
Abstract
Introduction
Shared decision-making is advocated in treating patients with multiple sclerosis (pwMS), enabled by the wide range of disease-modifying treatments (DMTs). However, the role of psychological characteristics in treatment decisions remains understudied.
Methods
In a prospective study, pwMS completed the Big Five Trait inventory, UPPS Impulsive Behaviour Scale and Brief COPE at treatment initiation. Associations between choosing high-efficacy DMTs (H-DMT; natalizumab, anti-CD20 monoclonal antibodies) versus low/moderate-efficacy DMTs were analysed using logistic regression, for each dimension separately, then in a multidimensional model. Propensity scoring adjusted for MS-associated determinants of DMT choice (sex, age, disease duration, prior DMT, relapse in previous year, Expanded Disability Status Scale [EDSS]).
Results
Of 148 pwMS (75.7% female, age 36.5 years [SD 9], EDSS 1.0 [IQR, 0–2]) 53.4% initiated H-DMT. Higher active coping (adjusted odds ratio [aOR] 1.59, p = 0.024) and openness (aOR 1.48, p = 0.046) were significantly associated with H-DMT choice, with trends for extraversion (aOR 1.38, p = 0.097), supportive coping (aOR 1.42, p = 0.069), and higher perseverance (aOR 1.43, p = 0.068). In the multidimensional model, neuroticism demonstrated the most substantial association (aOR 2.17, p = 0.005).
Conclusion
Personality structure, particularly neuroticism, active coping and openness may influence treatment decisions among pwMS.
Introduction
For multiple sclerosis (MS), a broad variety of disease-modifying treatments (DMTs) is available, which differ in both their efficacy for suppressing inflammatory disease activity as well as in their respective risk profile, adverse events, and mode of application.1,2 With treatment paradigms shifting toward the early use of high-efficacy DMT (H-DMT), the availability of multiple options with comparable efficacy enables greater incorporation of personal preferences of people with MS (pwMS), thus, complying even more with the demand for a shared decision-making process. 3
Although most pwMS are intrinsically motivated to start treatment, up to 70% of pwMS have been found to be reluctant to initiate H-DMT despite best-practice recommendations. 4
However, personal preferences are affected by psychological characteristics such as personality traits, impulsivity, and coping strategies. 5 While the influence of personality traits on treatment decisions has not been extensively explored, previous studies have reported an association of high-risk-seeking behaviour with choosing H-DMT, whereas avoidant coping was negatively associated with the likelihood of initiating treatment.6–9
The PeRiCoMS battery, comprising the Big Five Trait inventory (B5T), the UPPS Impulsive Behaviour Scale, and the Brief COPE, was shown to provide a practicable measure to evaluate personality, risk, and coping in pwMS with the goal of contributing to improved shared decision-making in future clinical practice. 10
Here, we aimed to examine whether personality traits, coping strategies, and impulsivity influence the selection of H-DMT.
Material and methods
In an ongoing prospective study at the Department of Neurology of the Medical University of Vienna, 148 patients completed the PeRiCoMS battery at treatment initiation between October 2020 and July 2025 (see Figure S1). 10 Based on their clinical characteristics and medical indications, patients were offered all guideline-concordant DMT options together with their respective risk-benefit profiles. In a shared decision-making process, a specific substance was then chosen following an extensive discussion of advantages and disadvantages of each DMT option with the treating physician and in line with patients’ individual preferences. Following the final treatment decision, pwMS completed the questionnaires independently and without physician supervision. Patients included in this study were aged 18 years or older and had a confirmed diagnosis of relapsing MS according to the 2017 revised McDonald criteria. 11 Patients were excluded if they had other relevant neurological diseases besides MS, or if they presented with severe depression or anxiety. DMTs were categorized according to their efficacy based on the current guidelines of the German Neurological Society (DGN). 12 Low/moderate-efficacy DMT (L/M-DMT) included beta interferons, dimethyl fumarate, glatiramer acetate, teriflunomide, sphingosine-1-phosphate receptor (S1P) modulators (i.e. fingolimod, siponimod, ozanimod and ponesimod) and cladribine. Natalizumab and anti-CD20 monoclonal antibodies (i.e. ocrelizumab, ofatumumab and rituximab) were considered as H-DMT.
Big five trait inventory
The B5T measures the five-factor personality structure consisting of extraversion, neuroticism, openness to new experiences, conscientiousness and agreeableness by ten items for each dimension. The items were answered on a Likert scale from one to five with a higher score expressing higher levels of the respective attribute.13,14
UPPS impulsive behaviour scale
The UPPS consists of 45 items quantifying four dimensions: urgency, sensation seeking, lack of premeditation and lack of perseverance. Urgency describes the tendency to behave impulsively to relieve negative emotions with awareness of potential consequences. Sensation seeking includes the drive to engage in exciting or unknown activities, neglecting consequences that could stem from it. People who lack premeditation show difficulties reflecting and evaluating negative effects before acting. Lack of perseverance is shown in people who cannot focus on unpleasant or complicated tasks. Each item was answered on a Likert scale from one to four. Higher scores reflect an increased expression of each dimension. Twenty-five items were reverse-coded and thus adjusted before summing the values for each dimension.15,16
Brief COPE
The Brief COPE inventory was translated to German with 28 items, measuring 14 different coping strategies of which 11 had sufficient psychometric properties. The four overarching coping dimensions are positive coping, active coping, supportive coping and evasive coping.17,18 Positive coping consists of acceptance, positive reframing and humour. Supportive coping measures include the amount of instrumental support, emotional support and religion. Active coping also contains the ability to plan, while evasive coping includes self-blame, denial and venting. All items were measured on a four-point Likert scale from ‘I have not been doing this at all’ 1 to ‘I have been doing this a lot’, 4 with higher scores representing increased utilization of the respective coping strategy.
Statistical analysis
Continuous variables are described with mean and standard deviation (SD) or median with interquartile range (IQR), as appropriate. Categorical variables are shown as absolute and relative frequency in percent. Associations between psychological dimensions and both demographic and clinical characteristics were quantified with Pearson or Spearman correlation, as appropriate. The influence of personality, impulsivity and coping strategies on the treatment decision of H-DMT versus L/M-DMT was analysed using logistic regression first for each z-standardised dimension separately, then combined in one model using Firth's bias-reduced penalised maximum likelihood estimation.19,20 Propensity scoring was applied to adjust for MS-associated determinants of DMT choice (i.e. sex, age, disease duration, DMT prior to baseline, relapse in the year before baseline and Expanded Disability Status Scale (EDSS) at baseline). As a sensitivity analysis for unidimensional models, cumulative logit models were estimated treating DMT category as the ordinal dependent variable (L-DMT < M-DMT < H-DMT) to control potential information loss caused by dichotomisation. For this, the propensity score for covariate balancing was calculated with a baseline logit model with L-DMT as the reference category. Sensitivity analyses for the multidimensional model included a logistic regression model with ridge penalisation, choosing the optimal regularisation parameter lambda via 5-fold cross-validation based on minimising the mean cross-validated error. Model stability was evaluated using bootstrap estimates of the beta coefficients based on 2000 resamples alongside their bias-corrected and accelerated (BCa) 95% confidence intervals (CIs). These BCa CIs represent a measure of variability and cannot be used for inference. In a sensitivity analysis, the potential effect of the treating physician was evaluated using a leave-one-out approach. For this purpose, the multidimensional analysis was repeated, each time excluding all patients treated by one physician. Additionally, possible bias related to the desire for childbearing in treatment choice was examined in the subgroup of participants for whom this information was available. Collinearity was assessed with the variance inflation factor (VIF), excluding variables with a VIF > 3. Complete case analyses were performed, and the assumption that missing values were missing completely at random (MCAR) was assessed using Little's MCAR test. All statistical analyses were conducted in R version 4.5.0 or higher. 21 Two-sided p-values < 0.05 were considered statistically significant and were not adjusted for multiple comparison, reflecting the exploratory nature of this study.
Ethics and data availability
The study has been approved by the ethics committee of the Medical University of Vienna (EK No: 1378/2020). Written informed consent was obtained from all study participants.
Anonymised data can be made available from the corresponding author upon reasonable request following approval of the data-clearing committee of the Medical University of Vienna.
Results
In the 148 pwMS included in these analyses, 112 were female (75.7%), the mean age was 36.5 years (SD 9 years) and the median EDSS was 1.0 (IQR, 0-2). Treatment was initiated with L/M-DMT in 46.6% and with H-DMT in 53.4%. Among those who initiated L/M-DMT, one (1.4%) received interferon beta, four (5.8%) teriflunomide, four glatiramer acetate (5.8%), 19 dimethyl fumarate (27.5%), 15 S1P modulators (21.7%) and 26 cladribine (37.7%). Among those treated with H-DMT, 20 (25.3%) received natalizumab and 59 (74.7%) anti-CD20 monoclonal antibodies.
Female pwMS reported higher levels of extraversion (r = 0.21) and neuroticism (r = 0.23), while sensation seeking was lower (r = −0.26). Increasing age was associated with lower neuroticism (r = −0.18), lower agreeableness (r = −0.18), lower sensation seeking (r = −0.25), and less use of supportive coping (r = −0.20), while disease duration showed only negligible correlations. PwMS with a greater disability (higher EDSS score) were more neurotic (r = 0.19), less open to new experiences (r = −0.19), and engaged in less sensation seeking (r = −0.18). Within the PeRiCoMS measures, neuroticism showed a positive correlation with urgency (r = 0.56) and lack of perseverance (r = 0.41), openness with sensation seeking (r = 0.40) and active coping (r = 0.36), and extraversion with supportive coping (r = 0.32) (see Figure S2). Meanwhile, consciousness was negatively correlated with lack of premeditation (r = −0.41) and lack of perseverance (r = −0.62), as well as agreeableness with urgency (r = −0.38) and lack of premeditation (r = −0.32).
Looking separately at each PeRiCoMS measure, active coping (adjusted odds ratio [aOR] 1.57 per standard deviation increase [95% CI 1.08–2.35], p = 0.022) and openness to new experiences (aOR 1.48 [95% CI 1.02–2.20], p = 0.046) had significantly higher odds of choosing H-DMT (see Tables 1 and 2). This corresponds to an increase in the odds for choosing H-DMT for every 1-SD increase by 57% or 48%, respectively. The same trend was found in extraversion (aOR 1.38 [95% CI 0.95–2.03], p = 0.097) and supportive coping (aOR 1.42 [95% CI 0.98–2.09], p = 0.069), while lack of perseverance showed lower likelihood of choosing H-DMT (aOR 0.70 [95% CI 0.47–1.02], p = 0.068). These trends were confirmed by unidimensional cumulative logit models (see Table S1).
Patient characteristics.
EDSS: Expanded Disability Status Scale; DMT: disease-modifying therapy.
Unidimensional logistic regression results for the association between personality traits, impulsivity and coping strategies with the choice of H-DMT.
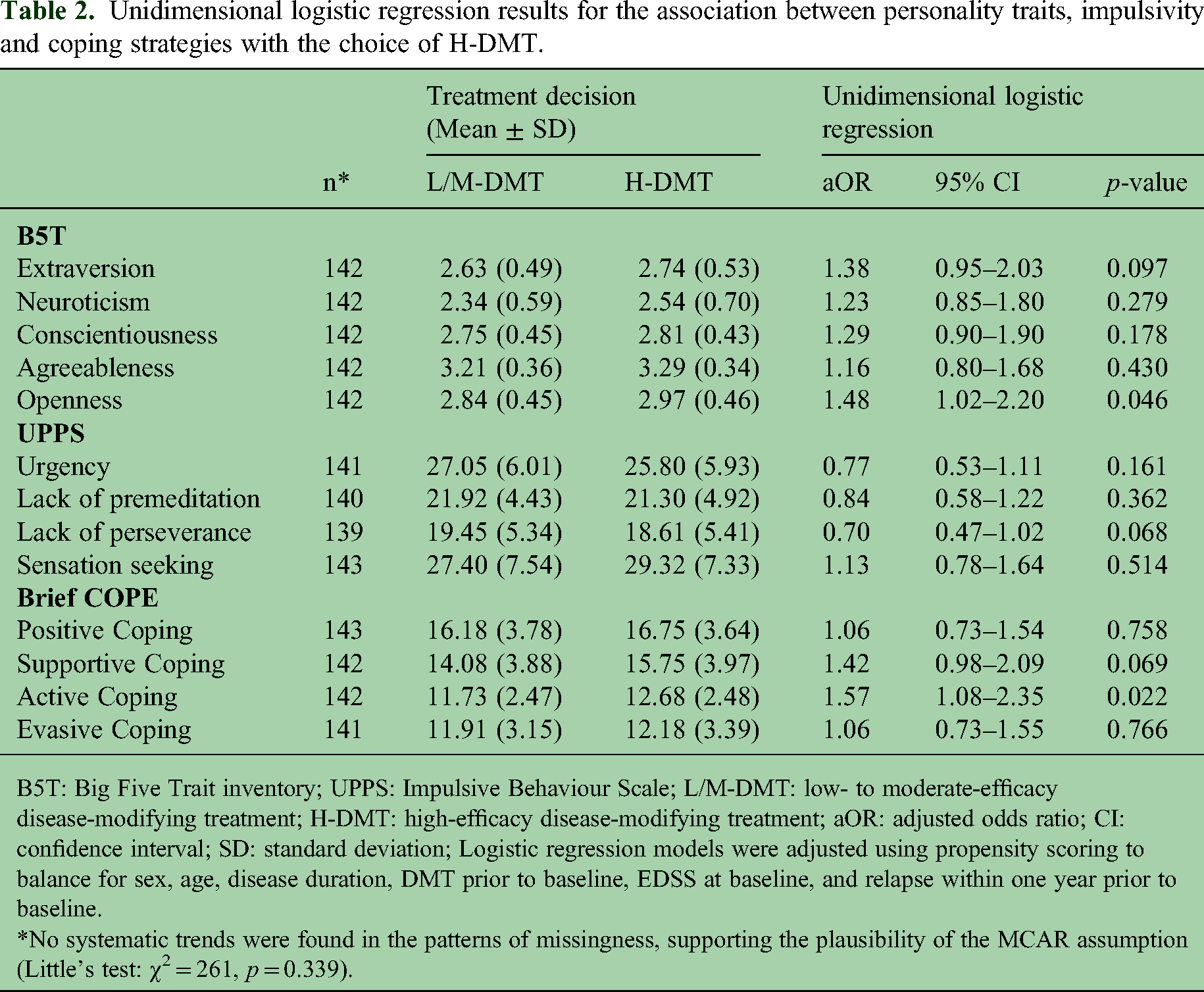
B5T: Big Five Trait inventory; UPPS: Impulsive Behaviour Scale; L/M-DMT: low- to moderate-efficacy disease-modifying treatment; H-DMT: high-efficacy disease-modifying treatment; aOR: adjusted odds ratio; CI: confidence interval; SD: standard deviation; Logistic regression models were adjusted using propensity scoring to balance for sex, age, disease duration, DMT prior to baseline, EDSS at baseline, and relapse within one year prior to baseline.
*No systematic trends were found in the patterns of missingness, supporting the plausibility of the MCAR assumption (Little's test: χ2 = 261, p = 0.339).
After integrating all dimensions into a single model, the directions of most associations remained unchanged, although their statistical significance was lost (see Figure 1). Notably, in the full model, high neuroticism was significantly related to a higher likelihood of choosing H-DMT (aOR 2.17 [95% CI 1.25–4.03], p = 0.005; Table S2). The results were similar in logistic regression with ridge penalisation, where neuroticism, perseverance, reduced urgency, active coping, supportive coping, and openness to new experiences showed the most pronounced associations with the choice of H-DMT in that order (see Table S3). Negligible psychological characteristics were conscientiousness, agreeableness and positive coping. In sensitivity analyses, neither the treating physician nor childbearing desire had a meaningful independent effect on the results.

Adjusted odds ratios with 95% confidence intervals for initiating a high-efficacy disease-modifying therapy, based on unidimensional models including one psychological dimension and the propensity score (blue, upper) and a multidimensional model including all psychological dimensions and the propensity score (orange, lower).
Discussion
To enhance our understanding of factors influencing shared decision-making in MS treatment, we used the PeRiCoMS battery to assess how personality traits, impulsivity and coping styles affect the choice of DMT.
We found that – beyond MS-specific factors – individual differences in personality structure, particularly more pronounced neuroticism and openness to new experiences, as well as a proclivity towards active coping, were associated with an increased likelihood of opting for H-DMT. A personalised approach to treatment selection, thereby allowing individual preferences to be incorporated into the shared decision-making process, is crucial for promoting adherence and treatment satisfaction.
Previous research found a discrepancy between DMT choices in hypothetical scenarios and the treatments actually received by pwMS. 22 This may partly be explained by impaired cognitive processing, reduced rationality or increased susceptibility to framing effects in pwMS when health information is presented by clinicians.23,24 However, it seems highly likely that individual differences in psychological characteristics play a role in treatment decisions by pwMS but have not yet been extensively considered.
Notably, the choice of DMTs in a hypothetical scenario seems not to align with real-world treatment decisions made by pwMS.7,22 Up to 7 out of 10 pwMS have been found to be reluctant to initiate H-DMT despite clinical justification. This was partly attributed to status quo bias – a tendency to maintain current treatment despite clinical or radiological activity – which was influenced by patients’ individual perception of the impact of MS. 4 In contrast, other studies reported that nearly half of pwMS chose H-DMTs in hypothetical treatment scenarios when there were no signs for evidence of disease activity. 7
It is known that pwMS often show an intrinsic preference for treatment initiation, partly to regain control over their disease.5,22 Our findings suggest that this preference may extend to the choice of H-DMT among pwMS exhibiting personalities with more pronounced neurotic traits. These individuals tend to experience higher anxiety levels, engage more frequently in rumination, and have reduced coping capacity in stressful situations. 25 This finding aligns with previous studies that showed pwMS with high neuroticism were more concerned about disease activity than potential adverse events. 26 As a result, the perception of control over the disease may increase in individuals with an enhanced sense of regulation over their disease. Another aspect might be a more threatening illness perception, characterized by heightened disease-related concerns and emotional impact, which may further explain the increased odds of choosing H-DMT in pwMS that are more neurotic. 27 Neuroticism was associated with greater evasive coping and elevated urgency, which may reduce the likelihood of choosing H-DMT and explain why its effect was masked in unidimensional analysis.15,25 Furthermore, neuroticism was negatively associated with self-management in pwMS in previous studies, potentially leading to greater reliance on physician recommendations for treatment choices. 28 Evasive coping, on the other hand, has been associated with delayed treatment initiation, but this effect did not appear to extend to the choice of treatment category. 8
PwMS scoring high on extraversion tended to engage more in supportive coping, while high openness to new experiences was associated with active coping strategies. PwMS who engage in active coping strategies are known to perceive a greater sense of control over their health. 29 Thus, choosing H-DMT may be interpreted as a sign of stronger motivation to act against the disease. Similarly, supportive coping was associated with initiation of H-DMT, whereas self-blame and denial were more common among those choosing L/M-DMT. Conscientiousness, agreeableness and positive coping were not meaningfully associated with treatment choice in this study.
Another important factor in the selection of H-DMT is individual risk perception. Our results show that pwMS with reduced behavioural inhibition, limited capacity to reflect on negative consequences and decreased ability to focus on complex tasks were more likely to prefer L/M-DMT. This finding contrasts with results from hypothetical scenarios, where risk-seeking behaviour was predictive of H-DMT selection even in the absence of a clinical indication. 7 This discrepancy may be explained by fundamental differences between decision-making in hypothetical scenarios and real-life clinical contexts. In hypothetical settings, pwMS are often more focused on identifying the treatment option that offers the best long-term outcomes, placing greater weight on efficacy and disease control. In contrast, real-life decisions – particularly among individuals with reduced capacity to reflect on negative consequences and difficulty processing complex information – may be more strongly influenced by immediate concerns, such as potential side effects or perceived treatment burden. For these individuals, the risks associated with H-DMT may outweigh the abstract or delayed benefits, leading them to prefer options with less efficacy despite evidence supporting early intensive treatment.
There are several limitations to this study. First, the sample size is still relatively modest, and our exploratory findings require external validation in independent cohorts with correction for multiple testing. Of note, framing effects in the presentation of health information could not be controlled for, as patients were treated by different physicians. Although sensitivity analyses did not reveal meaningful differences in results between treating physicians, further investigation is needed to directly operationalise framing effects.
Furthermore, the study cohort comprises primarily patients with short disease duration, active disease, and low disability. Thus, it remains unclear to what extent these findings generalise to pwMS with more advanced stages of disease. Other factors that might influence coping and decisions, such as education level, socioeconomic status or cognitive impairment were not controlled for in this study and should therefore be investigated in future research. Moreover, the timing of the questionnaires after the treatment-choice discussion may have influenced responses through mechanisms of cognitive dissonance and should be considered when interpreting the results. The potential impact of childbearing desire was also not systematically evaluated. However, a meaningful influence is unlikely, given that options exist for both L/M-DMTs and H-DMTs and that sensitivity analyses did not reveal an effect. Also, changes in coping and impulsivity in relation to treatment decisions over the disease course should be examined, in contrast to personality traits, which are known to remain relatively stable over time.
In conclusion, individual differences in psychological characteristics – particularly neuroticism, active coping, and openness to new experiences – were associated with the choice of H-DMTs among pwMS beyond MS-specific factors. Recognising these psychological factors may enhance the shared decision-making process. This is particularly relevant not only for treatment satisfaction and adherence, but also in situations where pwMS are hesitant or reluctant to initiate an H-DMT despite clinical indication. Equally important is the identification of risk-seeking individuals who demand H-DMTs contrary to guideline recommendations. In either case, the brief and readily available PeRiCoMS battery provides a practicable tool to assess personality, impulsivity and coping strategies both in studies and in routine clinical practice, offering more detailed information to support personalized medicine for pwMS.
Supplemental Material
sj-docx-1-mso-10.1177_20552173251408627 - Supplemental material for Association of treatment decision with personality, coping strategies and impulsivity in patients with multiple sclerosis
Supplemental material, sj-docx-1-mso-10.1177_20552173251408627 for Association of treatment decision with personality, coping strategies and impulsivity in patients with multiple sclerosis by Jan Philipp Nolte, Fabian Föttinger, Nik Krajnc, Markus Ponleitner, Fritz Leutmezer, Tobias Monschein, Paulus S Rommer, Christiane Schmied, Barbara Kornek, Tobias Zrzavy, Gudrun Zulehner, Thomas Berger and Gabriel Bsteh in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Austrian MS Research Society.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jan Philipp Nolte: has participated in meetings sponsored by, received speaker honoraria or travel funding from Novartis and Biogen. Fabian Föttinger: has participated in meetings sponsored by, received speaker honoraria or travel funding from Novartis, Biogen and Merck. Nik Krajnc: has participated in meetings sponsored by, received speaker honoraria or travel funding from Alexion, BMS/Celgene, Janssen-Cilag, Merck, Neuraxpharm, Novartis, Roche and Sanofi-Genzyme and held a grant for a Multiple Sclerosis Clinical Training Fellowship Programme from the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). Markus Ponleitner: has received speaker or consulting honoraria from Amicus, Sanofi-Aventis, and Novartis and participated in meetings sponsored by and received travel funding from Amicus, Merck, Novartis and Sanofi-Genzyme, as well as grants for clinical, research and exchange fellowships awarded by the European Academy of Neurology (EAN) and the Austrian Society of Neurology. Fritz Leutmezer: has participated in meetings sponsored by, received speaker honoraria or travel funding from Actelion, Almirall, Biogen, Celgene, Johnson&Johnson, MedDay, Merck, Novartis, Roche, Sanofi and Teva, and received honoraria for consulting Biogen, Celgene, Merck, Novartis, Roche, Sanofi and Teva. Tobias Monschein: has participated in meetings sponsored by, received speaker honoraria or travel funding from Biogen, BMS/Celgene, Merck, Novartis, Roche, Sanofi and Teva. Paulus Rommer: has received honoraria for consultancy/speaking from Alexion/Astra Zeneca, Allmiral, Amgen/Horizon, Amicus, Biogen, Merck, Novartis, Roche, Sandoz, and Sanofi. He has received research grants from Amicus, Merck, Roche, and Austrian Science Funds (FWF). Christiane Schmied: declares no conflict of interest relevant to this study. Barbara Kornek: has received honoraria for speaking and for consulting from Biogen, BMS, Johnson&Johnson, Merck, Novartis, Merz, Neuraxpharm, Roche, Teva and Sanofi outside of the submitted work. No conflict of interest with respect to the present study. Tobias Zrzavy: has participated in meetings sponsored by or received travel funding from Biogen, Merck, Novartis, Roche, Sanofi and Teva. Gudrun Zulehner: has participated in meetings sponsored by or received travel funding from Biogen, Merck, Novartis, Roche, Sanofi and Teva. Thomas Berger: has participated in meetings sponsored by and received honoraria (lectures, advisory boards, consultations) from pharmaceutical companies marketing treatments for MS: Allergan, Bayer, Biogen, Bionorica, BMS, Eisai, Genesis, GSK, Jazz Pharma, Horizon, Janssen, MedDay, Merck, Neuraxpharm, Newbridge, Novartis, Octapharma, Roche, Sandoz, Sanofi, Teva, TG Therapeutics and UCB. His institution has received financial support in the past 12 months by unrestricted research grants (Biogen, Bayer, BMS, Merck, Novartis, Roche, Sanofi, Teva) and for participation in clinical trials in multiple sclerosis sponsored by Alexion, Bayer, Biogen, Merck, Novartis, Octapharma, Roche, Sanofi, Teva. Gabriel Bsteh: has participated in meetings sponsored by, received speaker honoraria or travel funding from Biogen, BMS, Heidelberg Engineering, Janssen, Lilly, Medwhizz, Merck, Neuraxpharm, Novartis, Roche, Sanofi, Teva and Zeiss, and received honoraria for consulting Adivo Associates, Biogen, BMS, Janssen, Merck, Novartis, Roche, Sanofi and Teva. He has received unrestricted research grants from BMS and Novartis. He serves on the Executive Committee of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) and the Board of Directors of the International Multiple Sclerosis VisualSystem Consortium (IMSVISUAL).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.