accepted by the end users.
Keywords
Introduction
Parkinson’s disease (PD) is a progressive neurological disorder that affects 1 in 500 people in Canada. Currently, nearly 100,000 Canadians are living with PD. 1 As the population in Canada grows and ages, it is predicted that the overall number will double in the next 20 years.2,3 The progressive and chronic nature of PD leads to a substantial economic burden on individual patients and the health care systems.4,5 It is estimated that the economic burden of PD in Canada is more than $1.2 B in direct and indirect costs associated with the disease. 3 Tremor is one of the most disabling symptoms of PD, and affects about 65% of people living with PD. 6 The existence of tremor can result in individuals experiencing limitations of physical functions, emotional stress, and social isolation, which may significantly compromise their quality of life. 7
Medication and brain surgery are the mainstays of treatment for parkinsonian tremor.8,9 However, it has been reported that medication provides a suboptimal benefit to 25% of the individuals living with parkinsonian tremor. Furthermore, medication often presents side effects and issues with drug tolerance.
10
Although brain surgery is often very effective in managing tremor, it carries a risk of significant complications for the individual,
11
and is only considered for those individuals with advanced PD (less than 2% of the PD population
12
). As an alternative, research in wearable tremor suppression devices (WTSD, Figure 1) has been facilitated by the development of wearable technology. A wearable tremor suppression glove developed in.
13
It suppresses tremor in the index finger, the thumb, and the wrist using mechanical loading.
For the past two decades, many WTSDs have been developed and validated. These devices suppress tremor by applying external controllable stimulations on the target joint(s) or the muscles that actuate the target joint(s), such as mechanical loading13–27 and electrical stimulation.28–39 The validation of these devices has proven their feasibility for suppressing tremor, with reported tremor suppression ratios ranging from 40% to 95.2%. 40 Although these technologies have shown promising results, none of these WTSDs have become commercially available. Furthermore, very few of them have even been evaluated in the clinic. Other than the hurdles presented in the commercialization process, the lack of acceptance by the stakeholders may be caused by several factors, such as size, weight, discomfort, safety, cost, performance when suppressing tremor, adaptability to the user’s lifestyle, or inadequate knowledge of this technology among the stakeholders. Whether these factors contribute to the lack of acceptance of WTSDs is an important question to be answered; however, no existing studies have responded to this question. Hence, in order to facilitate the acceptance of WTSDs by clinicians and individuals with PD, it is imperative to understand why the current WTSDs are not widely used, and what aspects of a WTSD are considered to be the most important to the stakeholders.
In view of the identified gaps in the field of wearable tremor suppression technology, the primary goal of this study was to survey individuals with PD and movement disorder specialists (MDS) to understand their opinions and expectations about WTSDs. The secondary goal was to obtain the user-centered design requirements for future WTSDs. The objectives of this study include the identification of the obstacles to the acceptance of the current WTSDs by the stakeholders, and the establishment of guidelines for future research in the development and evaluation of WTSDs.
The rest of the article is organized as follows: in Methods, the survey design, participant recruitment, and data analysis methods are described. Results presents the findings of the survey. The outcomes of the survey study are discussed in Discussion. The last section presents a summary of this study.
Methods
This paper presents findings from an analysis of quantitative data collected from an online survey of people with PD and MDS in Canada, exploring the current state of parkinsonian tremor management in Canada, the stakeholders’ opinions on the tremor management approaches and WTSDs, and the desired design requirements of future WTSDs. The survey was developed based on the guidelines for the design of questionnaires for survey research. 41 The presentation of this paper follows the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 42 The study protocol was approved by the University of Western Ontario’s Human Research Ethics Board (Protocol no. 112194, approved on March 19, 2020).
Survey Design
The online survey was developed and conducted using Qualtrics XM. It contains two self-administered questionnaires (See Appendix) that include a mixture of open ended and multiple–choice questions. The questionnaire for the MDS participants includes a total of 13 questions, two of which were open ended, and 11 were multiple choice questions, asking the participants to provide information about their experience when treating parkinsonian tremor and their opinions on the use of a WTSD. The questionnaire for the participants with PD includes a total of 17 questions, one of which was an open ended question, and 16 were multiple–choice questions, asking the participants to provide their demographic information (including age, sex, years since PD diagnosis), received treatments, and their opinions on the treatments and WTSDs. The participants from both groups were also asked to rank the aspects of a WTSD they consider important. Prior to opening the survey, preliminary runs were conducted by one person with PD, one movement disorders specialist, and four research collaborators to detect flaws, ambiguity, and missing questions/answers of interest.
Recruitment and data collection
People who were diagnosed with PD and capable of completing an online survey were invited to participate in the study from April 2020 to March 2021. As there is no national database of individuals with PD, a Google search was performed to identify the Parkinson’s societies, associations, and support groups in each province. The coordinator of each identified organization was contacted via email for distribution of the survey. Upon completing the screening of the study by each organization, the survey was sent out to individuals with PD via weekly newsletter and was posted on the webpage of each organization. Both the newsletter and the online poster contained a link to the survey, where a letter of information and a consent form were displayed before the questionnaire. Note that no description of WTSDs was given to the participants before they participated in this survey. The participants with PD were not administered any cognitive tests since these tests must be conducted in person. By continuing to the questionnaire, the participant agreed to give consent to enroll; and by navigating and completing the questionnaire, it was considered that the participants with PD were able to answer the questions.
In addition to the participants with PD, MDS with a practice focus on PD were invited to participate in the study from August 2020 to May 2021. The contact information of MDS was identified on the Canadian Movement Disorder Group, as it has a public internet database of MDS in Canada, which can be searched by area of practice. A total of 61 MDS with a PD focus to their practice were identified for recruitment. Recruitment was conducted through direct email invitation. A total of six reminder emails were sent out after the initial contact. Each email contained a link to the survey, where a letter of information and a consent form were displayed before the questionnaire. By continuing to the questionnaire, the participant agreed to give consent to enroll.
Participation in this study was completely voluntary. The participants from both groups were not offered any incentives to complete the questionnaire. Since the recruitment of people with PD relied on the distribution of the survey by each Parkinson’s association, the survey response rate could not be calculated traditionally based on the number of invitations and respondents. As an alternative, the completion rate was used for the participants with PD, i.e., the ratio of users who finished the survey versus users who completed the consent page. As for the MDS respondents, the response rate was calculated as the ratio of the number of responses versus the number of invitations. Lastly, an IP check was enabled in the survey to prevent duplicate entries by the same user.
Data analysis
The survey responses were analyzed using the IBM Statistical Package for Social Science (SPSS version 24) statistics software. Descriptive statistics and frequency counts were used to present the obtained data, and cross-tabulation analysis was used to examine potential associations between different variables. Since these variables are ordinal data, the Gamma test was used for the cross-tabulation analysis between the independent variables and the response variables, and the Somers’ Delta test was used for the explanatory variables and the response variables. As for the numerical ranking questions, Friedman’s ANOVA test was used to assess whether the ranking result rejects the null hypothesis of equal mean ranks. Furthermore, Kendall’s W test was used to quantify the agreement among the respondents on these ranking questions. The α was set to 0.05, and an 80% power was used.
Results
In this section, the results obtained from the respondents with PD are reported in the first subsection. The second subsection presents the results obtained from the MDS respondents.
Respondents with PD
Demographics and opinions on received treatments
Demographics of the respondents with PD.
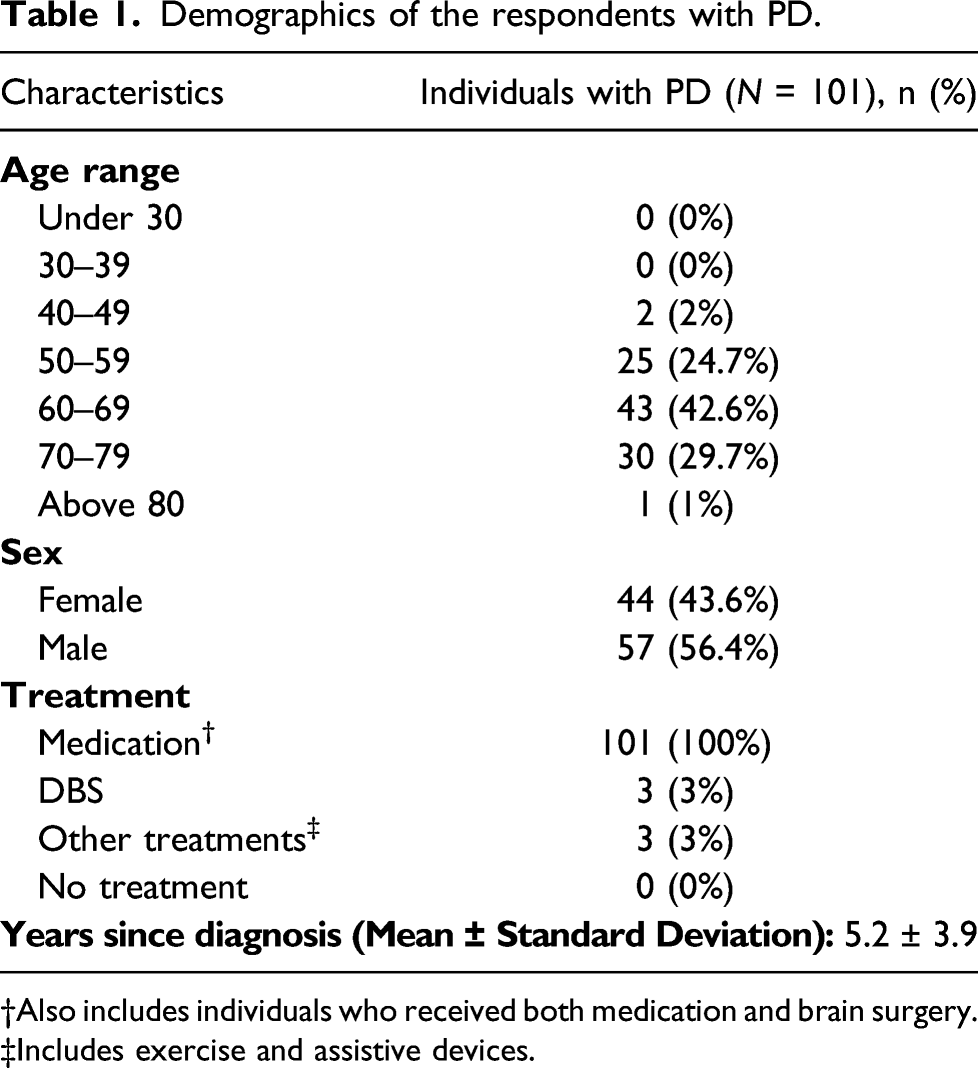
Also includes individuals who received both medication and brain surgery.
Includes exercise and assistive devices.
Opinions of the individuals with PD on the received treatments.

Also includes the individuals who received both medication and brain surgery.
Lastly, among the three respondents who have undergone brain surgery, 2 (66.7%) are not satisfied with the improvement of their symptoms, 2 (66.7%) had complications due to surgery, and 1 (33.3%) has difficulty with the maintenance of the DBS device.
Knowledge and opinions on WTSDs
Knowledge and opinions of the individuals with PD on WTSDs.

p < .05, Kendall’s W = .576.
In general, personal opinions are directly affected by knowledge of the examined subject. In this study, it was found that most of the respondents have little knowledge of WTSDs; however, their opinions on the concept of a WTSD are mostly positive (68.3%, 69/101). 29 (28.7%) felt uncertain about the concept of using WTSD to treat parkinsonian tremor and only 3 (3%) felt that the WTSDs would not improve upon their current treatment. Although the respondents’ opinions on the concept of WTSD are generally positive, less enthusiasm was found among the respondents when they were asked about trying a WTSD. Only 47 (46.5%) rated strongly in favor of trying a WTSD, 40 (39.6%) would have to see the design first, 10 (9.9%) are either not interested or are happy with their current treatment, and 4 (4%) did not answer this question.
Lastly, the respondents reported that medication is their most favored treatment, followed by WTSD, and brain surgery (DBS). The Kendall’s W test on the ranking results found a high variability (37.9%, i.e., Kendall’s W = 0.621) on the ranking, indicating that not every respondent agreed on the answer; however, the Friedman’s ANOVA test rejected the null hypothesis of equal mean ranks (p < .05), which indicates that a statistically-significant similarity in the ranking answers was found to represent the opinion of the group.
Influencing factors of the opinions on WTSDs
Figure 2 shows the influence of nine factors, which include three independent variables and six explanatory variables, on the participants’ opinions about WTSDs, including two response variables. The quantified influence of the nine factors on the two response variables is divided into two columns (Figure 2(a)). The subplots in the left column present the influence of the nine factors on the participants’ opinions about the concept of WTSDs in general, and the subplots in the right column present the influence of the nine factors on the participants’ opinions on trying a WTSD. Influence of nine factors on the opinions of the individuals with PD on WTSDs. a. Each row presents the quantified influence of each factor on the participants’ opinions on the concept of WTSDs (Left) and the opinions on trying a WTSD (Right). The first row represents the factor age, followed by the year since diagnosis, sex, their awareness of WTSDs, the overall satisfaction with their current treatment, the Effectiveness of their current treatment on managing tremor, the difficulty of managing treatment in daily life, the side effects of their current treatment, and the cost of their current treatment. The y axis of each bar graph shows the frequency count, and the x axis shows the options of each independent/explanatory variable. The numbers above each set of bar graphs present the percentage distribution of the answers. The factors that statistically associate (p 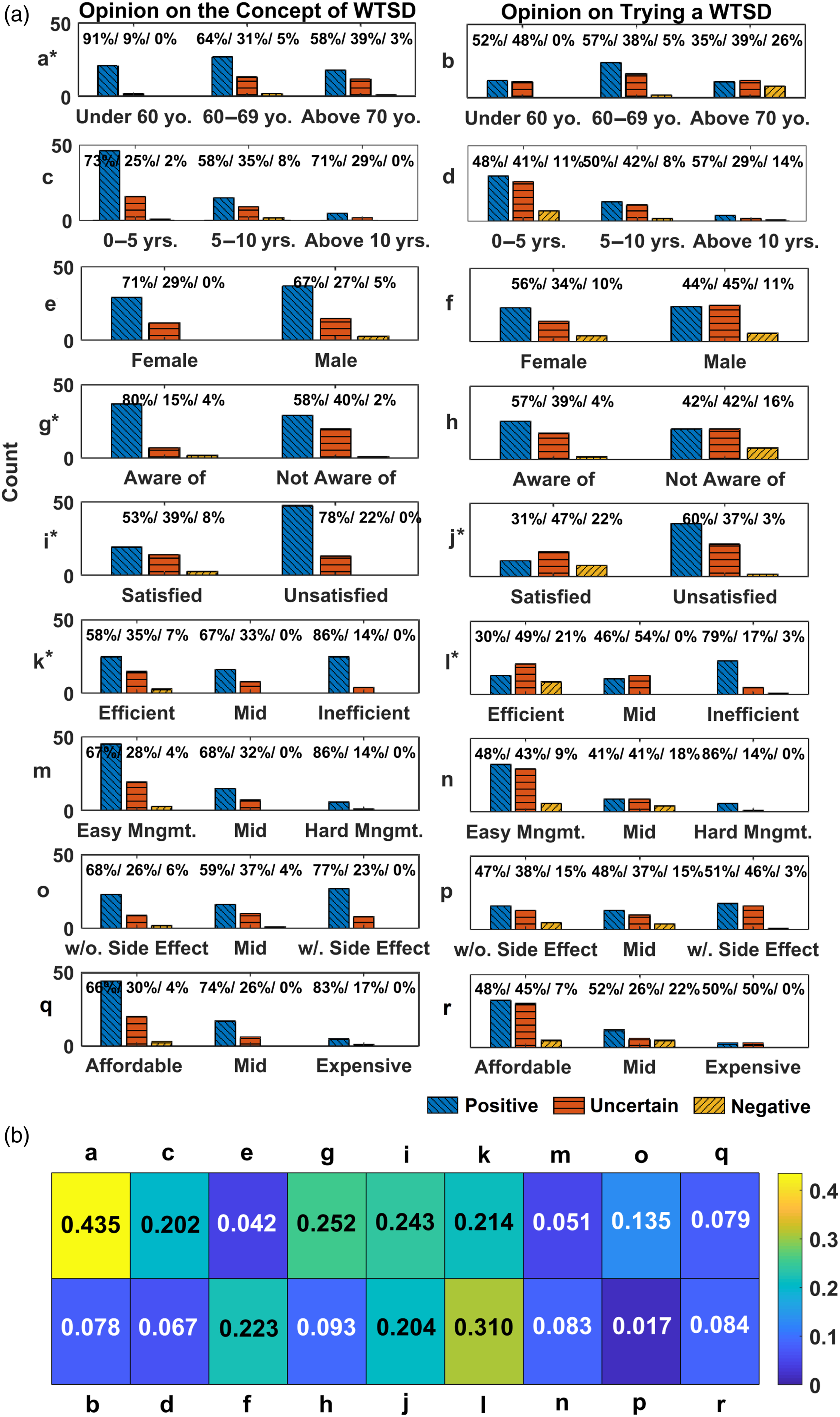
The independent variables are age (a and b), year since diagnosis (c and d), and sex (e and f). Note that the number of the respondents under the age of 50 and above the age of 80 accounts for only 3% (3/101) of the entire cohort. The respondents under the age of 50 and those between 50 and 59 years old were grouped together, i.e., age under 60, for cross-tabulation analysis. Similarly, an age group above 70 years old was created by combining the respondents from the age group between 70 and 79 years, and above 80 years. The explanatory variables include their awareness of WTSDs (g and h), the overall satisfaction of the treatment they currently receive (i and j), the Effectiveness of their current treatment on managing tremor (k and l), the difficulty of managing treatment in daily life (m and n), the side effects of their current treatment (o and p), and the cost of their current treatment (q and r). Note that the year since diagnosis was categorized into three groups based on a time range of five years,43,44 i.e., 0–5 years, 5–10 years, and above 10 years; the overall satisfaction of the treatment was categorized into two groups, i.e., satisfied and unsatisfied. A respondent was placed into the satisfied group only when none of the four aspects of the treatments were rated as negative. The descriptive statistics are shown by the bar graphs (Figure 2(a)), and the statistical association between each influencing factor and each response variable is shown by the color map in Figure 2(b).
The y axis of each bar graph in Figure 2(a) shows the frequency count, and the x axis shows the options of each independent/explanatory variable. Note that each option on the x axis contains three bars that indicate the answers, i.e., positive (left), uncertain (mid), and negative (right), of the response variables, and each answer/bar is marked by a different hatching pattern. The numbers above each set of bar graphs present the percentage distribution of the answers. Lastly, the numbers in Figure 2(b) present the strength of the statistical association, either Gamma value or Somers’ D value, between the independent/explanatory variable and the response variable. The color scheme is shown in the color bar, ranging from dark blue (no association) to yellow (strong association). It was found that the respondents’ age has a strong association (γ = .44) with their opinions on the concept of WTSD; their year since diagnosis (γ = .20), the awareness of WTSDs (γ = .25), the Effectiveness of their current treatment on managing tremor (γ = −0.21), the side effects of their current treatment (γ = .14), and the overall satisfaction of the treatment (γ = −0.24) have a moderate association with their opinions on the concept of WTSD; the Effectiveness of their current treatment on managing tremor has a strong association (γ = −0.31) with their opinions on trying a WTSD; the sex of the respondents (γ = .22) and overall satisfaction of the treatment (γ = −0.20) have a moderate association with their opinions on trying a WTSD; and lastly, the rest of the cross-tabulation analysis showed weak association (γ within ±.09).
Other than the strength of statistical association, it was found that the respondents’ age influences their opinions on the concept of WTSDs (p < .05). The younger age group has more positive views on the concept of WTSD when compared to the older age group; however, such association was not found between their age and their opinions on trying a WTSD (p = .60). Similarly, their awareness of WTSDs led to a positive opinion on the concept of WTSD (p < .05); however, no such association was found between their awareness of WTSD and their opinions on trying a WTSD (p = .34).
In addition to the aforementioned factors, it was found that the respondents’ satisfaction with the treatment they are receiving also plays a significant role in their opinions on the concept of WTSD (p < .05) and on trying a WTSD (p < .05). The respondents who are unsatisfied with their current treatments are generally more favorable to the concept of a WTSD and on trying a WTSD, while the other respondents are either uncertain or negative about this technology.
Among the four aspects of the treatments, only the Effectiveness of the treatments on managing tremor has significant associations with the respondents’ opinions on WTSD (p < .05 for both opinions). It showed that the respondents who are experiencing ineffective treatments are generally more open to the WTSD technology, while the others who are satisfied with the Effectiveness of the treatments are generally not interested at the moment.
Lastly, year since diagnosis, sex, cost of the treatment, side effects, and difficulty of managing treatment in daily life do not significantly associate with the respondents’ opinions on WTSD. The factors that statistically associate (p
Design requirements and affordability
Design requirements and affordability are the other primary outcomes examined. Figure 3(a) shows the respondent-reported significance of seven design aspects of a WTSD. They are accurate motion, weight and size, cost, comfort, safety, quick response, and adaptability to lifestyle. All seven aspects were ranked in order from the lowest significance (1) to the highest significance (7). The x axis shows the stacked frequency count of the significant levels. The “Neutral” levels of all design aspects are centered at 0. The Kendall’s W test on the ranking results found a high variability (77.9%, i.e., Kendall’s W = .221) on the ranking, indicating that not every respondent agreed on the answers; however, the Friedman’s ANOVA test rejected the null hypothesis of equal mean ranks (p < .05), which indicates that a statistically-significant similarity in the ranking answers was found to represent the opinion of the group. Therefore, based on the averaged quantified ratings, i.e., the lowest significance has a value of one and the highest significance has a value of seven, the most important design requirement is the adaptability to lifestyle (4.30), followed by weight and size (3.79), accurate motion (3.76), comfort (3.26), safety (2.48), quick response (1.99), and cost (1.43). a. Seven design requirements ranked by the respondents with PD. b. Distribution of the acceptable price of a WTSD.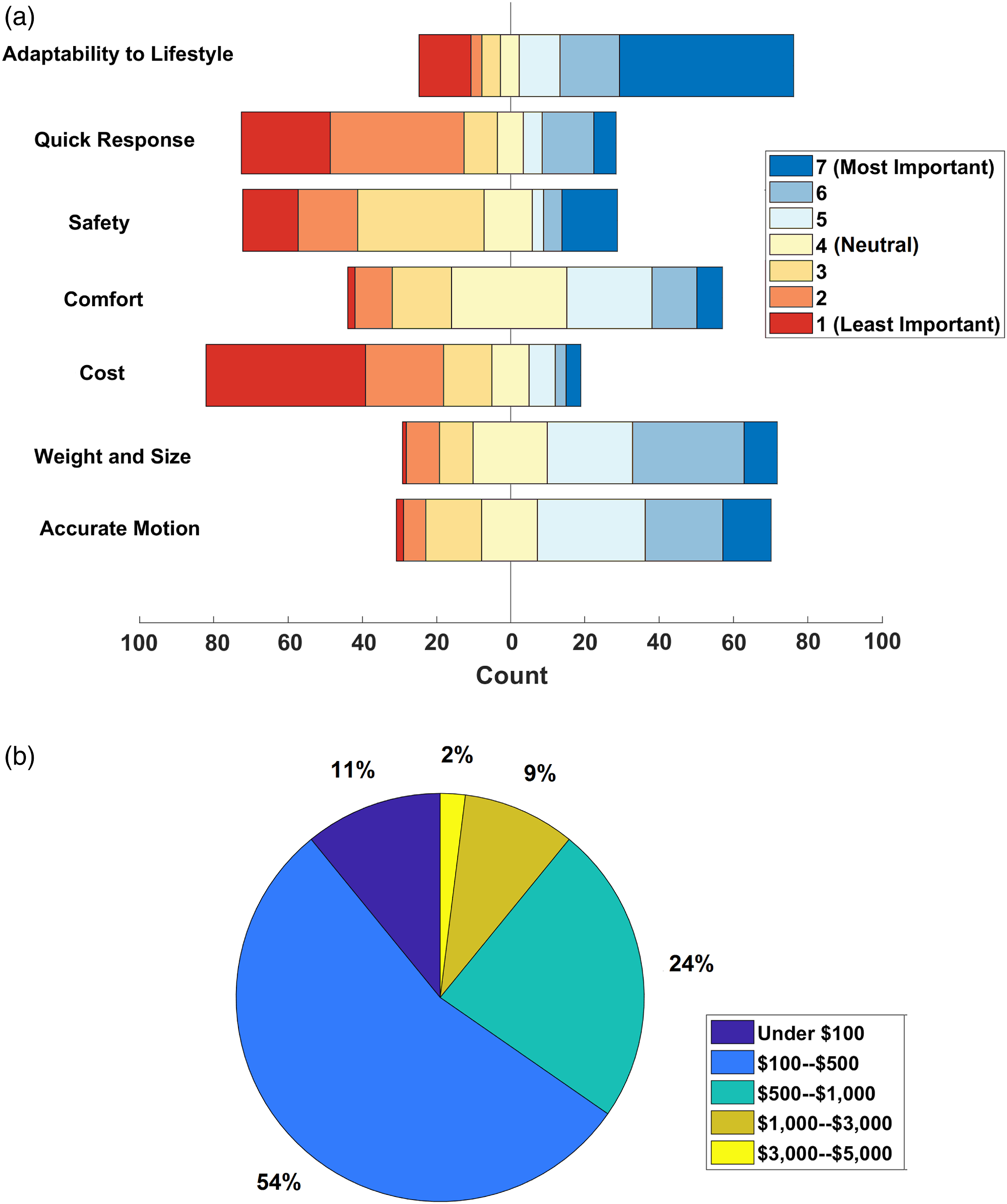
Figure 3(b) shows the maximum acceptable price range of a WTSD reported by the respondents with PD. The percentage of respondents who would spend under $100, $100–$500, $500–$1,000, $1000–$3,000, and $3000–$5000 are 11%, 54%, 24%, 9%, and 2%, respectively.
MDS Respondents
Demographics
Demographics of the movement disorder specialists.

Knowledge and opinions on WTSD technology
Similar to the respondents with PD, the knowledge and opinions of the MDS on WTSD technology are among primary outcomes examined for the MDS respondents. It was found that most of the MDS (23, 95.8%) were aware of the existence of WTSD technology, only 1 (4.2%) reported that they were not aware of such technology. Among the MDS who are aware of WTSD technology, 1 (4.2%) has tried WTSDs on patients, 3 (12.5%) have participated in a WTSD-related research study, and 19 (79.2%) have heard of the concept. Among the 23 MDS who are aware of the WTSD technology, 4 (16.7%) obtained the knowledge from their patients, 5 (20.8%) from their co-workers, 14 (58.3%) from literature, 8 (33.3%) from news, 1 (4.2%) from industry contacts, and 1 (4.2%) from an international conference.
Based on their knowledge of WTSDs, all MDS respondents believed that WTSDs are not widely used. Among the ones who did not believe that WTSDs are widely used, 11 (45.8%) considered that the size and weight of WTSDs restricted their adoption among the end users, 12 (50%) indicated the prohibitive cost of WTSDs, 9 (37.5%) indicated the lack of ergonomic designs, 5 (20.8%) indicated that the design was too complex, 4 (16.7%) indicated that they were ineffective in managing tremor, and 22 (91.7%) indicated inadequate knowledge of the WTSDs among professionals. The distribution of each opinion is shown in Figure 4(a). a. MDS rated drawbacks of the current WTSDs that have restricted the acceptance by end users. b. The influence of the MDS' opinion on whether they will recommend WTSDs to their patients (left) and whether they will participate in WTSD-related studies (right). The y axis of each bar graph shows the frequency count, and the x axis shows the options of each independent/explanatory variable, i.e., Positive, Neutral, and Negative. The numbers above each set of bar graphs present the percentage distribution of the answers. Statistically‑significant associations (p 
Lastly, the influence of the MDS' opinion on whether they will recommend WTSDs (when they become available in the market) to their patients and whether they will participate in WTSD-related studies is shown in Figure 4(b). The MDS' opinion on WTSD technology is the independent variable (x axis) with three categories, i.e., Positive, Neutral, and Negative; their attitude towards recommending WTSD to patients and participating in WTSD-related studies are the dependent variables, which consist of three categories, i.e., Yes (left), Uncertain (mid), and No (right). Each of these categories is marked by a different hatching pattern. The descriptive statistics are shown by the bar graphs. Strong associations were found between the MDS' opinions on WTSD technology and the two dependent variables, i.e., the MDS' opinion on whether they will recommend WTSDs (when they become available in the market) to their patients (γ = .48) and whether they will participate in WTSD-related studies (γ = .51). The numbers above each set of bar graphs present the percentage distribution of the answers.
It was found that MDS' opinion significantly influences their decisions (both p < .05) on the acceptance of WTSD technology. The MDS with negative opinions on the WTSD technology are more skeptical about recommending WTSDs to their patients and participating in WTSD-related studies, while the MDS with positive opinions on the WTSD technology are more willing to accept the technology.
Design requirements
In addition to the knowledge and the opinions of the MDS regarding WTSD technology, the design requirements of a WTSD were the other primary outcomes examined for the MDS respondents. Figure 5 shows the MDS-reported significance of seven design aspects of a WTSD. They are the same as the ones presented to the respondents with PD. The Friedman’s ANOVA test found no significant difference (p = .645) between the obtained rankings from the MDS and the equal mean ranks. The Kendall’s W test on the ranking results showed a 97.1% (Kendall’s W = 0.029) variability. Although no agreement on the rank of the seven design aspects of a WTSD was obtained, the following ranking is presented herein as a descriptive result without statistical significance. Based on the average ratings, the safety has the highest importance (4.50), followed by accurate motion (4.33), quick response (4.29), adaptability to lifestyle (3.92), weight and size (3.67), comfort (3.71), and cost (3.58). Seven design requirements ranked by the movement disorder specialists respondents.
Discussion
This study is part of a larger project that aims to develop a user-centered WTSD for individuals whose tremors are not effectively managed by traditional treatments. Although many WTSDs have already been developed, none of them have become commercially available and used by people living with parkinsonian tremor. This study aimed to understand better the stakeholders’ opinions on WTSD technology and their requirements for such a device. Findings from this study will provide essential guidance for developing future WTSDs that are more acceptable by the end users, and facilitate the transition of WTSDs from the lab to end users.
Current state and opinions on traditional treatments and WTSDs
The demographics of the individuals with PD have shown that the majority of the respondents received medication to manage their tremor. A small group received other treatments, i.e., DBS and exercise; however, none of them have been using a WTSD to manage their tremor. This finding supports the hypothesis that the technology of tremor suppression devices has not been developed to the level that it can be accepted by the end users. In addition, this hypothesis is also supported by the responses from the MDS; namely, that the main treatments that they have been prescribing to the patients are medication and brain surgery (Table 4).
As one of the nine factors, age has shown a strong association with the opinion of parkinsonian participants on WTSDs. It was found that older participants are generally not optimistic about this technology. Although the reasons for this result were not explicit in the current study, it is essential to identify these factors in a follow-up study so that future WTSDs can be designed to be more inclusive for end users from different age groups.
The technology of WTSD has been developed for a couple of decades; however, most of the WTSDs are still being evaluated in the lab. The drawbacks of the existing WTSDs have certainly played a role in restricting their acceptance by the end users; however, a major finding was identified in this survey that more than half of the respondents with PD (52.5%, Table 3) were not aware of any WTSDs. Due to this unawareness, the end users may not have used or inquired about such technology. In addition, meaningful engagement between the researchers and the end users may not have been established due to the unawareness of any WTSDs, leading to the aspects of a WTSD that the end users value the most not being properly considered in the design process. Furthermore, it was found that only 2% (Table 3) of the respondents with PD have heard the concept of WTSDs from their primary doctors; however, this does not indicate that their primary doctors are not aware of the technology. In fact, most of the MDS respondents (95.8%) know of the existence of the technology, and 16.7% have tried a WTSD or participated in a related research study. Although the MDS are aware of the technology, most of them (91.7%, Figure 4(a)) believe that there is not enough knowledge of the WTSDs among the professionals, which may explain their unwillingness to inform their patients about this technology.
Although there is a lack of knowledge about WTSD technology among the stakeholders, the survey found that most of the end users (68.3%, Table 3) have positive opinions on the concept of WTSDs. In addition, the cross-tabulation analysis showed that people who are aware of the technology have more positive opinions than those who are not aware. This indicates that higher exposure of the technology to the end users likely will facilitate its acceptance. Interestingly, no statistical association was identified between the awareness of the technology and end users’ opinion on trying a WTSD. This is likely because only a small group of individuals (3%, Table 3) had the experience of using a WTSD. This finding also aligns with the current state of development of WTSDs in the literature, in which only a few WTSDs 45 have been preliminarily tested on a small group of people in the world.
In addition to the awareness of the technology, the cross-tabulation analysis found a statistically‑significant association between the end users’ experience on their current treatment and their opinions on the concept of WTSD and opinion on trying a WTSD. The end users show more enthusiasm towards the WTSD, as an alternative treatment approach, when they have experienced difficulties with their current treatments. However, not every surveyed aspect of the received treatment contributed equally to this outcome. It was found that, among the four surveyed aspects, only the Effectiveness of the treatments showed a significant association with the end users’ opinions on the WTSD, and the rest presented only weak associations. Therefore, it is sufficient to conclude that the low Effectiveness of the current treatments is the leading factor that encourages the end users to find alternative treatments.
All MDS participants have confirmed that it is important to treat tremor. The level of treatment certainly varies by the severity of each individual’s tremor; however, the reported MDS' opinion on treating tremor may provide some indirect evidence regarding the ineffectiveness of the current treatment for managing tremor. The ineffectiveness of the current treatments for managing tremor and the awareness of the WTSDs have encouraged the end users to accept WTSDs; however, the opinions of the MDS on WTSDs also played a crucial role in the acceptance of this technology. It was found that the MDS who do not have a positive opinion on WTSDs are more skeptical about recommending the technology to their patients. Therefore, getting more MDS involved in developing and evaluating WTSDs may provide them with a better understanding of the technology, hence encouraging them to recommend the technology to their patients.
Both individuals with PD and health professionals certainly are essential stakeholders in determining the acceptance of WTSD technology; however, the family caregivers, especially those supporting the elderly with PD, also play an essential role in adoption. Therefore, other than their opinions on this technology and desired functionality, the social impact of this technology on the caregivers’ life, such as employment, mental health, and family relationship, should be investigated. The current study has surveyed both MDS and individuals with PD; however, a comprehensive follow-up study that includes caregivers should be carried out.
In this study, several aspects related to the PD treatments were found to play significant roles in the parkinsonian participants’ opinions on WTSDs; however, an interesting aspect of PD treatments that was not studied is the doses of daily medication taken. This factor could provide further insights into the participants’ opinions on WTSDs, which should be addressed in a follow-up study.
Design requirements and constraints for future WTSDs
The ultimate goal of WTSDs is to provide an alternative tremor management approach to individuals living with tremor. In order to promote the acceptance of WTSDs by end users, it is essential to understand which aspects they value the most. The survey showed that the three most important aspects are the adaptability to lifestyle, the weight and size of a WTSD, and accurate motion. From the design perspective, future WTSDs should include the following features: 1. Mechanism that allows easy donning and doffing process. 2. Unobtrusive and compact hardware design that does not hinder upper-limb motion. 3. Distributed actuation and transmission system that is remotely located from the hand. 4. Light weight. Note that the maximum acceptable weight was not surveyed as part of this study. A recent study assessed a WTSD on an individual with PD reported that a weight of 580 g is acceptable.
13
5. An optimal control system that considers the dynamic model of the WTSD for accurate motion control.
In addition to the aforementioned aspects, it was surprising to find that safety was ranked in the lower half of importance by the respondents with PD. A potential reason could be the daily struggle with tremor has eroded the participants’ patience with the treatments that they are undergoing. Furthermore, as a disease with no cure, individuals with PD take action by involving themselves in more fundamental research initiatives. As a group, it is likely that they are more open to alternatives as it is an understood community effort to support finding new treatments. Hence, the strong demand for an alternative approach may outweigh the importance of safety. However, this does not suggest that safety should be considered as a lower priority than any other aspects. To ensure the safety of a WTSD, both software and hardware measures should be implemented in the design process of a WTSD; in addition, an emergency stop button should also be incorporated.
Unlike the ranking results from the end users, the MDS respondents considered that the safety of a WTSD is the most important aspect, followed by accurate motion and quick response. Noticeably, the MDS were more concerned about the functionality and safety aspects of a WTSD than its cost and ergonomic design, while the end users expressed the opposite. However, considering that no agreement was achieved among the MDS in this question, more MDS respondents are required in order to draw a robust conclusion about their opinions on the design requirements of a WTSD.
Limitations
Since there is no nationwide database of individuals with PD in Canada, the online questionnaire was first sent to the Parkinson’s associations and support groups in each province, which may have introduced a selection bias by the third party. In addition, the spread of COVID-19 has significantly impacted the recruitment process as most in-person activities have been canceled. This unfortunate situation has prolonged the time necessary to receive a proper number of respondents for data analysis.
Because of the inherent nature of the online survey, a self-selection bias may play a role in the obtained results. People who already know about the technology may be more likely to participate in the survey, and to be in favor of adopting the WTSD technology. In addition, people without regular access to the Internet, or who are not proficient with using a computer or a tablet, may not have had access to this survey. Future work is needed to collect the perceptions from this group of people. Lastly, whether individuals live at home or in an institution may also play a critical role in determining the functionality and acceptability of the WTSDs, which should be investigated in the future study. To facilitate the aforementioned follow-up studies and to investigate the issue of user acceptability more broadly and comprehensively, the “Matching Person and Technology” model 46 can be used.
The design requirements section asked the respondents to rank the importance of seven aspects of their imaginary WTSD. Since there were no conceptual graphics provided with this question, the answers obtained may be limited by the respondent’s imagination or their impressions of other types of wearable devices.
In addition, several questions developed in this survey used Likert scales with a limited number of points, which may not provide enough resolution to the answers.
Conclusions
This study has highlighted the current state of parkinsonian tremor management in Canada. The results have given insights into the opinions of individuals with PD and MDS on tremor management approaches and WTSDs. Furthermore, this study has gathered information on the desired design requirements of future WTSDs from the stakeholders.
Both groups of participants are generally open to the idea of using WTSDs for managing tremor; however, many respondents require more evidence of the successful implementation of WTSDs. This suggests that extensive clinical evaluations of the WTSDs should be conducted in order for them to be accepted by stakeholders; note that very few of the existing WTSDs have been tested on humans. The information on the design requirements can be used as a guideline for the development of future WTSDs and optimization of the existing WTSDs, such that future versions could potentially become available for end users to use in daily life.
Footnotes
Appendix
Acknowledgement
The authors would like to thank all of the participants for their time and support in data collection.
Author contributions
YZ researched literature, YZ, KGH, MEJ, SJG, MDN, and ALT conceived the study. YZ, MEJ, MDN, and ALT contributed to protocol development, and obtained research ethic approval. YZ and DB recruited MDS and participants with PD. YZ, SJG, MEJ, MDN, and ALT interpreted the data. YZ processed and analyzed the data and wrote the manuscript. All authors reviewed, edited, and approved the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Natural Sciences and Engineering Research Council (NSERC) of Canada and the Canadian Institutes of Health Research (CIHR) through a Collaborative Health Research Projects (CHRP) grant #396234; by the Canadian Foundation for Innovation (CFI), by the Ontario Research Fund (ORF); by the Ontario Ministry of Economic Development, Trade and Employment and the Ontario Ministry of Research and Innovation through the Early Researcher Award; and by the Peter C. Maurice Research Fellowship in Biomedical Engineering.
Guarantor
ALT