
Abstract
Background
Ankle dorsiflexor muscle strength is a crucial component of gait.
Objective
We describe the development of a simple, hand-held dynamometer to measure the ankle dorsiflexor muscle strength in the sitting position. In addition, we examine its intra- and inter-rater reliability.
Methods
Measurements of the peak ankle dorsiflexor muscle strength were obtained by two examiners for 30 ankles of 15 healthy adults at two time points, with a one-day interval between measurements, to determine the inter- and intra-rater reliability. The intraclass correlation coefficients were calculated, and an intraclass correlation coefficient > 0.90 was considered as excellent reliability. A Bland–Altman analysis was used to assess systemic bias. The minimal detectable change in muscle strength was calculated with a confidence level of 95% (MDC95).
Results
The reliability of the device was excellent for both intra- (intraclass correlation coefficients [1,3] = 0.94) and inter-rater (intraclass correlation coefficients [2,3] = 0.96) comparisons. No fixed or proportional bias was observed between the two examiners. The MDC95 was 0.77 N/kg.
Conclusions
Our results indicate the excellent reliability and responsiveness of our device. By obtaining the measurements of dorsiflexor strength while sitting, compensatory motions are suppressed, yielding a more consistent measurement that can be reliably used to detect subtle changes in the ankle dorsiflexor muscle strength.
Keywords
Introduction
Ankle dorsiflexor muscle strength is a crucial component of functional mobility for patients with upper 1 and lower 2 neuron disease. Hand-held dynamometers (HHDs) provide an easy-to-use technique in practice for the quantitative assessment of isometric muscle strength.3–8 Although the intra-rater4,5 and inter-rater3,6,8 reliability of HHDs for the measurement of the ankle dorsiflexor muscle strength has been previously discussed, issues regarding optimal positioning of the patient to avoid compensatory motions remain controversial; these include the position of the patient (supine3,4,6,8 or sitting5–7), the position of the knee (extension3,4,6–8 or flexion 5 ), the position of the ankle (in dorsiflexion,7,8 neutral3,4 or in plantarflexion 6 ), and fixation or non-fixation of the HHD (with 7 or without3–6 a belt). Therefore, we developed a new, simple device for the measurement of the ankle dorsiflexor muscle strength to avoid compensatory motions, relax the excessive tension of the gastrocnemius muscle, and allow a firm hold of the HHD. The purpose of this study was to describe our novel HHD, determine its intra- and inter-rater reliability in a group of healthy adults, assess the systematic bias, and calculate the minimal detectable change (MDC).
Methods
Measurement system
We developed a measuring device made of wood (length 25 cm, width 30 cm, height 15 cm, and weight 800 g; Figure 1). The examinee places his/her foot on the footrest of the device, and an examiner fastens it with a belt after the HHD (μTas F-1®; Anima Co., Ltd, Tokyo, Japan.) is inserted between the device and belt. The distal side of the belt is positioned over the proximal portion of the metatarsal phalangeal joints. The belt, which was made of nylon that had been braided, was not elastic and was hard to rub.
Measurement position for use of the hand-held dynamometer.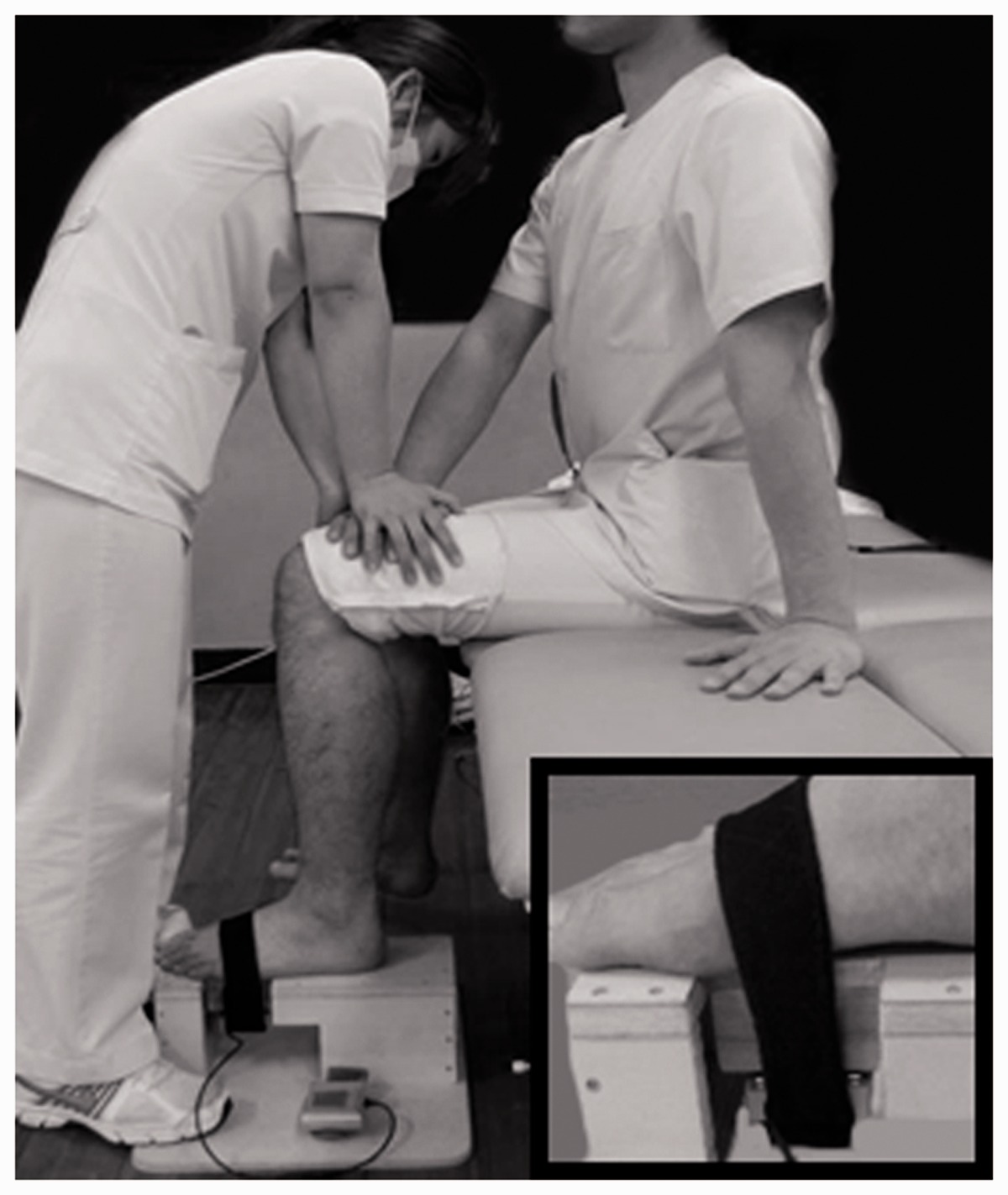
First, the examinee sits on the edge of a treatment table, with the hip and knee flexed to 90° and the ankle in a neutral position. The contralateral lower limb is placed on the floor to avoid compensatory motion. The examinee presses the knee down on the test side using the contralateral hand, while the examiner also presses down on the examinee’s hand to prevent compensatory motions. The examiner keeps his/her foot on the base of the device to fix it firmly. The examiner conducted several exercise sessions for the measurement under the manual.
Procedure
We included 30 legs of 15 healthy participants (eight males and seven females, mean age 27.1 ± 6.1 years, mean height 164.8 ± 11.0 cm, and mean weight 57.4 ± 9.0 kg). All participants provided informed consent. Our study was approved by the University of Occupational and Environmental Health.
Measurements were obtained independently by two physical therapists with >8 years of clinical experience. After instruction, each participant was asked to dorsiflex the ankle joint as hard as possible for 3–5 s, with verbal encouragement provided by the examiner. An examiner measured the muscle strength three times on the same day, and a 2-s rest was given between each trial. The other examiner measured it again on a different day. The ankle dorsiflexor muscle strength is expressed as a force body weight ratio (the average value of three measurements/body weight, N/kg).
Data analysis
The intra-rater reliability was evaluated using two interclass correlation coefficients (ICCs) ([1,1] and [1,3]). In the first and second sessions, the muscle strength was measured bilaterally using the Bland–Altman analysis. 9 The standard error of the mean (SEM = SD√1-ICC) and MDC95 (1.96 × √2 × SEM) were calculated. 10 The ICC was classified as follows: excellent, ≥0.90; good, 0.90 > ICC ≥ 0.75; moderate, 0.75 > ICC ≥ 0.50; and poor, ICC < 0.50, with the lower boundary of the 95% confidence interval (CI) of the ICC ≥ 0.50. 10 All analyses were performed using SPSS (version 21J, IBM Japan, Tokyo, Japan), and the statistical significance level was set at <5%.
Results
The intra-rater reliability of the measured ankle dorsiflexor muscle strength showed excellent agreement, with an ICC (1,3) of 0.94 (95% CI 0.88–0.97) and an ICC (1,1) of 0.87 (95% CI 0.74–0.94). No systematic bias between the two sessions was determined by the Bland–Altman analysis (Figure 2(a)). The average and standard deviation of the ankle dorsiflexor muscle strength to body weight ratios were 3.33 N/kg and 1.15 N/kg, respectively, with an SEM of 0.28 N/kg (SEM%, 8.3%) and MDC95 of 0.77 N/kg (MDC95%, 23.0%).
Bland–Altman intra-rater reliability data plot (a) and inter-rater reliability data plot (b).
The inter-rater reliability of the strength showed excellent agreement, with an ICC (2,3) of 0.96 (95% CI 0.92–0.96) and an ICC (2,1) of 0.94 (95% CI 0.87–0.97), with no systematic bias between the two examiners (Figure 2(b)).
Discussion
We have developed a new, simple HHD device that allows for measurement of the ankle dorsiflexor muscle strength and effectively suppresses compensatory motion with excellent reliability. The adjustable height of the seat improves positioning, while the belt provides effective stabilization, regardless of the shape of the foot. The reliable positioning and high ICC, with no significant systematic bias, support the use of our device to obtain reliable measurements of the ankle dorsiflexor muscle strength. The MDC95 of 0.77 N/kg further indicates that the device can be used to reliably identify subtle changes in the ankle dorsiflexor muscle strength, which would be useful in determining the effectiveness of interventions in clinical practice. Moreover, the device is light and portable and can be easily used in various settings. Although an isokinetic dynamometer may be desired to measure the ankle dorsiflexor muscle strength accurately in a sitting position, it is expensive and not portable.
The limitations of our study include the use of a small sample of healthy young adults; the reliability needs to be confirmed in patients with hemiparesis or peripheral nerve palsy. Additionally, effects of foot deformity or spasticity need to be considered. In the future, we should examine the reliability and detect the clinical change in elderly people and hemiplegic patients. Our HHD device does require more skill and time for set-up and positioning of the examinee than conventional manual muscle testing. Once set up, however, measurement of the ankle dorsiflexor muscle strength takes only a few minutes. Furthermore, a comparison with manual muscle testing would be useful to provide the effort of the developed device.
Conclusions
We developed a new and simple HHD device to measure the ankle dorsiflexor muscle strength with excellent reliability. We suggest that our device would be useful in clinical practice to identify subtle but clinically meaningful changes in the ankle dorsiflexor muscle strength.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MO
Contributorship
MK, YO, MO, and KH designed the study; MK, YO, and TA performed the experiments; MK, TA, and MO analyzed the data; and MK and MO wrote the manuscript that was edited by SS and KH. All authors contributed to and have approved the final manuscript.