
Abstract
Background
This scoping review aimed to identify existing information and gaps in knowledge regarding the diversity characteristics of the multiple sclerosis (MS) population in Canada.
Methods
We searched MEDLINE, EMBASE, Cumulated Index in Nursing and Allied Health Literature (CINAHL), SCOPUS and ProQuest's global dataset of theses and dissertations from 2010 to January 12, 2024. Data sources were case reports/series, cohort studies, case-control studies, analytical cross-sectional studies, randomized clinical trials, qualitative, mixed methods, participatory studies and systematic reviews conducted in Canada, published in English or French, that included participants with clinically isolated syndrome or MS. Sample characteristics were extracted applying Cochrane's PROGRESS-Plus framework.
Results
We included 259 studies, most often studying disease-modifying therapy (24.3%) and access to care (20.9%). Among primary data collection studies 40% used one recruitment strategy, usually MS Clinics and MS Canada. Age (92.7%) and sex (86.9%) were reported most often, ≤10% of studies reported race or ethnicity; religion, sexual orientation and language were not reported.
Conclusions
We lack an understanding of characteristics of people living with MS in Canada relevant to health equity. Existing research has been insufficiently inclusive. Better reporting of diversity characteristics is needed, along with specific efforts to recruit and retain more diverse samples.
Introduction
Multiple sclerosis (MS) is a heterogeneous disease and prognostication based on clinical features is poor. 1 Recognition is growing regarding the contributions of demographic characteristics and social determinants of health (SDoH),2–6 even in countries with universal health systems such as Canada. For example, a few studies suggest that First Nations Canadians with MS have more disability progression than non-First Nations Canadians.2,7 However, Canadian national surveys assessing MS prevalence only measured age and sex. 8 Diversity also encompasses sex, gender, sexual orientation, age, race, ethnicity, comorbidity, ability and SDoH. We must understand the diversity characteristics of people with MS living in Canada to assess health disparities and develop strategies to address them.
Diversity characteristics are also associated with differential research involvement. 9 Scoping reviews of clinical trials of rehabilitation therapies found that over ninety percent of participants were White; reporting of characteristics other than age and sex was rare.10,11 The failure to recruit diverse, representative populations in MS clinical trials means that their findings do not generalize to the whole MS population, and raises concerns about health care inequities. 12
We sought to answer two questions: What are the diversity-related characteristics of the MS population in Canada? What are the gaps in our understanding of the diversity of the MS population in Canada?
Methods
As described in the protocol, registered with Open Science Framework (https://osf.io/5twdj), the scoping review was conducted following the methods delineated by Arksey & O’Malley, as updated by the Joanna Briggs Institute (JBI).13,14 We report this review according to the PRISMA Extension for Scoping Reviews. 15
Inclusion criteria
Participants
We included participants: diagnosed with MS and clinically isolated syndrome (which is often later diagnosed as MS) based on medical records, clinical assessment data, self-report or via a validated algorithm applied to administrative or similar data source (studies involving people with radiologically isolated syndrome, or MS and other diseases could be included if results were reported separately for MS); representing any diversity-related characteristics of interest including age, sex, gender, sexual orientation, race, ethnicity, comorbidity, ability, religion and social determinants of health; and living in Canada.
Concept
The review's core concept was diversity, a multidimensional construct encompassing many factors including sex, gender, sexual orientation, age, race, ethnicity, comorbidity, ability and SDoH. Race and ethnicity are distinct constructs although these terms are often used interchangeably; race is a social construct based on physical appearance such as skin color whereas ethnicity refers to a group's shared cultural practices and perspectives. SDoH refer to the social and economic conditions in which people are born, grow, live, work, play and age, and which influence health. 16 SDoH include education, neighborhood and built environment, health care access and quality, social and community contexts, and economic stability. 12
Context
This review included studies conducted anywhere in Canada, regardless of the setting (e.g. hospital, outpatient, primary care, community, long-term care). We allowed multi-country studies if characteristics of the participants from Canada were reported separately.
Types of sources
This review considered: (i) descriptive observational study designs including case series and case reports; (ii) analytical observational studies including prospective and retrospective cohort studies, case-control studies, analytical cross-sectional studies; (iii) randomized controlled trials; (iv) qualitative studies including interview-based, focus groups and other methods generating narrative data; (v) mixed methods studies; (vi) participatory studies; and (vii) systematic reviews. Primary data collection and secondary data analysis were acceptable.
Search strategy
The strategy was designed to find published and unpublished studies performed in Canada that included participants with MS from Canada. Research team members developed initial search strategies for OVID Medline and Embase databases and provided feedback for further development of the search strategy and searches conducted by an academic health sciences librarian with >20 years’ experience in conducting systematic reviews. Specifically, the research team provided search terms for MS and clinically isolated syndrome derived from a published scoping review, 17 and a geographical filter. We tested performance of an unvalidated geographic filter for Canada, lacking complete citation information, that existed for MEDLINE, EMBASE and CINAHL.18–20 As described in the registered protocol, when tested using 99 articles from 3 systematic reviews of Canadian literature,21–23 the filter with country/province names for MEDLINE had a relative recall of 91.8% and precision of 100% and for EMBASE a relative recall of 94.0% and precision of 84.8%.
The Search strategies for OVID Medline and Embase were reviewed by an independent health sciences librarian according to the criteria in PRESS Peer Review of Electronic Search Strategies. 24 Additional changes were made in collaboration with members of the research team. Databases searched [JL] were: Embase and Medline on OVID; Scopus; EBSCOhost scholarly databases (Academic Search Complete, CINAHL, MasterFILE Premier, Canadian Reference Centre); and ProQuest Dissertations & Theses Citation Index on Web of Science. Searches were conducted between 22-December-2023 and 12-January-2024 (Appendix I).
Studies published in either of Canada's official languages, English and French, were included. We limited the search to 2010 onward because the diagnostic approach to MS changed substantially after 2010, 25 and we were interested in relatively recent knowledge about the characteristics of the MS population in Canada.
Study/source of evidence selection
After the search was conducted, all identified citations were uploaded into Covidence and duplicates were removed. Systematic reviews were screened to ensure that studies within the reviews were not duplicated as independent citations. Two reviewers (RAM, MF) pilot tested the screening process on 10 articles. The remaining titles and abstracts were screened by ≥2 independent reviewers according to the inclusion criteria, following which full text articles were retrieved and reviewed by two independent reviewers. At both stages of the selection process disagreements between pairs of reviewers were adjudicated by a third reviewer.
Data extraction
A draft extraction form was developed as part of protocol registration. As planned, the form was modified after two reviewers (RAM, MF) pilot-tested data extraction in 10 articles in Covidence (see Appendix II). The data elements extracted included title, author (year), language, sample size, region where the study was performed, data source, study design, study purpose, recruitment strategy, inclusion/exclusion criteria and characteristics of the study population, based on the terms used by the authors. We applied the PROGRESS-Plus framework to data extraction. PROGRESS refers to:
Scoping reviews normally do not include risk of bias assessments because synthesis of outcomes in relation to study quality is not the goal; however, we wished to understand how selection bias might influence the findings. Therefore, we assessed bias with respect to the recruitment methods and selection procedures using an appropriate tool for each study design. These included the Newcastle-Ottawa scale for case-control and cohort studies, 28 the adaption of the Newcastle-Ottawa scale for cross-sectional studies, 29 the Cochrane revised risk of bias tool for clinical trials 30 and the Critical Appraisal Skills Programme (CASP) qualitative checklist (items 4, 6, 7) for qualitative and mixed method studies.31,32 Case series and case reports were considered to have a high risk of selection bias by design. For those tools with over one question related to recruitment and selection, we assigned a low risk of bias only if responses for all items had a low risk.
Data analysis
We used mean (standard deviation), median (interquartile range) and frequency (percent), to summarize the review findings, organized according to the PROGRESS-Plus framework.26,27 We used tables and graphical methods to present the findings. Where possible, we summarized continuous variables and proportions using random effects meta-analysis. For categorical variables, this required harmonizing some characteristics to a lowest common denominator. Thus, we report the percentage of participants with any post-secondary education, any employment, and severe disability. We quantified heterogeneity using the I2 statistic. Some findings could not be summarized because of the lack of comparability across studies, such as those related to occupation/employment or socioeconomic status. We summarized the risk of selection bias and compared it by study type and data source using Chi-squared statistics. We acknowledge that for some designs, such as qualitative studies and clinical trials, the goal of the inclusion criteria is not to obtain a sample representative of the entire population, in contrast to the goal of this review.
Results
Study inclusion
The search of databases yielded 2659 references representing 2546 studies. After removal of 1417 duplicates identified by Covidence and 63 identified manually, 1066 citations were available for screening (see Figure 1 for PRISMA flowchart). Following title and abstract screening, 464 citations remained, representing 259 unique studies. Studies were excluded most often because no diversity characteristics were reported, the participants from Canada were not reported separately, or the population was not in Canada.

PRISMA flow diagram.
Characteristics of included studies
The publication years of the 259 studies ranged from 2010 to 2023 (see Appendix III for study data and Appendix IV for selection bias assessment). All studies were published in English and included people with MS; five studies also included people with CIS. Twenty-seven (10.4%) studies were national in scope. At the provincial/territorial level, one-third of studies were conducted in British Columbia (BC), and over one-quarter were conducted in Ontario; < 5% were conducted in each of Newfoundland, New Brunswick, Prince Edward Island and the territories (Figure 2). Seventy-one percent (n = 184) of studies involved only one region.

Geographic distribution of studies by province*. *Excludes national studies (n = 27).
The most common topics investigated were disease-modifying therapy (n = 64, 24.3%), followed by access to care or health care use (n = 54, 20.7%), and quality of life (n = 49, 19.0%). The least common topics were the MS prodrome, employment or work ability (both n = 4, 1.5%), and chronic cerebrospinal venous insufficiency (n = 2, 0.8%) (Figure 3).

Study topics, organized by percentage. CCSVI: chronic cerebrospinal fluid insufficiency.
Slightly over half of the study designs were longitudinal, including cohort studies (n = 134, 51.7%), non-randomized experimental studies (n = 5, 1.9%) and randomized controlled trials (n = 8, 3.1%). One-third of studies were cross-sectional (n = 79, 30.5%). The remaining designs used included qualitative or mixed methods approaches (n = 21, 8.0%), case-control (n = 5, 1.9%), case series or case reports (n = 5, 1.9%) and systematic review (n = 1, 0.4%). Eighty-eight percent of cohort studies relied on secondary data sources, as did one-third of cross-sectional studies.
Sixty percent (n = 157) of studies used secondary data analysis; the remainder used primary data collection except for one that used both. Of the studies that used secondary data analysis, 92 (58.2%) used administrative (health claims) data. Local clinical databases were used in 24.1% of studies, government-supported registries and databases (e.g. cancer registry) in 7.6%, and Statistics Canada data, including census data and national surveys were used in 33.6%. Census data were often used with administrative data to derive area-level socioeconomic status. The remaining studies used a mixture of re-analysis of study-specific datasets, medical records review and the Canadian Longitudinal Study on Aging platform. 33
Primary data collection studies (n = 102, including the one that also used secondary data) most often relied on MS Clinics for recruitment (n = 56, 54.9%), followed by MS Canada (n = 26, 25.5%), other clinical sites (n = 4, 3.9%), other advocacy organizations (3, 2.9%) and other sources (4, 3.9%); 9 (7.8%) studies did not report recruitment sources. Eighty-eight (86.3%) studies relied on one recruitment source, and this did not differ between qualitative and quantitative studies (p = 0.83). When we stratified the studies into qualitative and quantitative, excluding case reports/series and systematic reviews, we found that qualitative studies were less likely to recruit from MS Clinics (n = 5, 9.1%) than quantitative studies (n = 50, 90.9%, p = 0.008) but more likely to rely on MS Canada (56.0% vs. 44.0%, p = 0.0005).
Various recruitment strategies were employed, most often clinician referral (n = 35, 34.3%), followed by digital advertisements (n = 14, 13.7%), accessing an existing registry (n = 14, 13.7%), posters (n = 12, 11.8%), telephone (n = 12, 11.8%), traditional news media including newspaper and radio (n = 8, 7.8%), and mail (n = 10, 9.8%). Twenty-seven (26.5%) studies did not specify a strategy. Forty-one (40.2%) studies relied on one strategy, and only 10 (9.8%) used three or more strategies.
The most common inclusion criteria were confirmed diagnosis of MS or validated case definition if using secondary data (194, 74.9%), followed by age (n = 144, 55.6%), and ability (in terms of disability (32, 12.4%) or cognitive function (n = 7, 2.7%). Other selection criteria included language (n = 29, 11.2%), ability to consent (n = 18, 6.9%), comorbidity (n = 15, 5.8%), ethnicity (n = 5, 1.9%), employment status (n = 3, 1.2%), setting (n = 2, 0.8%), education (n = 2, 0.8%) and immigrant status (n = 2, 0.8%). Several other inclusion criteria were used other than diversity characteristics, such as ability to undergo MRI, presence of specific symptoms, and clinical course.
Characteristics of study populations
The median (IQR) number of participants with MS was 408 (59-2656). Studies involving primary data collection had a lower median sample size of 58 (23–188) than those involving secondary data collection (1748.5; 403–5445). The most frequently reported diversity characteristics were age (n = 240, 92.7%), sex (n = 225, 86.9%) and disability status (n = 85, 32.8%) (Figure 4). Eleven percent of studies reported race or ethnicity, and 8.9% reported gender. Religion, sexual orientation and language(s) used by participants were not reported in any study. Additional findings regarding reported characteristics are summarized using the order from PROGRESS-Plus.

Percentage of studies reporting diversity characteristics.
Place of residence
Of the 25 studies that reported place of residence, 24 captured this as urban or rural34–45,46–55; 1 reported a suburban category56 while another stratified urban settings by population size.57 Using random-effects meta-analysis, 65% (53–77%; I2 = 99.9%) of participants lived in urban settings (Figure 5). All 24 studies involving secondary data analysis (23 used administrative data) defined urban/rural status by postal code.

Proportion of study participants residing in urban settings*. *Total indicates sample size. Marrie 2014 with n = 5035.42 Marrie 2014 with n = 5797.46
Race and ethnicity
Twenty-eight studies reported race or ethnicity or both,7,44,58–83 including one that reported characteristics of individuals with clinically isolated syndrome. Reporting categories varied across studies, but many studies reported only the percentage of White participants. The percentage (95%CI) of participants with MS identifying as White was 83.4% (72.4–92.1%, I2 = 99.3%) (Figure 6). Among the 4 studies that reported including Black participants, the percentage was 2.5% (0.7–5.2%, I2 = 54.7%) (Figure 7). Among the 3 studies that reported Asian participants, the percentage was 3.9% (3.3–4.6%, I2 = 0.01) (Figure 8). The percentage of participants classified as ‘Other’ race was 44.9% (7.0–86.8%, I2 = 99.9%) (Figure e1).

Proportion of study participants identifying as White*. *Total indicates sample size.
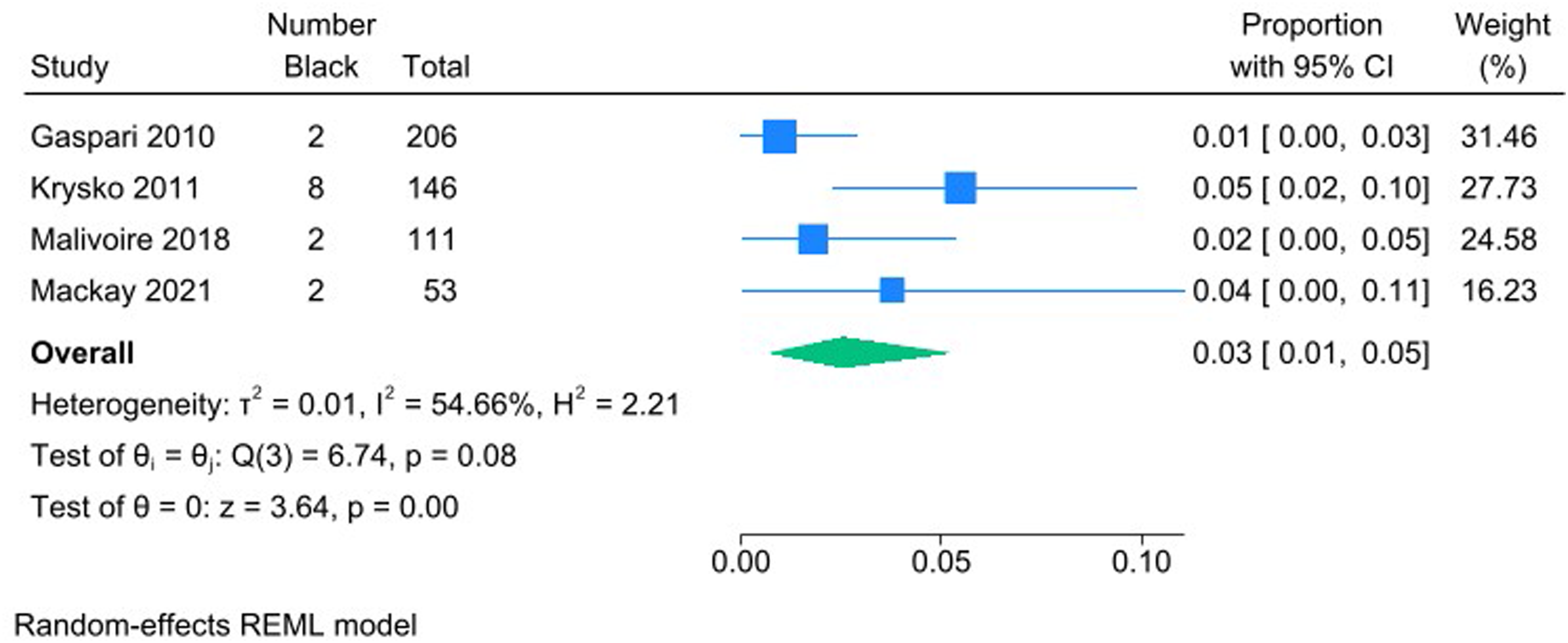
Proportion of study participants identifying as Black*. *Total indicates sample size.

Proportion of study participants identifying as Asian*. *Total indicates sample size.
Occupation/out of work
Twenty-four studies reported employment status,57,61,69–71,78,79,84–99 although the categories used varied widely, limiting the ability to summarize findings. For example, some studies simply reported if participants were working or not working, whereas others captured whether employment was full-time or part-time, as well as whether individuals were disabled from work, retired, looking for work, students or homemakers.
Gender and sex
Overall, 248 studies reported sex or gender.2,3,7,8,34–81,83–276 Although some studies reported they captured gender, all reporting of gender was binary (men/women) or used language that evoked sex (male/female). The proportion of females was 72.8% (70.8–74.8%, I2 99.8%) and of women was 71.3% (66.2–76.1%, I2 99.81%).
Education
Forty-seven studies reported educational status,57,61,63,67–69,71,76–79,81,85–91,95,96,99,101,103,105,116,135,158,165,168,172,178,179,185,199,202,208,223,231,247,251,259,265,271,272,277 either as years of education or level of education attained. The mean (95%CI) years of education obtained were 14.3 (13.1–15.6%, I2 = 0%). The percentage of participants with any post-secondary education was 54.5% (45.7–63.2%, I2 = 98.4%) (Figure e2).
Socioeconomic status
Seventy-three studies reported SES,3,6,34–39,41–43,45–49,51–55,57,76,77,79,89,96,106,111–113,120,125,136,157,167,169,171–173,178,180–182,186–188,193,195,206,209,210,223,232,233,237,239,242,243,246,247,250–252,260,261,263,266,267,269,277 in most studies this was an area-based measure of SES.
Age
Among the 240 studies that reported age,2,3,7,8,34–53,55,56,58–75,77–81,83–97,99–114,116–139,141–146,148–150,152–168,170–176,178–188,190–197,199–214,216,217,219–229,231–238,240–243,245,247–257,259–263,266–276,278–286 it was reported in multiple ways including as a mean, median or categorical variable; the categories used varied substantially. The mean (95%CI) age (n = 150 studies) was 43.4 (39.7–47.0, I2 89.7%).
Disability
Eighty-five studies reported disability status,35,36,40,59,62,63,69,71,72,75,79–81,85,87,92–95,99,101,104–107,114–116,118,119,121,130,131,135,137–139,141,142,147,153,155,156,158,163,165,166,168–170,179,183,185,191,192,195,197,198,200–204,207,212,219,220,224,229,230,233,234,241,243,246,249,250,253,262,264,268,269,278,287 75 using the Expanded Disability Status Scale (EDSS) score. Patient-determined disease steps, a self-report measure of disability, as well as activities of daily living, and use of home care or long-term care services were also used as measures. The mean (95%CI) EDSS for studies reporting the mean was 2.54 (1.81–3.27) (Figure e3). Among the 13 studies for which we could derive the percentage of participants with severe disability, the proportion affected was 40.0% (25.3–55.8%, I2 = 99.8%) (Figure e4).
Immigrant status
Five (1.9%) studies, all using secondary data analysis of existing datasets, reported whether participants were immigrants at the individual level. 4 ,70,82,113,245 A sixth study reported immigrant status at the neighborhood level only.55 Among the five studies reporting at the individual level, 17% (4–35%, I2 = 99.9%) of participants were immigrants (Figure e5); these studies included immigrants as a particular population of interest.
Risk of selection bias
Eighty percent of qualitative studies had a low risk of bias versus only 41.4% of quantitative studies (p = 0.0002) (Appendix IV). Among the quantitative studies, the risk of bias differed by study design (p < 0.0001). Clinical trials had the highest percentage rated as having low risk (75%), followed by cohort (59.0%), case-control (20.0%) and cross-sectional studies (12.7%). A higher proportion of studies involving secondary data analysis had a low risk of bias (58.5%) than those involving primary data collection (24.2%, p < 0.0001). Among quantitative studies, most (97.7%) studies using administrative (health claims) data, or national surveys with random stratified sampling schemes were rated as having a low risk of selection bias unless the sample was restricted by linkage to a clinical data source. Studies relying on clinical databases or medical records review all had moderate or high risks of selection bias.
Discussion
In this scoping review, we assessed what is known about the diversity characteristics of the MS population in Canada. Over ten years, 259 studies reported a limited range of diversity characteristics, most often age and sex. Most participants were White, females or women, resided in urban centers and had post-secondary education. Half of the studies were conducted in BC, where 13% of Canada's population resides, or Ontario, where 40% of Canada's population resides; only three included the northern territories. All gender reporting was binary suggesting a mis-understanding about differences between biological sex and the social construct of gender and the relevance.288 Relatively few studies included or focused on older adults with MS, or those in home care or long-term care settings, although individuals aged 55 to 65 years have the highest peak prevalence of MS in North America, 8 ,289 and have complex care needs. A low proportion of individuals with severe disability participated in primary data collection studies. Religion, sexual orientation and language were not reported. These findings highlight key gaps relevant to health care and policy.
Most studies used one recruitment source, usually an MS clinic or MS Canada. Using an MS clinic offers the advantage of ensuring that diagnoses of MS are confirmed, convenience, and lower recruitment costs. Similarly, the MS Canada research portal offers a low cost means of recruitment. However, individuals recruited through these sources are unlikely to represent the whole MS population as exemplified by differences in age and treatment by people with MS who did and did not use MS Clinics in BC.290
Studies using secondary data sources such as administrative data, or national surveys were uniformly rated as having a low selection bias, but were limited to reporting age, sex and area-level socioeconomic status. This reflects deficits in those data sources,291 hampering the study of diversity and epidemiology across Canada, regardless of disease. These deficits reflect discrimination in the structures and systems that created them.292 Individual provinces have begun to capture information regarding race and ethnicity,293 however, these efforts have not been harmonized. Qualitative studies were assessed as having samples appropriate to their purpose, but their goals and small samples mean that they are unsuitable for determining the characteristics of the general MS population.
Unfortunately, the limited reporting of diversity characteristics also occurred in primary data collection studies, where the investigators controlled the information captured. The inadequacy of description of participants has been described previously, including in a scoping review of rehabilitation trials in MS. 10 In that review, 97.9% of trials reported age, and 93.0% reported biological sex, but <10% of trials reported race, ethnicity, income, or type of community, suggesting that inadequate description of participants extends beyond the Canadian MS research community. Other systematic reviews suggest that this problem affects the health field broadly.294 Recently, the International Advisory Committee on Clinical Trials in MS recommended that all clinical trials report participant characteristics relevant to health equity, minimally gender, race and ethnicity, education, income and place of residence. 12
Although the limited reporting of diversity characteristics prevents us from truly describing the MS population in Canada, it offers hypotheses about who is being missed in research. In the United States, which has a similar MS prevalence to Canada, the prevalence of MS in Black populations is nearly as high as in White populations.295 Since 4.3% of the Canadian population identifies as Black, our findings suggest they are underrepresented in MS research, consistent with observations in the global literature.9,17 Conversely, the percentage of participants with post-secondary education was consistent with the 57.5% of the Canadian population with post-secondary education.296 Nearly three-quarters of Canadians live in large urban centers with populations >100,000,297 thus people with MS in rural areas may have been slightly over-represented in some studies. Given their difficulties with access to health services, this is valuable.
This review has limitations. We limited the search to English and French, Canada's two official languages; so, we do not expect that this significantly affected the findings. We merged publications derived from the same study, but may have missed some, thus double-counting. Multiple studies used the same secondary data sources and were not truly independent; 92 studies used administrative data from 5 provinces, and 9 other studies collectively used 3 data sources (Canadian Community Health Survey, Survey on Living with Neurological Conditions in Canada, Resident Assessment Instrument datasets). The varied approaches to reporting diversity characteristics limited the ability to summarize them. Given the evolution in diagnosis of MS and understanding of social constructs such as race and gender, we focused on articles published between 2010 and 2024.
Although an understanding of population characteristics, including those contributing to inequitable health care is important, our findings indicate that this lacking for people living with MS in Canada, and existing research has not been sufficiently inclusive. Reliance on limited recruitment sources during primary data collection, and secondary data sources that have limited information contribute to these issues. Moving forward, adoption of recommendations to report diversity characteristics is needed, along with specific efforts to recruit more diverse samples. Funders and journal editors can play a role in supporting these efforts.
Supplemental Material
sj-docx-1-mso-10.1177_20552173251321814 - Supplemental material for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review
Supplemental material, sj-docx-1-mso-10.1177_20552173251321814 for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review by Ruth Ann Marrie, Afolasade Fakolade, Janice Linton, Colleen J. Maxwell, Dalia Rotstein, Brayden Schindell, Helen Tremlett, Ann Yeh and Marcia Finlayson in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-rtf-2-mso-10.1177_20552173251321814 - Supplemental material for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review
Supplemental material, sj-rtf-2-mso-10.1177_20552173251321814 for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review by Ruth Ann Marrie, Afolasade Fakolade, Janice Linton, Colleen J. Maxwell, Dalia Rotstein, Brayden Schindell, Helen Tremlett, Ann Yeh and Marcia Finlayson in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-rtf-3-mso-10.1177_20552173251321814 - Supplemental material for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review
Supplemental material, sj-rtf-3-mso-10.1177_20552173251321814 for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review by Ruth Ann Marrie, Afolasade Fakolade, Janice Linton, Colleen J. Maxwell, Dalia Rotstein, Brayden Schindell, Helen Tremlett, Ann Yeh and Marcia Finlayson in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-4-mso-10.1177_20552173251321814 - Supplemental material for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review
Supplemental material, sj-docx-4-mso-10.1177_20552173251321814 for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review by Ruth Ann Marrie, Afolasade Fakolade, Janice Linton, Colleen J. Maxwell, Dalia Rotstein, Brayden Schindell, Helen Tremlett, Ann Yeh and Marcia Finlayson in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-5-mso-10.1177_20552173251321814 - Supplemental material for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review
Supplemental material, sj-docx-5-mso-10.1177_20552173251321814 for Characterizing the diversity of the multiple sclerosis population in Canada: A scoping review by Ruth Ann Marrie, Afolasade Fakolade, Janice Linton, Colleen J. Maxwell, Dalia Rotstein, Brayden Schindell, Helen Tremlett, Ann Yeh and Marcia Finlayson in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgments
The authors thank Nicole Askin, MLIS (WRHA Virtual Library) for peer reviewing the submitted search strategies.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.A. Marrie receives research funding from: CIHR, MS Canada, Crohn's and Colitis Canada, National Multiple Sclerosis Society, CMSC, The Arthritis Society, US Department of Defense, UK MS Society, Public Health Agency of Canada, and is a co-investigator on studies receiving funding from Biogen Idec, Roche Canada and the Pfizer Foundation. She is supported by the Multiple Sclerosis Clinical Research Chair (Dalhousie).
A. Fakolade is an investigator on projects funded by MS Canada, Social Sciences and Humanities Research Council, Queen's University, National Research Council of Canada, and Government of Canada's New Frontiers in Research Fund. She has received consulting or teaching honoraria from Novartis.
J. Linton reports no disclosures.
C.J. Maxwell receives research funding from a University of Waterloo Research Chair, CIHR, MS Canada, National Multiple Sclerosis Society, CMSC and the Public Health Agency of Canada.
D. Rotstein receives research funding from MS Canada, the National MS Society, the Consortium of Multiple Sclerosis Centers, the University of Toronto Division of Neurology and Roche Canada. She has received consulting or speaker fees from Alexion, Amgen, Biogen, EMD Serono, Novartis, Roche, Sanofi Aventis and Touch International Medical Education.
B.G. Schindell reports no disclosures.
H. Tremlett has, in the last five years, received research support from the Canada Research Chair Program, the National Multiple Sclerosis Society, the Canadian Institutes of Health Research, MS Canada, the Multiple Sclerosis Scientific Research Foundation and the EDMUS Foundation (‘Fondation EDMUS contre la sclérose en plaques'). Advisor for Canada's Drug Agency (2024-25, payment declined). Scientific Advice Program: Invited as a Clinical Expert for In addition, in the last five years, has had travel expenses or registration fees prepaid or reimbursed to present at CME conferences or attend meetings (as a member of the International Advisory Committee on Clinical Trials in Multiple Sclerosis) from the Consortium of MS Centres (2023), the Canadian Neurological Sciences Federation (2023), National MS Society (2022, 2023, 2024), ECTRIMS/ ACTRIMS (2017–2024), American Academy of Neurology (2019). Speaker honoraria are either declined or donated to an MS charity or to an unrestricted grant for use by HT’s research group.
E.A. Yeh has received research funding from NMSS, CMSC, CIHR, NIH, OIRM, SCN, CBMH Chase an Idea, SickKids Foundation, Rare Diseases Foundation, MS Scientific Foundation, McLaughlin Centre, Leong Center, Peterson Foundation, Garry Hurvitz Centre for Brain and Mental Health, Canada's Drug Agency. Investigator initiated research funding from Biogen. Scientific advisory: Hoffman-LaRoche, Alexion. DSMB: Pipeline Therapeutics. Speaker honoraria: Biogen, JHU, Saudi Epilepsy Society, NYU, MS-ATL; ACRS, PRIME, CNPS. Co-Editor in Chief, MSARD. Governing Council: CANTRAIN. Steering Committee: Rare-Kids CAN.
M. Finlayson has research support from MS Canada and the Women's Giving Circle of University Hospitals Kingston Foundation, and is a co-investigator on studies funded by the Canadian Institutes of Health Research, the Social Sciences and Humanities Research Council, MS Canada, the Patient Centered Outcomes Research Institute, and the International Progressive Multiple Sclerosis Alliance.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Multiple Sclerosis Society of Canada (grant number 1186492).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.