
Abstract
Background
Grasping and manipulating objects are common problems for children with hemiplegic cerebral palsy. Multichannel-functional electrical stimulation may help facilitate upper limb movements and improve function.
Objective
To evaluate the feasibility of multichannel-functional electrical stimulation to improve grasp and upper limb function in children with hemiplegic cerebral palsy to inform the development of a clinical trial.
Methods
A prospective pre-/post-test/follow-up (six months) design with three children, aged 6–13 years, was used. Multichannel-functional electrical stimulation (mFES) was applied to the hemiplegic upper limb for up to 48 sessions over 16 weeks. Feasibility indicators included recruitment of participants and adherence rates, safety, and discomfort/pain. Effectiveness was assessed using the grasp domain of the Quality of Upper Extremity Skills Test, and other secondary clinical outcome measures with “success” criteria set a priori.
Results
Participant recruitment target was not met but adherence was high, and multichannel-functional electrical stimulation was found to be safe and comfortable. Of the three participants, two improved in grasp at post-test, whereas one child’s ability deteriorated. Only one child met success criteria on most outcomes at post-test.
Conclusions
Feasibility indicators met success criteria, except for participant recruitment. Treatment effectiveness was mixed. A future case comparison investigation with a larger but more selected sample is suggested.
Keywords
Introduction
Cerebral palsy (CP) is a neurodevelopmental condition and a common cause of childhood physical disability,1,2 with hemiplegic cerebral palsy (HCP) being one of the most prevalent forms, having an estimated prevalence ranging from 31% of cases in Canada 3 and 35% in other parts of the world.4,5 HCP affects one side of the body, typically with marked involvement of the upper limb (UL), and is associated with reduced selective motor control, weakness, decreased sensation, developmental disregard, and hypertonia. 6 Together these impairments limit performance in functional activities, as confirmed by a child's inability to achieve basic day-to-day activities 7 (e.g. drinking, eating, accomplishing self-care, or dressing), and their participation at home, school, and later vocational roles. 8 However, studies have shown that hand function of the involved limb is indeed amenable to treatment in these children. Some of the most promising treatment strategies for HCP, such as constraint-induced movement therapy (CIMT) 9 and bimanual training 10 involve repetitive task-specific practice. Yet, the retention of the therapeutic gains achieved from these interventions and how their positive effects translate to activities of daily living (ADLs) remain elusive. 11 Interestingly, functional electrical stimulation (FES) is another form of therapy that also involves task-specific functional training, and one which has been used for UL retraining in the clinical setting for adult stroke rehabilitation. 12 There is a gap in our understanding of the effectiveness of FES to improve hand function in children with HCP as compared to the current standard of CIMT/bimanual training.
FES involves the transcutaneous administration of electrical impulses to muscles to produce a contraction and obtain functionally useful movement. 13 FES emphasizes active (individual initiated), repetitive, task-specific movement of the paretic arm and hand and has been shown to increase function, range of motion (ROM), 14 enhance muscle strength, 15 and improve tone 16 of the UL in individuals with neurological conditions, such as stroke 17 and spinal cord injury.18,19 To date, studies have shown that FES therapy can lead to recovery of UL function, specifically, improvements in dexterity, ROM, and ADLs have been shown in adults with subacute stroke.12,20–22 Benefits of increased limb awareness 23 and improved sensory function 24 have been reported as well.
Previous approaches using FES for the UL usually targeted one or two muscles only. 25 However, advances in FES systems with multichannel capabilities (mFES) are unique in that they can stimulate and coordinate the synchronous activity of several muscles, thereby facilitating a wide variety of complex functional UL movements, such as reaching, grasping, and manipulating objects.19,25–27 FES paired with intense practice is thought to be crucial for motor learning and may lead to the restructuring of neural connections (i.e. neuroplasticity). 17 Recently, mFES has been found to be effective in improving arm and hand function (including better voluntary grasping function) in adolescents with hemiplegia secondary to an acquired stroke, with the mFES therapy provided in the chronic stage at least one year after the vascular injury. 13 Nevertheless, the use of mFES in individuals with CP has seldom been explored.
There are only a few published studies employing therapeutic FES in CP, and those are mainly focused on gait and lower limb rehabilitation. 28 This is surprising because children with congenital hemiplegia often share a similar underlying mechanism of injury 29 as those adults with stroke who have benefited from FES. Motivated by a prior successful study showing that FES therapy can improve voluntary grasp and hand function in severe pediatric chronic stroke patients, this was a proof of concept study that aimed to assess the feasibility of UL mFES training in children with HCP and identify shortcomings to support the potential development of a randomized controlled trial (RCT). Specific objectives were to evaluate: (1) feasibility as measured by participant recruitment and adherence rates, safety, and discomfort/pain; (2) treatment effectiveness as measured by the Quality of Upper Extremity Skills Test (QUEST) 30 grasp domain score (and other secondary outcomes) at post-test; and (3) maintenance of any clinical improvements six months after mFES was discontinued.
Methodology
Design and study setting
This study employed a prospective pre-/post-test/follow-up design in a pediatric rehabilitation hospital setting. All participants received up to 48 mFES therapy sessions applied to the hemiplegic UL. Assessments were made at pretest (i.e. before mFES), post-test (within one week after completion of the last therapy session), and follow-up (six months after the intervention period had ended). The protocol was approved by the Holland Bloorview Research Ethics Board (REB No. 15-549). The study was registered with ClinicalTrials.gov (Identifier NCT03016923). Written informed assent/consent was obtained from all participants/parents.
Subject selection
Eligibility criteria.

CIMT: constraint-induced movement therapy; FPS-R: Faces Pain Scale-Revised; HCP: hemiplegic cerebral palsy; mFES: FES systems with multichannel capabilities.
A child was excluded from the study if three or more of his/her muscle groups were deemed “unresponsive,” discomfort/pain rating score ≥8 on the Faces Pain Scale-Revised (FPS-R) 31 was reported upon receiving stimulation to any muscle, attended less than 36 (out of 48) mFES therapy sessions, developed new-onset seizures, and/or received any other form of therapy or treatment (i.e. a cointervention) for the UL during the intervention period.
Muscle responsiveness testing
Details of muscle responsiveness testing procedures.
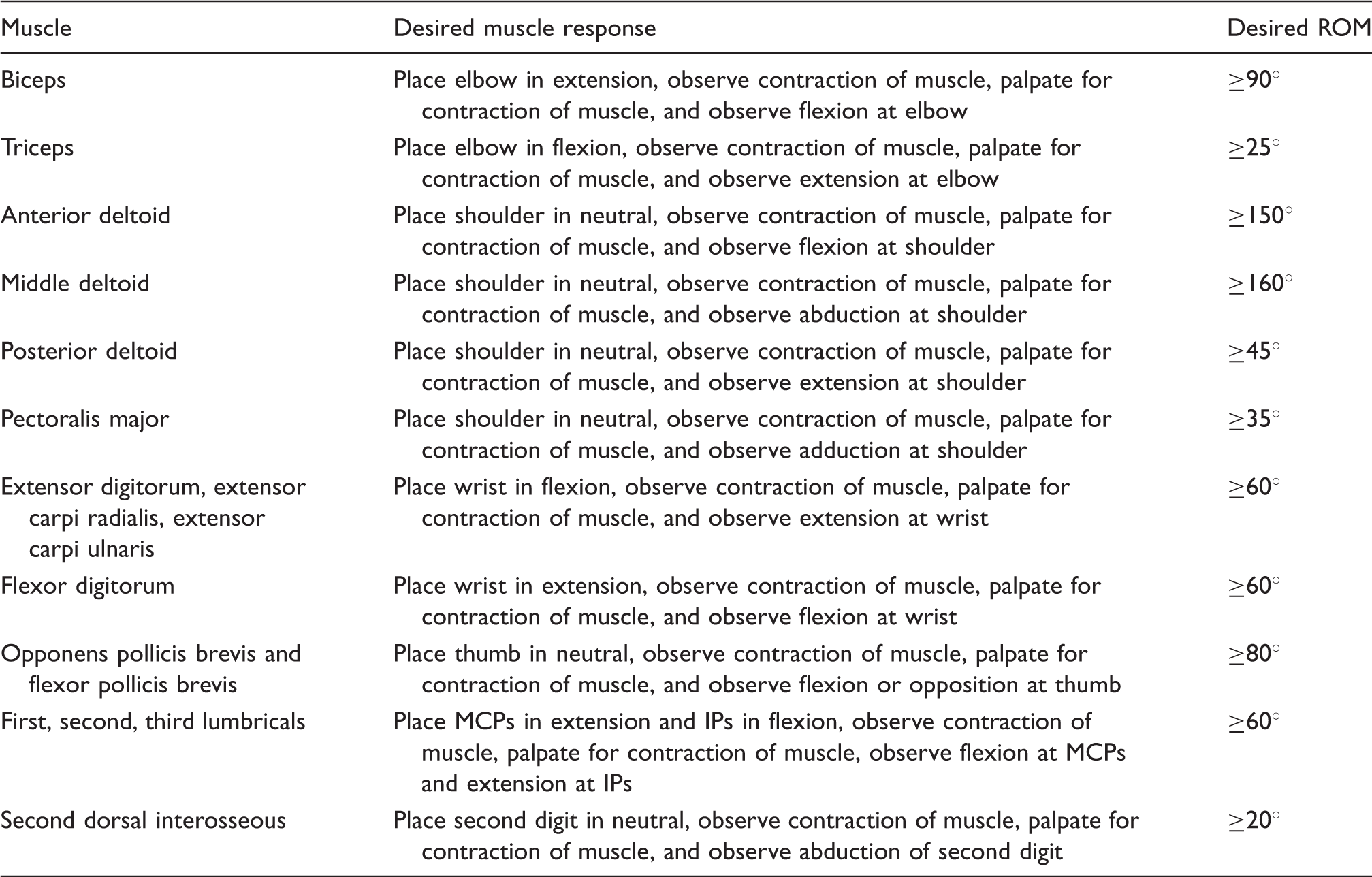
IPs: interphalangeal joints; MCP: metacarpophalangeal joints; ROM: range of motion. 32
Feasibility indicators
A feasibility framework was established measuring recruitment rate, adherence to the intervention and data collection times, safety, and discomfort/pain. Each indicator was evaluated as follows:
Participant recruitment rate
Aimed to have at least 40% of individuals who were approached and met eligibility criteria consent to participate. This rate was deemed satisfactory based on a study that showed a participant recruitment rate of 37.8% in children with CP aged 4–16 years through a combined recruitment approach of clinic- and population-based case register populations. 33
Adherence rate
Aimed for 100% of participants to complete at least 36 therapy sessions over 16 weeks, as well as completion of the QUEST grasp at both pre- and post-test assessments. The targeted treatment regimen remained at 48 sessions in total based on other studies showing it led to positive outcomes in both chronic severe pediatric and adult stroke patients.13,16,20,34 However, a range of 36–48 sessions was considered acceptable to accommodate any scheduling conflicts or missed sessions. Adherence to the data collection procedures was set to ensure treatment response with regards to grasping ability could be evaluated.
Safety
A serious adverse event (SAE) was considered an event that was associated with the intervention and that resulted in a serious deterioration in state of health or death. Thus, the study aimed for no SAEs associated with the intervention. Any adverse events or unintended effects detected were also documented according to REB processes.
Discomfort/pain
Some studies have reported several dropouts because children with CP were unable to tolerate the FES stimulation.35,36 Therefore, discomfort and/or pain was evaluated once a week throughout the intervention period using the FPS-R. A rating score of ≤6 (out of 10) was determined to be the cutoff value for what was considered a comfortable session. Overall, the intervention was deemed comfortable if ≥95% of the reports had a rating score of ≤6 for all treatment sessions.
Treatment effectiveness and clinical outcome measures
The use of mFES was focused on augmenting hand function, mainly related to grasping and manipulating objects. Thus, the evaluation of treatment effectiveness was measured using the QUEST grasp domain as the primary clinical outcome and was supplemented by secondary outcome measures assessing other aspects of UL function. For all clinical outcome measures, the minimally clinically important difference (MCID) was used as a benchmark to interpret individual changes observed following the mFES intervention. If the MCID was not yet established, a threshold termed clinically important difference (CID) was set based on the judgment of the study’s clinician scientists and therapists as to the minimum value of a clinically meaningful change. The two occupational therapists who administered the mFES also acted as nonblinded assessors to evaluate all clinical effectiveness outcomes. Evaluators were asked to alternate between assessments for each child (i.e. neither completed two consecutive assessments) in efforts to reduce potential biases. Treatment outcomes for this study were as follows:
Primary outcome measure
The primary outcome measure of interest was unimanual hand grasp using the score of the QUEST grasp domain 30 for the involved hand at post-test. The QUEST grasp domain evaluates a child’s usual performance in grasping activities of everyday objects as well as the posture of the head, trunk, and arm during these activities. For the QUEST grasp, a positive change of at least five points was determined to be clinically meaningful. This value was set based on a change score of 4.89 units in the QUEST total score (i.e. the score including all four domains) which was considered to reflect a genuine improvement in the child’s manual function and positive treatment response in a neurodevelopmental therapy and casting trial.37,38
Secondary outcome measures
The remaining three additional domains of the QUEST: dissociated movement, weight bearing, and protective extension were also assessed for the hemiplegic side. Each domain assesses several movements using a dichotomous scale (yes/no). Scores are calculated as percentages for each domain, summed and divided by the total number of domains to obtain the QUEST total score, which ranges from <0 (if sitting postures during grasp items are “atypical”) to 100. The QUEST 30 is a condition-specific standardized functional test that has been validated for children with CP aged 18 months to eight years, 39 with established psychometric properties including responsiveness 40 (MCID: positive change of at least five points37,38). The Canadian Occupational Performance Measure (COPM) 41 identified three functional goals by parents or other caregivers as proxies involving hand use for each child. The mean rating (1–10) of the performance on the defined goal or task and satisfaction with that performance were documented (MCID: positive change of at least two score units 42 on mean performance and/or satisfaction ratings). The COPM is reported to be a valid, reliable, and responsive measure.43,44 The Children’s Hand-Use Experience Questionnaire (CHEQ) 45 assessed child/parental report of the child’s typical hemiplegic hand usage in regular bimanual activities. Responses on the CHEQ were used to calculate the percent of activities performed independently with the assistance of the paretic hand (used as either support or grip) from the activities selected as being “applicable” to the child out of 29 (CID: 10% positive change in percent of bimanual activities performed independently). The Jebsen–Taylor Hand Function Test (JTHFT) 46 was used to assess unimanual grasp and release speed and manual dexterity. A total score (in seconds) for each hand was calculated from the sum of the individual scores for each of the six timed subtests, after excluding the writing subtest due to the age of some participants (MCID: at least 6 s decrease in total score 47 ). Grip strength was measured in millimeters of mercury (mmHg) using a modified sphygmomanometer 48 with the forearm cuff bent into thirds and positioned inside a cloth pouch, and the gauge pumped up to 20 mmHg. The child remained in the sitting position and was asked to exert as much force as possible by squeezing the pouch. The mmHg displayed on the gauge was used to determine the grip strength score for each trial. The mean of three successive trials was calculated (MCID: positive change of at least 10 mmHg48,49). Wrist extension active range of motion (aROM) 50 of the involved limb in the sitting position with forearm in neutral and resting on a table was assessed. The wrist joint was aligned with a goniometer axis, the child was instructed to move the wrist to maximal extension, and the maximum extension range value (in degrees, with fingers, both flexed and extended) above the table surface was measured (CID: positive change of at least 10° in joint angle). The Australian Spasticity Assessment Scale (ASAS) was used to evaluate muscle-specific tone of the elbow flexors and wrist flexors in the paretic UL (CID: at least one score unit decrease 51 ). Joint position sense (proprioception) in the transverse plane (forearm pronation) was evaluated with a series of 10 proprioceptive-matching trials using targets located around the axis of a custom-built semigoniometer. 52 Testing involved obscuring of the forearm while target angles remained visible. The orientation angle achieved (i.e. the performance in degrees) and the direction (pronation/supination) and mean magnitude (in degrees) of error between the performance and the 10 target locations were recorded for each UL (CID: a 10° decrease in mean magnitude of error). A stereognosis test 53 was used to identify nine common objects. One set of objects was placed to the side of the child within the child’s view minimizing any errors due to incorrect naming, and another identical set was used for the child to manipulate using each hand. The vision of the testing hand was occluded with a curtain. The stereognosis score was calculated as the number of correctly identified objects out of a maximum of nine (CID: correct identification of three or more additional objects from baseline). The two-point orientation discrimination (2POD) 54 test was used to measure tactile spatial acuity in the index finger of both hands. Twenty-five trials were tested for each hand using a two-interval two-alternative forced-choice up-down transformed procedure version of the task55,56 at each of several tip separations using a digital caliper. A two-down one-up adaptive staircase protocol 56 was used to adjust the caliper (with a 0.2 mm step size) and tip separations 2–25 were averaged and reported as the participant’s spatial acuity threshold for the paretic hand (CID: a 1 mm decrease in calculated tactile spatial acuity threshold).
The pretest assessment also involved gathering demographic variables including gender, age, and side of involvement. Brain injury patterns were collected from available neuroimaging (MRI or CAT scan) data, and the child’s ability to manipulate objects in daily activities was classified using the Manual Ability Classification System (MACS), 57 as well as the ability to carry out self-initiated movements related to sitting and walking with the Gross Motor Function Classification System (GMFCS). 58
In addition, an 18-item feedback questionnaire was adapted from an instrument used in a previous study and administered at post-test, 59 to investigate perceptions of the mFES intervention. The questions pertained to the stimulation itself, the tasks that were paired with mFES, the child’s perceived awareness of their paretic limb, recommended use of mFES to others, and willingness to continue treatment. The response to each question was scored using a five-point Likert scale, ranging from “Strongly Disagree” to “Strongly Agree.” Together, the child and at least one parent agreed upon each rating.
Intervention
The mFES was delivered during 1 h therapy sessions three days a week, over approximately 16 weeks, for up to a maximum of 48 sessions, by two trained occupational therapists. Transcutaneous mFES was applied targeting the motor points of muscles in the involved UL. The MyndMove™ (MyndTec Inc., Mississauga, ON, Canada) programmable stimulator was used, employing up to eight channels and four sizes of skin electrodes producing low-frequency currents to assist in the performance of functional, repetitive, and goal-oriented activities using real objects. The experimental setup is presented in Figure 1. The participant was seated with the arm unsupported and the therapist triggered the stimulation using a foot switch. The stimulation parameters used are presented in Table 3.
Schematic representation of the mFES system and participant setup during a therapy session. The participant sat in chair with arm unsupported and electrodes were positioned on various UL muscles. Stimulation parameters. CFTs: constant frequency trains; circ: circumference; mFES: FES systems with multichannel capabilities.

The mFES system had 17 “protocols” (i.e. preprogrammed stimulation patterns) that were designed to evoke desired motor behaviors such as palmar grasp and lateral pinch in adult stroke patients as outlined by the manufacturer. 60 These protocols were used in this study without any modification. Current intensity was set for each muscle at the lowest level sufficient to elicit a visible motor response, and when the child reported perceiving a tingling feeling that felt comfortable.
Like with the muscle responsiveness testing, stimulation was started at 0.05 mA and increased using the smallest allowable increment (0.05 or 0.1 mA depending on the muscle) for each channel and was adjusted at every therapy session before commencing and during (if necessary) training with each protocol, according to participant’s comfort and muscle activity. Overall, therapists aimed to administer three to four protocols within each session, repeating the same motion 10–15 times before moving onto the next protocol, and with electrodes requiring approximately 5–10 min to don and doff. Stimulus intensity (in mA) for each channel, number of protocols, and the number of repetitions performed as well as total time spent on each protocol were recorded by the device.
The mFES therapy first focused on reaching with the paretic arm and hand forward and sideways with finger extension. After participants achieved this, the intervention focused on fine motor skills, and different protocols were carried out to perform various forms of grasping (palmar grasp, lateral pinch, pinch grasp, lumbrical grip, lumbrical and palmar grasp, and tripod grasp), side and forward reach, and wrist extension involving tasks using small objects of various sizes. The participants were first asked to attempt to carry out the task on their own, making sure they had reached their limit of voluntary ROM before attempting the same movement using the stimulation. Protocols were paired with unimanual game-like activities to keep the child motivated. Exercises were goal oriented and primarily focused on reach-to-grasp movements, combining different objects to play games (e.g. make a puzzle, “concentration,” “build a pie,” or “feed the alligator”). As the child completed more sessions, he/she may have gained better voluntary control, and lower amplitude stimuli may have been enough to produce the desired functional movement.
Data processing and analysis
Feasibility indicators for recruitment, adherence, safety, and discomfort/pain were evaluated based on the criterion established and considered either “successful” or “unsuccessful.”
Likewise, a similar framework based on threshold criteria was used to interpret the evidence for positive treatment response (i.e. effectiveness) of mFES. The MCID (where available) or CID for each clinical effectiveness outcome measure was used to determine if the change in scores at post-test and at follow-up were clinically meaningful and in a positive direction. To assess the robustness of the study findings, the percentage of the effectiveness outcomes meeting the MCID/CID criteria for positive treatment response was then calculated as an overall marker of therapy effectiveness. If a child met or exceeded the MCID/CID criteria in the positive direction in 50% or more of the treatment outcomes (including the QUEST grasp score) at post-test, they were designated as a positive responder and mFES was considered effective. Improvement in scores between pretest and follow-up was used to identify whether any observed gains had been maintained at six-month follow-up.
Means and standard deviations were calculated for the number of protocols and repetitions performed at each therapy session. To explore trends in the amplitudes required as the child progressed through the intervention period, a standard regression curve (using the least squares fit for a line), slope, and the square regression coefficient were generated from the mean amplitudes calculated from all the protocols that were administered each week. Results of the feedback questionnaire were also collated and summarized.
Results
Participant demographics
Three children enrolled in the study. Case 1 was a six-year-old female, Case 2 was a nine-year-old female, and Case 3 was a 13-year-old male. All children in the sample were independent ambulators (GMFCS I) and could complete some manual activities without assistance (Case 1 was MACS level I, and Cases 2 and 3 were MACS level II). All had right-sided HCP. The following brain imaging results were obtained from their health records: Case 1, middle cerebral artery (MCA) injury including lateral lenticulostriate artery and associated basal ganglia injury; Case 2, MCA injury; and Case 3, a left-sided periventricular venous infarction.
Feasibility indicators
Participant recruitment rate
Twelve potential subjects were identified from the case records of the therapists, and all were approached for recruitment into the study. Eight (67%) families declined to participate, with seven reporting a high burden of time commitment to attend the number/frequency of therapy sessions, and one was not interested in participating in research. Four (33%) children were initially invited to do the pretest and muscle responsiveness evaluation in the hospital, but one child suffered a new seizure shortly before the scheduled visit and consequently had to be excluded. Altogether, 3/12 families agreed to participate, resulting in a recruitment rate of 25%.
Adherence rate
These children did 2.84 (2–4) sessions on average every week. Cases 1 and 2 completed a total of 47 sessions and Case 3 completed 45 sessions. However, despite being able to meet the total number of required sessions, the mFES regimen was briefly interrupted on one occasion for Case 1 and Case 3, and two times for Case 2 due to family holidays and/or other personal commitments. Treatment suspension ranged from seven to 14 consecutive days. All three (100%) participants completed pretest, post-test, and follow-up assessments.
Safety and discomfort/pain
There were no reports of any SAEs that occurred during the study protocol. On one occasion, a participant perceived the stimulation as being too intense and painful and the stimulation was immediately stopped. It was discovered that one of the electrode cables was poorly connected to its port located at the back of the device. Except for this one episode of electrode cable disconnect, all children rated the intervention as being comfortable (i.e. ≥95% of sessions had FPS-R score ratings ≤ 6).
mFES parameters
The number of muscles stimulated per session varied from four to eight, depending on the stimulation protocol(s) employed. The mean number of protocols used per session was 2.06 ± 0.48 (mean ± SD) for Case 1, 2.68 ± 0.73 for Case 2, and 3.33 ± 0.95 for Case 3. The mean number of repetitions completed (all protocols combined) per session was 17.80 ± 8.19 for Case 1, 14.78 ± 5.77 for Case 2, and 15.58 ± 6.09 for Case 3. Desired functional movements were achieved using amplitudes that ranged from 0.1 to 2.55 mA.
At pretest, Case 1 demonstrated the ability to pick up a small object with a palmar grasp with their hemiplegic hand. Both Case 2 and 3 were unable to grasp a small object with their hemiplegic hand at pretest. However, when assisted by the mFES, all children could grasp a small object with a pincer grasp while receiving the stimulation. Different grasps could also be achieved during mFES (e.g. radial digital, static and dynamic tripod, and digital pronate grasps).
Treatment effectiveness outcomes
Individual participant pretest scores and summary of treatment response as assessed using the clinical outcome measures at post-test and follow-up.

aROM: active range of motion; ASAS: Australian Spasticity Assessment Scale; CHEQ: Children’s Hand-Use Experience Questionnaire; CID: clinically important difference; COPM: Canadian Occupational Performance Measure; EF: elbow flexors; FE: fingers extended; FF: fingers flexed; JTHFT: Jebsen–Taylor Hand Function Test; MCID: minimally clinically important difference; QUEST: Quality of Upper Extremity Skills Test; 2POD: two-point orientation discrimination; WF: wrist flexors.
Data cells shaded in  indicate outcomes where change in scores post-test/follow-up (compared to pretest) met MCID/CID criteria in a positive direction (i.e. improvement). Data cells shaded in
indicate outcomes where change in scores post-test/follow-up (compared to pretest) met MCID/CID criteria in a positive direction (i.e. improvement). Data cells shaded in  indicates outcomes were change in scores post-test/follow-up (compared to pretest) met MCID/CID criteria in a negative direction (i.e. deterioration). Data cells shaded in
indicates outcomes were change in scores post-test/follow-up (compared to pretest) met MCID/CID criteria in a negative direction (i.e. deterioration). Data cells shaded in  indicate scores did not change.
indicate scores did not change.
Follow-up data from Case 2 was not usable due to CIMT cointervention which occurred during this follow-up period.
COPM score ratings on the performance and satisfaction for one goal were unattainable at post-test because the child did not attempt to work on the functional task established by that goal prior to this assessment. Thus, mean scores were calculated based on the remaining two (rather than three) goals.
Case 1. At post-test, clinically meaningful improvements were observed on three (21%) outcomes, including better grasping ability (QUEST grasp score increased +14.8 points), grip strength (increase in mean score of +12.4 mmHg), and stereognosis (+7 objects). In contrast, a clinically significant decline was noted on five (36%) outcomes at post-test, including dissociated movements, weight bearing, and protective extension (QUEST total score decreased −42.1 points); functional goals (COPM average satisfaction rating decreased −2.4 points); bimanual performance (CHEQ percentage of bimanual activities performed independently decreased by −17.3%); and wrist aROM (child was unable to activate wrist extension with both fingers flexed and extended). This child could not complete the JTHFT within the allotted time during all three testing sessions. The ASAS grade was zero at pre-/post-test and follow-up as the child had hypertonia (i.e. increased muscle tone) attributable to dystonia rather than spasticity. Meaningful gains compared to pretest were observed in five (36%) outcomes at the six-month follow-up, with two outcomes showing maintenance of benefits, including the QUEST grasp (+7.4 points), and stereognosis (+4 objects), whereas new improvements appeared on the QUEST total (+10.7 points) and wrist extension aROM with fingers flexed (+15°) outcomes. Two (14%) outcomes met MCID/CID criteria in the negative direction, including grip strength (–14.0 mmHg), and wrist aROM with fingers extended (not able to activate wrist extension) at follow-up.
Case 2. At post-test, clinically meaningful improvements were observed on five (36%) outcomes, including better bimanual performance (CHEQ percentage of bimanual activities performed independently increased by +17.6%), unimanual capacity (total time to complete the JTHFT was reduced by −41.5 s), grip strength (+15 mmHg), wrist extension aROM (+25°), and spasticity grading (ASAS score for the wrist flexors showed a −1 score unit reduction). In contrast, a significant decline was observed in three (21%) outcomes, including deterioration in grasping ability (QUEST grasp decreased by −7.45 points), mean performance rating of functional goals (COPM mean performance rating decreased −4.5 points), and spasticity grading (ASAS score for the elbow flexors increased +1 score unit) at post-test. Both stereognosis and QUEST total score did not change at post-test. Follow-up data were not usable for this participant who went on to receive two weeks of CIMT between post-test and follow-up assessments.
Case 3. At post-test, clinically meaningful improvements were observed on 11 (79%) outcomes, including better grasping ability (QUEST grasp increased +7.4 points), dissociated movements, weight bearing and protective extension (QUEST total increased +15.4 points), functional goals (COPM mean performance and satisfaction ratings increased +3.7 points and +3.6 points, respectively), unimanual capacity (total time to complete the JTHFT was reduced by −46.2 s), grip strength (+11 mmHg), wrist extension aROM (+72°), spasticity grading (ASAS had a −2 score unit reduction for both elbow and wrist flexors), proprioception (24.9° reduction in magnitude of error), and tactile spatial acuity (2POD test score decreased −1.1 mm). No outcomes met criteria for a significant decline at post-test. Stereognosis remained intact at all assessment times. Meaningful gains were maintained in seven (50%) outcomes at follow-up, including the QUEST total (+11.1 points), COPM performance (+3.6 points) and satisfaction ratings (+2 points), JTHFT (–36.8 s reduction in total test completion), grip strength (+22 mmHg), wrist extension aROM (+60°), and proprioception (–29.4° reduction in magnitude of error). One outcome, the QUEST grasp score declined (–22.3 points) from pretest to follow-up.
Intervention goals determined by the Canadian Occupational Performance Measure (COPM) and corresponding goal performance and satisfaction scores.

COPM score ratings on the performance and satisfaction for this goal were unattainable at post-test because the child did not attempt to work on the functional task established by that goal prior to the post-test assessment.
Feedback questionnaire
Overall, participants and parents found the therapy sessions enjoyable, comfortable, and shared positive views for the intervention procedures, but most were dissatisfied with the amount of time needed to complete the prescribed therapy dosage. Further, two children said they would not recommend mFES to others, but would be willing to continue with the intervention themselves.
Discussion
To our knowledge, this study was the first to evaluate the feasibility and explore the effectiveness of UL training with an eight-channel mFES system in children with HCP. Within the feasibility framework that assessed the potential of developing an RCT, it was found that criteria for adherence, safety, minimal discomfort/pain were met successfully. However, participant recruitment targets were not met.
The recruitment strategy used was limited by a small sample pool and this study was met with high refusal rates. The most common reason for nonparticipation was the high frequency of the therapy and amount of time needed to travel to the study site. This is a critical feasibility limitation because failure to reach a sufficient sample size for statistical power is a key determinant in the success of an RCT. Besides exploring a multifaceted recruitment approach using multiple sites, providing rehabilitation in the home-based setting, could be an approach to enhance recruitment rate. Developing an mFES home therapy program consistent with research protocols could be effective while alleviating the time constraints associated with living too far away, traveling difficulties, and treatment interferences because of school, work, and other responsibilities. Indeed, a recent study successfully implemented an FES program that was delivered at the child’s home by the mother and supervised remotely by a therapist via video conference. 61
All participants completed the intervention regimen without any SAEs. Generally, mFES was also comfortable except for a single session where the stimulation felt painful secondary to a loose connection. Participants also showed good adherence to both completing the outcome assessments and completing the required number of therapy sessions, and follow-up rates were good.
Assessment for treatment effectiveness considered both motor and sensor function, and most outcome measures had excellent psychometric properties (some with established responsiveness to change), were clinically relevant, and some were also specifically designed for this patient population. More specifically, treatment effectiveness evaluated grasp (QUEST grasp), quality of movement (QUEST total), functional goals (COPM), bimanual performance (CHEQ), unimanual capacity (JTTHF), grip strength, aROM wrist extension, spasticity (ASAS), proprioception, stereognosis, and tactile spatial acuity (2POD test). In reviewing the change in these outcomes, the amounts and areas of improvements varied widely across participants, failing to demonstrate robust and consistent gains. However, all children demonstrated an increase in grip muscle strength, as measured by the modified sphygmomanometer, immediately after the intervention phase. The evidence for a positive treatment response was largely inconclusive because Cases 1 and 2 improved in less than 40% of outcomes. In contrast, Case 3 was considered a “positive responder” with most (i.e. 79%, including gasp) clinical outcomes demonstrating clinically important improvement immediately after the intervention had ended and retaining positive effects in 50% of outcomes at follow-up.
Like other individuals with lesions in the basal ganglia, Case 1 had secondary dystonia associated with CP. Dystonia is characterized by fluctuations in hypertonia 62 and may have created significant variability in the clinical outcome measures for this child. It is recommended for future research to differentiate between the three neurologically mediated subtypes of hypertonia (i.e. spasticity, dystonia, and rigidity) 62 upon enrollment and focus participant recruitment primarily on the spastic form of HCP.
Overall, preliminary evidence for a positive treatment response remains inconclusive as only one-third (33%) of the sample (Case 3) showed improvements in 50% or more of the clinical outcomes at post-test (including QUEST grasp). Treatment response was mixed, and given that effectiveness criterion was only met by one child, the evidence was considered insufficient to justify moving forward with an RCT. Nevertheless, the current work presents an important platform onto which other studies can build. Of note, Case 3 demonstrated better hand function in some respects prior to commencing the mFES intervention, obtaining higher scores than the other two participants on the CHEQ, JTHFT, grip strength, and 2POD tests. Case 3 also achieved almost the highest scores possible at pretest on the CHEQ, wrist extension aROM (with fingers flexed), and stereognosis outcomes. Not surprisingly, this child could not demonstrate any further improvements at post-test or follow-up because his baseline scores were already at or around the highest level (i.e. ceiling effect) on these measures. The treatment response observed in this child was consistent with previous findings that individuals with higher baseline functioning respond better to FES than those with lower levels of function. 63 Case 3 was also the oldest participant and had the same age (13 years) as the adolescents with chronic pediatric stroke that participated in a similar study and showed improvements in grasp and UL function after using the same mFES system. 13
Changes in scores that met MCID/CID criteria in the negative direction (i.e. showed deterioration) were unexpected, as current literature review did not find any evidence to suggest FES has any contraindications for children with HCP. In addition, only the aROM wrist extension (with fingers extended) for Case 1 showed a decline in score that was present at both post-test and follow-up assessments. Furthermore, understanding change is a particularly complex endeavor for those diagnosed with CP. 64 Haapala et al. 65 noted that factors such as muscle spasticity, contractures, and scoliosis sometimes make outcome measurement difficult to perform among these individuals. For example, aROM measurement for Case 1 (wrist extension with fingers flexed) was not possible at both post-test and follow-up and could be interpreted within the context of her abnormal muscle tone and posturing associated with dystonia. Case 1 also showed the greatest unpredictability with scores meeting MICD/CID criteria in both negative and positive directions. However, all the outcomes (i.e. excluding grip strength and wrist aROM with fingers extended) that showed a decline at post-test for Case 1 had surpassed pretest scores and two (i.e. QUEST total and wrist aROM with fingers flexed) met improvement criteria at follow-up. Thus, the changes observed in Case 1 appear erratic suggesting they may not reflect a true “deterioration” but rather could be secondary to dystonia, which fluctuates in severity.
Intensive training with mFES alone, however, was not sufficient to lead to clinically relevant functional gains in UL function in two-thirds children from the patient sample. Despite sharing similar mechanism of injury, one aspect that sets conditions such as acquired brain injury and pediatric stroke apart from CP is that the child with CP will not be recovering lost motor functions. Thus, it is important to keep this in mind when comparing the positive effects of mFES seen in individuals with acquired stroke compared to those in children with HCP. Although this study did not find robust improvements in two of our three participants, facilitating the activation of several muscles using a functionally relevant approach, while still requiring active engagement from the child and permitting visual feedback of the arm kinematics, is an approach that closely mimics natural motor learning. In this way, mFES therapy may still be an effective strategy for educating the paretic limb to assist in bimanual tasks. It is very common for children with HCP to adopt compensatory strategies using their paretic arm as an assist, 66 but ultimately having a high ability to use that limb efficiently in bimanual activity performance is a crucial outcome 67 and important component in the rehabilitation goal of improving the child’s ability to participate in ADLs. 68
The mFES system used in this study was flexible as it facilitated intensive practice of several grasp types, and by placing electrodes on individual fingers, it further increased the complexity of the task-oriented exercises performed. Training with a multichannel stimulator facilitated the synchronous activation of many muscles, and by being able to choose from various protocols and to adjust the stimulation intensity (amplitude) of each channel before and during training, the intervention was tailored to the child’s needs and tolerance. However, as noted by de Kroon and IJzerman, 69 it is still unclear how setting and adjusting specific stimulation parameters (e.g. frequency, amplitude, and pulse duration) might influence clinical outcomes, and muscle activation and joint translation may be more pressing factors. Thus, future studies should continue to document and evaluate various treatment protocols as more research is required to determine what are the optimal stimulation paradigms. An interesting aspect from the analysis of the stimulation parameters used was the decreased amplitude required to elicit muscle contraction for Case 3 as the child approached end of treatment. The slope of the mean amplitudes over time (−0.03) and the square regression coefficient (0.78) for Case 3 suggest that the required amplitudes to elicit the desired muscle response had a negative trend, declining as this child completed more therapy sessions. This finding is consistent with the decreased amounts of electrical stimulation required to achieve muscle contraction reported in a case study of a spinal cord injury patient who eventually returned to ambulation using mobility aids after receiving 11 lower limb FES sessions. 70 Also, when evaluating lower limb muscle response to FES in hemiplegic stroke patients, Lee et al. 71 found that the amplitude required to elicit muscle response was significantly higher for the paretic limb as compared to the nonparetic side. Thus, one can postulate that decreased stimulation intensity may be a sign of improved muscle response and improved selective motor control.
Subjectively, the increased awareness of the involved arm and hand was also reported by all participants on the feedback questionnaire. However, these reports were only accompanied by clinically important changes on the perceived hand usage as assessed by the CHEQ in Case 2 at follow-up. Responses to the questionnaire also indicated that the number of weekly therapy sessions was sometimes too high. This aligns with the low participant recruitment rate found in the study, stressing the low willingness to participate due to the burden of a high time commitment. Future studies will need to implement more robust recruitment strategies or alter the study setting (e.g. closer to home) and/or frequency of the mFES intervention.
There are strengths and limitations to the study that need to be highlighted. A strength of the study is the inclusion of multiple psychometrically sound clinical outcome measures to explore the impact of mFES on multiple aspects of UL function. Although these constitute potential outcome measures for a definitive trial, other measures such as the Assisting Hand Assessment (AHA), 67 which evaluates how effectively the paretic hand is used in bimanual activities within a play context or wearable wrist monitors, are convenient tools to assess functional use of the hemiplegic hand at home, school, and play environments, 72 and they are considered suitable options for objectively validating the perceived spontaneous hand usage that was self-reported by children/parents. With respect to limitations, although this study was exploratory in nature, the sample size was too small and insufficient to determine subgroup effects and to generalize the findings. Child characteristics, such as age, severity of baseline motor impairment, and hypertonia subtypes are potential factors that may have influenced the results, as demonstrated by the significant disparity in treatment response. The use of some form of comparison such as multiple baseline assessments or a matched comparison group that did not receive mFES treatment would strengthen the study design. To this end, future investigations could include both control and experimental phases so that each child’s performance can be compared to the effects of mFES alone, repetitive task-oriented training alone, or a combination of both aspects. Finally, although a desired ROM was stipulated for each joint when using the mFES, kinematic evaluation was not part of the outcome measures in this study. Other investigations have highlighted the utility of using kinematic protocols when evaluating treatments for children with CP.73,74 Thus, future investigations could incorporate kinematic assessment to compare between pre- and post-mFES kinematic patterns, provide a more complete clinical analysis, and better describe changes on motor strategies.
Conclusion
The present study was limited by the low willingness of parents and children to participate in the study as demonstrated by the low participant recruitment rate. Despite the achievements made by one child, the results did not provide conclusive evidence to support or discard the potential implementation of UL mFES therapy in pediatric HCP. Thus, the intervention approach described here can serve as a starting point on which future research is based. Considerations for future studies comprise the potential modification of subject eligibility criteria to include those with predominantly spastic HCP, preferably in their early teens, and classified as having mild to moderate baseline severity of unimanual hand function (i.e. QUEST total >50). Including other tests of bimanual performance (e.g. AHA or a wearable wrist monitor) could help investigators obtain a more objective report on the paretic hand involvement during daily activities. Although there was not strong evidence to support the development of an RCT, multiple baseline assessments or a matched comparison group study design using blinded assessors would allow for comparisons to further elucidate the effectiveness of mFES for children with HCP. Lastly, developing a home-based approach, perhaps through either therapist outreach/monitoring, parent-provided therapy, or a combination of both may facilitate participant recruitment, provide a sample that is large enough to allow parametric statistical analyses, and increase internal and external validity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Centre for Leadership in Child Development funding, the Bloorview Children’s Hospital Foundation Chair in Developmental Paediatrics funding, and the Whipper Watson Graduate Research Studentship Award (to LG), all from Holland Bloorview Kids Rehabilitation Hospital.
Guarantor
DF
Contributorship
LG and DF were involved in the study design, subject recruitment, data collection, data analysis, and manuscript writing. LS assisted in the study design and subject recruitment. KM participated in the study design, data analysis and interpretation, critically revised the article, and approved the final draft.
Acknowledgements
Thanks are extended to Yvonne Ng and Betty Chan, the two occupational therapists who administered the intervention and conducted the assessments, to the children and families who participated in the study, and MyndTec for the equipment support. And, the findings within this paper were previously presented at the 21st Annual Conference of the International Functional Electrical Stimulation Society, IFESS, London 2017.