
Abstract
Background
As knowledge is limited about the real-world impact of relapse among patients with neuromyelitis optica spectrum disorder (NMOSD), we aimed to assess the impact of relapse(s) on patient disability, clinical outcomes, and patient and caregiver burden in a real-world setting.
Objective
To assess how NMOSD relapses impacts patient and caregiver burden.
Methods
Data were drawn retrospectively from the Adelphi Real World NMOSD Disease Specific Programme, a cross-sectional survey of neurologists and patients with NMOSD patients in five European countries from January–June 2023. Neurologists reported patients’ demographics, caregiver involvement and clinical outcomes. Analyses were bivariate.
Results
Overall, 99 neurologists provided data for 433 patients. In total, 128 patients had a relapse since their initial attack (1 relapse, 64.1%; 2 relapses, 18.8%; ≥ 3 relapses, 17.2%). Patients who had relapsed once had higher rates of control deficit for bladder (40.2% vs. 25.6%, p < .001) and bowel (8.5% vs. 5.6%, p = .042), which increased with additional relapses. Relapsed patients also required more caregiver support (41.4% vs. 31.1%, p = .048), often their partner (41.4% vs. 31.1%, p = .046).
Conclusions
NMOSD relapse occurrence was associated with debilitating symptoms and more caregiver support, highlighting the need for more highly effective interventions to prevent patient and caregiver burden.
Keywords
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a rare and debilitating autoimmune disease of the central nervous system (CNS), characterized by symptoms such as blindness and paralysis, which can lead to significant disability and mortality.1,2 Typically, the disease follows a relapsing course, with exacerbations often associated with incomplete recovery, resulting in cumulative neurological damage. This includes motor and sensory deficits, visual impairment, limited ambulation and manual dexterity, pain, and bowel/bladder dysfunction. 2 NMOSD is less common in White populations compared to Asian and African ethnic groups, 3 predominantly affecting females, particularly those of reproductive age. Approximately 80% of patients with NMOSD are aquaporin-4 antibody-positive (AQP4-Ab+). 4
The cumulative damage from multiple relapses in NMOSD is linked to poor health-related quality of life (HRQoL) and long-term disability, especially in patients with AQP4-Ab+ NMOSD. 5 The unpredictable nature of relapses also has a negative psychological effect, which can lead to a loss of independence and functioning. Consequently, both professional and non-professional caregiver support is often required, resulting in a caregiver burden which commonly goes unrecognised.
The risk of NMOSD relapse is reduced with off-label maintenance immunosuppressive agents (azathioprine, mycophenolate mofetil, oral steroids, rituximab and tocilizumab).6,7 Recently, four monoclonal antibodies (mAbs), eculizumab, ravulizumab, inebilizumab, and satralizumab, were approved as maintenance therapies for AQP4-Ab+ NMOSD. 8 A recent network meta-analysis showed that eculizumab and ravulizumab, complement C5 inhibitors, are more effective in reducing the risk of relapses in patients with AQP4-Ab+ NMOSD compared to other treatments with different mechanisms of action; 9 however, the risk of relapse still remains. 10
Despite a rising number of registries generating real-world evidence, there is little evidence about the impact of one or more relapses on clinical outcomes or how patients and caregivers are affected.
Aim of the study
The aim of this study was to assess the impact of NMOSD relapses on patient disability, clinical outcomes, and subsequent patient and caregiver burden in a real-world setting.
Materials and methods
Study design
Data were extracted from the Adelphi Real World NMOSD Disease Specific Programme (DSP)™, a cross-sectional survey, with retrospective data collection, of neurologists and their NMOSD patients in France, Germany, Italy, Spain and the UK between January and June 2023. The DSP methodology has been previously described,11,12 validated, and demonstrated to be representative and consistent over time.13,14
Physicians were eligible to participate in the DSP if they were personally responsible for treatment decisions and management of patients with NMOSD. Physicians were recruited in a geographically representative manner, and data collection took place in secondary neurology services (public or private hospitals, clinics, or offices).
Each physician was instructed to complete a survey for four to eleven consecutively consulting patients with AQP4-Ab+ NMOSD. Physicians reported patients’ demographics, clinical assessments, treatment history, and clinical outcomes. Completion of the survey was undertaken through consultation of existing patient clinical records, as well as the judgement of the respondent physician, which is consistent with decisions made in routine clinical practice.
Patients for whom a physician completed a survey were then invited to complete a patient self-reported questionnaire. Patients provided informed consent to participate. Patients were eligible for inclusion if aged ≥18 years with a physician-confirmed diagnosis of AQP4-Ab+ NMOSD and were not involved in a clinical trial at data collection. The patient-reported questionnaire included validated instruments measuring emotional and physical impact associated with NMOSD, including the 20-item Short Form Health Status questionnaire (SF-20) 15 and the EQ-5D-5L (tariff). 16 Patients were also asked about the impact of NMOSD on their care needs and use of home modifications and mobility aids.
Data analysis
As the primary objective of the survey was descriptive, with no a priori hypotheses specified, the sample size was constrained by the duration of the survey period. Therefore, formal sample size calculations were not applicable and were not performed. Patients were stratified into four cohorts, namely those who had relapsed since their initial attack (1 relapse, 2 relapses or ≥3 relapses), and those with a single attack who had not relapsed at the time of data collection.
Continuous data are expressed as means and standard deviation (SD) and compared using ANOVA or t-test. Categorical variables, summarized by frequencies and proportions, were compared using Fisher's exact, Mann‒Whitney, χ2 or Kruskal‒Wallis tests, as appropriate. Missing data were not imputed; therefore, the base of patients for analysis could vary from variable to variable and is reported separately where appropriate.
Inverse probability weighting regression adjustment (IPWRA) was used to compare treatment outcomes and well-being in patients who had or had not relapsed, adjusting for age, sex and time since diagnosis. IPWRA estimates the average treatment effect (ATE), and the potential-outcome means (POMs). Linear regression was used to assess differences in continuous numeric outcomes across the four cohorts, while logistic regression was used to assess differences in binary outcomes across the four cohorts.17,18 Analyses were conducted using Stata Statistical Software 17.0.5 (StataCorp. 2021; StataCorp LLC, College Station, TX, UK).
Ethical considerations
Data were collected according to European Pharmaceutical Marketing Research Association guidelines and thus did not require ethics committee approvals. 19 The survey materials were submitted to the PEARL Institutional Review Board (reference #22-ADRW-176) and deemed to be exempt. The survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 1996, 20 Health Information Technology for Economic and Clinical Health Act legislation, 21 and the Declaration of Helsinki
Using a checkbox, patients provided informed consent to take part in the survey. Data were collected in such a way that patients and physicians could not be identified directly. All data were anonymised and aggregated prior to receipt and analysis.
Results
Demographic characteristics
Overall, 99 neurologists provided data for 433 patients with AQP4-Ab + NMOSD across France (n = 71; 16.4%), Germany (n = 100; 23.1%), Italy (n = 95; 22.099%), Spain (n = 103; 23.8%) and UK (n = 64; 14.8%). In total, 128 patients had a relapse since their initial attack (1 relapse, 64.1%; 2 relapses, 18.8%; ≥ 3 relapses, 17.2%).
Patients who relapsed were older than those with a single attack [mean (SD) age was 44.2 (11.9) (1 relapse), 42.5 (12.5) (2 relapses), 48.2 (12.7) (≥3 relapses) vs 40.6 (12.1) years (single attack); p = .007] but were otherwise similar demographically (Table 1). Overall, most patients were female (63.7%), of whom 88% were of reproductive age (≤55 years of age).
Physician-reported demographic characteristics of patients with NMOSD.

NMOSD: neuromyelitis optica spectrum disorder; SD: standard deviation.
Clinical characteristics
Patients were often initially misdiagnosed, particularly in the ≥3 relapse group, commonly having their initial NMOSD attack diagnosed as optic neuritis [22.3% single attack, 40.9% ≥ 3 relapses, p = .072) or multiple sclerosis (12.5% single attack, 40.9% ≥ 3 relapses, p = .002]. The median time since patients’ initial attack and their first relapse was 1.9 years. Patients who relapsed had higher most recent mean (SD) EDSS scores at data collection [3.5 [1.94] (1 relapse), 3 [1.43] (2 relapses), 5.5 [1.90] (≥3 relapses) vs 2.5 [1.82] (single attack); p < .001] (Table 2).
Physician-reported clinical characteristics of patients with NMOSD.

NMOSD: neuromyelitis optica spectrum disorder; CIS: clinically isolated syndrome; ADEM: acute disseminated encephalomyelitis; EDSS: Expanded Disability Status Scale.
Last available EDSS Score at data collection.
Treatment patterns
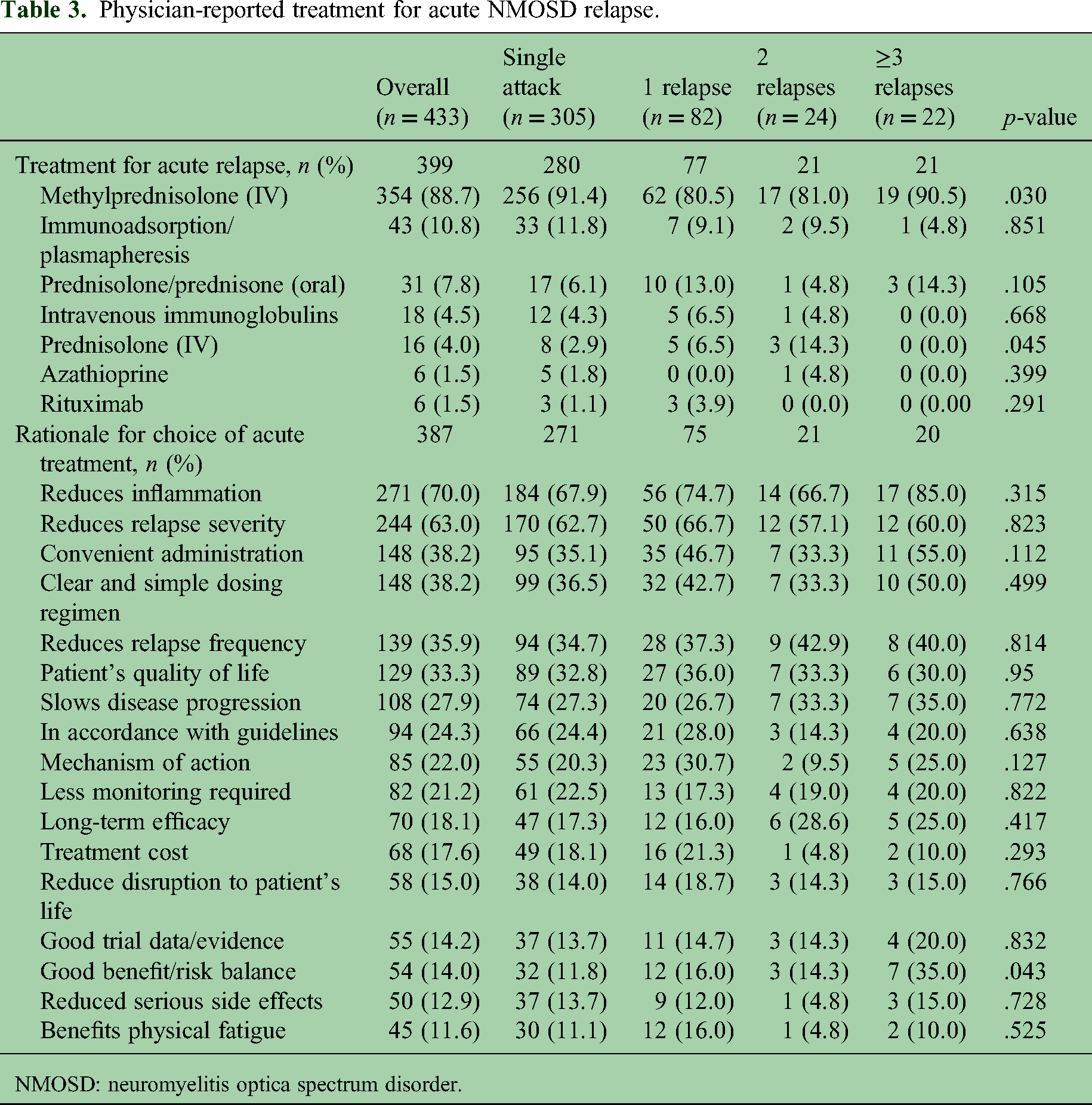
Most patients (92.1%) received acute treatment during their first symptomatic episode, predominantly methylprednisolone (88.7% of patients; Table 3). There was a marginal difference between methylprednisolone/prednisolone use during first attack in patients who relapsed compared to those who experienced single attack, although this was not significant. The rates of plasma exchange or immunoadsorption were not significantly different between the groups [9.1% (1 relapse), 9.5% (2 relapses) vs 11.8% (single attack), p = .851], and patients who had ≥3 relapses had a rate of 4.8%. Common rationale for the choice of treatment of acute attacks included reducing inflammation (reported by 70.0% of physicians) and reducing relapse severity (63.0%).
Physician-reported treatment for acute NMOSD relapse.
NMOSD: neuromyelitis optica spectrum disorder.
Maintenance treatment choice was primarily driven by the physician's desire to reduce relapse frequency (83.7%) and severity (69.0%). Fatigue (16.2%) and headache (12.2%) were the most frequently reported side effects overall. Physicians reporting of a much or very much improved clinical global impression of treatment effectiveness declined with increasing number of relapses [57.0% (single attack), 50% (1 relapse), 40.9% (2 relapses), 26.3% (≥3 relapses) p = .049; Table 4].
Physician-reported maintenance treatment of patients with NMOSD.

NMOSD: neuromyelitis optica spectrum disorder.
Symptom burden
Physician-reported symptoms related to NMOSD are summarised in Supplementary Table 3. Over half of patients (50.3%) had decreased visual acuity and 43.9% reported muscle weakness. Patients who relapsed had higher rates of blindness in one or both eyes, muscle atrophy, loss of bladder control, loss of bowel control, tactile deficit, nociceptive deficits, and back pain. The use of symptomatic treatments for NMOSD was higher in patients who relapsed than those who had a single attack, including botulinum toxin injections and baclofen; Supplementary Table 3.
Physician-reported impact on work and driving
Two thirds of patients with NMOSD were not working full time (categorised as: working part-time, retired, unemployed, or on long-term sick leave) because of their disease, broadly being more likely within the relapsed patient groups [76.7% (1 relapse), 50% (22 relapses), 83.3% (≥3 relapses) vs 56.4% (single attack) respectively, p = .036; Table 5]. Overall, 46.7% and 58.2% of patients reported inability to drive due to motor or visual disability, respectively, with no significant differences between patient groups.
Physician-reported impact on work and driving and patient reported use of aids and home modifications.

NMOSD: neuromyelitis optica spectrum disorder.
Use of aids, home modifications and caregiving
Overall, dark glasses were the most frequently utilised aid for patients with NMOSD (54.2%). There were no significant differences in patient-reported use of mobility aids, orthotics or home modifications between patient groups (Table 5).
Patients who relapsed had higher caregiver involvement, predominantly from a partner or spouse [37.8% (1 relapse), 41.7% (22 relapses), 54.5% (≥3 relapses) vs. 31.1% (single attack) respectively, p = .094; Table 6]. They also required more assistance with the following activities of daily living: home maintenance, shopping and meal preparation, dressing, and continence.
Physician-reported caregiver needs for patients with NMOSD.

NMOSD: neuromyelitis optica spectrum disorder.
HCRU
The most frequently consulted health care professionals were ophthalmologists (25.9%) and primary care physicians (22.2%), with a greater proportion of patients who relapsed consulting with physiotherapists and urologists (Supplementary Table 4). Among those who relapsed, 55.6% were hospitalized for relapse management, with the primary reason for admission due to complications related to NMOSD.
Physician-reported QoL
Patients who relapsed were more likely to be considered moderately to markedly ill at the time of data collection than patients who had experienced a single attack (42.2 vs 29.8%, p = .002), who were reported to have better quality of life (40.7% vs 59.7% p < .001; Supplementary Table 1). They were also more likely to be considered by their physicians to have NMOSD that completely limited their physical (p = .018) and social function (p = .004), as well as a greater impact on emotional well-being (p = .003). Physician-reported impact of NMOSD on patients was generally consistent across all geographic regions, but quality of life was more significantly impacted in the UK (Supplementary Table 2).
Patient-reported QoL
Six patients who relapsed and 67 who had experienced a single attack completed a questionnaire self-reporting data. Patient-reported health status was similar between those who relapsed and those who had not (
Self-reported health status in patients with NMOSD.

NMOSD: neuromyelitis optica spectrum disorder: SF-20: Short Form Health Status Survey; Lower scores indicate worse health and wellbeing expect for ‘pain’ where higher score indicates worse pain.; EQ-5D VAS: EuroQol 5 dimension visual analogue scale; ranges from 100 (best imaginable) to 0 (worst imaginable) with the patient rating themselves on how they feel on the day of answering; SD: standard deviation.
Discussion
In this large, real-world study of AQP4-Ab + NMOSD patients in five European countries, we assessed the impact of relapses on patients with NMOSD. We found that, despite different treatment options, including conventional immunosuppressive agents and novel mAb therapy, patients with relapsing NMOSD and their caregivers continued to experience a substantial disease burden. In our analysis, patients who were reported by their physician to have experienced 1 or more relapses had significantly higher rates of debilitating symptoms, with more daily activities requiring support compared to those patients who were reported to have had 3 or more relapses. Patients who were reported to have two or more relapses were also twice as likely to receive care from a healthcare professional. Approximately half the patients in our cohort had visual deficits and muscle weakness, and patients who experienced a greater number of relapses reported greater levels of disability. This highlights the importance of early and efficacious treatment to reduce the incidence of relapses and related symptoms.
We found that the majority of females who relapsed were of reproductive age, a group at risk of additional perinatal NMOSD complications.22,23 Almost a third of patients in our cohort were reported to have experienced at least one relapse, while in previous cohorts reported in the literature this proportion reached half or more.24–26 It is difficult to compare relapse rates, as they are dependent on patient population, physician record, treatment, and follow-up times.
A retrospective, single-centre study showed better outcomes and reduced disabilities when patients were treated within 14 days of symptom onset. 27 In our cohort, patients who relapsed were more likely to receive efficacious immunosuppression and monoclonal antibody therapies, including eculizumab and tocilizumab, highlighting an opportunity to improve patient outcomes by utilising effective treatments earlier in the disease course. 27
In this study, almost 90% of patients who experienced a single attack received intravenous methylprednisolone (IVMP), but only just over three quarters of patients who relapsed did. This suggests that lack of IVMP treatment was associated with a higher likelihood of relapse. Notably, our data shows that IVMP given for patients’ initial symptomatic attack reduces EDSS scores 28 and that this early treatment of IVMP improves visual acuity. 29 This suggests that patients who relapsed with a delayed diagnosis and did not receive IVMP at their initial attack may require alternative therapeutics to provide adequate relief. It is worth noting that patients who receive oral immunosuppressants often require concomitant steroids which may worsen side effects (such as infections, ophthalmologic or gastrointestinal adverse effects), therefore, worsening patient burden and QoL. 30 Furthermore, patients on these treatments still experienced relapses and long-term use of these steroids may also increase the risk of certain cancers. 31 These issues highlight why access to licensed monoclonal antibodies is important, as they offer substantially greater disease control and a favourable safety profile. Biosimilars (e.g., Rituximab, Tocilizumab, and Eculizumab) also provide cost-effective alternatives. 32 Patients still experiencing relapses whilst on maintenance treatment suggests that the lack of approved therapies for NMOSD means that many of the patients in this cohort were undertreated.
Symptom burden was significantly higher in patients who relapsed more than once, with a range of symptoms reported more commonly for patients who experienced more than three relapses. This finding supports previous studies which show an increased QoL burden for patients who experience NMOSD relapses. 33 The increased burden was reflected in the higher use of antispasmodics in these patients, suggesting physicians viewed muscle spasticity and spasms were a significant issue in this population.
Impact on daily living was high in both the relapsing and the non-relapsing cohorts, with over half of patients being affected in their ability to work or drive and having an impact on a wide range of ADLs. This was particularly the case for those patients with a history of relapse, as a significantly greater proportion were reported to not be in full-time work due to NMOSD and have impacted home maintenance, shopping/meal preparation and continence.
Over half of patients reported requiring support from an informal caregiver. For most patients, this was a spouse, with the frequency of the spouse being the caregiver increasing with the number of relapses patients experienced. In a recent study, caregivers of patients with NMOSD reported substantial burden, including heightened anxiety. 34 Although we did not study impact on carers in our cohort, it is likely that there is a comparable substantial impact present that warrants further research.
Whilst acknowledging the low base, surprisingly, patients who had experienced a single attack had the lowest EQ-5D-VAS scores overall compared to patients who had relapsed. However, patients who had experienced two or more relapses had the highest scores. There were no significant differences in EQ-5D-5L index scores. This is in contrast to data from clinical trial settings, which showed patients who had a single relapse had worse QoL than those who had not relapsed. 5 However, overall EQ-5D-5L index scores were similar to those previously reported for real-world NMOSD patient cohorts in the literature, which ranged from 0.69 35 to 0.82. 36 In contrast, physicians perceived the impact on patient QoL to be lower for those who had not relapsed than for those who had.
Overall, our study demonstrates a real-world, negative, long-term impact of NMOSD on patients especially when relapse activity is not adequately addressed. This supports the importance of disease awareness, early accurate diagnosis, and prescription of early effective treatment, to minimise relapse risk and the associated long-term burden to both patients and their caregivers.
Recent insights into the pathogenesis of NMOSD have led to the development of novel targeted and highly effective therapies for patients with AQP4-Ab+ NMOSD. These therapies provide a more personalized approach to treatment, considering factors such as disease activity, age, comorbidities, side effects, route of administration, patient choice, availability, switching between therapies, and costs. 8 However, long-term experience and therapy sequencing, as well as general risk-management for potential lifelong therapies, require further study, and the comparative efficacy of the novel therapeutic biologicals is still limited due to lack of clinical trial evidence. 37
It is vital that registries and platform trials are conducted, and that a standardized approach to the collection of real-world data be adopted in order to optimise the available treatment options that can minimise relapses in patients with NMOSD. 8
Limitations
The cross-sectional design of this survey limits conclusions about causal relationships but allows for the identification of significant associations
To minimize selection bias, physicians were asked to provide data for a consecutive series of eligible patients. Patient eligibility was based on the judgement of the respondent physician and not on a formalized diagnostic checklist; however, it is representative of the physician's real-world classification of their patients. The DSP only includes patients who are consulting with their physician. This means that patients who consult more frequently have a higher likelihood of being included
The study depends on the accuracy of physicians’ records and patients’ willingness to complete questionnaires.
Conclusion
Our real-world survey reported an association between the number of additional relapses experienced by patients since the initial NMOSD event and significant disability, as well as subsequent impact to patient HRQoL and functioning. This highlights the need for early diagnosis and effective treatment intervention to reduce relapse risk and the associated burden to patients and caregivers.
Supplemental Material
sj-docx-1-mso-10.1177_20552173251406973 - Supplemental material for The impact of relapse on patient disability, clinical outcomes, and subsequent burdens to patients with neuromyelitis optica spectrum disorder and caregivers
Supplemental material, sj-docx-1-mso-10.1177_20552173251406973 for The impact of relapse on patient disability, clinical outcomes, and subsequent burdens to patients with neuromyelitis optica spectrum disorder and caregivers by Saif Huda, Martin Kleman, Karl-Johan Myren, Mia Unsworth, Giorgio Castellano, Banu Kilic Taskopru and Kristie Fitzmaurice in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-2-mso-10.1177_20552173251406973 - Supplemental material for The impact of relapse on patient disability, clinical outcomes, and subsequent burdens to patients with neuromyelitis optica spectrum disorder and caregivers
Supplemental material, sj-docx-2-mso-10.1177_20552173251406973 for The impact of relapse on patient disability, clinical outcomes, and subsequent burdens to patients with neuromyelitis optica spectrum disorder and caregivers by Saif Huda, Martin Kleman, Karl-Johan Myren, Mia Unsworth, Giorgio Castellano, Banu Kilic Taskopru and Kristie Fitzmaurice in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
Medical writing support (including development of a draft outline and subsequent drafts in consultation with the authors, assembling tables and figures, collating author comments, copy editing, fact checking and referencing) was provided by K Ian Johnson BSc, MBPS, SRPharmS, Harrogate House, Macclesfield, UK on behalf of Adelphi Real World in accordance with Good Publication Practice (GPP) guidelines. 35 Concept development and data interpretation was assisted by Sarrina Tursunova and JT Tibung, Alexion, AstraZeneca Rare Disease. The authors received assistance in the submission of this manuscript from Natasha Jones, an employee of Adelphi Real World. All authors authorized the submission and have approved all statements and declarations included in the submission.
Author contributions
All authors were involved in the interpretation of results and writing, review & editing of the manuscript. SH, MK, KJM and BKT conceptualised the study. MU, KF and GC developed the methodology and conducted the formal analysis and visualisation of results.
Consent to participate
Using a checkbox, patients provided informed consent to take part in the survey. Data were collected in such a way that patients and physicians could not be identified directly. All data were anonymised and aggregated prior to receipt and analysis.
Data availability
All data (i.e., methodology, materials, data and data analysis) that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Mia Unsworth at mia.unsworth@omc.com.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Karl-Johan Myren and Banu Kilic Taskopru are employees of Alexion, AstraZeneca Rare Disease and own stock or stock options in AstraZeneca. Martin Kleman no longer works for Alexion, AstraZeneca Rare Disease but did at the time of writing. Mia Unsworth, Giorgio Castellano and Kristie Fitzmaurice are employees of Adelphi Real World (Bollington, United Kingdom) and have no conflicts of interest to declare. Saif Huda is funded by a National Institute for Health Research grant (NIHR304529) and NHS England Highly Specialised Services.
Ethical approval and informed consent statements
Data were collected according to European Pharmaceutical Marketing Research Association guidelines and thus did not require ethics committee approvals. 19 The survey materials were submitted to the PEARL Institutional Review Board (reference #22-ADRW-176) and deemed to be exempt. The survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 1996, 20 Health Information Technology for Economic and Clinical Health Act legislation, 21 and the Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection was undertaken by Adelphi Real World as part of an independent survey, entitled the Adelphi Real World NMOSD DSP. The DSP is a wholly owned Adelphi Real World product, and Alexion is one of multiple subscribers to the DSP. Alexion did not influence the original survey. Publication of survey results was not contingent on the subscriber's approval or censorship of the manuscript.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.