
Abstract
Objectives
To assess hematologic abnormalities in breastfed infants of mothers with multiple sclerosis (MS) receiving anti-CD20 therapies.
Methods
Breastfed infants with maternal anti-CD20 use were identified. Infant blood draws examined B-cell (CD19) and hematological counts.
Results
Nine of 10 identified infants had CD19 percentages in ranges expected for age. One infant had CD19 levels below the 5th percentile but was interpreted by their treating pediatrician as normal for age, with no increase in infections reported.
Discussion
The absence of significant CD19 abnormalities in our cohort may indicate infant hematology safety. This may allow mothers MS to utilize anti-CD20 therapies while breastfeeding.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic immune-mediated neurologic disorder that is most often diagnosed in women during their reproductive years. 1 While overall pregnancy rates in the United States have dropped, pregnancy rates in patients with MS have been steadily rising, with up to one-third delivering a child after MS diagnosis. 2 Earlier diagnosis, less severe disease at onset, as well as increased safety data around family planning, have likely contributed to this.
Multiple sclerosis relapse rates generally decrease during pregnancy but increase significantly postpartum, with estimates of postpartum clinical relapse in up to 30% and radiographic relapses noted in over 50%.3,4 Exclusive breastfeeding has been identified to reduce the risk of postpartum relapses, with one meta-analysis identifying a 43% lower rate of postpartum relapses compared to nonbreastfeeding.5,6 Additionally, breastfeeding is recommended by the American Academy of Pediatrics and World Health Organization for concurrent infant benefits.
There has been data identifying limited passage of anti-CD20 therapies (rituximab, ocrelizumab, ofatumumab) used in MS treatment into mature breastmilk, given their large molecular size.7,8 However, less is known about what effects, if any, these medications may have on breastfed infant hematologic parameters, particularly their CD19 counts. To date, the available information has been published as case reports or small case series.9,10 This is critically important as these B-cells are important in infant immunity and development of vaccination responses.
Our study aims to identify the frequency of abnormal infant hematologic parameters in mothers with MS who are currently breastfeeding and receiving anti-CD20 therapies.
Methods
A retrospective chart review was conducted at the University of Colorado between 2018 and 2023. Given limited safety data regarding anti-CD20 therapy and lactation available during this time period, patients who desired confirmation that there was no infant hematologic effect from maternal DMT use were provided the option to have infant bloodwork drawn with their pediatrician to look at B-cell counts. Women with MS being treated with an anti-CD20 therapy (rituximab, ocrelizumab, ofatumumab) and breastfeeding were included if they had opted to have their infants' bloodwork checked. Infants were excluded if it was unclear if mothers were actively breastfeeding at the time of blood draw or if a CD19 level was not drawn.
Collected data included dates of maternal DMT initiation postpartum, age of infant with DMT initiation and blood draw and CD19 levels. If available, infant complete blood count values and information about infection rates were also collected.
Results
Ten breastfed infants were identified for this cohort: five were exclusively breastfed. It was unknown, for the remaining five infants, whether they were exclusively breastfed or combination fed with formula. The average age of lactating mothers was 34.5 years (range 29–44) with minimal disability. Median patient determined disease steps scale value of 0 (range 0–1). All the mothers were White, with one identifying as Hispanic. Seven of the 10 mothers were on an anti-CD20 therapy preceding conception (5/7 ocrelizumab, 2/7 rituximab) with a mean of 14.9 weeks (range 2–59 weeks) between infusion and estimated conception date. The remainder were on glatiramer acetate throughout their pregnancy (n = 1), natalizumab until week 33 of pregnancy (n = 1) or no DMT prior to conception (n = 1).
All 10 infants were born at term with no reported complications during delivery. As illustrated in Table 1, on average, infants were 18.3 weeks old when DMT was reinitiated (8/10 ocrelizumab, 1/10 rituximab, 1/10 ofatumumab), and bloodwork was done on average 8.6 weeks after DMT initiation. Nine out of 10 infants had CD19 counts that were within the normal range for age, as seen in Figure 1. One infant (infant 10) had a CD19 percentage of 8.2 that was considered below the normal laboratory range of 10.2%–18.5%. This infant was delivered at 39 weeks of gestation with maternal reinitiation of ocrelizumab 600 mg at 4 weeks postpartum and infant blood draw 11 weeks postpartum. This mother received ocrelizumab 600 mg about 6 weeks prior to the estimated conception date. The interpretation of the B-cell panel by the Immunology Laboratory Director at the Children's Hospital of Colorado was “overall, the distribution of B-cell subpopulations is normal for age.” There was no increase in the number of infections noted in this infant. Two infants had white blood cell counts (WBC) that fell under normal laboratory ranges (infants 4 and 8), but with normal absolute lymphocyte counts. Both infants’ pediatricians noted no concerns with their WBC counts and no increase in the number of infections in either infant.
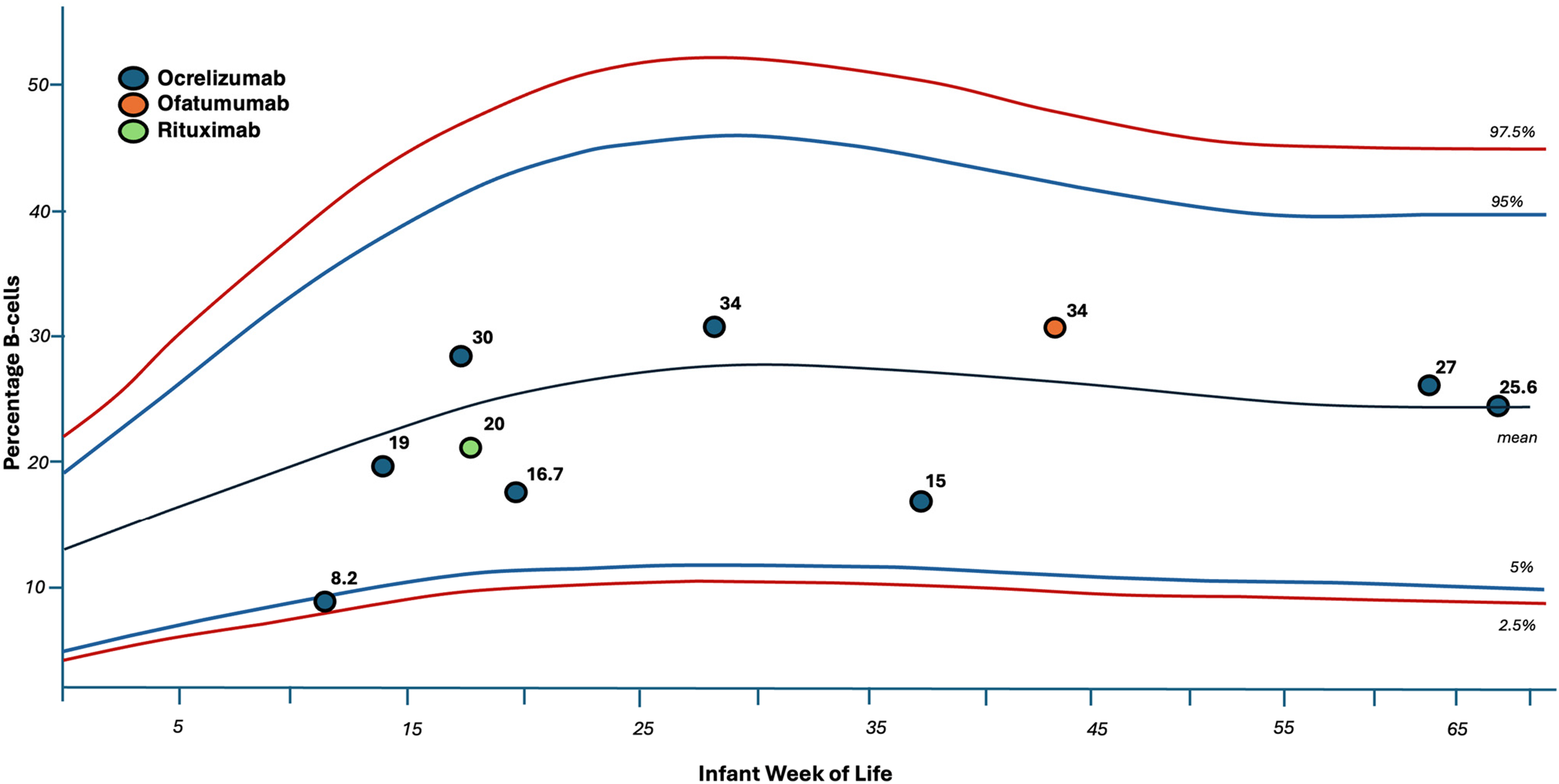
Demonstrates the individual CD19 percentages of each of the breastfed infants in this cohort. This is superimposed on a graphical representation of what is considered normal B-cell ranges for infants depending on weeks of life. 15
Hematologic parameters from breastfed infants.
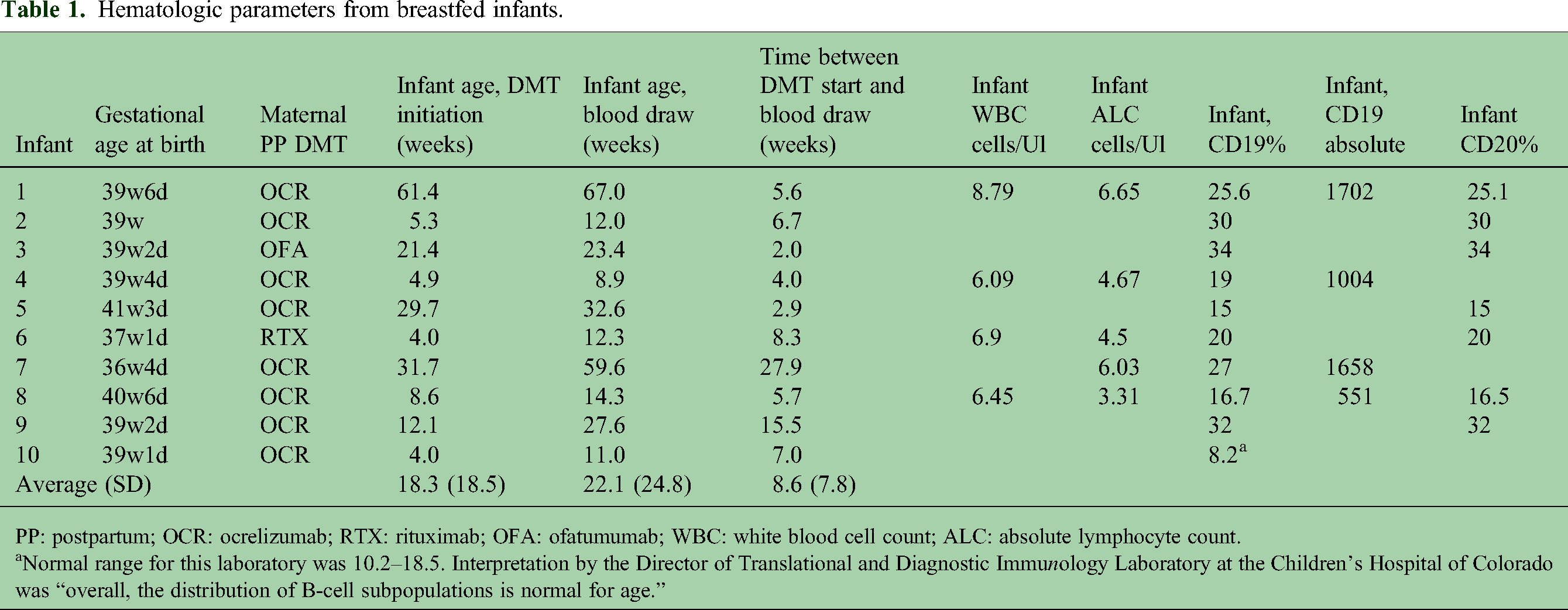
PP: postpartum; OCR: ocrelizumab; RTX: rituximab; OFA: ofatumumab; WBC: white blood cell count; ALC: absolute lymphocyte count.
Normal range for this laboratory was 10.2–18.5. Interpretation by the Director of Translational and Diagnostic Immunology Laboratory at the Children's Hospital of Colorado was “overall, the distribution of B-cell subpopulations is normal for age.”
Discussion
The decision involving DMT reinitiation postpartum and breastfeeding is critically important to patients with MS and their neurologists. Limited data causes uncertainty for both parties, potentially leading to suboptimal decision-making. Our data set helps fill in a critical gap in existing literature of the impact of maternal anti-CD20 therapy use on breastfed infant's hematologic parameters. This is one of the largest retrospective cohorts published with maternal anti-CD20 use, and on par with the total number of anti-CD20 cases observed in SOPRANINO (a phase IV study evaluating breastmilk transfer of ocrelizumab from women with MS to infants). 11 Additionally, our data complements other case series that also demonstrate limited infant CD19 effect from maternal anti-CD20 therapy use during lactation.12–14 Cumulatively, these cohorts demonstrate CD19 levels that are normal for age in 41/42 infants.
All ten infants in our cohort did not have clinically significant hematologic abnormalities. One infant with a CD19 percentage below the laboratory cutoff had a pathology review that was thought to be normal for age. While this infant did have reinitiation of maternal ocrelizumab on the earlier end of the spectrum in our cohort, this finding with CD19 counts was not seen in the other infants that restarted around similar timelines. Two infants had slightly low WBC counts but normal absolute lymphocyte counts with no concerns from their physicians nor recommendations to repeat infant bloodwork. Gestational age at birth did not play a role in hematologic abnormalities, as all babies were full term. This may indicate infant hematologic safety while breastfeeding and allow concurrent use of anti-CD20 therapies postpartum to mitigate postpartum relapse risks.
There are limitations to this study. A retrospective design limits the ability to gather some data, including whether mothers were exclusively or partially breastfeeding at the time of infant blood draw. Laboratory testing was conducted at multiple sites, so the reporting results are inconsistent. Additionally, there is notable variation in DMT reinitiation postpartum and infant blood draw dates in our cohort; while this may provide some real-world generalizability, it does introduce variability. Although all patients had similar counseling at our center, it is not clear why there was a clear cohort that reinitiated DMT later than others. Our infants were all born at term, so it is unclear what impact maternal anti-CD20 use may have on preterm infant hematologic parameters.
Overall, our study supplements existing data in the field regarding breastfed infant CD19 B-cells in mothers treated with anti-CD20 therapies. This provides important reassurance to patients with MS and allows greater flexibility with breastfeeding postpartum.
Footnotes
Acknowledgments
The authors would like to acknowledge the mothers and infants who contributed to this data set, without whom this work would not have been possible. The authors would also like to thank Genentech/Roche for providing funding for this project.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Enrique Alvarez has received compensation for activities such as advisory boards, lectures, and consultancy with the following companies and organizations: Biogen, Celgene/BMS, EMD Serono/Merck, Genentech/Roche, Horizon/Amgen, Novartis, Sanofi, Cionic, and TG Therapeutics and research support from: Atara, Biogen, BMS, Genentech/Roche, Novartis, Sanofi, TG Therapeutics, Patient-Centered Outcomes Research Initiative, National Multiple Sclerosis Society, National Institutes of Health, and Rocky Mountain MS Center. Anna Shah has received compensation for consultancy for EMD Serono/Merck, Genentech/Roche, Novartis, Horizon/Amgen, and TG therapeutics and has received research funding or been the primary investigator in clinical trials sponsored by Genentech/Roche, Novartis, Biogen, and the Rocky Mountain MS Center.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Genentech.