
Abstract
The goal of this narrative review is to evaluate the efficacy of available questionnaires for assessing the outcomes of “continence difficulty” interventions and to assess the selected questionnaires concerning aspects of stigmatization. The literature was searched for research related to urinary incontinence, as well as questionnaires and rating scale outcome measurement tools. The following sources were searched: Cochrane Library, EMBASE, Medline, and PubMed. The following keywords were used separately or in combination: “Urinary incontinence,” “therapy,” ”treatment outcome,” “patient satisfaction,” “quality of life,” “systematic reviews,” “aged 65+ years,” and “questionnaire.” The search yielded 194 references, of which 11 questionnaires fit the inclusion criteria; 6 of the 11 questionnaires did not have any stigma content and the content regarding stigma that was identified in the other five was very limited. A representative model of how stigma impacts continence difficulty interventions was proposed. While the 11 incontinence specific measurement tools that were assessed were well researched and designed specifically to measure the outcomes of incontinence interventions, they have not been used consistently or extensively and none of the measures thoroughly assess stigma. Further studies are required to examine how the stigma associated with continence difficulty impacts upon health care interventions.
Keywords
Introduction
Urinary incontinence is a condition for which involuntary leakage of urine is objectively demonstrable. 1 The prevalence of urinary incontinence is estimated to be 5–10% among the general elderly population, 10–20% among those receiving home care, and at least 50% among those individuals living in long-term care institutions. 2 In Canada, close to 1.5 million people experience episodes of urinary incontinence, a number that is bound to increase as the population ages rapidly. 3 Most studies indicate that women have a higher prevalence of urinary incontinence than men, due to differences in the structure of the male and female urinary tracts. The causes of urinary incontinence among women include childbirth, menopause, obesity, presence of lower urinary tract symptoms and decreased mobility. It is common for men to experience urinary incontinence following a prostatectomy, as suggested by the prevalence rate for men spiking from 5% to over 60% following this surgery. 4 The literature includes numerous definitions of incontinence and continence symptoms. 5 For this study, we sought to assess a range of continence questionnaires. Consequently, we selected the term “continence difficulties” (CD) to embrace symptoms of both urinary incontinence as well as urinary continence, which includes conditions that are not necessarily associated with involuntary leakage.
CD can lead to various negative psychosocial outcomes. Individuals with this condition have reported feelings of powerlessness, 6 that serve as an obstacle to engaging in activities of daily living 7 and social participation.8,9 While some reports associate CD with reduced self-esteem, 10 other authors have reported that no association is found between CD and self-esteem. 8
Despite common misconceptions that CD is inevitable and untreatable, 11 the evolution of treatment options over the past few decades has resulted in the development of various conservative, pharmacological, surgical, and technological treatments. Urinary CD can be eliminated or improved in the vast majority of patients (70%, according to this survey). 3 With alternatives comes a responsibility to assess the efficacy of these treatments so that future clients may make informed health-care decisions.
Stigma
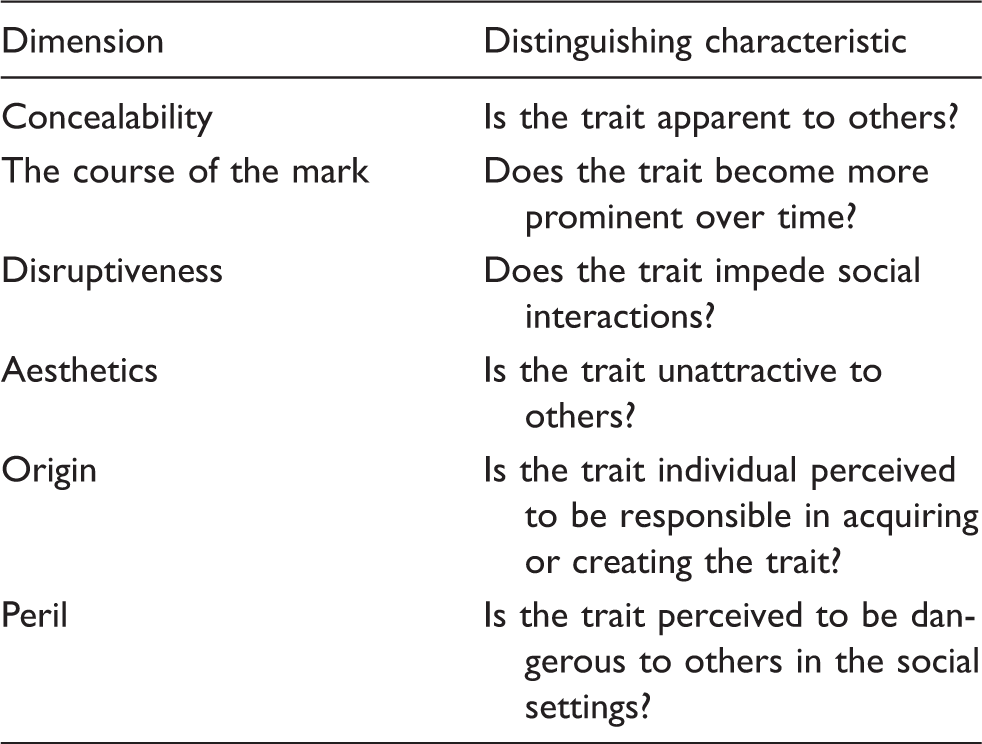
A topic that has received scant attention in the research literature is the stigma associated with CD. Individuals are stigmatized when they possess, or are thought to possess, an attribute or characteristic that conveys a social identity that is devalued in a particular social context. 12 Stigmatization is a social phenomenon, whereby two groups of people exist: insiders, those who have a stigmatizing trait; and outsiders, those who do not have the trait. In social settings, outsiders may recognize that another individual possesses a characteristic that sets them apart, potentially prompting the devaluation of the insider. Stigma is fundamentally a threat to one’s self-identity. 13
Dimensions of stigma.
Contemporary theorists identify three types of stigma. Perceived-stigma is fear and worry of being subjected to a stigmatizing event. 16 Self-stigma is directing prejudicial attitudes inwards to one’s self. 17 Finally, enacted-stigma includes episodes of discrimination based on a stigmatizing attribute. 18 There is great variability in the stigma process, 19 such that stigmatization may potentially lead to both adaptive or maladaptive responses. For example, an insider who perceives a stereotype to be unreasonable, 17 may respond constructively to stigmatization. 20
In Western societies, we are socialized to understand that elimination of bodily waste is a private matter that should be done in a tidy way. 7 Failure to do so risks being stigmatized. 21 Individuals who present CD symptoms may be perceived as “different” and are commonly stereotyped as frail, dependent, incompetent or simply old. 7 CD is associated with both old age and young age. CD threatens one’s adult status. 22 Individuals with CD may be both embarrassed and shamed by having CD.7,21,23 Urinary incontinence symptoms, including daytime frequency, urgency, and nocturia are also stigmatizing, as they are socially disruptive indications of loss of control over bodily functions. 5
Responses to stigmatization vary. 17 It is common for individuals with CD (a concealable trait) to withdraw from social participation and conceal identifiers of their condition.24,25 Brittain and Shaw 26 found that stroke survivors with CD were embarrassed and fearful of leakages and odour, resulting in isolating tendencies. Disengagement is associated with elevated levels of stress, 19 perhaps because attempts to conceal may be thwarted by accidents, smells, and the visibility of the management products used to deal with the condition.
Denial, concealment, and reluctance to acknowledge health status all potentially serve to prevent or delay entry into treatment, thereby decreasing the possibility for successful intervention.6,27–30 Individuals with CD may be reluctant and embarrassed to consult health care practitioners concerning treatment options,31,32 such that the proportion of individuals who seek out treatment options is in the order of 5–25%.4,33
The numerous effects of CD on a person’s psychological and social wellbeing make it challenging to measure the relative success of a particular treatment. For example, it is prudent to ask oneself if reducing the number of leakage episodes constitutes a better treatment success than a client’s own perception of dryness. The former is an objective measure, acquired by using a pad weight test, for example, while the latter is a subjective measure. 34 Unlike objective measures, subjective questionnaires are highly versatile in their production and administration. But versatility raises concerns about accuracy. 35 In order to eliminate bias, questions such as “who should ask the questions,” “to whom should questions be asked,” “what questions should be asked” and “when should they be asked” need to be considered when determining the efficiency of a questionnaire. 35 Hence, a combination of both subjective and objective measures is most likely the best way to assess the efficacy and effectiveness of CD treatments.
With these issues in mind, the purpose of this review was to examine stigma-related content in a selection of popular instruments for assessing the outcomes of urinary CD interventions. A characterization of each measure is presented, followed by an identification and evaluation of stigma-related items.
Methods
The method used was a narrative (or traditional) literature review. It was designed to provide a comprehensive overview of the topic area, highlight significant areas of research, and identify gaps in the research.
We sought to answer the following questions: In research on adults who have undergone an intervention (behavioral, drugs, surgery, and/or management products) to help manage their urinary incontinence, what instruments were used to measure continence improvement? What were the stigma-related contents of these instruments?
The population of interest was individuals aged 65+ with urinary incontinence. The intervention of interest included any form of urinary incontinence measurement tool. All types of study designs, methods, and outcomes were considered, with an emphasis on randomized controlled trials. The following sources were searched: Cochrane Library, EMBASE, Medline, and PubMed. Articles screened in had to contain the keywords “Urinary incontinence,” “aged 65+ years,” “therapy,” and “treatment outcome.” These articles were then searched for each of the following keywords separately, “patient satisfaction,” “quality of life,” “systematic reviews,” and “questionnaire.”
Literature selection
The first author manually searched relevant journal articles if the abstracts made any mention of a measurement tool that was used to assess outcomes after a certain treatment for CD. All potential sources for “gray literature” (unpublished or government related technical documents) were searched. Books, proceedings, and presentations were excluded. The search was limited to sources published within the past 15 years, from December 2000 to July 2015, in English. Systematic reviews and meta-analyses were also sought to compare the transparency and accuracy of the assessment. Articles were included if they made mention of a questionnaire outcome measurement tool in the abstract. A research assistant read all of the abstracts, then compiled a list of questionnaires and scales that were used, along with corresponding reference IDs so as to track how often each measure was used in studies. Only questionnaires dealing directly with urinary CD were considered. Outcome measures qualified for consideration either by having obvious words such as “incontinence”, “urinary tract”, “urinary symptom” in the questionnaire title, or being identified in other studies to be a specific outcome measurement instrument for CD. Articles that fit within the selection criteria described above were traced back to their original publication, from which details of their psychometric evaluation were extracted and assessed.
Assessing questionnaires for stigma
At present a well-validated measure of self-stigma does not exist. Even so, Van Brakel 36 suggested that aspects of the stigmatization process are quite similar across health conditions, cultures and public health programmes. Thus, the development of a nonspecific (i.e. generic) measure to assess health-related stigma may one day be feasible. But until then, Van Brakel recommended that a comprehensive assessment of stigma associated with health conditions incorporate (ideally in interview format) five aspects of health-related stigmas (the first two items seek to assess the social and physical factors that precipitate stigmatization, and are thus not relevant to the present discussion): (a) attitudes of community members and groups (e.g. health care providers) towards people who possess stigmatizing health conditions; (b) discriminatory services and legislation; (c) perceived-stigma (i.e. fear of stigmatizing event); (d) enacted stigma (i.e. episodes of discrimination); and (e) self-stigma (i.e. directing prejudicial attitudes inwards).
Definitions, identifiers and instructions for the coding process.

The questionnaires were analyzed by the first author using content analysis. 37 The objective was to ensure that all items addressing any aspect of stigma be assigned a code. Questionnaires were read item by item, searching for content relevant to perceived-stigma, enacted-stigma, and self-stigma. 38 Selected items were highlighted and assigned a meaningful label, a process known as coding. As soon as all questionnaires had been coded once, the questionnaires were re-read scrutinizing content and adjusting to the coding scheme as needed. This process continued until code list adjustments were no longer deemed necessary. The next step was to test the reliability of the application of codes. This was tested by comparing how the first author coded three randomly selected questionnaires, with the coding of the same questionnaires performed independently by an individual from outside the research team. A researcher who had basic understanding of outcomes research, and experience coding text-based data was enlisted to complete this task. This person was provided with the most up to date version of the definitions and the three questionnaires. Inter-rater reliability was established by calculating the number of items similarly coded, divided by the total number of items. An acceptable reliability score (kappa) of 0.94 39 was established on the first attempt.
Results
Key features of the selected questionnaires.
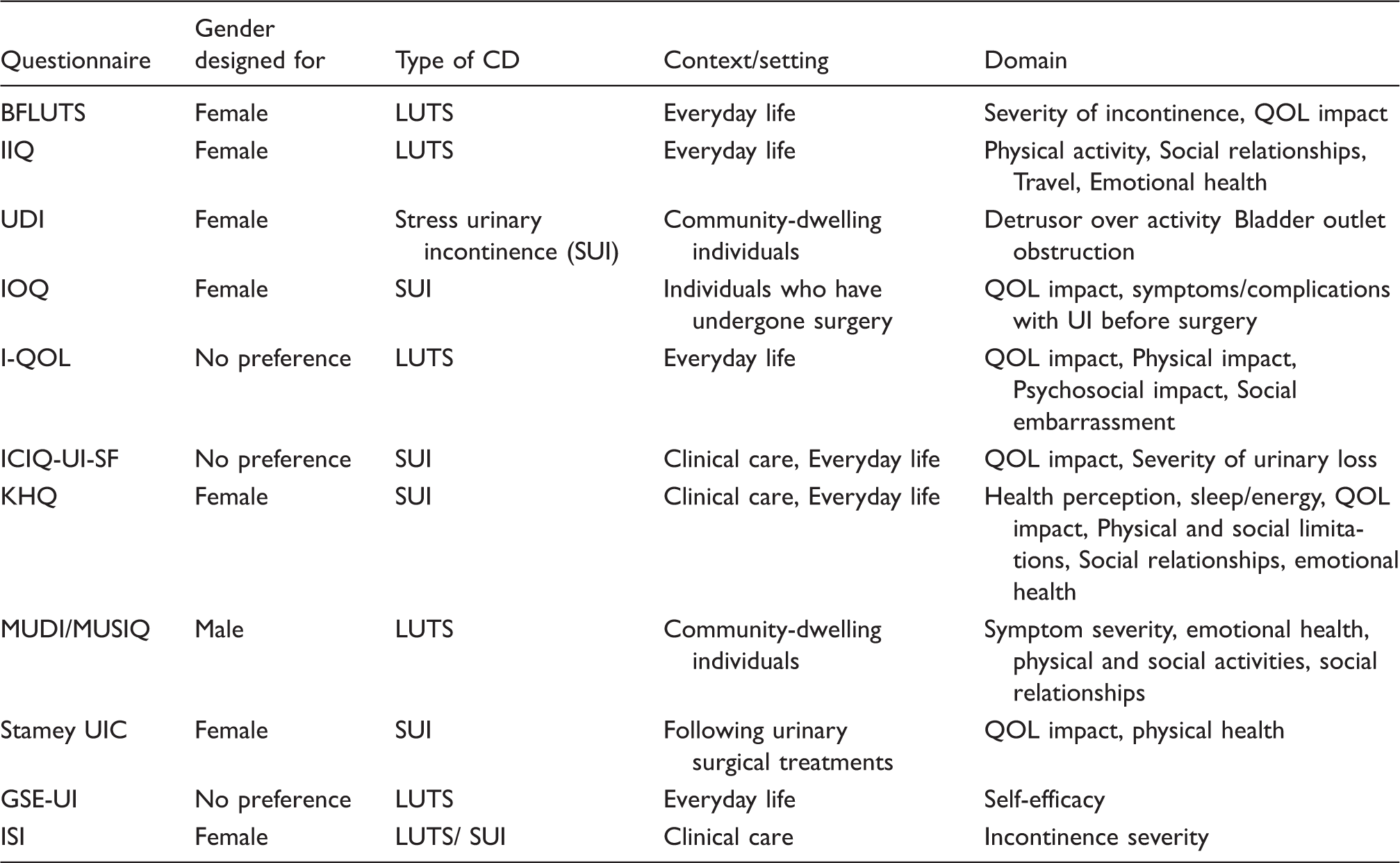
BFLUTS: Bristol female lower urinary tract symptoms; IIQ: incontinence impact questionnaire; UDI: urogenital distress inventory; IOQ: incontinence outcome questionnaire; I-QOL: incontinence quality of life; ICIQ-UI-SF: international consultation on incontinence questionnaire-urinary incontinence-short form; KHQ: kings health questionnaire; MUDI: male urogenital distress inventory; MUSIQ male urinary symptom impact questionnaire; GSE-UI: geriatric self-efficacy index for urinary incontinence; ISI: incontinence severity index.
Reliability and validity of questionnaires. a

Values of 6.0 and higher are generally considered to be acceptable.
Refers to the RAND 36-Item Health Survey. 24
Centers for epidemiologic studies depression scale. 40
Medical outcomes study measure of social support 1992. 41
Profile of mood states. 16
BFLUTS: Bristol female lower urinary tract symptoms; IIQ: incontinence impact questionnaire; UDI: urogenital distress inventory; IOQ: incontinence outcome questionnaire; I-QOL: incontinence quality of life; ICIQ-UI-SF: international consultation on incontinence questionnaire-urinary incontinence-short form; KHQ: kings health questionnaire; MUDI: male urogenital distress inventory; MUSIQ male urinary symptom impact questionnaire; GSE-UI: geriatric self-efficacy index for urinary incontinence; ISI: incontinence severity index.
Summary of stigma content from identified measures.

BFLUTS: Bristol female lower urinary tract symptoms; IIQ: incontinence impact questionnaire; UDI: urogenital distress inventory; IOQ: incontinence outcome questionnaire; I-QOL: incontinence quality of life; ICIQ-UI-SF: international consultation on incontinence questionnaire-urinary incontinence-short form; KHQ: kings health questionnaire; MUDI: male urogenital distress inventory; MUSIQ male urinary symptom impact questionnaire; GSE-UI: geriatric self-efficacy index for urinary incontinence; ISI: incontinence severity index.
Bristol female lower urinary tract symptoms questionnaire
The Bristol female lower urinary tract symptoms (BFLUTS) questionnaire was developed by Jackson et al. 42 to assess female patients’ severity of incontinence and its impact on quality of life. Consisting of 19 questions, items are grouped by symptoms of CD, sexual matters, and lifestyle. Stigma: BFLUTs does not include content relevant to perceived- or self-stigma. However, the developers recommended in-depth interviews to probe patients’ understanding of the questionnaire and their responses. During this interview, patients may choose to describe previous experiences of enacted-stigma.
Incontinence impact questionnaire
The incontinence impact questionnaire (IIQ) was developed by Shumaker et al. 43 to assess the impact of stress CD on the everyday lives and emotions of women. The IIQ consists of 30 questions among subscales of physical activity, travel, social relationships, and emotional health. Stigma: Two IIQ items are pertinent to perceived-stigma: Item W (Does fear of odor restrict your activities?) and Item X (Does fear of embarrassment restrict your activities?). Both questions assess emotions associated with symptomology and the potential of being devalued by others. Three IIQ items address self-stigma: Item Z (Does your problem cause you to experience fear?); Item AC (Does your problem cause you to experience depression?); and Item AD (Does your problem cause you to experience embarrassment?). Each of these questions assesses how the CD condition has impacted upon relevant feelings and emotions.
Urogenital distress inventory
The urogenital distress inventory (UDI) was developed by Shumaker et al. 43 to be a companion to the IIQ. The UDI is used to assess the degree to which symptoms associated with incontinence are bothersome to women, and consists of 19 questions probing three domains: symptoms related to stress urinary incontinence, detrusor overactivity, and bladder outlet obstruction. Stigma: UDI does not include stigma relevant content.
Incontinence outcome questionnaire
The incontinence outcome questionnaire (IOQ) was developed by Bjelic-Radisic et al. 44 to assess the quality of life of individuals following surgery for stress urinary incontinence. The IOQ contains 27 questions related to symptoms, complications, quality of life and satisfaction, problems with urinary incontinence before surgery, and demographic and treatment-related information. Stigma: One IOQ item is pertinent to self-stigma: Item IOQ14 (Change in feeling about body). Post-operative reductions in body image may be a reflection of self-stigma.
Incontinence quality of life
The incontinence quality of life (I-QOL) was developed by Wagner et al. 45 to assess the quality of life of persons with urinary incontinence. The I-QOL consists of 22 items in the following subscales: avoidance and limiting behaviors, psychosocial impacts and social embarrassment. Stigma: Eight I-QOL items address perceived-stigma (* denotes items which address future events or occurrences that may lead to an incontinence accident): Item 1 (I worry about wetting myself); Item 4 (I worry about coughing or sneezing because of my incontinence*); Item 6 (I worry about where toilets are in new places*); Item 11 (I worry about others smelling urine on me); Item 17 (I worry about my incontinence getting worse as I grow older*); Item 19 (I worry about being embarrassed or humiliated because of my incontinence); 24 (I worry about not being able to get to the toilet on time*); and 28 (I worry about having sex because of my incontinence*). These items relate to perceived-stigma as they assess level of worry associated with forthcoming and potentially embarrassing events. Three I-QOL items are pertinent to self-stigma: Item 7 (I feel depressed because of my incontinence); Item 21 (My incontinence makes me feel like I’m not a healthy person); and Item 22 (My incontinence makes me feel helpless) are all relevant to self-stigma.
International consultation on incontinence questionnaire-urinary incontinence-short form
The international consultation on incontinence questionnaire-urinary incontinence-short form (ICIQ-UI-SF) was developed by the International Consultation on Incontinence. 46 This four-item questionnaire provides a summary of the severity, impact on quality of life and perceived cause of symptoms of incontinence. Stigma: ICIQ-UI-SF does not include stigma-relevant content.
Kings health questionnaire
The kings health questionnaire (KHQ) was developed by Kelleher et al. 47 to assess the influence that urinary incontinence has on the quality of life of women. The KHQ includes 21 questions concerning: perceived health status, severity of urinary incontinence symptoms, physical limitations, social limitations, role limitations, emotions, personal relationships, and sleep/energy. Stigma: One KHQ item addresses perceived-stigma: Item 8D (Worry in case you smell?). This item is relevant insofar as assessing the level of worry individuals feel due to future events that could be potentially embarrassing. One KHQ item is pertinent to self-stigma: Item 6C (Does your bladder problem make you feel bad about yourself?). This item addresses relevant emotions associated with CD-related difficulties.
Male urogenital distress inventory and male urinary symptom impact questionnaire
The male urogenital distress inventory (MUDI) and male urinary symptom impact questionnaire (MUSIQ) were developed by Robinson et al. 40 to assess specific impact of lower urinary tract symptoms (LUTS) on health-related quality of life for community-dwelling men. MUDI and MUSIQ are an adaptation of the commonly used UDI and IIQ. 43 The MUDI is a 27-item questionnaire which assesses presence of LUTS, and the degree to which symptoms are bothersome. The MUSIQ is a 32-item questionnaire that prompts respondents to indicate the degree to which LUTS affect emotional status and a range of activities, relationships, and roles. Stigma: MUDI does not include stigma relevant content. Similar to the IIQ, a number of questions in the MUSIQ are pertinent to stigma. These items include: Two MUSIQ items address perceived-stigma: MUSIQ-25 (How much do you limit what you do because of a fear of being embarrassed?) and MUSIQ-26 (How much do you limit what you do because of a fear of odor?). These items address future events or occurrences that could lead to an incontinence accident. Three MUSIQ items are relevant to self-stigma: MUSIQ-12 (Have urinary symptoms changed the way you feel about yourself?); MUSIQ-28 (How much do urinary symptoms cause you to feel afraid?); MUSIQ-32 (How much do urinary symptoms cause you to feel embarrassed?). These items address relevant emotions associated with CD symptoms.
Stamey urinary incontinence scale
Stamey 48 developed the Stamey Urinary Incontinence Scale to be a grading scale for the evaluation of stress urinary incontinence. The scale can be used to gauge improvement in incontinence following various treatments. Stigma: The Stamey Urinary Incontinence Scale does not include stigma relevant content.
Geriatric self-efficacy index for urinary incontinence
The geriatric self-efficacy index for urinary incontinence (GSE-UI) was developed by Tannenbaum et al. 49 to assess self-efficacy for reducing or preventing urinary incontinence. The developers applied the concepts of Bandura’s Guide for Constructing Self-Efficacy Scales 50 such that all items began with ‘‘How confident are you that you can…”. Stigma: GSE-UI does not include stigma relevant content.
Incontinence severity index
The incontinence severity index (ISI) was developed by Sandvik et al. 41 to produce a valid epidemiological measure of female incontinence severity. The ISI is composed of two questions: (1) How often do you experience urinary leakage?; (2) How much urine do you lose each time? Stigma: Neither of the ISI items addresses stigma.
Discussion
Analyses revealed that more than half (six) of the measures do not have any stigma content (i.e. BFLUTS; UDI; ICIQ-UI-SF; Stamey; GSE-UI; ISI). Four of the measures address perceived-stigma (IIQ; I-QOL; KHQ; MUDI- MUSIQ). The I-QOL had the greatest number of perceived-stigma items. Whereas, five measures address self-stigma (IIQ; IOQ; I-QOL; KHQ; MUDI- MUSIQ). Only the BFLUTS recommends conducting an interview with individuals as a way to supplement information provided by the questionnaire, and could thus serve as a way to examine enacted-stigma.
Four points are noteworthy concerning these findings. First, there is a conspicuous lack of content that seeks to assess attitudes about CD treatments, and how stigma may impact these attitudes. In their current format, the measures are unable to assess key questions, such as ‘How do attitudes about CD management products impact upon intervention outcomes?’ Second, the questionnaires that do contain stigma content only address the negative impacts of stigmatization on the individual. Recall that individuals may have adaptive responses to stigmatization. Therefore, it is conceivable that an individual with CD may never feel shame about their condition, or may come to terms with CD after some time. At present, existing CD outcome measures do not adequately address positive stigma. Third, there is a need for opportunities to assess enacted-stigma. Only BFLUTS provides a means to assess enacted-stigma by recommending that interviews be conducted with individuals, to uncover how past experiences of stigmatization may impact quality of life outcomes. Fourth, concerning the gender specific nature of IIQ and UDI, and MUSIQ and MUDI, the subscales covered by these measures appeared to be very similar, which raises questions of how the expressions of CD stigma may be similar or different across gender. Moreover, one wonders if there is a need to further personalize questionnaires to be more gender specific, or whether a gender-neutral approach would perform just as well as a gender-specific approach.
Representation of CD stigma impacts CD intervention
To aid in the conceptualization of CD, and perhaps the eventual incorporation of stigma items into CD intervention outcome measures, a representative model of how stigma impacts CD intervention is proposed. The representation (Figure 1) portrays accepted information concerning health-related stigma (drawn from a variety of health disciplines), and offers an approximation of how stigma factors may interact to impact upon CD intervention outcomes. This representation is not intended to be a comprehensive conceptual framework; rather, it is intended to be a starting point to initiate a dialogue and aid in the identification of stigma items for inclusion in CD quality of life outcomes measures. A key assumption associated with this model is that all clients will access health care, employ services and be impacted by their use (i.e. outcomes).
Model of effects of stigma on outcomes of CD interventions.CD: continence difficulty; Central box: typical chronology of CD intervention and outcome; Oval-shaped items: factors that moderate medical, rehabilitation, and self-directed interventions that address CD difficulties, known as “moderators”; +/-: represents the varying interactions between the central box and moderators, and the moderators themselves.
The model (see Figure 1) illustrates the interaction between the individual, health care provider and societal inputs of stigma. The centre box portrays a typical chronology, from onset of CD, to help seeking for symptoms, leading to intervention outcomes. The oval-shaped items that surround the central box serve to moderate medical, rehabilitation, and self-directed interventions to address CD difficulties. These moderators include: relevant CD stereotypes, self-stigma, participation in activities of daily life, previous instances of enacted stigma and significant others’ attitudes about CD. It is assumed that interactions between the central box and the moderators, and the moderators themselves vary greatly (as depicted with the ‘+/-’ symbols). Also, although it is not immediately obvious upon inspecting the model, it is assumed that all moderators may influence any of the four landmarks in the central box (e.g. participation in activities of daily life may impact upon CD intervention outcome).
Prior to the onset of CD, in early childhood, individuals learn relevant CD stereotypes from community members and significant others, and develop their own attitudes about CD issues. 7 Following the onset of CD, the individual may be conflicted by the knowledge that she or he now possesses a trait that she or he had once ridiculed, 17 which may initiate a process of self-stigmatization.7,21,23 At some point, the individual realizes that they need to use CD management products and or seek professional consultation for their CD condition. Seeking for help may be delayed if the individual self-stigmatizes, or has had previous instances of enacted stigma.6,27,30 Individuals may be reluctant to access health care and adhere to recommended treatments due to the stereotypes associated with CD. Help-seeking may lead to self-stigma or prejudicing from others. Consultations with health professionals may be another potentially stigmatizing situation, if practitioners do not perceive CD to be a treatable condition.21,51 Finally, intervention outcomes (e.g. product satisfaction, participation in activities of daily life and well-being) may be impacted by previous instances of perceived-stigma, self-stigma, and enacted-stigma. In particular, the balance between confidence that one can successfully participate in activities of daily living versus fears and worries of accidents and stereotyping (i.e. perceived-stigma).
Implications
There is ample evidence that many individuals who have CDs are reluctant to seek help and to engage in recommended treatment regimens. These individuals are, in effect, foregoing rehabilitation services that could possibly improve their quality of life. We believe that stereotyping and stigmatization play a critical role in this reluctance to access. Across numerous health conditions and according to the literature reviewed in this paper, stigma has been shown to impede recognition and early identification of health conditions, and serve as a barrier to help-seeking, including for assistive technology devices. In order to design, implement, and evaluate effective rehabilitation intervention programs, a better understanding of stigmatization is vital.
Over the past few decades, we have seen the development of various treatment options for individuals with incontinence. These treatments and management products represent valued rehabilitation alternatives for those living with CD symptoms. If consumers are to make informed health-care decisions concerning these treatments, it is necessary to assess their efficacy. In the present review, we uncovered 11 incontinence-specific outcome measurement tools. The identified instruments are reasonably well-researched, designed principally to assess the health-related quality of life impact of incontinence symptoms. But they have not been used consistently or extensively in research to measure effectiveness of management products, and none of the measures completely and thoroughly assesses stigma.
To achieve a standardized, objective, and measurable assessment of the psychosocial outcomes attributable to the use of management products, specifically designed tools are required. Our team has begun to explore if one particular measure (i.e. PIADS) requires modifications to address the needs of continence device users and to inform any subsequent item development. The PIADS is a 26-item self-report questionnaire called the (PIADS). 52 In a recent progress report, 53 we reported that the PIADS largely addresses many of the fundamental psychosocial elements of adults who have CDs. Development of a version of the PIADS for continence, the C- PIADS, is underway and is likely to contain new items. This measure, once completed, aims to provide a valid and reliable measure of psychosocial outcomes attributable to assistive technology use that is sensitive to stigma.
Limitations of this review
A narrative review may be susceptible to bias because of the search methods criteria for selection. It is possible that the search omitted significant sections of the literature.
Conclusion
There is an increasing range of procedures, management products, medications, and strategies that individuals with CD may choose from to address CD-related needs. Yet, the extent to which these services are beneficial remains in question. There is little doubt that CD stigma is a determinant of CD intervention outcomes. For some people, there is embarrassment and shame associated with having CD, and these emotions likely play a role (albeit, as yet, not clearly defined) in intervention outcomes. Clinicians should be aware of CD stigma, and may be watchful for manifestations of perceived- and self-stigma, and are encouraged to enter into discussions with their clients to better understand how previous instances of discrimination may affect current practices. Further studies are required to examine how the stigma associated with CD impacts upon health care interventions. There is a need for a comprehensive examination and characterization of the stigma associated with CD, to better understand how stereotypes, perceived-stigma, self-stigma impact upon intervention outcomes. This would be a first step toward the design of device-specific outcome measures that take into account social stigma.
Footnotes
Acknowledgments
The authors gratefully acknowledge technical assistance from Nujhat Bashir and Gabriel Kashindi in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Kenneth Southall.
Contributorship
Kenneth Southall, Eleanor A van den Heuvel, and Jeffrey W Jutai researched literature and conceived the study. WW led data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.