
Abstract
Background
Patients with multiple sclerosis (MS) have individual needs, preferences, and barriers to how they receive care; providers require an understanding of these to facilitate comprehensive clinical care.
Objective
To determine MS clinic characteristics currently valued by or desired by adults with MS, their unmet support needs, and their barriers to care.
Methods
An electronic cross-sectional survey was iteratively developed by a multidisciplinary team and distributed to adults with MS.
Results
Three hundred and eighty-seven participants completed the survey. The most desired characteristics in an MS clinic were the training or knowledge (55%) and compassion (54%) of providers, along with urgent appointment availability (48%). Appointment availability, transportation, and financial costs were barriers to accessing care (44%, 39%, and 30%). Support was requested most often for making lifestyle changes, including improving exercise (52%) and diet (45%). Opportunities for additional support included in-clinic rehabilitation therapies, mental health, and nutritionist services.
Conclusions
Adults with MS report multiple desired clinic characteristics and support needs that are currently unmet. Opportunities for improving care and support include expanding in-clinic services, greater appointment availability, transportation, and education on exercise and diet. Future studies will benefit from assessing the effectiveness of expanded services or support programs in these areas.
Introduction
As a chronic medical disease, multiple sclerosis (MS) becomes a lifelong health journey for many individuals. The development of highly effective disease-modifying therapies (DMT) for MS in the past two decades has greatly decreased relapse rates and limited disability acrual. 1 However, it is known that persons with MS still experience multiple physical, psychological, or financial needs which may negative impact their overall health and well-being.2–6 In the clinic setting, non-DMT factors that influence well-being may include appropriate treatment of the comorbidities or symptoms of MS, feeling educated on their health and treatments, and feeling important to and cared for by their providers. 7 Appropriate management of comorbidities or symptoms related to MS may require coordination and collaboration across disciplines within a health system. 8 The MS clinic has a key role in providing comprehensive care and working to meet these needs for persons with MS.
However, to achieve this level of care and given the number of potential factors relevant to care, additional information is needed to plan and prioritize interventions or services that can be implemented in a clinical setting. In this study, we sought to identify the characteristics desired by individuals in their MS clinics and assessed current associated unmet support needs and barriers to accessing clinical care in this population, focusing specifically on the characteristics, needs, and barriers that may be addressed by a clinic. To accomplish this, we analyzed data from a large parent cross-sectional survey distributed to adults with MS in the USA through social media.
Methods
Survey development
As part of a parent study evaluating long-term outcomes in MS, 9 an electronic cross-sectional survey was developed for adult participants with MS. This survey included questions on participants’ demographics, socioeconomic outcomes, MS disease history, mental health diagnoses and treatments, valued and desired MS clinic characteristics, unmet support needs, barriers to care, and functional and quality of life outcomes.
To determine how to best assess the valued or desired clinic characteristics, unmet support needs, and barriers to care in this population, the multi-disciplinary study team collaborated with a partnering local nonprofit patient organization for individuals with MS. This partnership included clinical providers, leaders of the non-profit, and individuals with MS to ensure input from all relevant parties and to provide a breadth of experience and expertise. The team and partners first considered the personal, clinical, and community factors that may influence the well-being or clinical care of an individual with MS in the USA, and that may be addressable by a medical clinic or clinical provider. The team reviewed current medical literature on the topic, and drew from their personal experience and expertise in working with and providing medical care to this population. Prior literature with validated survey assessments were focused most on assessing unmet support needs, including the Long-Term Unmet Needs in MS (LUN-MS) questionnaire, 10 the Southampton Needs Assessment Questionnaire, 11 and the Social Support Scale of the Multiple Sclerosis Quality of Life Inventory. 12 Few studies used validated assessments for clinic characteristics or barriers to care.
The reviewed questionnaires did not encompass the breadth of the study goals, or include the scope of categories of characteristics, needs, and barriers seen by the team and its partners. Therefore, the team chose to develop a survey specifically for this study, to best accomplish the study's goals of assessing valued or desired clinic characteristics, unmet support needs, and barriers to care. For clinic characteristics, the broader categories of clinic services, location, and provider/staff characteristics were identified, which were subsequently divided into 13 individual valued or desired clinic characteristics. For potential support needs, categories of education, lifestyle changes, legal concerns, locations of medical services, and financial concerns were identified. With further discussion, these were subsequently divided in 12 individual potential support needs. Potential barriers to care were also considered. Categories identified included the logistics of attending clinic visits, social barriers, and prior medical experiences, which were divided into nine potential barriers to care. Clinic characteristics, potential support needs, and potential barriers were assessed as dichotomous Yes/No response options, although a free-text response option was also available if an “Other” characteristic, need or barrier was selected. Likert scales or free-text responses for all questions were considered, but the dichotomous response option was chosen to reduce cognitive burden for the survey, with a goal of increasing full completion rates for the parent and sub-surveys.
After 3 iterative reviews and revisions with the study team and its partners, the penultimate version of the survey was assessed for face validity and clarity by three patients with MS recruited through the partner organization, and the final version was ratified by the study team and organizational leaders. The final survey questions are provided in a Supplemental File. This study was determined to be exempt from further review by our institutional review board.
Survey distribution
The survey questions and responses were converted to a REDCap survey format for electronic distribution. The parent survey had a local and national distribution phase 9 ; however, for this current study only data from the national phase is reported to decrease regional bias of responses. During the national distribution phase, three social media campaigns were conducted focused on adults within the USA. These distribution campaigns are not able to focus specifically on individuals with MS. These campaigns occurred in 7–9 day sessions in October 2024, January 2025, and February 2025 on three social media platforms: Facebook, Instagram, and Square. Respondents to the survey link within these campaigns were directed to a pre-screening form assessing inclusion and exclusion criteria. Those who completed the survey fully were enrolled in a drawing for a payment of $100 or $250.
Participant inclusion and exclusion criteria
To be included in the parent study during this national distribution phase, participants were required to be ≥18 years-old and have a current self-reported diagnosis of MS, as reported previously. 9 Participants were excluded from survey participation if they had a current residency outside of the USA, were ≥80 years-old, had previously completed the survey or were unsure if they had completed it previously. Age limit was chosen to minimize risk of re-identification. Prior survey completion was checked by (1) comparison of a provided email address to those from previously completed surveys, and (2) through self-report of having previously completed the survey or being unsure if they had completed it.
Definition of desired clinic characteristics
Participants were asked about both what they valued in their current MS clinic, as well as what they wish their current MS clinic had. However, what is wished for may be dependent both on what a participant's overall preferences are for an ideal clinic, and what they already have in their current clinic. A respondent may also interpret wish to include what is already present in their clinic. To better determine what a participant's overall preferred clinic characteristics were, we defined desired clinic characteristics. Desired clinic characteristics were defined as those either valued by the participant in their current clinic, or that the participant wished their current clinic provided. The gap between a valued and a desired clinic characteristic therefore provides information on the perceived lack of a preferred clinic characteristic, with a larger gap indicating a greater discrepancy between current and preferred clinic characteristics.
Statistical analysis
Descriptive statistics were used to describe the participants’ demographics, disease characteristics, valued and desired clinic characteristics, barriers to care, and unmet needs. Response rates for valued/desired clinic characteristics and support needs between participants seeing MS specialists versus non-MS specialists and between participants from Colorado versus all other states were compared using chi-square or Fisher's exact tests. Statistical analysis was performed using SAS 9.4.
Results
Participants
The distribution through social media targeted social media profiles for adults within the USA, reaching 403,083 unique social media profiles over the three campaigns (Figure 1). Of these, 711 entered the provided link for the pre-screening survey. A total of 133 were excluded after pre-screening due to one or more exclusions, including a lack of self-reported diagnosis of MS (12), age ≥80 years-old (5), prior survey completion (10), their uncertainty on if they had completed the study previously (80), or not completing the pre-screening survey (40). Of the remaining participants, 387 completed the parent survey sections required for this current study.
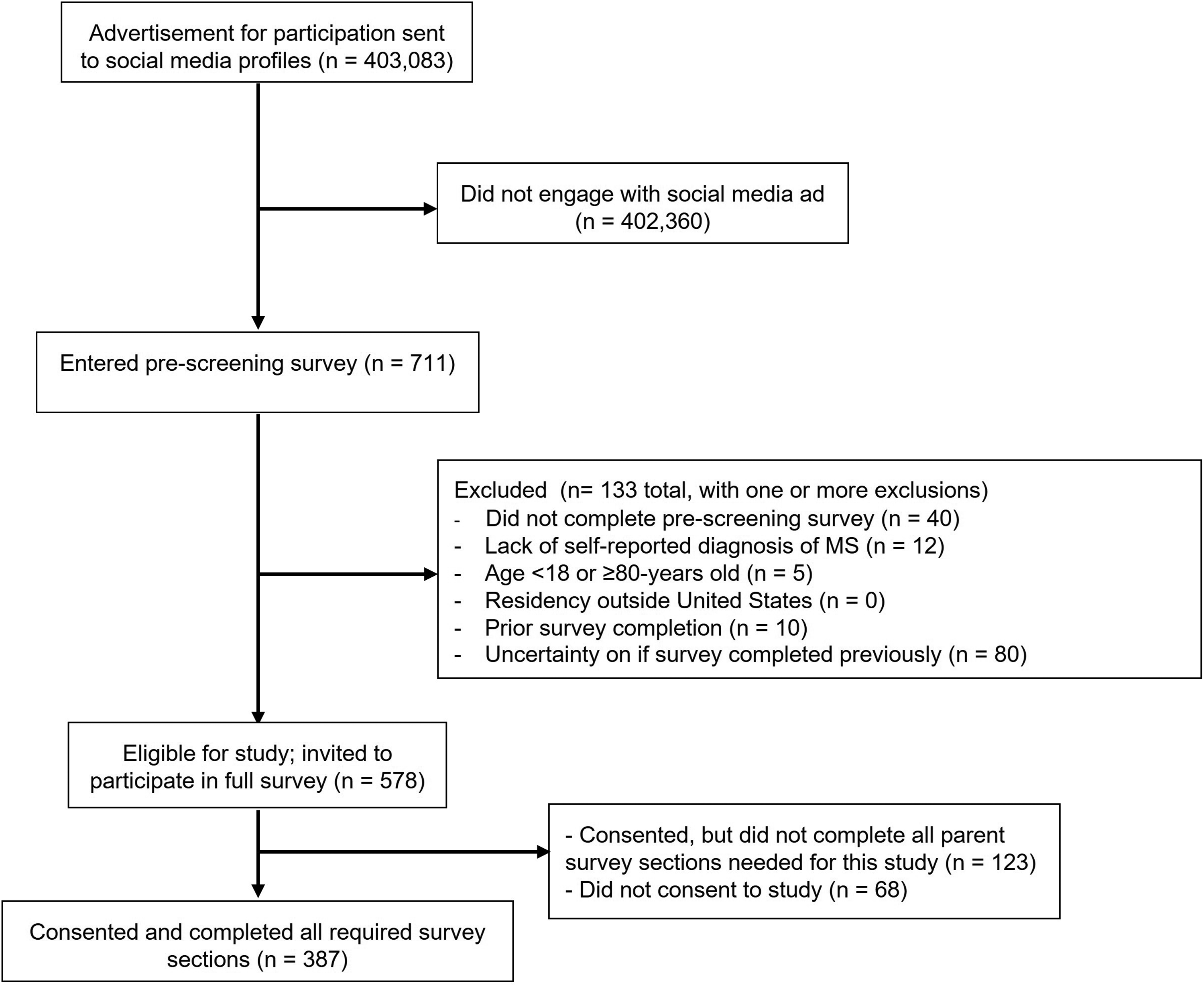
Recruitment of study participants and application of inclusion and exclusion criteria.
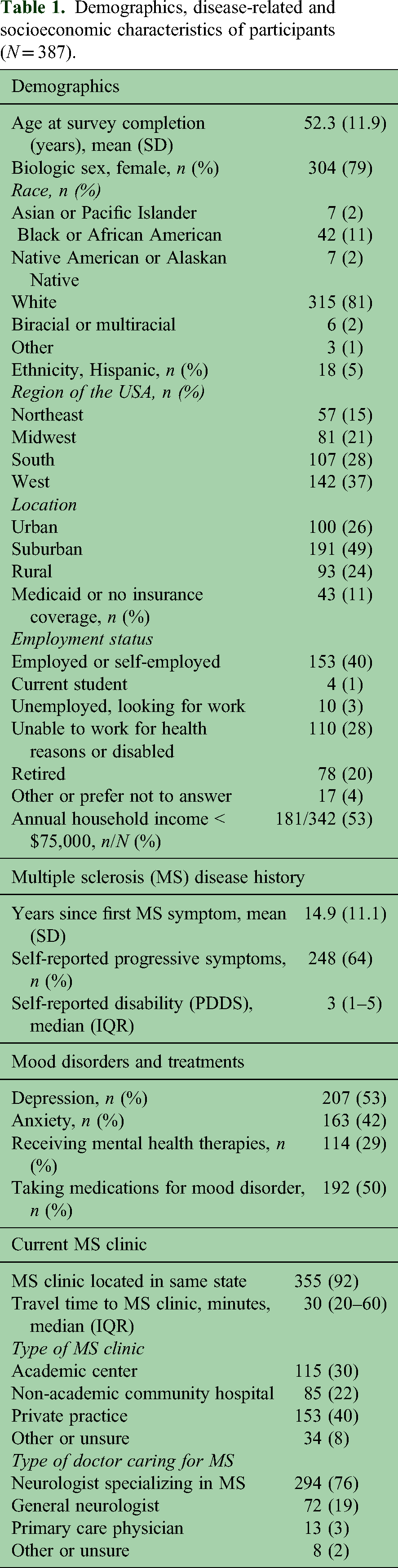
Demographic, disease-related, socioeconomic, and clinic-related characteristics are provided in Table 1. The participants had a mean age of 52.3 years-old and were predominantly female (79%) and White (81%). Compared to a large population-based estimate of MS prevalence in the USA, 13 our study had similar age (mean = 52.3 yo, vs. median age range = 45–54 yo), sex (79% vs. 76% female), and racial and ethnic distributions (White: 81% vs. 77%; Black: 11% vs. 11%; Hispanic: 5% vs. 7%). While the survey was distributed nationally via social media without a regional bias, 75 (19%) of respondents were from Colorado. Our participants had a mean duration since MS diagnosis of 14.8 years. Sixty-one percent reported progressive symptoms with a median Patient Determined Disease Steps (PDDS) score of 3 (gait disability). Seventy-seven percent were being seen by a neurologist specializing in MS for their MS care, with a plurality being seen in private practice (38%). Approximately half had a mental health diagnosis of depression or anxiety, with 29% of all participants receiving mental health therapies and 50% receiving a medication for treatment of a mood disorder. Thirty-one percent were unable to work due to health reasons or disability or were unemployed and looking for work.
Demographics, disease-related and socioeconomic characteristics of participants (N = 387).
Because clinics vary in respect to their structure and services, we assessed both the characteristics valued by participants in their current MS clinics and characteristics desired in a clinic (Table 2). The most valued characteristics of participants’ current MS clinics were the training and knowledge of providers (49%), compassion of providers (41%), compassion of clinic staff (30%), and availability for telehealth appointments (25%). The most desired characteristics in a clinic were the training and knowledge of providers (55%), compassion of providers (54%), proximity to home (51%), and availability for urgent appointments (48%). There was a large gap (>10%) between the desired and valued (currently present) characteristics in multiple areas. This included the availability for urgent appointments, in-clinic rehabilitation therapies (physical, occupational, or speech), social worker, mental health, or nutritionist services, research opportunities, proximity to home, and compassion of providers.
Multiple sclerosis clinic characteristics currently valued or desired by participants (N = 387).

Desired clinic characteristics are those either currently valued or wished for in their current MS clinic
Seventy-seven participants (20%) reported barriers or concerns to being seen in their MS clinic. Of these 77 participants, the most frequently reported barriers included a lack of availability of open appointments (44%), transportation to or from clinic (39%), financial costs (30%) and concerns related to prior negative experiences with neurologists (27%).
The unmet support needs reported by participants are given in Table 3. Greater help or support was desired most in making lifestyle changes—including improving exercise (52%) and diet (45%). Education on MS treatments and research, navigation of insurance or patient assistance programs, navigation of disability applications, and locations of available therapies were each an unmet need reported by >20% of participants. Fifteen participants (4%) reported other support needs via free-text response—this included complementary or alternative therapies, support groups, and supportive equipment.
Unmet support needs reported by persons with multiple sclerosis (N = 387).

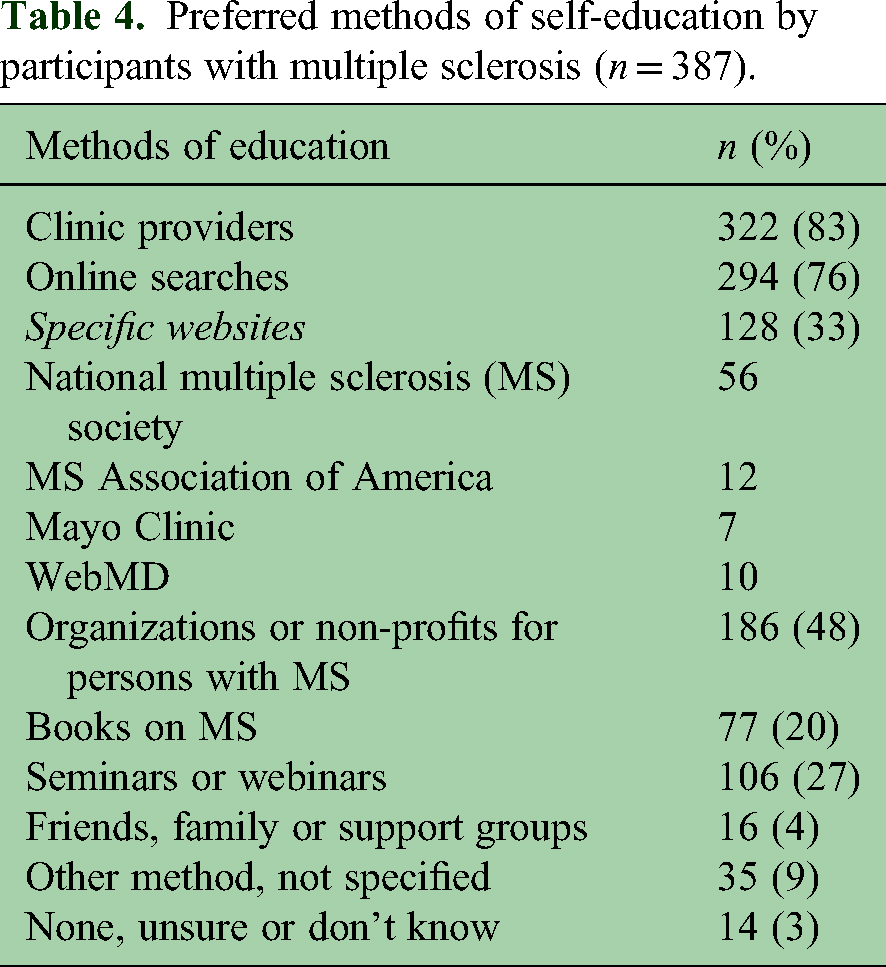
Given the unmet educational needs reported by participants, we also evaluated how participants educated themselves on MS, as shown in Table 4. Eighty-three percent learned from their clinic providers about MS topics, and 76% self-educated using online searches. Other common methods of self-education included organizations or non-profits focused on MS (48%), seminars or webinars (27%), and specific websites (33%). Websites used most often for self-education included those of the National MS Society, MS Association of America, Mayo Clinic, and WebMD.
Preferred methods of self-education by participants with multiple sclerosis (n = 387).
Because 19% of survey respondents were from Colorado, we compared between respondents from Colorado vs all other states in the USA to assess for a geographic bias to our results. Of the 13 valued clinic characteristics assessed, we found that those in Colorado more often reported valuing current research opportunities (27% vs. 14%, p = .0008) and training/knowledge of providers (62% vs. 49%, p = .008) compared to all other states. There were no significant differences for the other 11 valued characteristics. When looking at desired clinic characteristics, participants reported more often the training/knowledge of providers (66% vs. 55%, p = .04), without significant differences for the remaining 12 desired characteristics. There were no differences in the 12 support needs assessed between the two geographic groups.
Differences by provider type
We also compared the valued clinic characteristics and support needs between those who reported seeing a specialist in MS (77%) vs non-specialists (general neurologists, primary care, or other) (23%). Participants seeing a specialist in MS more often reported valuing the telehealth availability (28% vs. 17%, p = .04), infusion centers close to clinic (32% vs. 17%, p = .005), research opportunities (18% vs. 4%, p = .001), and compassion of clinic staff (34% vs. 19%, p = .008) in their MS clinics. For unmet support needs, a need for navigation of insurance or free drug programs was reported more often in those seeing an MS specialist compared to non-specialist (35% vs. 17%, p = .017), while other unmet support needs were reported at similar rates.
Discussion
This study assessed the desired clinic characteristics, unmet support needs, and barriers to care for adults with MS. We identified multiple opportunities to increase support and develop more comprehensive clinical care for this population.
In general, the training, knowledge, and compassion of providers, and urgent appointment availability were the most desired characteristics for a clinic. Given MS can be a complex and at times unpredictable disease, these desired characteristics are very understandable.
We also identified unmet opportunities for additional support by looking at the gap between desired clinic characteristics and what is currently being received. These opportunities included in clinic therapy, mental health, and nutritionist services, along with research opportunities. For unmet support needs, a high number of participants requested support in making lifestyle changes through improving exercise and diet. Education on MS and navigation of insurance, legal, financial and therapy services were other frequent support needs. While barriers to accessing care were only endorsed by 20%, the barriers reported of appointment availability, transportation to/from clinic, and financial costs are in keeping with the desired characteristics, opportunities, and support needs given above. Together, these findings assist providers and clinic staff in prioritizing clinic services and support efforts for individuals with MS.
These findings also align well with other survey-based, qualitative or mixed methods studies performed over the past several decades.2,4–6,11,14–23 Specifically, non-pharmacologic needs including financial assistance, physical and occupational therapy, and psychological care have been reported in several studies.2,4–6,11,14 Desired characteristics for an MS clinic or providers have included ability for research participation,4,18 the knowledge of MS providers, shorter clinic wait times, shorter distances to clinic, access to other supportive services such as therapies,4,19–21 and education on research or treatments.4,22 Unfortunately, little has changed over the decades since these studies began. For example, education on improving exercise and diet were the most reported unmet support needs in this study; advice on exercise and diet were also the most requested areas for education in a study from 24 years ago. 23 This may relate to the continued ubiquity of the Western-style diet and ultra-processed foods in the USA, cultural pressures that can make a healthier lifestyle difficult to achieve without additional support or national policy changes. 24 This also highlights the need to not just understand the support needs of patients with MS through research studies, but to actively develop strategies to address the results of these studies.
We also noted that about one-third of our participants were unemployed or unable to work due to health reasons or disability, similar to other studies. 25 Similarly, one-fourth of our participants reported needing more support in navigating disability applications. Together, this suggests that additional support or education around employment, vocational rehabilitation services or disability may be beneficial for individuals with MS.
While age, sex, and racial and ethnic distributions of our participants are similar to larger population-based estimates, 13 several characteristics of our participant group differ from those expected in the general MS population. For example, 19% of participants were from Colorado despite a national survey distribution. However, only three of the 38 assessed clinic characteristics or support needs were found to be significant different between participants internal and external to Colorado. Also, the rate of self-reported depression or anxiety in our study was almost twice the reported prevalence from population studies for depression (24%) or anxiety (22%). 26 This may be part of reason that in-clinic mental health services was reported as a desired MS clinic characteristic. A greater number of individuals were on medications for mood disorders than were receiving mental health therapies, perhaps reinforcing this need for access to mental health therapies. Additionally, those with a self-reported progression of MS symptoms was 64% in our study, also nearly twice another recent population-based survey study finding approximately 32% of persons with MS with self-reported gradual worsening. 27 These differences in participant characteristics may be due to differences in the survey distribution methods used in these studies, and these differences may have influenced our reported desired characteristics or support needs.
Participants seeing a specialist in MS reported several clinic characteristics that they valued or desired more than participants seeing non-specialist providers, along with a greater rate of an unmet need in navigating insurance or free drug programs. Some of these differences between specialists and non-specialists may reflect the values of individuals who specifically seek out specialist care, such as research opportunities, or the unique differences in the clinical approach of specialists and non-specialists (such as greater use of infusion or more recently approved DMTs in specialist clinics). These differences are important to recognize for both specialists and non-specialists serving MS patients, to determine what unique services they may provide or improve access to for their patients.
The ability to address this study's findings on a provider, clinic, or community level may vary depending on local resources; some may also require national advocacy efforts or changes in clinical or national culture to adequately address. Knowledge and compassion were two desired and valued provider characteristics. A provider may improve their knowledge or competence on MS through post-residency training, journal articles, conferences, or continuing education courses. Patients with MS have also recommended that providers share their qualifications and training with them to improve care, as a provider's qualification may not be immediately apparent to them. 28 Compassion from a provider may be perceived by a patient in multiple ways—including listening and paying attention, continuity and holistic care, respecting preferences, genuine understanding, counseling, body language, empathy, or spending a small portion of visit time talking about non-medical topics.29,30 Clinic visit lengths have decreased over time due to pressure to see higher patient numbers and increase revenue, 31 making cultivation of these factors in clinical practice seem challenging. Advocacy for longer visit durations may allow greater time for this cultivation. 30 However, a clinical trial found that even acknowledging psychological concerns, expressing support, and validating emotions could be done in less than 1 min, and had a notable impact on perceived compassion. 32 Developing these traits associated with compassionate care may require repeated and careful consideration of the impact of MS and a patient's journey with it on their overall well-being, and cultivating practices that acknowledge and validate the patient's emotions and the physician's support of them.
On the clinic or community levels, a multi-disciplinary effort or a partnership with MS-focused patient organizations may be needed to address some of our study's findings. Two changes on a clinic level may be the expansion of telehealth or urgent clinic appointment availability. While conversion of in-person to telehealth clinic visits or reservation of a few urgent clinic visits may be possible to accomplish in some clinics, given the long wait-times already present for neurology visits, increasing urgent appointments may also require more systemic changes. This may include advocacy for the training of more general neurologists or MS specialists, 33 or the engagement and training of advanced practice providers in MS clinics. 34 The ability to offer telehealth may also depend on national policy, as changes in Medicare and Medicaid policies during the COVID-19 pandemic allowed the large increase in telemedicine services seen subsequently. 35 Continued advocacy for the continuation of these policies will be needed to ensure their availability to providers and patients.
Another clinic change may be more purposeful assessment of ongoing support needs for an individual with MS in clinic. This could be elicited verbally by their provider as part of a standardized visit, or through the integration of validated questionnaires assessing current MS-related needs into clinic intake, such as the LUN-MS questionnaire. 10 Other clinic or community changes may include working to co-localize or improve access to dieticians or to physical, occupational, or mental health therapies, or standardizing patient education and discussion for exercise and diet. As the Western-style diet is prominent in the USA and linked to increased inflammation in persons with MS, 36 supporting patients in their exercise or diet changes after education may require connection with a health coach to maintain interest and compliance in the face of cultural pressures. Support from in-clinic social workers may assist in connection to financial or transportation resources. Education and non-medical supports are two areas where collaboration with MS-focused patient organizations or the local MS community may be especially fruitful.
Limitations
This study has several limitations. First, as a survey based on self-report, we cannot confirm key elements of the participants' medical histories, such as their diagnosis of MS or the characteristics of the clinics they receive care in. Second, we distributed this survey through social media campaigns focused on adults within the USA but could not distribute solely to individuals with MS using this method. As a result, it is difficult to estimate the specific response rate from individuals with MS who saw this survey invitation on social media, although the response rate to the survey (176 per 100,000 adults) is close to previous estimates of prevalence of MS in the USA (322 per 100,000 adults). 13
Third, this survey was iteratively developed by a regional partnership between multidisciplinary healthcare providers, non-profit staff, and individuals with MS to be distributed as part of a larger parent survey. As a result, there may have been a regional bias to the questions or response options provided in the final survey, and the depth of answers was limited. The assessed concepts, such as compassion, may also mean different things to different individuals. As a broad assessment of desired characteristics and support needs in survey form with predetermined response options, we were not able to assess in depth about all potential characteristics or needs, or about other needs external to the clinic setting that may also support patients, such as support groups. A future study focused on individual clinic preferences, needs, or barriers may be able to explore these topics more thoroughly with additional depth in survey responses, participant interviews, or focus groups.
Fourth, to check for prior responses and to contact for payment if chosen in the drawings, we obtained email addresses from participants. While only the Principal Investigator was able to view these, this provision of an identifier may have altered participant responses if they received care at our center. We attempted to minimize the potential of this bias through the national distribution of the survey through social media.
Finally, while the use of social media campaigns was effective in achieving a sampling of adults with MS from across the USA, this strategy may have resulted in a participant cohort that is different from the general MS population. Those choosing to participate may have had higher needs, concerns, or different preferences than the general MS population.
As mentioned earlier, despite the national distribution, 19% of respondents were still from Colorado, and a couple of clinic characteristics (training/knowledge of providers and research opportunities) differed from those within and outside of Colorado. A recognition of a center close to them as the sponsor of the study may have increased the willingness of these participants to join the survey study. However, many of the key findings remain similar despite these two differences. We also noted higher rates of individuals with depression and anxiety and self-reported progression within this study, whose desired clinical characteristics and support needs may differ from the general MS population.
Conclusions
Adults with MS reported multiple desired clinic characteristics and support needs that are currently unmet. Opportunities for improving care and support in the MS clinic include expanding in-clinic services, appointment availability, transportation, and education on exercise and diet. Future studies would benefit from assessing the effectiveness of expanded services or support programs.
Supplemental Material
sj-docx-1-mso-10.1177_20552173261456058 - Supplemental material for Desired clinic characteristics and unmet support needs for adults with multiple sclerosis: A cross-sectional survey
Supplemental material, sj-docx-1-mso-10.1177_20552173261456058 for Desired clinic characteristics and unmet support needs for adults with multiple sclerosis: A cross-sectional survey by Ryan Kammeyer, Stefan Sillau, Kimberly Chapman, Jennifer J. Lindwall, Kerri Cechovic, Kelsey Morrow, Christa Hutaff-Lee and Teri Schreiner in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgments
We would like to thank the clients of the Rocky Mountain Multiple Sclerosis Center for their participation and advice in survey development.
Consent for publication
Not applicable.
Consent to participate
Before beginning the survey, potential participants reviewed a form containing all necessary information regarding the study including study rationale, voluntariness, data handling, risks and benefits, and informed them that completion of the survey would imply consent.
Data availability
Deidentified data and statistical analysis plan will be shared with qualified investigators on reasonable request to the corresponding author.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report either employment by (KC, KM), or close affiliation, advocacy and grant funding (RK, JL, TS) from the Rocky Mountain Multiple Sclerosis Center, a community-based non-profit organization serving individuals with multiple sclerosis.
Ethical considerations
The Colorado Multiple Institutional Review Board reviewed the study protocol, and it was determined to be exempt from further review on January 9, 2024.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a donation from the Mowry family.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.