
Abstract
Introduction
The alignment of a prosthesis is clinically determined based on observations by clinicians and the subjective perception of amputees during gait. However, this process has been reported to be unreliable. Socket reaction moment has been reported to be significantly impacted by alignment changes, but the impact of these alignment changes on other gait parameters is unclear. The aim of this study was to investigate the effects of coronal alignment changes of a transtibial prosthesis on socket reaction moment, spatiotemporal parameters, and perceptions of alignment during gait in amputees.
Methods
Nine individuals with transtibial amputation participated in this study. Socket reaction moment and spatiotemporal parameters (step time, step length, step width, single limb support time, cadence, and gait speed) were measured under nine coronal alignment conditions (angulation: ±3°, ±6°, translation: ±5 mm, ±10 mm, and baseline) using a three-dimensional motion capture system (Vicon) and an embedded load-cell system (Europa™). In addition, subjective perceptions of alignment were examined.
Results
Coronal alignment changes of the transtibial prostheses demonstrated significant changes in socket reaction moment; however, no significant changes were found with spatiotemporal parameters or the amputee’s perception.
Conclusion
Measurement of socket reaction moment, along with the embedded load-cell system, may be a better metric for tuning the coronal alignment of transtibial prostheses compared to spatiotemporal parameters and amputee’s perceptions.
Introduction
The alignment of a transtibial prosthesis is defined as a spatial relationship between a socket and a prosthetic foot. 1 This alignment impacts gait symmetry, comfort, stability, and pressure distribution inside the prosthetic sockets.2–5 In clinical settings, the final prosthetic alignment is more frequently determined by the amputee’s subjective perceptions and the prosthetist’s observations. 6 However, the reliability of this subjective perception of amputees is limited. Boone et al. 7 analyzed the amputee’s perceptions of socket alignment perturbations and concluded that their perception was less reliable for determining alignment except in the coronal plane. In addition, Zahedi et al. 2 suggested that a prosthetist may not be able to reproduce the prosthetic alignment accurately for a single person with transtibial amputation. These studies have demonstrated that current clinical practice of establishing prosthetic alignment, based on amputee’s subjective perceptions and the prosthetist’s observations, may not be reliable and sensitive enough to distinguish appropriate alignment changes.
To address these limitations, several approaches have been reported to measure the forces and moments using load cells embedded in transtibial prostheses during gait.8,9 Boone et al. 10 measured the socket reaction moment (SRM) with force transducers embedded under the transtibial prosthetic sockets and pointed out that the SRM was systematically influenced by prosthetic alignment changes. They suggested that prosthetic alignment could be evaluated objectively with SRM in a clinical setting. Kobayashi et al. 11 investigated the effect of malalignment on both SRM and cadence and found that the SRM was significantly affected, but cadence was not. However, the alignment’s effects on the amputee’s subjective perception and spatiotemporal parameters such as step time and step length have not been adequately investigated. Furthermore, gait analysis studies of pre and post prosthetic alignment changes have primarily been performed in the sagittal plane, and there is a paucity of research examining the coronal plane. 12 Therefore, additional research investigating coronal plane variables may prove to be useful in determining appropriate alignment changes.
Therefore, to address these gaps in the literature, the aim of this study was to investigate the effect of coronal prosthetic alignment changes on SRM, spatiotemporal parameters, and the perception of alignment changes during gait in individuals with transtibial amputation.
Methods
Participants
Demographic information of the participants.

Gait analysis
To measure the spatiotemporal parameters including step time, step length, step width, single-limb support time, cadence, and gait speed, a three-dimensional motion capture system (Vicon, Oxford Metrics, UK) was used. Fourteen-millimeter reflective markers were used to define body segments based on the Plug-in Gait marker set (Vicon, Oxford Metrics, UK). The walkway used for the data capture was 15 m long and was equipped with eight infrared motion capture cameras and two force plates (AMTI, USA) collecting data at 100 and 1000 Hz, respectively. The trajectory and kinetic data were synchronized using Vicon Nexus software (version 1.8.5). In addition, an embedded load-cell system was placed in the prosthesis (Europa™, Orthocare Innovations, USA) and was used to measure SRM. 10 Even though both the motion capture system and the embedded load cell were used to collect data simultaneously, they were not synchronized.
A prosthetist with more than 25 years of experience assembled and adjusted all the experimental prostheses. A slide adapter (4R103, Ottobock, Germany) and Europa™ were placed under the participants’ prosthetic sockets to construct each experimental prosthesis (Figure 1). Before the experiments, the most acceptable alignment of the prostheses was determined based on the prosthetist’s observations and subjective opinions from the participants. This alignment was defined as “baseline.”
An experimental prosthesis used in this study: (a) sagittal view and (b) coronal view.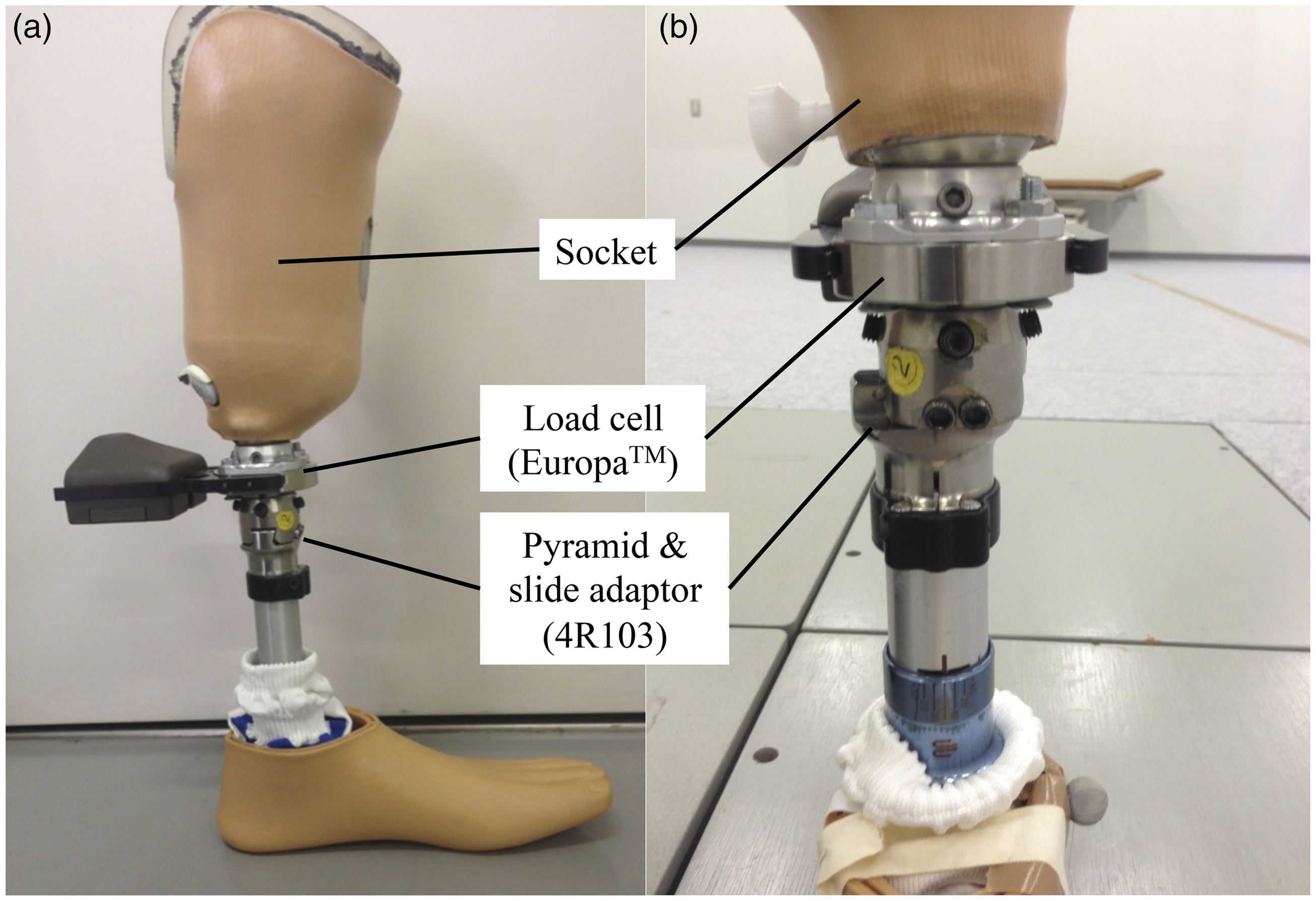
The gait parameters of participants were measured under nine conditions of prosthetic alignment in the coronal plane. These conditions included angulation changes (3° of adduction and abduction, 6° of adduction and abduction), translation changes (5 mm lateral and medial translation, 10 mm lateral and medial translation), and baseline. The ranges of these alignment changes were determined according to a preceding study, 10 and the available ranges imposed by the components were used in the study. These prosthetic components are commonly available and widely used in clinical settings. The ranges of 6° of adduction and abduction and 10 mm lateral and medial translation are within the adjustment ranges of the prosthetic components that we used in the present study. All the alignment changes were carried out using the adjustment mechanism of the 4R103, which allows angulation alignment changes by a pyramid mechanism and translation alignment changes by a slide mechanism (Figure 1). The angulation changes were confirmed using a digital level gauge (DP200Hi, STS Co. Ltd, Japan). The translation changes were confirmed using a ruler.
The participants were instructed to walk in a straight line at their self-selected gait speed. At first, they walked with the baseline alignment on the walkway, and data were collected. Subsequently, the participants were asked to walk under each selected alignment condition in a randomized order for data collection. A subject (ID4) walked only under five conditions (baseline, 6° of adduction and abduction, and 10 mm lateral and medial translation) in a randomized order owing to restriction of time. For each condition, a trial walk of 15 m was carried out only one time to confirm whether the participants could walk safely without fatigue just before each measurement. The participants were not aware of the type, direction, and amount of the alignment change (i.e. angulation or translation, adduction or abduction, medial or lateral translation, 3° or 6°, and 5 or 10 mm). During the data collection, no shoes or footwear were used to avoid their influence on the participant’s gait. 13 Furthermore, having the participants walk without footwear mimicked their daily life of walking without shoes in their home.
After walking in each alignment condition, oral interviews were conducted with the participants about their perception of the alignment changes (“What do you feel about this alignment setting of the prosthesis compared to the baseline setting? If you feel any changes, can you describe them?”). Therefore, perception was defined as an amputees’ feeling of the alignment during gait in this study. The answers were noted and classified into three categories: perceived correctly, perceived incorrectly, and uncertain. The responses were then recorded by the investigator. For example, if the participant responded that “I feel like I am falling to the prosthetic side” when the socket was laterally translated or abducted, it was classified as “perceived correctly.”
Data analysis
The Vicon Nexus software (version 1.8.5) was used to calculate spatiotemporal parameters (step time, step length, single-limb support time, cadence, and gait speed). In addition, step width was calculated as the distance between the heel markers of both legs in the coronal plane during stance. Three gait cycles were extracted from the middle part of each walking trial, and each variable was calculated and averaged across these gait cycles. The data of the coronal SRM were averaged over five gait cycles from the middle part of each walking trial and then divided by the body mass of each participant. The stance phase time was normalized to 100% under each alignment condition. Subsequently, the mean coronal SRM in stance phase was calculated and plotted across participants. The varus moment was defined as negative values of the coronal SRM. The maximum varus moment under angulation and translation alignment changes was extracted under each alignment condition.
For statistical analysis, a linear mixed model was used to analyze the gait parameters after confirming their normality with the Shapiro–Wilk test. A linear mixed model was used because one of the participants was tested under five alignment conditions (resulting in missing data points), whereas others were tested under nine alignment conditions. Gait parameters including maximum varus moment and spatiotemporal parameters, such as step time, step length, step width, single limb support time, cadence, and gait speed, were analyzed under each alignment condition. Paired T-tests with Bonferroni corrections were used for post hoc testing for multiple comparisons. Correlations between the alignment conditions and spatiotemporal parameters and between the alignment conditions and SRM were analyzed using Pearson’s correlation coefficient. The Chi-square test was used to analyze if there were any differences in the subjective perceptions among the different alignment conditions. The significant level was set at P-value < 0.05 for each analysis. SPSS v.19.0 (IBM Corp. Armonk, USA) was used for the statistical analysis.
Results
Spatiotemporal parameters
The spatiotemporal parameters of gait under coronal angulation and translation alignment changes.

N.S., no significant differences.
Socket reaction moment
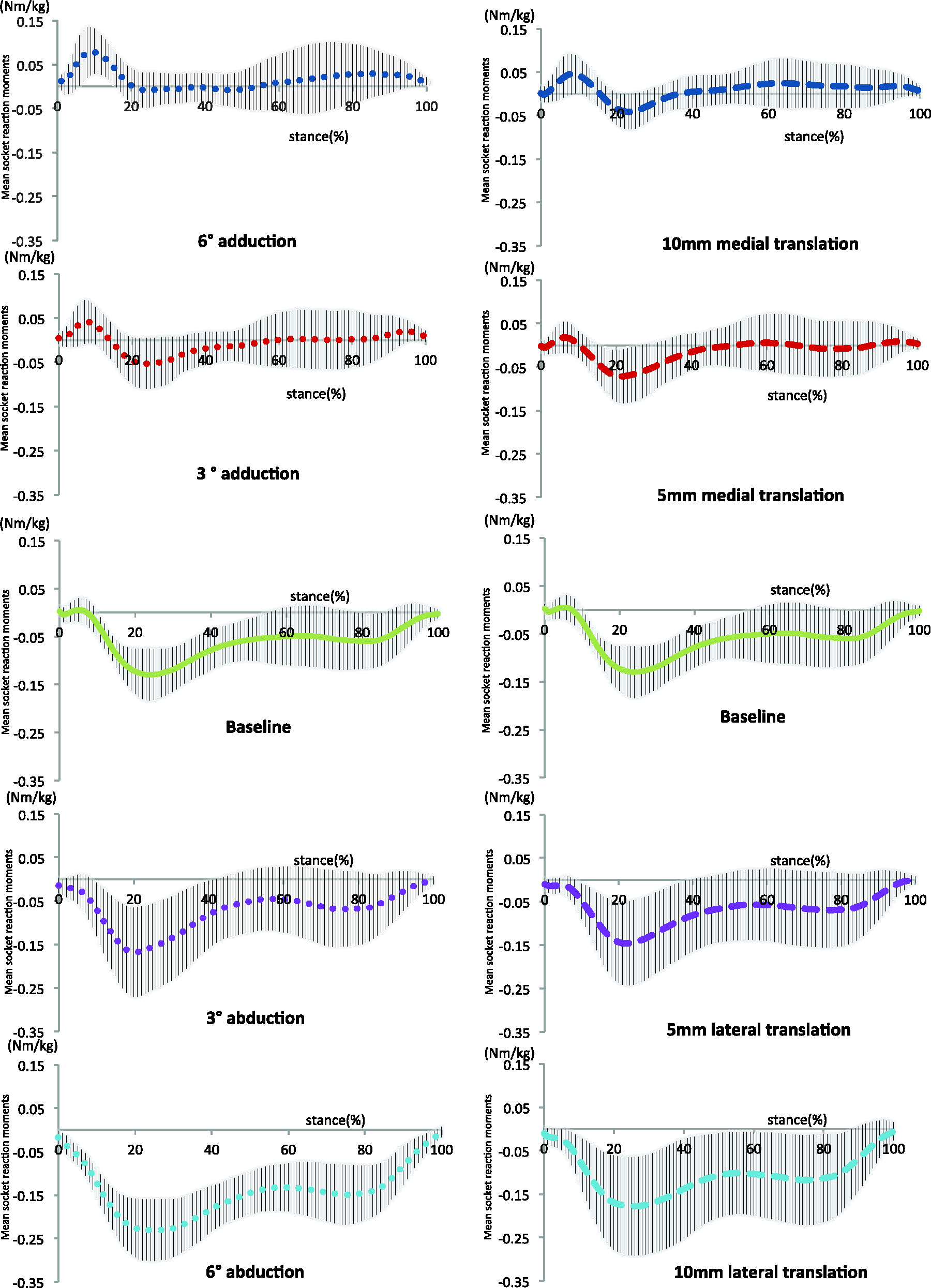
The coronal socket reaction moment (SRM) was significantly (P < 0.001) affected by both angulation and translation alignment changes (Figures 2(a) and 3(a)). The SRM corresponding to each angulation and translation change is shown in Figure 4. The results of post hoc analyses for angulation and translation alignment changes are shown in Figures 2(b) and 3(b), respectively. Significant correlations were found between the maximum varus moment and the alignment changes (r = − 0.96, P < 0.001 for angulation alignment changes and r = −0.99, P < 0.01 for translation alignment changes). The slope of the graph of SRM under the angulation alignment changes [−0.056 (Figure 2(b))] was steeper than that under the translation alignment changes [−0.035 (Figure 3(b))]. Therefore, the angulation alignment changes resulted in more changes in the coronal SRM than the translation alignment changes.
(a) Mean coronal SRM across participants in stance and (b) mean maximum varus moment across participants with standard deviation under angulation changes. An asterisk (*) indicates significant differences (P < 0.05). (a) Mean coronal SRM across participants in stance and (b) mean maximum varus moment across participants with standard deviation under translation changes. An asterisk (*) indicates significant differences (P < 0.05). Mean SRM under each alignment condition. The shaded area indicates standard deviations during stance (per % stance).

Subjective perceptions
Perception of coronal angulation and translation alignment changes.

N.S., no significant differences. Note: Each number indicates the number of responses in perception of coronal alignment changes among the participants.
Discussion
This study investigated the effect of coronal prosthetic alignment changes on the SRM, spatiotemporal parameters, and perception of alignment during gait in individuals with transtibial amputation. The results of this study demonstrated that coronal alignment changes significantly impacted SRM, but spatiotemporal parameters and amputee’s subjective perceptions were not affected. Therefore, these findings suggested that the embedded load-cell system placed in the transtibial prosthesis may be potentially useful in assisting in the fine-tuning of the alignment in the coronal plane.
With coronal alignment changes, there were no significant differences in spatiotemporal parameters. Thus, the observation of these parameters may not necessarily contribute to establishing the ideal coronal alignment of transtibial prostheses. Pinzur et al. 14 suggested that no subjects could walk adequately with 15° malalignment. If the angulation changes were more than 6°, some of these spatiotemporal parameters may have been affected. In clinical settings, it would be rare to evaluate prosthetic gait with a malalignment of more than 6° as long as the bench and static alignments are set in a proper manner. The participants had long-term experience (5 − 48 years) of walking with prostheses. During this time, they most likely have had ample opportunity to walk as symmetrically as possible under malaligned conditions. This prosthetic malalignment could lead to compensatory motion, such as lateral trunk bending during gait. One of the possible causes of lateral trunk bending at mid-stance toward the prosthetic side is because of an excessive outset of the prosthetic foot. 15 Some compensatory motions may occur to maintain balance in gait. Further investigation would be needed to clarify the effects of alignment changes on compensatory movements in amputee’s gait.
Although no significant changes in the spatiotemporal parameters were found among the alignment conditions, step width demonstrated significant correlations with the coronal socket alignment changes. The step width for normal walking in able-bodied individuals is reported to be in the range of 50–130 mm. 16 The step width for the baseline alignment in this study was 136 mm. Under 3° and 6° abduction, the step width was within the range (114 mm and 112 mm, respectively). A wider step width may increase lateral displacement of COM and metabolic cost.17,18 Additional studies with a larger sample size are needed to clarify how step width is related to overall gait efficiency and performance in amputees with transtibial prosthesis.
Since the gait speed and cadence were not significantly affected by the alignment changes, the changes in the coronal SRM appeared to be most likely caused by alignment changes. SRM under each condition showed the same systematic trends in correspondence to alignment changes as other studies.10,19 This outcome indicated that SRM may be useful to evaluate different prosthetic alignment conditions in the coronal plane under a constant gait speed. The mechanism of the prosthetic foot displacement in the coronal plane is different between translation and angulation alignment changes. Based on the illustration in Figure 5, the horizontal displacement was 25.3 ± 2.60 mm for the 6° angulation and 12.7 ± 1.30 for the 3° angulation, which was larger than that for 10-mm translation. This explains why the 6° angulation alignment changes affected the SRM more than the 10-mm translation alignment changes. A review study on transtibial prosthetic alignment pointed out that the pressure distribution in a prosthetic socket may be more sensitive to the angulation changes than to the translation changes because of the alteration in the effective limb length.
3
However, the vertical displacement by the 6° angulation alignment changes was 1.3 ± 0.1 mm and by the 3° angulation alignment changes was 0.33 ± 0.0 mm. Therefore, the change in the effective limb length caused by the angulation changes appeared to be very small (Figure 5).
An illustration explaining the horizontal and vertical displacement of the prosthetic foot under angulation alignment changes.
There was no significant effect by the alignment changes on the subjective perception of amputees. This implies that the subjective perceptions may not precisely reflect alignment changes. Boone et al. 7 used a software similar to the visual analog scale to quantify the perception of prosthetic alignment and suggested that the amputees might be able to perceive coronal angle alignment changes. In this study, only a simple question was asked. The participants expressed their perception verbally and not quantitatively. The process to classify the participants’ verbal expression into one of the three categories was performed subjectively. Therefore, errors could have been made both in perception and expression by the participants and in interpretation by the investigator.
There were some limitations to the present study. It was performed using a small sample size (with nine participants). The baseline alignment was determined according to the current clinical practice and it was not quantified. There were some demographic biases (i.e. only one female, no participants in 20 s, and the cause of amputations). The cause of amputation of the participants varied from trauma to diabetes. This variation might contribute to the variability of sensory abilities among the participants in detecting alignment changes. Finally, the results show immediate effects and long-term effects are still unknown.
Conclusion
This study focused on the effect of coronal alignment changes on SRM, spatiotemporal parameters, and subjective perceptions. The coronal alignment changes, both angulation and translation, significantly affected SRM (i.e. maximum varus moment), but they did not affect spatiotemporal parameters or subjective perception. This implies that the embedded load cell in the transtibial prosthesis could potentially contribute to the evaluation of prosthetic alignment in the coronal plane. Further studies are needed to explore optimal alignment using the embedded load cell in transtibial prostheses.
Footnotes
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HH is an employee of Pacific Supply Co., Ltd that distributes Europa™ in Japan. TK was an employee of Orthocare Innovations, the manufacturer of Europa™.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
HH
Contributorship
HH researched literature, conceived the study, and recruited the participants. TK was involved in literature review, protocol development, and data analysis. FG was involved in data analysis. MK and KO were involved in protocol development, gaining ethical approval, apparatus management, and data analysis. HH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
We appreciate the technical advice and support of Satoshi Okahara of Osaka General Medical Center, Japan, Wayne Daly of Seattle Orthotics and Prosthetics, USA, and K. Bo Foreman of The University of Utah, USA.