
Abstract
Introduction
Functional electrical stimulation applies electrical pulses to the peripheral nerves to artificially achieve a sensory/motor function. When applied for the compensation of foot drop it provides both assistive and therapeutic effects. Multi-field electrodes have shown great potential but may increase the complexity of these systems. Usability aspects should be checked to ensure their success in clinical environments.
Methods
We developed the Fesia Walk device, based on a surface multi-field electrode and an automatic calibration algorithm, and carried out a usability study to check the feasibility of integrating this device in therapeutic programs in clinical environments. The study included 4 therapists and 10 acquired brain injury subjects (8 stroke and 2 traumatic brain injury).
Results
Therapists and users were “very satisfied” with the device according to the Quebec User Evaluation of Satisfaction with Assistive Technology scale, with average scores of 4.1 and 4.2 out of 5, respectively. Therapists considered the Fesia Walk device as “excellent” according to the System Usability Scale with an average score of 85.6 out of 100.
Conclusions
This study showed us that it is feasible to include surface multi-field technology while keeping a device simple and intuitive for successful integration in common neurorehabilitation programs.
Keywords
Introduction
Functional electrical stimulation (FES) applies electrical pulses to motor and sensory nerves in order to restore or assist a function. 1 FES systems consist of a stimulator unit that generates the electrical pulses, and at least two electrodes, which act as an interface between the stimulator unit and the targeted nerves. Transcutaneous electrodes, i.e. surface electrodes, are placed on the skin over the targeted peripheral nerves and due to their ease of use and affordable price they are the preferred solution for therapeutic applications. 2 They are usually reusable and consist of a conductive hydrogel layer, which makes them easy to don/doff. 3
Several studies have shown the positive effects of FES applications in the neurorehabilitation field, where it has been successfully used in a great variety of therapeutic applications.4–9 Similarly, FES is commonly used for assisting impaired functions caused by neurological disorders, and is often denoted as a neuroprosthesis in these applications.10–13 One of the most frequent applications is the compensation of foot drop syndrome. Foot drop syndrome is a motor dysfunction that is usually caused by a neurological disorder and results in the inability of performing voluntary dorsiflexion of the affected ankle. This motor dysfunction results in a pathological gait characterized by a limited foot clearance during the swing phase, shorter stride lengths, reduced single-limb stance phases, and often lower gait speed. 14 People who have experienced a stroke usually exhibit additional compensatory movements such as circumduction of the leg and elevation of the pelvis of the affected side as a result of a reduced hip and knee flexion. 15 FES-based foot drop compensation devices have been shown to improve pathological gait both when used as an assistive device6,11,16 and when used as a therapeutic device in rehabilitation programs.6,11,17
Most available commercial devices consist of a portable one or two channel stimulator with surface electrodes targeting the peroneal nerve. The nerve is activated during swing phase of the gait. Often a tilt sensor or foot switch 18 triggers the activation pattern. One of the often-reported usability issues with commercial FES foot drop devices is the complex initial set-up and the difficulty to find the right electrode positions.19,20 The latter can be caused by the intra-subject variation of the spatial activation points from day to day21,22 that complicate the search for proper electrode positions and stimulation parameters valid over multiple unsupervised applications. This type of usability issue may discourage potential users from using FES foot drop devices, 20 so it is important to consider usability aspects from the initial design and development stages of FES systems to be able to improve uptake.
In the last years, surface multi-field electrodes have emerged 23 and have shown a great potential on improving activation selectivity24,25 over conventional surface electrodes. 26 Multi-field electrodes have also shown advantages in decrease of muscle fatigue.27–29 They can adapt the activation region to inter- and intra-subject differences by means of an automatic search of best activation points, so-called motor points.22,30–33 On the other hand, the multi-field electrode technology exponentially increases the number of possible stimulation combinations, and therefore potentially increases the complexity of its use. A recent study compared the usability of the multi-field FES system with commercial devices owned by the seven participants, where the former resulted in lower scores in terms of ease of use. 34 Nevertheless, the study proved the feasibility of using a multi-field FES-based foot drop system as a take-home system.
In the present study, we used a multi-field FES-based foot drop system that was designed to personalize and improve activation selectivity while keeping the interface intuitive and easy to use, and not to compromise usability aspects that are of key importance in a clinical environment. The aim of this field study was to analyze the usability and user satisfaction aspects of the device from both therapists’ and patients’ perspectives. A further aim was to check the feasibility of integrating surface multi-field electrode-based FES systems into a neurorehabilitation program in a clinical setting. The usability study was carried out with 10 subjects with foot drop syndrome and 4 therapists.
Methods
FES system
The Fesia Walk device, shown in Figure 1, is a rehabilitation device aimed to be used in therapy sessions in clinical environments with people who have a foot drop caused by neurological disorders. It delivers electrical pulses to the peroneal and tibial nerves in order to elicit a dorsal flexion and plantar flexion of the ankle in the corresponding phases of the gait. This system is based on surface multi-field electrodes that provide an improved activation selectivity and finds the stimulation motor-points by means of a semi-automatic calibration procedure.
22
The Fesia Walk device consists of a stimulator unit, a multi-field electrode, a gait phase detection sensor, a textile garment, and a software application.
Fesia Walk device.
Stimulator
The stimulator unit generates biphasic electrical current pulses. The device operates wirelessly and has a single current source capable of delivering pulses and controls up to 40 electrode fields independently. It is designed to be worn under the clothes. The system can be controlled remotely from a mobile device and a software application via wireless Bluetooth communication. The overall stimulation amplitude can be increased and decreased on the stimulator unit by means of two push buttons at any time during its use.
Multi-field electrode
The multi-field electrode, shown in Figure 2, was designed to cover the posterior and lateral sides of the knee in order to stimulate the peroneal and tibial nerves. It consists of 16 cathodes of 18 × 15 mm and four anodes of 18 × 33 mm size, which can be activated independently or combined, allowing the electrode to adapt to different physiologies. This multi-field electrode has two conductive gel (AG703) layers that cover the cathodes and the anodes.
Fesia Walk multi-field electrode and textile garment (inner view).
Sensor
The Fesia Walk gait phase detection sensor consists of a 9-degrees of freedom inertial measurement unit (IMU), a microcontroller and a Bluetooth radio. It has two main functions: (i) the search of optimal stimulation parameters (calibration) and (ii) the real-time detection of different gait phases. Its size is 50 × 42.5 × 16 mm and its weight is 30 g. The sensor can be attached to the shoelaces or the tongue of the shoe with an embedded clip.
The calibration stage is carried out while the user is sat down on a stretcher with his legs in an extended position and the ankle has freedom of movement. In this stage, the sensor measures ankle dorsal flexion, plantar flexion, inversion and eversion of the foot. During calibration the optimal fields and stimulation parameters are automatically determined for each of the movements. 22 During gait, the sensor detects heel-off and heel-on moments of the affected foot, and triggers the corresponding stimulation patterns.
Garment
The textile garment ensures proper skin–electrode contact and serves as support for both the stimulator and the multi-field electrode. The garment is ergonomically designed to be placed right under the knee. It comes in two versions, one for each laterality (left/right). The textile is breathable and washable. It does not include any rigid materials and adapts to different leg sizes and shapes. A magnetic closing system allows its single-handed donning.
Software application
The Fesia Walk system includes a HTML5 software application that runs on several platforms (PC, tablet, phone) and operating systems. The application controls and sets the stimulation parameters. It also allows supervision of the patient’s evolution in terms of range of motion (ROM) of the ankle in an easy and intuitive way. The application was designed to be used by therapists or clinicians and includes a patient management platform. With this platform therapists and clinicians can generate reports that describe the status and details of each patient, store specific parameters, and check the patient’s record history.
The application includes a calibration screen for semi-automatic detection of the optimal stimulation parameters. 22 In the first step, the calibration procedure automatically activates each of the independent fields of the electrode and selects the best field combinations to achieve four different ankle joint movements (inversion, dorsiflexion, eversion and plantarflexion). The user can set the stimulation frequency, pulse-width and amplitude ranges, select the cathodes to be skipped or restart and stop the calibration procedure at any time.
After calibration the user is directed to an optimization screen, shown in Figure 3. Here the user can supervise and adapt the determined stimulation fields and parameters, and can save them directly or modify them. Additionally, the user can manually test any field combinations before saving the definitive parameters. The parameters saved in this screen for obtaining dorsiflexion and plantarflexion are then used during the walking mode.
Optimization screen of the software application.
After these steps, the device gets configured and the user can initiate the walking mode. During the walking mode the software application shows the battery level and connection status of the device.
Lastly, the software includes an assessment screen where the IMU sensor can measure the active and passive ROMs of the ankle joint. This data is stored for each patient and is visualized in the form of graphs, where the clinicians can easily observe the evolution of the patient throughout time.
Protocol
In order to validate the usability of the Fesia Walk system, a field usability study was carried out in a clinical environment. The study was authorized by the local ethical committee (Comité Ético de Investigación Clínica de Navarra) and the Fesia Walk device was approved by the Spanish Agency of Medicines and Medical Devices for its use in this research study (578/16/EC).
Subjects
In this study, 4 therapists and 10 subjects with acquired brain injury (8 stroke subjects and 2 traumatic brain injury (TBI) subjects) were involved. The therapists were responsible for manipulating the system, i.e. performing donning, calibration, setting of parameters and doffing. The subjects with acquired brain injury, all showing a foot drop syndrome, wore the device and walked with it. Neither the therapists nor the subjects had previous experience with using FES foot drop devices.
The inclusion criteria for subjects were the following:
more than 18 years old foot drop caused by stroke or TBI time from injury more than one year independent ambulation (no human support) for more than 10 m capacity to understand and follow simple verbal instructions
Exclusion criteria were:
injury of peripheral nervous system severe spasticity (Modified Ashworth = 4) severe muscle contractures in the target leg use of pacemaker pregnancy metallic implants in target leg allergy to electrodes hypersensitivity to electrical stimulation
Therapist details.

Procedure
Therapists received a training lesson of 1 h and received the user manuals before starting the study to learn how to use the Fesia Walk device. Each therapist was randomly assigned to two or three subjects. Each subject received three adaptation sessions to become used to FES, followed by six therapy sessions. Finally, an evaluation session was carried out, where therapists and subjects were interviewed and filled out the satisfaction and usability questionnaires.
First, each therapist carried out all the sessions with a single subject, and once finished, they started with their second (and third) subject, as can be seen in Figure 4. This was done to ensure that the learning process was carried out from the beginning to the end with one subject to avoid noise or difficulties derived from managing more than one subject in parallel the first time they were using the device.
Protocol schedule.
Outcome variables
To assess the usability of the system, two different questionnaires were passed to the therapists only. One of them was the standard System Usability Scale (SUS),
35
which consisted of 10 items or statements that the participants had to rate according to their level of agreement. The scores were comprised between 1, meaning “strongly disagree”, and 5, meaning “strongly agree”. The items of the SUS scale are the following:
Item 1: I think that I would like to use this product frequently. Item 2: I found the product unnecessarily complex. Item 3: I thought the product was easy to use. Item 4: I think that I would need the support of a technical person to be able to use this product. Item 5: I found the various functions in the product were well integrated. Item 6: I thought there was too much inconsistency in this product. Item 7: I imagine that most people would learn to use this product very quickly. Item 8: I found the product very awkward to use. Item 9: I felt very confident using the product. Item 10: I needed to learn a lot of things before I could get going with this product.
For determining the satisfaction of both the therapists and subjects with respect to the Fesia Walk device, the standardized Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) questionnaire 36 was used. The last four questions of the QUEST related to product services were skipped because they were out of our scope. Thus, the questionnaire consisted in eight items (dimensions, weight, adjustments, safety, durability, ease of use, comfort and effectiveness) that the participants had to rate according to their satisfaction level, with 1 meaning “not satisfied at all”, and 5 meaning “very satisfied”. Furthermore, each participant had to select the three items that they considered to be the most important according to their criteria.
The QUEST and SUS are general satisfaction and usability evaluation scales. So, a complementary questionnaire that was specific to usability aspects of the Fesia Walk device was designed. The aim of this questionnaire was to extract more specific information about potential usability issues and thus, to increase the sensitivity of the evaluation. Therapists were asked to fill this custom-designed questionnaire after each session in order to analyze the evolution of the usability ratings of the device over sessions. The questionnaire consisted of 24 items that the therapists had to rate according to their level of agreement (scores ranged from minimum 1 to maximum 10). It included items related to donning/doffing, automatic calibration, manual configuration, and walking quality with the device. Additionally, it included a section for reporting problems. The items of the Fesia Walk questionnaire were the following:
Item 1: I placed the system on the subject’s leg easily. Item 2: I placed the sensor on the subject’s foot easily. Item 3: I initiated the application easily. Item 4: I selected or created a new subject easily. Item 5: I carried out the ROM measurements easily. Item 6: I understand the obtained measures. Item 7. I think that the ROM measures were correct (approximately). Item 8. I carried out the adaptation session easily (sessions 1 to 3). Item 9. I found the motor threshold easily (sessions 1 to 3). Item 10. The subject has shown tolerance to electrical stimulation. Item 11. I have carried out the calibration easily. Item 12. I think that the automatic calibration found a good dorsal flexion. Item 13. I think that the automatic calibration found a good plantar flexion. Item 14. I consider that the automatically selected fields were good. Item 15. I consider that the automatically selected parameters were good. Item 16. I carried out the optimization easily. Item 17. I think that the subject walked better with the system than without it. Item 18. I think that the subject walked worse with the system than without it. Item 19. I think that the stimulation was triggered in the correct phases of gait. Item 20. I think that the subject felt safer walking with the system than without it. Item 21. The subject has expressed positive comments about the device. Item 22. The subject was not fatigued while walking with the system. Item 23. I managed well in general with the device. Item 24. I managed well in general with the application.
Finally, a personal interview was carried out with each of the therapists and subjects to collect general comments and feelings about the device that were not covered by the questionnaires. The following list presents the interview guide with questions for therapists (T), subjects (S), or both (B):
Did the device meet your expectations? B Was it better than expected? B Was it worse than expected? B What did you like the most? B What did you like the least? B Would you use it daily? B Would you use it regularly? B Would you use it at home? S Would you recommend it for home? T Do you think you could learn to handle it? S Do you think it is easy to handle? T Was the device (garment) comfortable? S Was the electrical stimulation uncomfortable? S Did you feel safer walking with the system than without it? S Did you feel less safe walking with the system than without it? S Was it easy to don/doff? T Was it easy to adjust (garment)? T Was it easy to calibrate? T Did you prefer the automatic or manual tuning of parameters? T Was it easy to manage different patients? T Was it an intuitive system? T Did you find it easy to check the correct functioning of the system? T Was it easy to find a dorsal flexion with the system? T Was it easy to find a plantar flexion with the system? T Do you think that the gait improved with its use? T Do you think that the gait got worse with its use? T Would you like to continue using the system? B Did you like the design? B What part of the design did you like the most? B What part of the design did you like the least? B Would you add any function or feature to the device? B How would you describe the whole experience (one sentence)? B How would you describe the device (one sentence)? B Would you like to participate in another study with this device in the future? S
Sessions
Adaptation session
Number of sessions (each subject): three
Session duration: 30 min
The objective of the adaptation sessions was to make the subjects familiar to surface FES as well as adapting the neuromuscular system to the application of FES. Each session consisted of the following steps:
Don the Fesia Walk device and sit the subject in a chair with their legs in an extended position. Run a calibration iteration
22
adapting the amplitude to the subject’s comfort with frequency and pulse-widths set to 35 Hz and 250 µs, respectively. Repeat the previous step increasing the amplitude in 2 mA steps until subject’s tolerance. Stop the stimulation and doff the Fesia Walk device. Fill the usability questionnaires designed specifically for Fesia Walk (only therapists).
Although the adaptation sessions did not include walking with the device, the therapists were instructed to find a proper ankle movement, as performed during walking, when the subject’s tolerance to stimulation was above motor threshold.
Fesia Walk session
Number of sessions: six
Session duration: 45 min
The objective of these sessions was to provide gait therapy sessions based on the Fesia Walk device to check the feasibility of integrating it in rehabilitation routines. Each session consisted of the following steps:
Don the Fesia Walk device and sit the subject in a chair with their legs in an extended position on top of a support cushion, ensuring movement freedom for the ankle. Run the Fesia Walk calibration
22
with the amplitude set to subject’s tolerance, frequency 35 Hz and pulse-width 250 µs. Start the gait mode of the Fesia Walk and ask subjects to walk with the device until the end of the session. The gait was adapted to each subject, adding resting times or including more complex functions (stairs, obstacles,…) depending on the condition of each subject. Stop the stimulation and doff the Fesia Walk device. Fill the usability questionnaires designed specifically for Fesia Walk (only therapists).
Evaluation session
Number of sessions (each subject): one
Session duration: 30 min
The objective of these sessions was to collect feedback regarding satisfaction and usability of the Fesia Walk device from both therapists and subjects. The evaluation session was carried out at the end of the sessions to the subjects, and at the end of all the studies to the therapists. The evaluation session for the subjects consisted of the following steps:
Present and ask to fill the modified QUEST scale to the subject. Carry out an interview with the subject.
The evaluation session for the therapists consisted of the following steps:
Present and ask to fill the modified QUEST and the SUS scales to the therapist. Carry out an interview with the therapist.
Results
Usability
The usability results were obtained from the SUS and the Fesia Walk specific questionnaire scores. These were only obtained from the therapists, as they were the ones handling the devices. According to the SUS scale, 35 the therapists considered the Fesia Walk device as “excellent” from the usability perspective with an average score of 85.6 out of 100.
In Figure 5, it can be seen the average total score of the SUS scale and the total scores of each therapist ranging from 77.5 to 90 out of 100.
Average SUS usability scores.
Regarding specific item scores shown in Figure 6, the Items 2, 3, 4, 7, and 8 got a median score of 10 out of 10, which were all items related to the ease of use. The Items 1, 5, 6, and 9 were scored the lowest with median scores of 7.5 out of 10 and corresponded to statements related to the frequency of use, the consistency, and the confidence of the therapists when handling the system.
Item SUS median usability scores.
The questionnaire designed specifically for the Fesia Walk device provided us with the evolution of the usability scores over sessions, which we expected to increase with the therapists’ experience in using the device. Figure 7 shows the learning curves of each therapist, i.e. an increase of the usability scores, until approximately the 5th session. After the 5th session, the usability scores either reached a plateau or increased slowly. This effect is more evident in Therapist 3. All therapists scored higher with the second and third subject than with the first subject, which indicates that they got used to the device after the first subject. Some usability aspects like donning, adaptation, or calibration were carried out easier even in the first session with next subjects.
Fesia Walk usability questionnaire scores over sessions for the four therapists. Vertical black lines indicate the last adaptation session for each of the subjects.
Specific items related to the donning of the device (Items 1, 2, 3 and 4) were rated highest by all therapists together with items related to the general use of the device (Items 21, 23, 24). The lowest scores were found in the items related to calibration (Items 11, 12, 13, 14, 15, 16). Specially, Item 13, related to the ease of finding plantar flexion, and Item 14, related to the quality of the automatically selected fields, received low scores.
Overall 27 problems were reported during all the studies, which did not interfere at all with the completion of the sessions. Twelve of these problems were related to wireless connection issues between the tablet and the stimulator. The application crashed six times and the stimulator crashed (stopped stimulating) three times during the entire study. All these problems happened during the configuration process, never during gait, and were solved fast by resetting the application or/and the stimulator. Finally, one of the therapists reported problems on electrode positioning. She had to reposition the electrodes in three sessions with one of the subjects and in two sessions with another subject. This issue was only reported by one therapist and in two of her three subjects. It could be caused by an incorrect method of initial electrode positioning or calibration of electrode fields and parameters, or by the difficulty of generating specific ankle joint movements for these two subjects due to their physiological characteristics.
Satisfaction
Subjects
The satisfaction results from the QUEST questionnaires of the subjects are shown in Figure 8. The average score was 4.2, meaning that in average they were “quite satisfied” with the device according to the QUEST scale.
36
Subject 9 reported the lowest overall score of 3.4, meaning “more or less satisfied”, which was the result of low scores related to size, weight, and ease of adjustment of the device.
Average QUEST satisfaction scores—subjects.
In Figure 9, we compared the results obtained in this study with results obtained in the feasibility study of another multi-field FES foot drop system known as Shefstim.
34
Shefstim was tested on seven participants who were already users of commercial FES devices. Fesia Walk got higher scores than the Shefstim, and the commercial devices in those items related to dimensions and weight. It also resulted in higher scores than the Shefstim in terms of safety and ease of use. However, Fesia Walk got lower effectiveness scores than the Shefstim. It should be remarked that the Shefstim, and other commercial devices were described as assistive devices, whereas the Fesia Walk was described as a rehabilitation device, which could have affected the scores of this item. We can see that safety was the item that got the highest median score of 5 out of 5. This comparison should be taken cautiously, as the population, sample size, and protocol of the Shefstim study were different,
34
and thus, statistical analysis cannot be applied. However, it can serve as a reference for the Fesia Walk as it is the only usability study carried out with a multi-field FES foot drop system.
Item QUEST median satisfaction scores. Comparison with the ShefStim feasibility study results34—subjects.
In Figure 10, we can see the items that were considered most important for the subjects. They considered the effectiveness to be the most important aspect of a medical device, followed by the comfort and the ease of use.
QUEST most important items—subjects.
Therapists
Figure 11 shows the satisfaction results from the QUEST questionnaires obtained from the therapists. Similar to the subjects, the average score was 4.1 out of 5, meaning that in average therapists were also “quite satisfied” with the device. Indeed, Therapist 1, who was the most experienced on neural rehabilitation, was “very satisfied” with the device having rated an overall score of 4.7 out of 5.
Average QUEST satisfaction scores—therapists.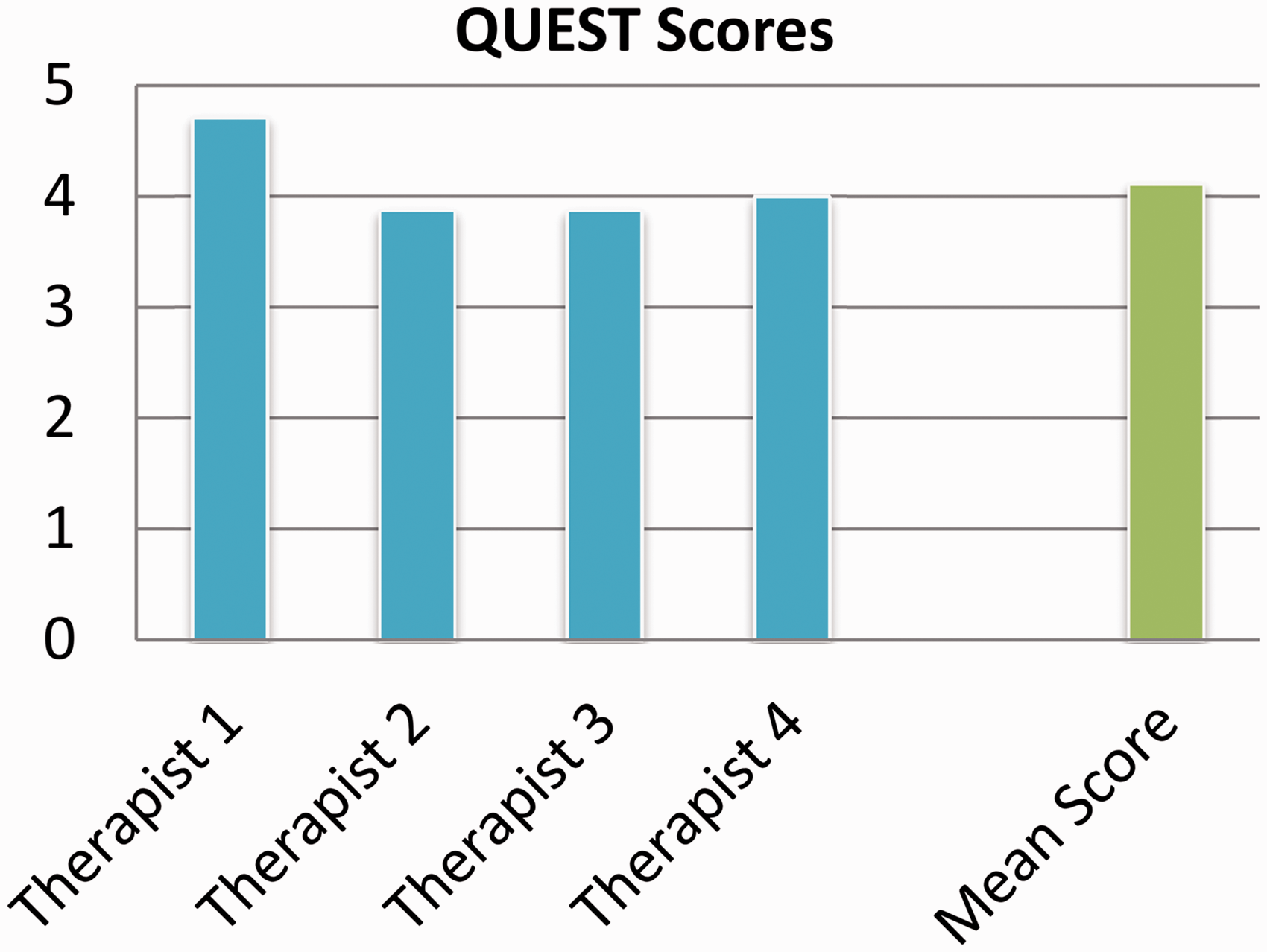
When we analyze specific item scores given by the therapists in Figure 12, we can see that again safety was the item with the highest median score with 4.5 out of 5, whereas the rest of the items scored 4 out of 5.
Item QUEST median satisfaction scores—therapists.
Finally, Figure 13 shows the effectiveness to be the most important aspect of a medical device for therapists and gave importance to the ease of use. Unlike the subjects, they did not consider comfort to be such an important aspect, and dimensions of the device were more important instead.
QUEST most important items—therapists.
Interviews
A heterogeneous collection of comments, opinions, and suggestions was received during the interviews, and most of them had positive connotation. All the subjects reported that the device met or exceeded their expectations; all of them found the device comfortable. All but one person expressed their wish to keep and use the device periodically and all but one person felt safer during gait when wearing the device. Similarly, all therapists expressed their wish to keep applying the device continuously and all of them found the device easy to use in all aspects.
However, few negative comments were also received. Some of the subjects expressed difficulties in donning the device without assistance, and three of them found the sensation produced by FES a bit unpleasant. The therapists mentioned that they sometimes did not fully agree with the parameters suggested by the automatic calibration and preferred to do manual adjustments. They noticed that there was a high inter-session variability of the functional response to the device.
Discussion
Regarding usability, the therapists rated the Fesia Walk using the SUS scale as “excellent” and were all in agreement that they could use the device without any support from a technician. However, most of them agreed to use the device sporadically and not daily. This could be linked to some comments that therapists did at the end of the study. The automatic calibration did not always determine the best fields for all movements and the electrode position affected the quality of the movements. Thus, some therapist chose to manually adjust the stimulation parameters and to reposition the electrode in few sessions, which may have influenced their ratings about the daily use of the device. Donning and general aspects of the use of Fesia Walk received the highest scores. Analyzing the usability scores throughout the sessions we could see that the learning curve of the therapists to apply the Fesia Walk device took around five sessions, and some usability aspects like donning, adaptation, or calibration were easier to carry out after the first subject.
When compared in terms of usability to another multi-field electrode-based system 34 and other commercial FES devices, the Fesia Walk showed similar scores, although this comparison should be taken cautiously as both studied followed different protocols and had different sample sizes. The lower score on the effectiveness item could be affected by the purpose of the device. Shefstim and other commercial devices were developed as assistive devices, whereas Fesia Walk was introduced to the participants as a rehabilitation device. Therefore, the effectiveness score was based on the subjects’ and therapists’ perception of recovery. The aim of this study was not to check the therapeutic effect of the device so its duration was not enough for the participants to observe significant improvements on gait. This fact could have affected the scoring of the effectiveness item.
The satisfaction scores showed that both therapists and subjects were “quite satisfied” with Fesia Walk. Both groups agreed that the best aspect of the device was that they felt safe when using it. Actually, it was interesting to find out that effectiveness and ease of use were important aspects for both therapists and the subjects, but the latter group seemed to give more importance to comfort, whereas the therapists were more concerned about the physical dimensions of the device and suggested that it could be smaller to fit better under tighter trousers. It might be that the subjects did not share this concern because the device was presented to them as a rehabilitation device to be used in therapy sessions in the clinic and in this environment, they might not care much about the size. However, therapists tended to think of it as a rehabilitation and assistive device that subjects could wear during their daily activities.
Finally, it should be remarked that most subjects expressed their wish to keep using Fesia Walk periodically, that they felt safer when walking with the device and that they found the device comfortable. Similarly, all therapists expressed their wish to continue using Fesia Walk and found the device intuitive and easy to use.
Conclusion
Despite the fact that surface multi-field electrodes increase the number of stimulation parameters and might increase the overall complexity, it seems feasible to include this advanced technology with a thoughtful design that does not compromise usability aspects. In fact, the presented system benefits from the advantages of multi-field electrodes such as automatic electrode selection, adaptability to different physiologies, and the possibility of stimulating different fields for achieving different ankle movements.22–33 The user-interface was designed to be as simple and intuitive as possible, resulting in a fair balance between technological advance and prioritization of usability aspects.
All the participants were very satisfied with the Fesia Walk device in terms of usability and we could confirm the feasibility of integrating a FES device based on surface multi-field electrodes in a clinical rehabilitation program.
Further improvement of the weakest aspects of the device discovered in this study may help to increase acceptance of these devices even more. Usability studies like the presented one or feedback from end-users are crucial to guarantee the success of FES devices in clinical practice. Furthermore, clinical studies should be carried out to confirm the therapeutic effect of these types of multi-field electrode-based FES systems in neurorehabilitation.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eukene Imatz-Ojanguren, Thierry Keller and Haritz Zabaleta are employed at TECNALIA, San Sebastián, Spain, from which they receive financial compensation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this study was supported by the European Regional Development Funds through the Interreg Sudoe Program, project SOE1/P1/F0370.
Guarantor
EIO.
Contributorship
EIO, HZ, and TK researched the literature, conceived the study, partly designed the Fesia Walk device, developed the documentation for obtaining the ethical approval and carried out the data analysis. GSM, JRAA, JCM, and EJG were involved in the protocol design and development, subject recruitment, and carried out the usability study. EIO wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
The authors want to thank David Valencia, Milos Kostic, and Javier Camarena for their great technical support and to the volunteers for their participation in this study.