
Abstract
Background
Multiple sclerosis (MS), a chronic neurological disease, is typically managed with disease-modifying therapies (DMTs) to reduce relapse rates and slow disease progression. Some of these DMTs can cause infusion-related reactions (INRRs), which range from mild symptoms to severe allergic reactions. Corticosteroids are commonly used in premedication regimens to mitigate INRRs. However, long-term use of corticosteroids carries health risks. This study aims to compare the effectiveness of a standard corticosteroid regimen with an adjusted, low-dose regimen in reducing INRRs among people living with MS, receiving ocrelizumab (Xacrel), with the goal of optimizing safety while minimizing corticosteroid exposure.
Methods
In a single-blind, randomized, parallel-group clinical trial conducted at Sina Hospital, 200 adult patients with MS who had previously received ocrelizumab were recruited and randomly assigned to either a standard or adjusted premedication regimen groups. The standard regimen group (n = 101) received 100 mg intravenous (IV) methylprednisolone, along with cetirizine and acetaminophen tablets as premedication, while the adjusted regimen group (n = 99) received a reduced dose of 8 mg IV dexamethasone. The incidence of INRRs and their severity was monitored up to 1-hour post-infusion and 24-h post-infusion. Statistical analyses, including Chi-square tests and logistic regression, were used to evaluate the frequency of INRRs, characterize symptom profiles, and identify potential predictive factors for INRRs occurrence.
Results
Overall, the standard premedication demonstrated more efficacy in reducing the occurrence of INRRs, while the adjusted regimen group showed a significantly higher incidence of INRRs compared to the standard regimen group (78.8% vs. 40.6%, p-value <0.01). Specific INRRs symptoms, such as itching (29.3% in the adjusted group vs. 8.3% in the standard group, p-value <0.01) and throat irritation (65.7% vs. 31.7%, p-value <0.01), were notably more frequent in the adjusted regimen group. Most INRRs were mild to moderate in severity in both groups. There was no statistically significant difference in the occurrence of severe reactions between the two groups. Notably, a history of INRRs from previous infusions was identified as a strong predictor of INRRs in the current study, with an odds ratio of 6.27 (95% CI: 3.36–11.70), highlighting the importance of patients’ history in managing INRRs risk.
Conclusions
The standard premedication regimen was more effective in reducing INRRs in people living with MS, receiving Xacrel compared to the reduced corticosteroid regimen. However, the findings suggest that a lower corticosteroid regimen may be beneficial for some patients, as there was no significant difference in the incidence of severe INRRs between the two groups.
Keywords
Introduction
Multiple sclerosis (MS) is the leading cause of non-traumatic neurological disability. 1 Initially, T cells were considered the exclusive mediators of central nervous system damage in MS. However, current understanding reveals that MS immunopathogenesis is complex, involving various immune cells, including B cells, T cells, and myeloid cells. 2
Preliminary studies with anti-CD20 monoclonal antibodies have highlighted the role of B cells in the pathogenesis of MS. 3 The first anti-CD 20 medication utilized in MS was Rituximab, a chimeric monoclonal antibody of the IgG1 subtype. 4 This medication depletes B cells from the bloodstream through complement-dependent and partial antibody-dependent cytotoxicity. 5 Rituximab was initially used off-label 6 and ocrelizumab–a fully humanized monoclonal anti-CD20 antibody–received first approval from the United States food and drug administration for the treatment of relapsing-remitting multiple sclerosis (RRMS) and primary progressive MS following the phase three clinical trials of OPERA I, OPERA II, and ORATORIO. 7 Its primary mechanisms of action include antibody-dependent cellular cytotoxicity and complement-dependent cytotoxicity (CDC). 8 Notably, ocrelizumab exhibits a reduced CDC activity compared to other anti-CD20 antibodies, which may contribute to its favorable tolerance profile. 9 The antibody's structure, as a recombinant humanized IgG1 (consists of two identical heavy chains and two identical light chains), plays a crucial role in its efficacy and safety. 10 Additionally, ocrelizumab's ability to preserve plasma cells and preexisting humoral immunity may further enhance its tolerability.11,10 In individuals with RRMS, ocrelizumab is anticipated to significantly reduce relapse rates compared to interferon beta-1a, with minimal to no difference in side effects. 12
The primary adverse event documented in the clinical trials of Rituximab and ocrelizumab was infusion-related reactions (INRRs). 13 INRRs are defined as side effects that manifest within 24 h following the administration of ocrelizumab. These reactions are categorized based on the timing of their onset: during the infusion, 1-hour post-infusion, and within 24 h after the completion of the infusion. 14 The severity of these reactions can vary from serious adverse events associated with INRRs, including fatal or life-threatening outcomes, to mild, transient reactions. 15
To minimize the risk of INRRs, it is recommended to initiate the ocrelizumab infusion at a low rate and gradually increase the infusion speed. Additionally, premedication with 100 mg of methylprednisolone (or an equivalent) should be administered intravenously at a slow rate, along with the optional use of analgesics and antihistamines 30 min prior to the infusion. 14
Research indicates that accelerating the ocrelizumab administration process does not increase the risk of INRRs.16,17 Based on evidence and clinical experience, the incidence of INRRs does not appear to be a major concern, particularly when precautions such as slow infusion speed are employed. The aim of this study was to investigate the prevalence of INRRs associated with ocrelizumab (Xacrel®) and the factors influencing their occurrence when premedication protocols are adjusted with lower dose of corticosteroid, in order to consider this protocol as an alternative for patients with limitations regarding corticosteroid use.
Materials and methods
Study design
This single-blind, parallel-group trial in Sina Hospital investigated the prevalence and determinants of INRRs following Xacrel® (Iranian biosimilar ocrelizumab) infusion with premedication adjustment. The single blinding minimized bias in outcome assessment.
Participants and sampling
Participants were adults living with MS who had received at least two prior doses of ocrelizumab. Exclusion criteria included a history of severe/life-threatening INRRs as defined by the Common Terminology Criteria for Adverse Events (CTCAE), ensuring safety and focusing on the target population.
Convenience sampling was used for accessibility and efficiency. Based on the study objectives, lack of similar research, and pilot data, the minimum sample size was determined to be 70 cases per arm. Anticipating a possible 10% dropout, a minimum of 77 patients should be enrolled in each group. In this study, we have enrolled 101 patients in the standard control group, and 99 patients in the intervention group with adjusted medication.
Randomization and interventions
Following informed consent, participants were randomly assigned to one of the two premedication groups:
Intervention Group (A): 8 mg intravenous (IV) dexamethasone in 100 ml normal saline.
Control Group (B): 100 mg IV methylprednisolone in 200 ml normal saline, along with oral administration of cetirizine (10 mg) and acetaminophen (1 g).
Adjusting the premedication involves reducing the corticosteroid dose to half the standard amount (50 mg of methylprednisolone), which is equivalent to 8 mg of dexamethasone.
Random assignment was conducted in simple randomization using a computer-generated randomization sequence to ensure concealment. Both groups received their premedication 30 min before the ocrelizumab infusion. The interventions aimed to reduce INRRs risk and identify the most effective regimen.
Data collection
Patients’ baseline information and characteristics were recorded by two trained, blinded physicians using a standardized questionnaire.
Then premedication and ocrelizumab infusion was administered by two trained nurses who were not blind to the treatment condition, as no placebo was used for acetaminophen and antihistamine.
INRRs were defined as adverse events occurring within 24 h of drug administration. These reactions could take place during the infusion, within 1 hour after the infusion, or at any point during the following 24 h. INRRs could present as a variety of new symptoms, including itching, skin rash, fatigue, cough, dyspnea, throat irritation, faint, fever, chills, flushing, nausea, headache, dizziness, tachycardia, flu-like syndrome, or any other newly onset issue with no other identifiable cause. All INRRs were categorized as mild, moderate, or severe according to the CTCAE grading system. 18
Blinded physicians then followed-up with participants in person during the infusion and 1 hour after, as well as by phone, to monitor any potential INRRs within the first 24 h.
For standard care, if any participants experienced severe to life-threatening INRRs, the infusion was stopped immediately and ocrelizumab was changed to another disease-modifying therapies. In case of less severe reactions, the drug was infused at half of its initial rate after a brief pause in the infusion. Moreover, an emergency hotline was established for participants to report on any INRRs occurring outside the hospital.
We have chosen not to use antihistamines or acetaminophen in the intervention group for several reasons. According to the ocrelizumab brochure 19 antipyretics like acetaminophen are listed as optional. As such, we opted to exclude them from the abbreviated regimen. Additionally, we excluded antihistamines to evaluate their impact, allowing us to better understand whether patients experienced any issues without their use.
Outcome measures
The primary outcome was the prevalence of INRRs following the ocrelizumab infusion in intervention and control groups. Secondary outcomes included severity, as well as the potential association of various factors with their occurrence, and the impact of additional interventions, such as changes in infusion rate and/or the use of additional medications.
Statistical analysis
Descriptive statistics were used to summarize participant characteristics and the prevalence of complications among them. Besides, comparative analyses were conducted between the intervention and control groups to evaluate the effectiveness of the premedication regimens. The factors affecting the complications were measured by logistic regression and the Chi-square test was used to check the significant difference in INRRs between the two protocols. Statistical analyses were performed using SPSS version 24, with significance level set at p-value < 0.05.
Ethical considerations
The research protocol was designed in accordance with the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their enrollment in the study. Ethical approval for the study was granted by Tehran University of Medical Sciences under reference code IR.TUMS.SINAHOSPITAL.REC.1402.024. The study has also been registered in the IRCT registry with the code number IRCT20090429001859N10.
Results
Table 1 compares the demographic and clinical characteristics of participants in the intervention and control groups. The mean ± SD age was 37.77 ± 9.71 years in the intervention group and 39.48 ± 9.84 years in the control group (p-value = 0.21). In the intervention group, 80.8% (n = 80) of participants were female, compared to 76.2% (n = 77) in the control group (p-value = 0.43). The number of previous ocrelizumab doses was similar between the two groups, with averages of 4.46 ± 1.17 in the intervention group and 4.73 ± 1.57 in the control group (p-value = 0.17). Additionally, 59.6% (n = 59) of participants in the intervention group and 55.4% (n = 56) in the control group reported a history of previous INRRs (p-value = 0.53).
Baseline characteristics of participants.

These data are presented as number (percent).
These data are presented as mean (Standard deviation).
EDSS: Expanded Disability Status Scale; MS; multiple sclerosis; RRMS: relapsing-remitting MS; annual attack rate for RRMS patients.
Table 2 demonstrates the prevalence of ocrelizumab INRRs in premedication-adjusted and control groups and compares the reactions between the two groups. Overall, INRRs occurring during and up to 1 hour after infusion were more prevalent in the intervention group (n = 78; 78.8%) compared to the control group (n = 41; 40.6%) (p-value < 0.01).
The prevalence of ocrelizumab infusion-related reactions in participants.

Bold value indicates significant p values.
P-values are calculated using Chi2 analysis.
When categorizing reactions as mild, moderate, or severe, the intervention group had a significantly higher prevalence of mild (p-value < 0.01) and moderate (p-value < 0.01) reactions, while there was no significant difference in severe reactions (p-value = 0.31).
Sub-analysis of each reaction occurring during and within 1 hour after infusion regardless of their severity showed significantly higher prevalence rates in the intervention group for itching (29.3% vs. 8.9%; p-value < 0.01), skin rash (6.1% vs. 0.0%; p-value = 0.01), fatigue (4.0% vs. 0.0%; p-value = 0.04), throat irritation (65.7% vs. 31.7%; p-value < 0.01), and headache (6.1% vs. 1.0%; p-value = 0.05). However, no significant differences were found for cough, dyspnea, fainting, fever, chills, flushing, nausea, dizziness, tachycardia, or flu-like symptoms p-value > 0.05). Comparison of INRRs 24 h post-infusion revealed that only flu-like symptoms were significantly more prevalent in the intervention group compared to the control group (6.1% vs. 0.0%; p-value = 0.01).
Table 3 reports the number of participants in each study group who received interventions to manage INRRs during ocrelizumab infusion. Overall, 63 participants (63.6%) in the intervention group and 29 participants (25.7%) in the control group required interventions for symptom management, as determined by physicians or nurses (p-value < 0.01). The most common interventions included oral hydration, temporary discontinuation of the infusion, antihistamines, and reducing the infusion speed. These interventions were significantly more prevalent in the intervention group compared to the control group (p-value < 0.05).
Symptom therapy interventions during ocrelizumab infusion in participants.

Bold value indicates significant p values.
P-values are calculated using Chi2 analysis.
Table 4 evaluates demographics and clinical variables which could affect odds of INRRs in study participants. Higher disease duration was associated with lower odds of INRRs (OR: 0.94; 95%CI: 0.90–0.99). Having a history of any previous INRRs to ocrelizumab was associated with higher odds of experiencing INRRs (OR: 6.27; 95%CI: 3.36–11.70).
Assessing the impact of demographic and clinical variables on the incidence of infusion-related reactions following ocrelizumab infusion.
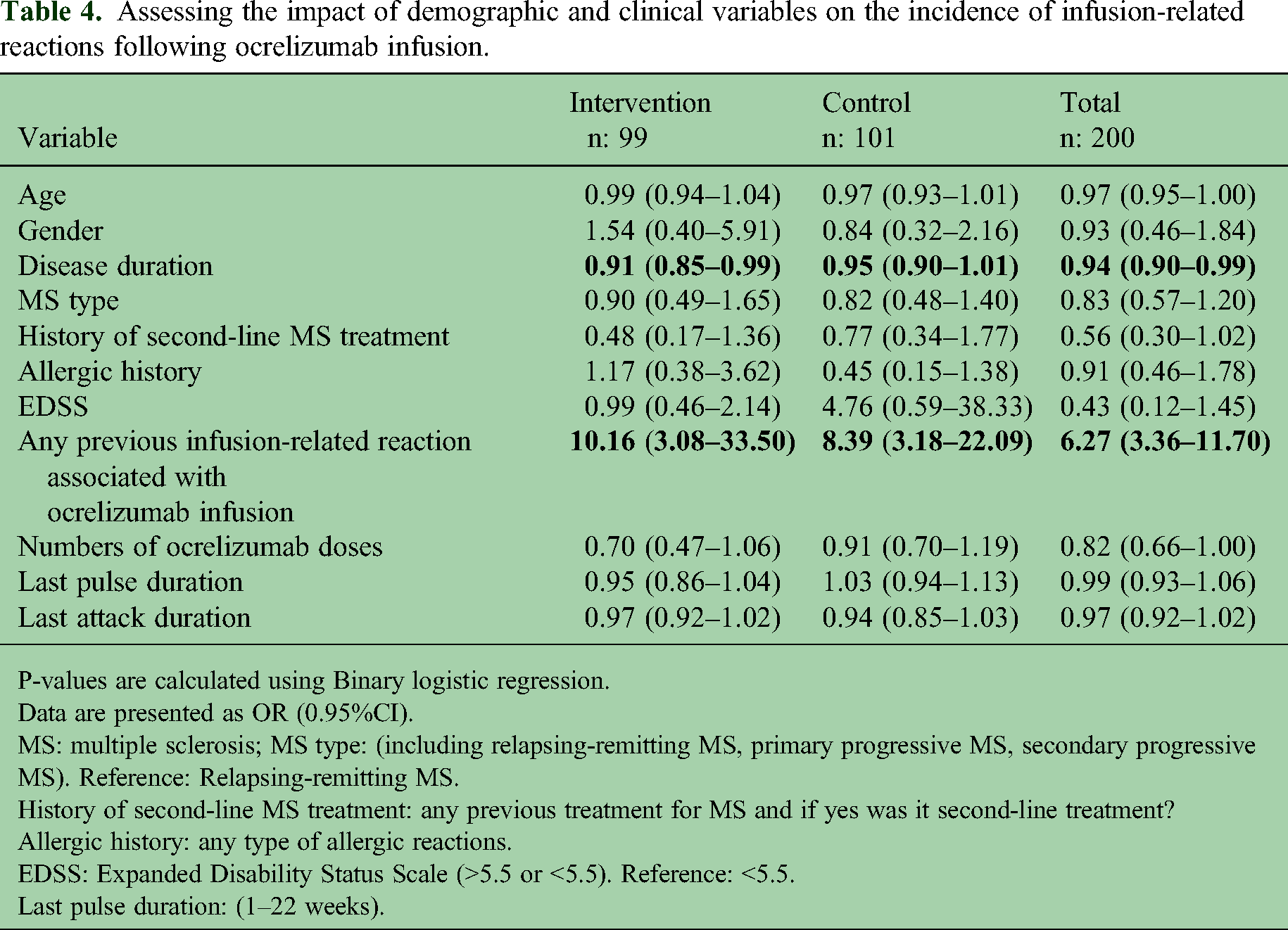
P-values are calculated using Binary logistic regression.
Data are presented as OR (0.95%CI).
MS: multiple sclerosis; MS type: (including relapsing-remitting MS, primary progressive MS, secondary progressive MS). Reference: Relapsing-remitting MS.
History of second-line MS treatment: any previous treatment for MS and if yes was it second-line treatment?
Allergic history: any type of allergic reactions.
EDSS: Expanded Disability Status Scale (>5.5 or <5.5). Reference: <5.5.
Last pulse duration: (1–22 weeks).
Discussion
The incidence of infusion-related reactions during ocrelizumab infusion
In this study, we aimed to deepen the current understanding on premedication of ocrelizumab and how adjusting them could affect INRRs. Interestingly, our results demonstrated that even though mild and moderate INRRs are significantly more prevalent among patients who received adjusted doses of premeditation, there was no significant difference in severe reactions. Furthermore, patients in the intervention group had higher rates of particular INRRs such as itching, skin rash, fatigue, throat irritation, and headache. The higher prevalence of INRRs observed only during and within 1-hour post-infusion in the adjusted premedication group suggests that this regimen does not result in more INRRs 24 h after infusion compared to the standard premedication protocol. Therefore, the effect of the adjusted regimen appears to be limited to the immediate post-infusion period and does not extend 24 h after the infusion. Consequently, this adjusted regimen may not provide adequate protection against these adverse reactions such as standard protocol. 20
Studies have reported several INRRs for people living with MS using ocrelizumab, as far as ORATORIO trial which reported more than 39% of patients experienced INRRs. 21 The symptoms of INRRs primarily include fever, chills, and myalgias, typically occurring within the first hour of infusion. Previous studies investigated how different premedication can impact the INRRs. For instance, PRECEPT trial recently showed using cetirizine instead of diphenhydramine does not lead to a higher incidence of INRRs, though the cetirizine group showed reduced fatigue symptoms compared to the other treatment. 22 Our results were in line with the previous studies as we found about 40.6% of patients receiving the normal premedication have had the symptoms.
Premedication generally improves the patient experience during ocrelizumab infusion but may be associated with both short- and long-term side effects. Notably, corticosteroids have been linked to the development of avascular necrosis (AVN) in people living with MS. 23 Previously Gokse et al. demonstrated how an annual dose of corticosteroid may increase the rate of femoral head AVN formation in people living with MS. 24 Furthermore, corticosteroids could affect patients’ blood sugar level and increase the chances of diabetes mellitus (DM) in people living with MS. 25 These concerns about the long-term safety of premedication, emphasize the need for an alternative, adjusted regimen with a minimal corticosteroid dosage, particularly for patients at high risk of side effects. 26 The current study found that adjusting the corticosteroid dose did not increase severe INRRs in patients receiving ocrelizumab, suggesting that dose reduction may be appropriate for patients with conditions like diabetes, AVN, or other situations where limited steroid use is advised.
Management of infusion-related reactions during ocrelizumab infusion
The findings in table 3 highlight the effectiveness of premedication strategies and the differences in the management of sudden INRRs between the adjusted and standard premedication protocols.
The management of INRRs in ocrelizumab-treated patients has been evaluated across several studies, including OPERA I, OPERA II, and ORATORIO trials. 14 These studies provide insight into the frequency and management strategies employed for INRRs, particularly focusing on infusion rate adjustments and symptomatic treatments.
One of the primary methods for managing INRRs involves adjusting the infusion speed. If a patient experiences an INRR, the infusion can be slowed or temporarily halted until symptoms are resolved. This approach allows for the continuation of therapy while minimizing discomfort and potential complications.14,27 In our study, we performed temporary discontinuation in 35.4% of the intervention group vs. 9.9% in the control group (p-value < 0.01), slowing the infusion speed in 5.1% of the intervention group vs. 0% in the control group (p-value = 0.02). In the pooled analysis of the OPERA studies, 7.3% of patients had their infusion speed reduced, and 8.4% of patients had their infusions interrupted. Similarly, in the ORATORIO trial, 31.4% of patients required infusion-related interventions, with most involving a reduction in infusion speed or interruptions. 14
In symptomatic treatment, the interventions administered to manage INRRs by oral hydration, antihistamines, corticosteroids, or acetaminophens. These medications can help alleviate symptoms such as itching, rash, and fever, thus improving patient comfort during the infusion process. The prevalence of these interventions in our study was significantly higher in the intervention group. However, significant ones include oral hydration in 39.4% of the intervention group vs. 18.8% in the control group (p-value < 0.01), antihistamines in 29.3% of the intervention group vs. 7.9% in the control group (p-value < 0.01). None of the patients needed hospitalization. In comparison to our study, in OPERA studies, symptomatic medications were administered to 65.4% of patients, 46.6% of patients received at least one antihistamine. Other common symptomatic treatments included corticosteroids, analgesics, and nonsteroidal anti-inflammatory drugs. In the ORATORIO study, 47% of patients received symptomatic treatments, including 30.0% of patients who were given antihistamines. Other treatments included analgesics and corticosteroids like OPERA studies. 14
Demographics and clinical variables affecting NIRRs
Table 4 evaluates various demographic and clinical factors that may influence the odds of experiencing INRRs during ocrelizumab infusion.
Notably, the analysis shows that longer disease duration is associated with lower odds of INRRs (OR: 0.94; 95% CI: 0.90–0.99), suggesting that patients with prolonged MS may develop greater tolerance to the infusion process. One possible explanation is physiological adaptation, where repeated ocrelizumab exposure induces shifts in both innate and adaptive immunity. This includes a persistent decrease in CD19+ B cells, a reduction in memory B cells, and an increase in immature and naïve B cells after two treatment cycles. Additionally, there is a rise in memory T helper cells and a decrease in regulatory T cells, while the percentage of B-cell dependent TH17.1 central memory cells drops. These immune changes may reduce hypersensitivity responses over time, lowering INRRs risk. Furthermore, patients with longer disease duration likely have accumulated experience with various infusions, which can enhance both psychological and physical tolerance, reducing anxiety and hypersensitivity reactions.28,29,30
Conversely, the history of previous INRRs associated with ocrelizumab infusion significantly increases the odds of experiencing similar reactions in subsequent infusions (OR: 6.27; 95% CI: 3.36–11.70). Research has shown that INRRs are most reported during the first infusion of ocrelizumab and tend to decrease in frequency with subsequent infusions. However, patients with a history of INRRs are at a higher risk of experiencing similar reactions again, suggesting a potential sensitization effect or a lack of tolerance development over time.17,31
In our study, gender and age were not identified as factors significantly linked to INRRs. However, it has been suggested that hormonal differences could influence the experience of side effects. For instance, fluctuations in estrogen and progesterone levels in women may affect immune system behavior, consequently influencing the likelihood of experiencing INRRs during treatment. 32 In the OPERA I and II trials, patients under 40 demonstrated a significant reduction in annualized relapse rates compared to those aged 40 and older. This suggests that younger patients may exhibit different tolerability and response profiles to ocrelizumab, which could potentially influence INRRs. Older patients may have a higher risk of adverse events, including INRRs, though age-specific data on INRRs incidence was not extensively provided in the trials. 31 This finding underscores the importance of assessing patient history prior to initiating treatment, as it can help guide clinicians in tailoring premedication and monitoring strategies (Table 5).
Previous IRR data prior to study enrollment.

One of the limitations of this study was its single-blinded design, which may have introduced observational bias. Future research should address this limitation.
Conclusion
In conclusion, our study demonstrated that while mild and moderate INRRs were significantly more prevalent among patients who received the adjusted premedication regimen, there was no significant difference in severe reactions. Tailored management of INRRs based on patient characteristics can optimize the safety of ocrelizumab premedication administration. Clinicians should consider factors such as disease duration and prior INRRs history when developing premedication plans to enhance outcomes and improve patient comfort. Although the standard regimen of premedication was more effective in controlling INRRs during ocrelizumab infusion, since severe reactions were not significantly different, reducing the corticosteroid dose could be considered in special cases, such as patients with DM, AVN, or any contraindication for IV methylprednisolone.
Footnotes
Acknowledgment
Not applicable.
Declaration of conflicting interests
Naghmeh Abbasi Kasbi, Ali Rezaei, Reyhaneh Montazeri, Sahar Nikkhah Bahrami, Nasim Rezaeimanesh, Melika Arab Bafrani, Sajjad Ghane Ezabadi, Kosar Kohandel, Faezeh Khodaie, Shima Jahani, Abdorreza Naser Moghadasi, Amirreza Azimi Saeen, Samira Navardi, Hora Heidari, Zahra Ebadi: Nothing.
Mohammad Ali Sahraian: He has received consulting and/or lecture fee from Cinnagen, Zistdaru, Cobeldarou, Merck Serono, Roche, Byer Schering, as well as travel grant from Cinnagen, Zistdaru, Zahravi, Cobeldarouand Sanofi Genzyme.
Ethical approval and informed consent statements
The research protocol was designed in accordance with the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their enrollment in the study. Ethical approval for the study was granted by Tehran University of Medical Sciences under reference code IR.TUMS.SINAHOSPITAL.REC.1402.024. The study has also been registered in the IRCT registry with the code number IRCT20090429001859N10.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Tehran University of Medical Sciences under the reference code: IR.TUMS.SINAHOSPITAL.REC.1402.024.