
Abstract
Background
Research cohort data suggest diagnostic delay in multiple sclerosis (MS) has diminished in tandem with MS diagnostic criteria revisions, yet other studies have not replicated this finding. Recent data indicate misdiagnosis of initial symptoms of MS is a frequent contributor to diagnostic delay.
Objectives
This survey study assessed diagnostic delay and misdiagnosis in an MS patient registry.
Methods
Participants completed the survey study between November 12, 2021, through December 22, 2021.
Results
There were 428 participants. Diagnostic delay was a median of 2.0 months (mean of 22.8 months, range: 0–32.9 years); 173/428 (40.4%) reported misdiagnosis of symptoms later attributed to MS, and this was associated with longer diagnostic delay (p < 0.001). Diagnostic delay decreased over time proximal to revisions to MS diagnostic criteria. 217/428 (50.7%) reported earlier symptoms retrospectively recognized as referable to MS that were not clinically evaluated, resulting in a diagnostic delay median of 5.4 years (mean 8.9 years, range: 0–47.4 years).
Conclusions
Diagnostic delay was prevalent and associated with frequent misdiagnosis of initial symptoms of MS and earlier unevaluated symptoms later attributed to MS. Studies tracing the diagnostic journey of patients with MS are needed to understand and prevent causes of diagnostic delay.
Introduction
Early diagnosis of multiple sclerosis (MS) results in early treatment and improved clinical outcomes.1,2 However, the duration of time between onset of symptoms referable to MS and its diagnosis remains suboptimal in many patients. 3 Although recent data suggest that the time to diagnosis of MS has diminished in tandem with revisions to MS diagnostic criteria aimed to improve their sensitivity, 4 some studies have not demonstrated a significant change over more than two decades. 5 The causes of diagnostic delay in MS care are often multifactorial and involve healthcare system, clinician, and patient-specific factors. 6 Many prior studies have quantified the prevalence of diagnostic delay from administrative claims data—a methodology that makes evaluation for causal factors challenging. 7 Several recent studies have suggested misdiagnosis of initial symptoms of MS, even by neurologists, is a frequent contributor to diagnostic delay.3,8 These findings suggest opportunities for interventions to expedite diagnosis in MS care. In this survey of patients with MS participating in a research registry, we retrospectively queried their diagnostic journey with an aim to determine the prevalence of misdiagnosis of initial MS symptoms, evaluate for temporal changes over time in the duration from symptom onset to MS diagnosis, and to assess factors associated with diagnostic delay.
Materials and methods
These previously unreported data are part of a larger cross-sectional patient survey study completed in collaboration with the Accelerated Cure Project and performed within their participatory research network (iConquerMS.org). Development and implementation of the survey instrument was described in prior studies.9,10 The survey instrument included demographic items and questions concerning the onset and evaluation of MS symptoms, potential misdiagnosis of those symptoms, and date of final MS diagnosis. Although subsequently reformatted for implementation online, a final draft of the survey instrument is available in supplementary materials. The survey was available to participants of iConquerMS during six weeks spanning November 12, 2021, through December 22, 2021. This study conforms to Consensus-Based Checklist for Reporting of Survey Studies 11 guidelines for survey studies.
Statistical analysis
Diagnostic delay was calculated from the time between two definitions of symptom onset and the date of diagnosis of MS: (1) symptom onset that prompted participants to seek care, and ultimately resulted in diagnosis of MS (SO-D), (2) earlier symptom onset retrospectively recognized as referable to MS, occurring prior to subsequent symptoms that resulted in care-seeking and that resulted in diagnosis (SO-e).
Andrew J. Solomon reviewed participants who reported misdiagnoses and labeled each with one of the following disease categories: neurological, psychiatric, orthopedic, rheumatological, neoplastic, infectious, metabolic, other, and unclear misdiagnosis. Andrew J. Solomon further placed each neurological diagnosis into a diagnostic subcategory where possible. Unaltered free-text participant responses regarding misdiagnosis of initial symptoms of MS are available as supplementary material.
Participant characteristics were summarized by counts and percentages (categorical variables) or means, medians, and ranges (continuous variables). Categorical variables were compared using chi-square test or Fisher's exact test. Continuous variables were compared using Welch's two-sample t test. Correlations were assessed using Pearson correlation coefficient r. All statistical tests were two-tailed; differences were considered significant at an alpha level of 0.05. We considered all analyses in this study to be exploratory; therefore, we did not adjust for multiple comparisons.
Ethics approval
Institutional review board approval was granted to Accelerated Cure Project for enrolling participants in iConquerMS by Copernicus Group IRB. Written informed consent for iConquerMS was obtained from all participants via eConsent. This specific study was also reviewed and approved by the University of Vermont Institutional Review Board, and an additional electronic consent for survey participants was obtained.
Results
Participant characteristics
There were 428 participants. As reflected in data denominators, some participants did not complete the entire survey instrument. Detailed participant demographics have been described previously.9,10 Mean age was 56.2 (range 21–81), and participants were predominantly female (324/404; 80.2%), identified as white (387/405; 90.4%) and 355/403 (86.6%) had a college degree or above; 162/404 (40.1%) were employed while 137/404 (33.9%) reported disabled work status; 357/405 (88.1%) were from 42 states within the United States; 340/422 (80.6%) carried a diagnosis of relapsing-remitting MS (RRMS); 356 study participants had completed patient-determined disease steps (PDDS) within 12 months of completing the study survey, and median PDDS score was 3.0.
Symptom onset, evaluation, and diagnosis
The onset of MS symptoms resulting in first contact with any type of healthcare provider and that ultimately led to a diagnosis of MS (SO-D) were a median of 16 years (mean of 18.4) prior to survey completion. The most frequently reported symptoms prompting care (with more than one choice permitted) were “sensory” in 193/428 (45.1%), “weakness” 143/428 (33.4%), “vision” in 113/428 (26.4%), and “dizziness” in 56/428 (13.1%). 217/428 (50.7%) reported symptoms later explained by MS prior to the symptoms that caused them to initially seek care (SO-e), a median of 24 years (mean 25.2) prior to completing the survey.
A total 400/428 (93.5%) reported evaluation by any type of healthcare provider for symptoms of MS before the doctor that evaluated them and diagnosed MS, 158/428 (39.9%) reported evaluation by at least two other providers and 63/428 (6.3%) reported evaluation by least three other providers. Participants reported waiting a median of 0.5 months (mean of 3) before evaluation by a neurologist for their symptoms.
In relation to survey completion date, 10/422 (2.3%) participants were diagnosed with MS within the last year, 73/422 (17.3%) within 5 years or less, and 91/422 (21.3%) 5–10 years prior. 131/422 (31.0%) were diagnosed greater than 10 years ago and 126/422 (29.9%) were diagnosed greater than 20 years ago.
Age at onset of SO-e was younger than participants who only reported SO-D (mean age 32.1 years compared to mean age 35.9 years; p = 0.01). There were no significant demographic differences between participants who reported SO-e compared to those that only reported SO-D including sex (p = 1), ethnicity or race (p = 0.18), or highest level of education (p = 0.71).
Diagnostic delay
Diagnostic delay from SO-D was median of 2.0 months with a mean of 22.8 months (range: 0–32.9 years), excluding 13/428 (3.0%) participants reporting dates that resulted in a negative difference. In participants reporting SO-e, diagnostic delay was a median of 5.4 years and a mean 8.9 years (range: 0–47.4 years).
Considering SO-D, there was a significant difference in diagnostic delay for participants diagnosed with MS greater than 5 years from study participation compared to less than or equal to 5 years from study participation (mean time 2.1 vs 1.2 years, p = 0.03). Considering SO-e, there was no significant difference in diagnostic delay for participants diagnosed with MS greater than 5 years from study participation compared to less than or equal to 5 years from study participation (mean time 8.7 vs 10.1 years, p = 0.44). Diagnostic delay was also evaluated by epoch proximal to the approximate timing of revisions to MS diagnostic criteria, suggesting diagnostic delay is decreasing over time (Table 1). In addition, diagnostic delay over time from SO-D and SO-e are plotted in Figure 1 and Figure 2.

Diagnostic delay by year of diagnosis. Here, diagnostic delay is quantified as the difference between the time from symptom onset that prompted participants to seek care and ultimately resulted in diagnosis of multiple sclerosis (MS) (SO-D) and the time of diagnosis. The curve shows the (smoothed) median diagnostic delay for each year, calculated using splines.

Diagnostic delay by year of diagnosis. Here, diagnostic delay is calculated as the difference between earlier symptom onset retrospectively recognized as referable to multiple sclerosis (MS), occurring prior to subsequent symptoms that resulted in care-seeking and that resulted in diagnosis (SO-e), and the time of diagnosis. The curve shows the (smoothed) median diagnostic delay for each year (based on this definition of diagnostic delay), calculated using splines.
Evaluation of diagnostic delay between epochs corresponding to revisions to multiple sclerosis diagnostic criteria.
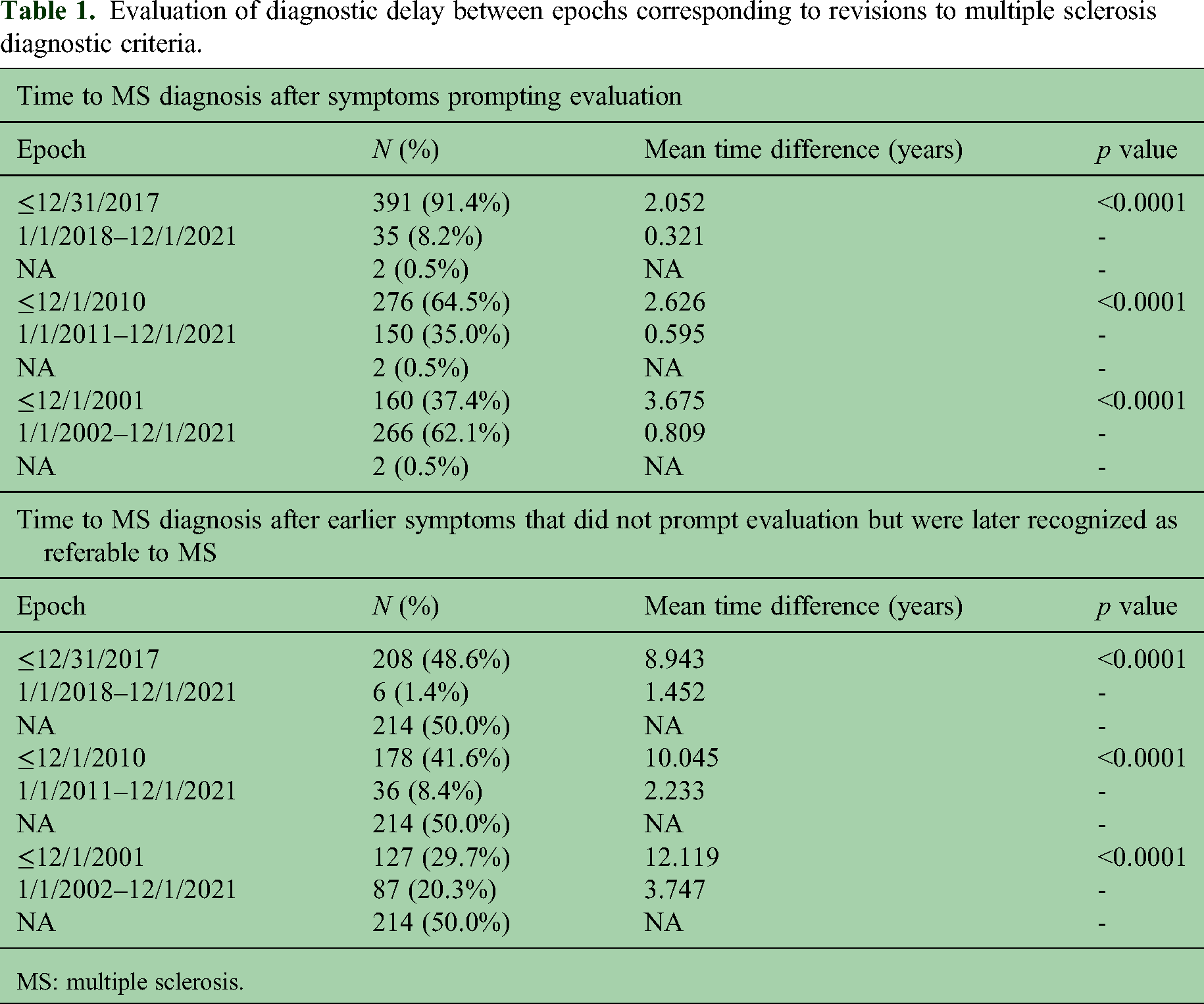
MS: multiple sclerosis.
Excluding 13 participants reporting a negative diagnostic delay, there were no significant differences between symptom onset subtype of SO-D and diagnostic delay (i.e., “vision” p = 0.27, “dizziness” p = 0.43, “sensory” p = 0.32, “weakness” p = 0.76). There was a correlation between age at SO-e or SO-D and time to MS diagnosis (Pearson correlation of −0.25, 95% CI [−0.339, −0.153] and Pearson correlation of −0.56, 95% CI [−0.652, −0.46]).
There was no association between sex and time to MS diagnosis from SO-e or SO-D (p = 0.87 and p = 0.19). There was no association between college level and greater education level (341/405) compared to less than college education level (64/405) and diagnostic delay from SO-e (p = 0.59). However, college or greater education level was associated with longer diagnostic delay from SO-D (p = 0.01).
Misdiagnosis
173/428 (40.4%) participants reported that before seeing the doctor that diagnosed them with MS, they were misdiagnosed with other conditions for the symptoms they were later told were due to MS. Reporting a previous misdiagnosis was associated with a significantly longer delay to MS diagnosis from SO-D (p < 0.001). 132 identified as female, 30 as male, and 11 did not specify sex. Neither males nor females were more likely to report 1 or more misdiagnosis of any type (p = 0.65).
A total of 150 participants reported one or more specific misdiagnoses (mean number of misdiagnoses reported was 1.6 and median was 1). In 16, an alternative diagnosis or diagnostic category was uncertain based on the diagnosis reported, and they were excluded from further analyses based on diagnostic category. 87 (58.0%) reported an alternative neurological diagnosis, 37/150 (24.7%) reported an alternative psychiatric diagnosis, and additional diagnostic category data are presented in Table 2. Of neurological misdiagnoses, compressive or other type of neuropathy excluding cranial neuropathy was most frequently misdiagnosed as MS as reported in 41/150 (27.3%), followed by migraine in 9/150 (6.0%). Further subcategories of neurological alternative diagnoses are provided in Table 2. Participants also reported nine (6.0%) misdiagnoses of initial symptoms of MS that included lack of fitness or exercise (3), overwork or exhaustion (2), and overweight or obesity (4).
Self-reported misdiagnoses of initial symptoms of MS grouped into diagnostic categories and neurological subcategoriesa.
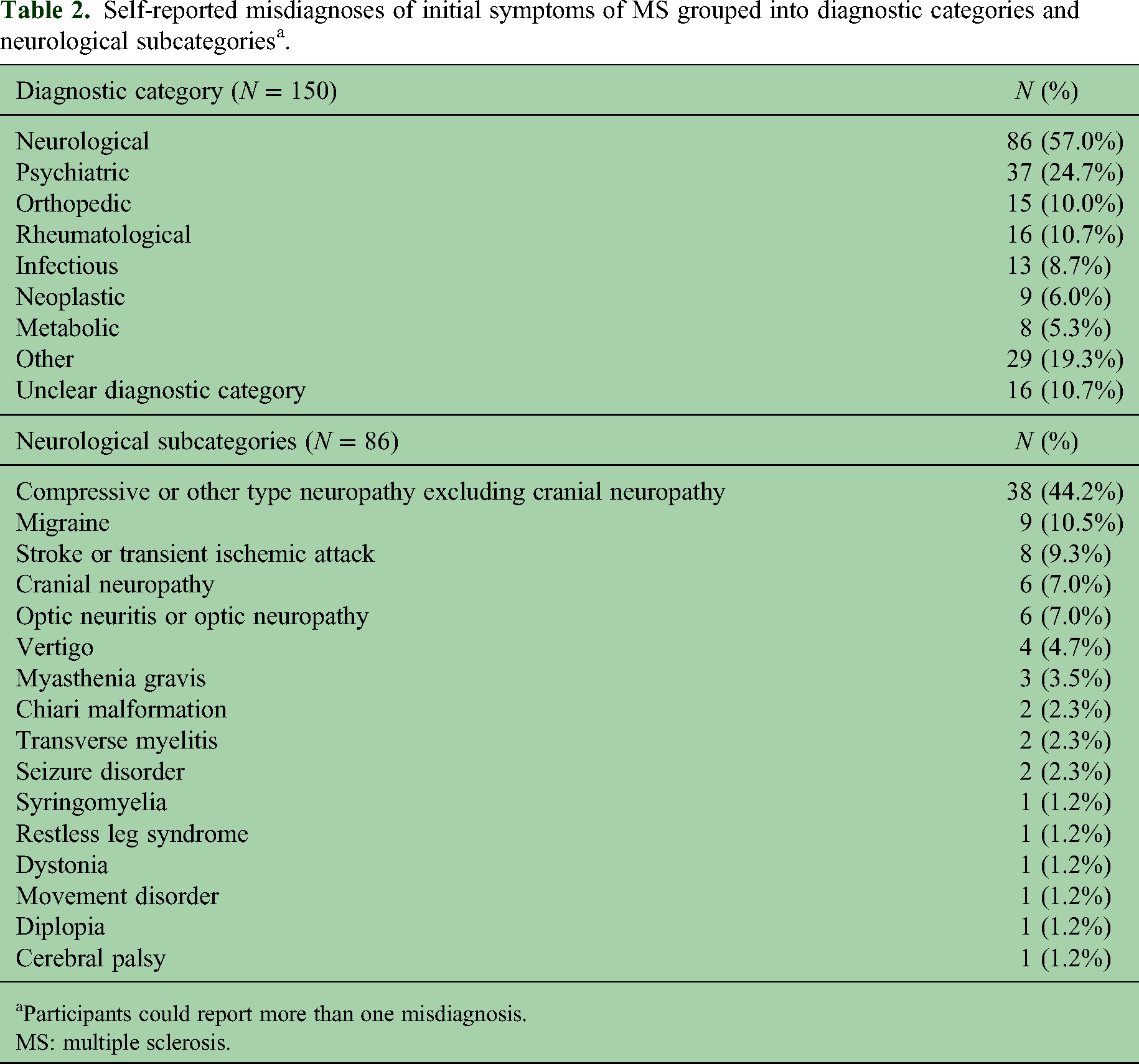
Participants could report more than one misdiagnosis.
MS: multiple sclerosis.
Diagnostic delay from SO-D was not significantly different in patients reporting neurological compared to those reporting psychiatric diagnoses (p = 0.71). There was no difference between the proportion of misdiagnosed with neurological (p = 1) or psychiatric diagnoses (p = 0.33). Among females, psychiatric misdiagnoses were not more common than neurological misdiagnosis (p = 0.06).
Discussion
In this survey of MS patients participating in a research registry, we found that diagnostic delay was prevalent and that misdiagnosis of initial symptoms of MS was frequent and associated with prolonged duration to diagnosis. The time from onset of symptoms that caused participants to seek care and diagnosis of MS was only a median of two months for the entire cohort. However, half of the participants reported earlier symptoms that were not clinically evaluated and were later attributed to MS, contributing to a median diagnostic delay of almost five and a half years. Forty percent of the participants also reported misdiagnosis of initial MS symptoms, almost doubling their mean time to diagnosis of MS. Overall, patients diagnosed more recently and during successive epochs associated with revisions to MS diagnostic criteria had shorter diagnostic delay, suggesting efforts aimed at earlier diagnosis of MS have yielded some success.
Previous studies aimed to assess trends in diagnostic delay are limited and have been primarily derived from cohorts at subspeciality centers, administrative claims data, or regional and national registries. 7 A 2005 study that included 16,681 participants from the US NARCOMS registry with symptom onset between 1980 and 2004 found that the delay from symptom onset to diagnosis was decreasing. 12 However, this study primarily includes patients from the pre-2001 McDonald criteria era. More recently and by contrast, data derived from 1422 participants in a regional Norwegian registry in a 2020 study 5 demonstrated persistent diagnostic delay from 1990 to 2017 despite successive revisions to MS diagnostic criteria aimed to improve sensitivity over that time. A study that evaluated data derived from 1174 participants from 1994 to 2020 in the Barcelona Clinically Isolated Syndrome (CIS) cohort indicated a 77% reduction in the median time from CIS to MS diagnosis from the 1983 Poser criteria to the 2017 McDonald criteria periods. 4 These conflicting data likely reflect varying definitions of symptom onset, methods to determine the time of diagnosis, and regionally specific healthcare system and patient-level differences in barriers to care and MS diagnosis. 6 More importantly, the latter study is derived from a rigorously monitored prospective research cohort at an MS subspeciality center, while the former study was reflective of a regional population–based registry which perhaps may be more reflective of “real world” data. Further studies are needed to fully understand the impact of revisions to MS diagnostic criteria in diverse populations and healthcare settings, yet our data from the population we surveyed suggest that the delay from symptom onset to diagnosis is decreasing over time.
Our data also suggest that misdiagnosis of initial symptoms of MS is frequent, and as would be expected, associated with diagnostic delay. Participants were often evaluated by two or three providers before contact with the provider who diagnosed MS, perhaps indicating diagnostic challenges or lack of expertise. Multiple sclerosis is widely recognized as a phenotypically heterogenous disease with many mimics13,14 which can at times prolong diagnostic evaluation. Recent data also suggest MS diagnostic criteria are often misunderstood or misapplied.15–17 Our findings concerning misdiagnosis are supported by a recent subspeciality single-center study from Czechia aimed to assess diagnostic delay. In this study of 146 patients with RRMS diagnosed from 2016 to 2021, diagnosis was delayed by 15% because of an initial misdiagnosis by a neurologist. Similarly, an administrative claims study representing 85% of the population of Bavaria that included 10,262 incident cases of MS from 2010 to 2017 found frequent ICD-10 codes associated with neurologic diagnoses years before MS diagnosis, suggesting misdiagnosis of earlier MS symptoms and missed opportunity for earlier diagnosis and treatment.3,18
Few studies have investigated specific causes of diagnostic delay or reported diagnoses initially mistaken for MS. Atypical presentations that require evaluation for rare alternative diagnoses 13 may delay diagnosis of MS, yet our data indicate that MS is frequently mistaken for common neurological and psychiatric conditions, perhaps supporting global data reporting a lack of expertise as a frequent barrier 6 that prevents completion of additional clinical and paraclinical investigations that could result in diagnosis of MS. A 2003 study in Israel surveyed 50 consecutive patients with MS and found 58% were initially given 41 misdiagnoses. Females were more likely to be given psychiatric misdiagnoses and males’ orthopedic misdiagnoses, 19 likely reflecting gender biases. Recent small retrospective studies from Portugal, Spain, Denmark, Italy, and Switzerland20–24 have also found that motor symptoms at presentation, progressive phenotype, older age, comorbidities, and lower educational level were associated with diagnostic delay. Our study did not find that sex, symptom presentation, or education level were associated with diagnostic delay or that psychiatric misdiagnoses were associated with female sex. However, further data from large rigorously designed multicenter studies are needed to better evaluate potential factors associated with MS diagnostic delay.
This study had limitations including self-reported diagnoses and responses potentially influenced by recall bias. Similarly, misdiagnoses could not be confirmed, and in some instances based on responses, misdiagnosis was uncertain. Given the lack of data in the literature, we sought to subcategorize misdiagnoses to provide initial data for further study—this process was necessarily subjective, and these diagnostic categories should be considered tentative. Furthermore, questions surrounding earlier symptoms later attributed to MS may be prone to error by patients or their providers. Response rate could not be accurately calculated due to survey distribution methodology, and this prevented assessment of how representative the data was from the potential participant population. Our cohort of participants was comprised predominantly of highly educated white females from the United States who participated in an MS research network, and thus the generalizability of our findings to diverse populations in the United States and more broadly is uncertain. It is possible that this population, due to these demographic characteristics, is less likely to experience a diagnostic delay in their care. In addition, the questions in our survey instrument pertaining to diagnosis had not been previously validated. However, as previously described, 10 reviewers with varied expertise reviewed the survey and contributed to its revisions, including people with MS.
Diagnostic delay and misdiagnosis of initial symptoms of MS persist and can increase the risk for disability. 1 Future studies tracing the diagnostic journey of patients with MS from first contact with their healthcare system25–27 are needed to best understand the causes of diagnostic delay and how to prevent misdiagnosis of early symptoms of MS. Although earlier administrative healthcare claims data studies have provided evidence of frequently missed symptoms of MS, 18 half of our participants reported early symptoms of MS for which they did not seek care. Future studies must also investigate whether patient-specific and/or healthcare system barriers prevent evaluation of early symptoms of MS to optimally develop interventions to address diagnostic delay in MS care.
Supplemental Material
sj-pdf-1-mso-10.1177_20552173251333390 - Supplemental material for Diagnostic delay and misdiagnosis of symptoms reported by patients with multiple sclerosis participating in a research registry
Supplemental material, sj-pdf-1-mso-10.1177_20552173251333390 for Diagnostic delay and misdiagnosis of symptoms reported by patients with multiple sclerosis participating in a research registry by Andrew J Solomon, Sarah M Weinstein, Russell T Shinohara, Samar M Aoun, Hollie Schmidt and Alessandra Solari in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-pdf-2-mso-10.1177_20552173251333390 - Supplemental material for Diagnostic delay and misdiagnosis of symptoms reported by patients with multiple sclerosis participating in a research registry
Supplemental material, sj-pdf-2-mso-10.1177_20552173251333390 for Diagnostic delay and misdiagnosis of symptoms reported by patients with multiple sclerosis participating in a research registry by Andrew J Solomon, Sarah M Weinstein, Russell T Shinohara, Samar M Aoun, Hollie Schmidt and Alessandra Solari in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-pdf-3-mso-10.1177_20552173251333390 - Supplemental material for Diagnostic delay and misdiagnosis of symptoms reported by patients with multiple sclerosis participating in a research registry
Supplemental material, sj-pdf-3-mso-10.1177_20552173251333390 for Diagnostic delay and misdiagnosis of symptoms reported by patients with multiple sclerosis participating in a research registry by Andrew J Solomon, Sarah M Weinstein, Russell T Shinohara, Samar M Aoun, Hollie Schmidt and Alessandra Solari in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Data availability
The datasets generated and analyzed during the current study are not publicly available but will be made available upon reasonable request.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew J. Solomon has received research funding from Bristol Meyers Squibb; personal compensation for consulting, advisory boards, or non-promotional speaking from Bristol Meyers Squibb, EMD Serono, Horizon Therapeutics, Kiniksa Pharmaceuticals, Octave Bioscience, and TG Therapeutics; contract research with Sanofi, Actelion, Genetech/Roche, and Novartis. Russell T. Shinohara has personal compensation for consulting to Octave Bioscience and the American Medical Association. Alessandra Solari has received personal fees for advisory board and non-promotional speaking for Almirall and Merck.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.