
Abstract
Introduction
Ankle sprain is a common injury that can have long-term sequelae resulting in pain, swelling and a reduction of physical activity participation. Previous research has shown a laterally deviated centre of pressure (COP) during running gait increases the risk of lateral ankle sprain. As a method of altering COP, electrical stimulation has been considered.
Method
A group of 14 healthy males were randomly allocated to case control groups which were single blinded. The intervention involved an 8-week training programme of functional electrical stimulation to the peroneal muscles during treadmill running, with a sham control group. Outcomes were COP position and star excursion balance test. Statistical analysis was through SPSS using a combination of MANOVA, T-tests and Wilcoxon signed rank
Results
There was a significant difference in the results post intervention at max pressure for intervention M = 0.7(±0.7) and control M = −6.0 (±4.6) conditions; t(6) = −2.9, p < 0.05
Conclusion
It has been demonstrated that FES can alter COP during max pressure in running gait after an 8-week training programme, although carry over effect appears limited and further testing is required.
Introduction
Ankle sprain is a common injury that can have long-term sequelae resulting in pain, swelling and a reduction of physical activity participation.1,2 There are approximately 5600 injuries a day in the UK, 3 each sprain in 2019, cost approximately £1497.40–2093.18 4 when adjusting for inflation based upon a 3% average inflation per year; 5 the price includes the cost of healthcare and sick leave. 4 It is known that there is a high incidence in sport particularly in indoor/court based games with 4.9 occurring per 1000 h played, making it the second most common injured joint after the knee. 2
Due to the high incidence of first time ankle sprains and re-injuries, a substantial amount of research is now focused on prevention. 6 A review by Dizon and Reyes indicated that bracing could reduce re-injury of ankle sprain by 69% 7 and Van der Wees et al found that exercise intervention therapy is effective at reducing re-injury risk after an acute sprain (RR 0.38) 8 though it is unclear what the effect of either of these interventions is on first time injuries. 6
When designing prevention strategies it is important to be aware of the risk factors and aetiology of the injury. For lateral ankle sprain injury the two commonly suggested aetiologies are, delayed peroneal muscle reaction time and incorrect foot positioning at landing. 9 Previous research shows a laterally deviated centre of pressure (COP) during running gait, increases the risk of lateral ankle sprain. 10 COP is the location where the total sum of the pressures are treated as a force through a single point, the location varies dependant on where the peak of the pressure occurs, 11 when the COP shifts laterally risk of ankle sprain is believed to increase. 10
Different types of electrical stimulation can be used for various purposes, such as rehabilitation and pain relief. 12 When used as pain relief such as during labour or for back pain, transcutaneous electrical nerve stimulation (TENS) is typically used. 10 Electrical stimulation applied to a motor nerve can bring about a contraction of the muscle, and when creating a functional movement this is known as functional electrical stimulation (FES). 12 FES has been used for a number of benefits including, but not limited to, providing function to both upper and lower limbs and assisting with the respiratory system (Ragnarsson, 2007). 13 As can been seen in articles such as that by Ragnarsson 13 and Rushton, 14 much of the work surrounding FES is focused on neurological conditions, such as spinal cord injury, and other issues causing neurological loss of function. As Santos and Liu the aim of this paper is to investigate how FES may have the potential to reduce ankle sprain risk by using FES in an alternative manner to which it has previously been used. 15
A study by Yoshida, Tanino and Suzuki involving 7 participants used TENs to stimulate the common peroneal nerve during a balance exercise. 16 The research identified that the length of the COP was significantly longer on the injured side compared to the non-injured side. The results shows the length of COP is significantly decreased post intervention of TENs, reducing ankle instability. 16 Those with ankle instability after an ankle sprain, have been found to have altered position sense, poorer postural function, and a slower reaction time when engaging peroneal muscles. 16 It is thought that when the length of COP is increased, it may be as a result of slower response from the peroneal’s, an element of functional instability. 16 These results suggest there may be scope to use some form of electrical stimulation as a training intervention. 16 A study assessed the effect of subsensory stimulation applied to the ankle muscles and ligaments during single leg stance; the study indicated that electrical stimulation may improve proprioception of those with ankle instability. 17 These studies are useful to learn from though very different in their methods, both focus on balance exercises whereas in our study gait retraining during running is used.16,17 They indicate that electrical stimulation could have an impact upon balance and proprioception, the current study is more focused on the potential to use stimulation as a method to retrain to correct the foot position and therefore potentially the proprioception of the ankle.16,17 Another study using electrical stimulation looked at the effect of foot position on the unloading reaction, it is noted that position of the foot has a significant impact upon the reaction to the stimulus and that a more supinated position, exhibits a greater reaction compared to a more neutral position, this may indicate that targeting those with a lateral COP may have a greater effect than those without. 15 Fong, Chu and Chan, 18 and Fong et al., 19 used myoelectric stimulation to stimulate the peroneal muscles to prevent an ankle sprain. It was found that myoelectric stimulation can prevent ankle sprain motion, therefore it may be possible to stimulate the peroneal muscles to avoid the ankle sprain motion before it occurs. This has therefore laid the preliminary ground work that could be applied to create a rehabilitation programme to avoid initial injury.
It is hypothesised training the lower limb using FES to stimulate the common peroneal nerve activating peroneal longus and brevis muscles would shift a laterally-deviated COP to the medial direction.
Method
A sample size calculation was based upon previous work by Yoshida, Tanino and Suzuki. 16 The study assessed the effect of electrical muscle stimulation to the peroneal muscles during a landing from a jump on COP length, the study reported the length of COP reduced from 627.0 ± 235.4 mm to 551.8 ± 172.1 mm. 16 This sample size calculation was based upon an a priori-power analysis using the statistical test comparing means between matched pairs power was set at 0.95 α = 0.05, the estimated required sample size was calculated to be 14. COP length was used as the primary outcome for the calculation as there were no studies directly comparable with our method, it was concluded that the method of this study and the length of COP was a good comparison as both are concerned with proprioceptive sense, neuromuscular control.
Plantar pressure data was processed in a similar method described in a previous study 21 to determine if a participant showed laterally or medially deviated plantar pressure at foot strike. The plantar pressure data from the 30 second running sessions were extracted and analysed and the mean value determined, the outputs from the software were the position and magnitude on an X/Y axis, which were produced over the complete time series of the experiment. The quantified values and locations of the COP were then categorised as lateral or medial by using the Y values only and splitting the foot in two using the width, as calculated by the measured distance between the 1st and 5th metatarsal. A line bisected the foot, with Medial points being taken as positive and lateral points negative. By taking a summation of the all these COP values during stance phase throughout the whole gait cycle, a participant is classified as either medial or lateral strikers by the overall value of the summation, e.g. positive as medial and negative as lateral with a cut-off point of zero; the number that is calculated is unit-less. The participants were then categorised into two groups, medial and lateral strikers, by this method. 12 participants showed results that indicated both medial and lateral COP whilst running these were removed as they did not display a clear COP position.
Analysis on both feet in foot and ankle research could generate spurious or false positive results; Menz, argues that when using studies, participants are identified as a single contributor to the study ie, n = 1. Though assessing components of an individual, such as feet or legs, the components can be counted as 2 per person ie, n = 2 and therefore analysed as 2 separate measures as opposed to 1. This can therefore significantly affect results, by analysing both feet the assumption of independence during statistical analysis has been violated. 22 In this study data from only the right foot was analysed, though insoles were placed in both shoes to ensure normal gait.
Prior to intervention participants were assessed using the SEBT (star excursion balance test).23,24 The SEBT is a dynamic balance test that requires strength, flexibility and proprioception, this was carried out pre and post intervention and followed the protocol as set out by Gribble and Hertel. 25 For the SEBT, firstly a star is drawn on the floor (see Figure 1). The participant stands on one foot (right leg) in the centre of the star, next they extend the opposite leg (left) as far forwards along the anterior line as possible without placing their foot down, the distance reached is recorded. The participant returns their leg to the centre before progressing to the next line in an anticlockwise manner, repeating the same method for each line, the participant must maintain their balance throughout without placing their foot down. This test is carried out 3 successful times with the furthest distance recorded for each line on each test. A test is deemed unsuccessful if the participant was to use too much support from the reaching leg, removed the foot front the centre of the star, or were unable to maintain their balance. If unsuccessful the trial would be discarded and the participant would start that round again to gain 3 full sets of data.

Star excursion balance test layout.
Stimulation to the limb was provided by an Odstock Medical limited (Salisbury, UK) functional stimulation Pace device. Five different levels of stimulation were applied throughout the testing, ranging from 20 to a maximum of 70 mA with a pulse width of 50%. The aim of this level of stimulation was to engage the muscles to gently evert the foot during running, not to cause a rapid and strong eversion to avoid an injury the levels were was based upon previous research.15,19 Stimulation was provided to the Peroneal nerve to stimulate the Peroneal muscles to bring about eversion of the foot. As can be seen in Figure 2, the typical mechanism on LAS is through a laterally deviated COP with a supinated foot position, or the foot rolling over the lateral edge leading a rapid torque injuring the lateral ligaments; COP is usually laterally deviated. Figure 2 indicates how the aim of the study is to stimulate the common peroneal nerve at the lateral shank causing contraction on the peroneal muscles pulling up the lateral edge of the foot upwards creating a motion that is opposite to inversion, thus the COP would shift back to the centre or medial side. Previous research has indicated that using FES for sport can be advantageous however research identified has mostly been focused on those with injuries or disabilities such as work by Taradaj et al. 27 (2013) who indicated electrical stimulation gave beneficial effects when recovering from ACL injury or Hettinga and Andrews 28 who increased performance in those with spinal injuries. A review article that was concerned with recovery mechanism in football identified electrical stimulation as a method sometimes used by teams however they focused on transcutaneous stimulation and found that studies focused around electrical stimulation in football was somewhat lacking. 29 Research appears to be limited when assessing the effect of FES on injury avoidance in sport, however Santos and Liu investigated the effect of noxious and non-noxious electrical stimulation on the unloading reaction in neutral and supinated foot positions, the research indicated that the stimulation had a stronger effect whilst the foot was in a supinated position and indicated that this could be a potential prevention strategy for ankle sprains, which further supports the method being used in this study. 15 The device in this study was set at a maximum of 70 Ma which is slightly less than in the works by Taylor et al who used 80Ma, however that was with stroke patients who had experienced a drop foot, whereas the participants in this study where healthy individuals with no health concerns. 30 Work by Burridge et al used a level of 40 Hz to stimulate the muscles in the with foot drop, whereas this study used 20 Hz however it was felt that because this study used healthy participants and did not want to create a strong rapid contraction, that this level would be suitable. 31

How FES causes peroneal contraction, everting the foot changing COP from a lateral position to a medial position.
The levels of stimulation were set to maintain participant comfort throughout the training programme. The electrodes were placed on the common peroneal nerve and motor point of peroneus longus and confirmed by ensuring stimulation caused eversion of the foot. Participants in the intervention group were exposed to the different levels of stimulation in ascending 10 mA intervals. Prior to running, the participants were exposed to the levels of stimulation that were based upon previous research until they felt they were at the highest level they were comfortable with, it was then checked that they felt they would be able to run whilst experiencing this level of stimulation. 30 , 31 This was carried out on both legs independently with subsequently both legs being set at the same level of stimulation for the duration of the running task. Once optimal dosage (defined as highest level of stimulation comfortable to participant that creates eversion of the foot) was established, this was the level stimulation was set at for the duration of the study, unless the participant was in the control group. Participants in the control group experienced the same protocol, except the device was switched to level zero of stimulation. Participants in the control group were told they may or may not feel the stimulation, this was to try to reduce risk of individuals guessing which groups they were in. Participants were blinded to which group they were allocated to with no participants in the intervention group reporting they were aware of their allocation.
After establishing level of stimulation participants were set up with the device in a waist mounted container and foot switches placed in the heel of the shoes that would create a stimulation on heel contact. The electrodes were placed on the lateral side of the superior part of the lower leg over the common peroneal nerve. Participants were instructed to run on the treadmill (TechnoGym Excite Med, Italy) at a comfortable pace for 15 minutes with the set level of stimulation. The duration of the study was 8 weeks with participants training twice a week on non-subsequent days.
After a 15-minute run with FES, the device was removed and the participant was fitted with Novel pressure insoles and system in their normal running shoes, they then ran on the treadmill for approximately 2 minutes at 11 km/h. All runs were recorded using a Basler (Ahrensburg, Germany) high speed camera and the Novel system, synchronised data was collected at 100 Hz. Prior to the intervention, data was collected from the pressure insoles in 30 second durations and repeated 4 times.
Statistical analysis
The COP data recorded during the trials was post processed using Matlab. The foot width divided by two was subtracted from the x position to give a COP position normalised about the centre of the foot. This allowed for a positive vs negative comparison of medial vs lateral COP. These values were measured throughout the running trial and the sum all of the data points throughout a trial then gave a unit-less measure of magnitude of how medial or lateral the COP was. Each of the trials was repeated 4 times therefore each data point was added then divided by four.
SPSS version 26 (SPSS Incorporated, Chicago, IL) was used to perform a MANOVA on time points (pre-intervention, post intervention, after 8 week intervention and 4 week follow up) and COP position, with COP being the dependent variable. A MANOVA was also performed to identify if there was a significant difference at points during the gait cycle (heel strike, max pressure, heel strike to max pressure) and COP position being the dependent variable. A MANOVA was used so that comparisons could be made at different time points and controlling for uncertainty at 5% when using multiple comparisons. Post hoc T-tests were carried out and Wilcoxon signed rank test tests when data did not meet statistical parameters (such as normal distribution of data) to compare means of the COP values.
Results
There were 44 participants recruited to the initial study, 23 individuals were excluded for having a medial or inconsistent COP during running gait. 14 agreed to take part in the study with 7 declining to take part or unresponsive to recruitment. 14 participants completed up until immediate effect, 8 post 8 week training programme (4 in each group), a total of 6 completed the whole study (intervention = 2; Control = 4). All participants that reached each time point had a 100% compliance rate with the study, none reported any feelings of discomfort.
There was no statistical difference, comparing average COP position pre-intervention, immediately post intervention, after 8 weeks or at 4 week follow up, F(4, 1) = 6.360, p = 0.288; Wilk’s Λ = 0.038, partial ɳ2=.962.
As seen in Table 1, a paired t-test was carried out for COP at different points during the running cycle to compare pre, immediate, post training, follow up effect of stimulation. This was calculated using the values from the statistical analysis as previously described in the statistical analysis section. A Wilcoxon signed rank test was carried out for heel strike to max pressure, as the data was non-parametric due to it not being normally distributed.
Comparing COP at set time points.
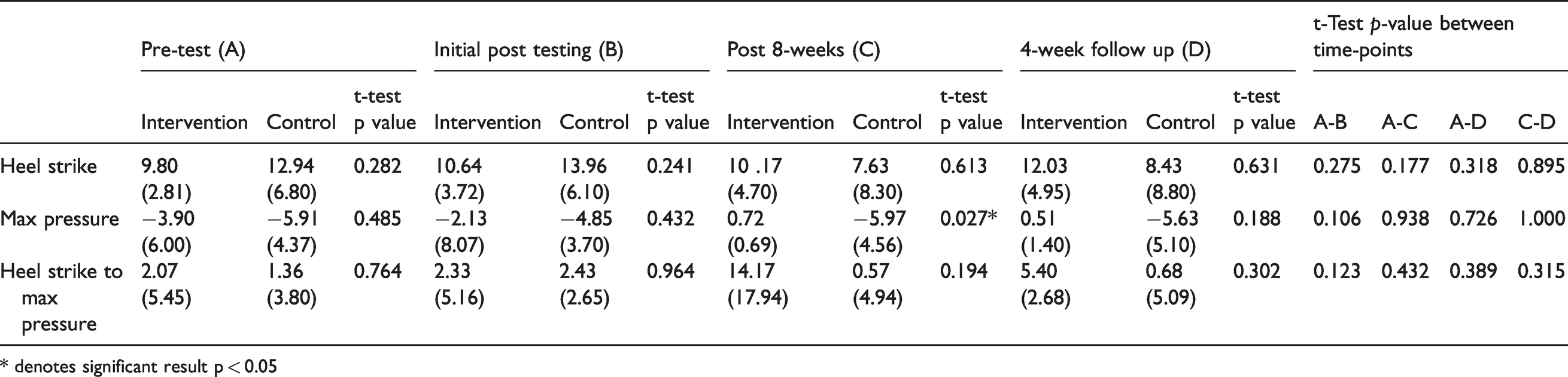
* denotes significant result p < 0.05
There was a significant difference in the results post intervention at max pressure for intervention M = 0.7 (0.7) and control M = −6.0 (4.6) conditions; t(6) = −2.9, p < 0.05.
A Wilcoxon signed-rank test showed that an immediate effect post functional electrical stimulation to the peroneal muscles did not elicit a statistically significant change to COP with those with a lateral COP for those in either the intervention p > 0.05 or the Control group in the period between heel strike and max pressure.
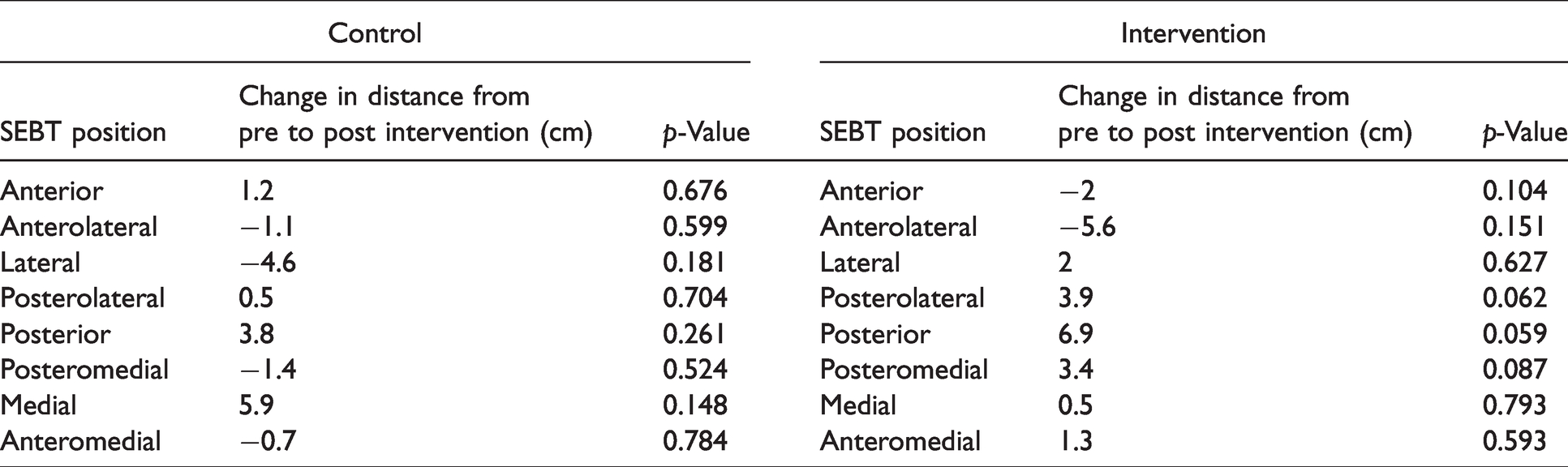
Analysing the difference between the pre and post intervention for the SEBT (Table 2), there was no significant difference between pre and post intervention for those in the intervention group, though for movement, posterior (t(6) = −2.325, p = 0.059), posterior left (t(6) = −2.041, p = 0.087) and posterior right (t(6) = −2.292, p = 0.062) whilst balanced on the right leg there was a difference approaching significance. On average the score increased approximately by 2 cm posterior right, 7 cm posterior and 4 cm posterior left.
Mean change in SEBT in relation to direction and t-test p-values.
Discussion
There was a significant difference when comparing max pressure after 8 weeks intervention, this agrees with the hypothesis, that training the lower limb with FES could shift the COP from a lateral to a medial direction. However, this was not apparent at other stages in the gait cycle. This significant result was from data post 8 weeks of uninterrupted training time, this effect disappears at follow up. There was no significant difference identified when comparing data pre and post intervention immediately after initial session of training protocol, when looking at the other specific points during the running cycle, this was the same for both the intervention and the control group. Comparing pre and post initial training session with FES for COP throughout gait cycle indicated results were approaching significance, though this effect seems to disappear after 8 weeks of training. The SEBT identified an increase of distance reached whilst stood on the right leg in directions, posterior, posterior left and posterior right in those in the intervention groups, though these values were not significant they were approaching significance, no significant difference was noted in the control group. This indicates that there is an improvement in dynamic balance with those that underwent the intervention of the functional electrical stimulation
The study indicates that there may be a positive effect of FES on COP and therefore may be a potential to use it as a training regime, this is somewhat similar to some previous research using stimulation as a method of reducing risk of ankle sprain, however the method of application is significantly different. 18 , 19 The alternative method uses a stronger stimulation to rapidly alter foot position whilst undergoing an inversion as presented by Fong, Chu and Chan, 18 and Fong et al., 19 though the benefit of the current method is that the individual would not need to wear a device during matches or on pitch training where it may cause an impact on performance. Though a significant amount of training would be required to gain any potential benefits, however the hope is that this type of intervention could be applied and used during normal training or running. The effect seen on the SEBT also agrees with previous research such as that by Yoshida, Tanino and Suzuki and would indicate a positive effect of using the electrical stimulation 16 on balance, however again the method is quite different in that they used TENS as opposed to FES. 16
The significant result for max pressure at 8 weeks of uninterrupted training time indicated that the effect disappears at follow up. Therefore the intervention may require a long period of uninterrupted training, as effects may wear off. Longer time periods were not looked at in any of the previous research identified and only focused on immediate effects. This study did not look at time points other than immediate, 8 weeks and 4 week follow up, and therefore would suggest further investigation into training length would be required. Another consideration is the dosage level of stimulation, the level of stimulation was set at a comfort level to allow participants to continue with the training, it is believed that if the dosage was set higher, drop outs may have increased due to potential discomfort. Also it is less likely in the future people would want to adapt it as part of a training regime if deemed painful of uncomfortable.
The whole foot effect that disappeared after 8 weeks could be attributed to the dropout rate. None of those that dropped out reported the reason for drop out being the stimulation device. It is thought that time requirement from the participant was a factor for drop outs, though if this device could be assessed on individuals as part of their normal training regimen the drop out experienced may be avoided. The dosage was set at 2 times a week for 8 weeks, this was set at this level to try and encourage participation, particularly as current research indicates that muscle training should occur 2–3 times a week with at least 1 set of 8–10 reps, however due to the nature of the system the repetitions of the peroneal contractions are much greater, therefore the level of intervention was believed to be appropriate. 32 If frequency had increased drop outs may have been greater, though it is hoped in the future that this form of stimulation could be used anytime an individual trained, by using it more of an adjunct of normal training there would be the potential to increase compliance and frequency which may yield more significant results. When considering the literature this does not fit into the model of increasing muscle volume using high loads and set reps, however that method is likely to be problematic with this type of intervention. 33 The method used is closer linked to a low resistance high rep technique that has been linked with little to no increase in muscle mass but improved muscle endurance which could be beneficial for athletes to avoid LAS. 34 However the strength of muscle contraction was not measured for this study and therefore difficult to compare, though it was unlikely to be near maximum due to the low level of FES used and the comfort of the participants.
Summary
The study indicates that using FES to stimulate the common peroneal nerve activating peroneal longus and brevis muscles could shift a laterally-deviated COP to the medial direction, as results indicated during max pressure in running gait after an 8 week training programme that there was a significant change. Although carry over effect appears limited and further testing is required. It is also indicated that there is some improvement in balance post intervention. Overall this may indicate FES as a potential training regime to reduce risk of LAS.
Footnotes
Author contribution
Zoe Bamber contributed to the study design, data collection, data analysis, writing up of the first draft. Patrick Wheeler contributed to the study design, data analysis, interpretation, and approved the final draft. Ian Swain contributed to the study design, implementation of the intervention, data interpretation, and approved the final draft. Daniel Fong contributed to the study design, data interpretation, revision and approval of the final draft, and supervision of the entire project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.