
Abstract
Background
Multiple sclerosis (MS) is a chronic condition that affects the central nervous system. Factors such as insurance coverage and income influence its prognosis.
Objectives
To evaluate whether insurance type and socioeconomic factors, including race and ethnicity, employment status, and transportation difficulties affect disease-modifying treatment (DMT) access and clinical outcomes in MS.
Methods
We performed a retrospective chart analysis of patients with MS treated at Rush University Medical Center. Patients were divided based on primary insurance. Primary outcomes were number of clinical relapses, radiological activity, and Expanded Disability Status Scale score at 18 months. The secondary outcome was time to DMT initiation from the time of diagnosis.
Results
This study included 160 patients: 119 had private insurance and 41 had Medicaid. Patients with Medicaid were more likely to experience delays in DMT initiation, clinical relapses, and disability progression. There was no significant difference in time of DMT initiation in patients with Medicaid versus private insurance after adjusting for baseline covariates. We did not find a significant media effect of DMT delay on any clinical outcomes.
Conclusions
In this study, Medicaid coverage was associated with worse clinical outcomes, including more clinical relapses and higher EDSS progression compared to privately insured patients.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system (CNS) leading to CNS demyelination, neurologic deficits, and disability. 1 The prevalence of MS is 374 per 100,000 adults, with an average onset ranging from ages 20 to 40. MS causes a variety of neurological symptoms in relapsing-remitting and progressive forms, leading to variable prognoses often affected by socioeconomic factors including insurance status and income.2–4
Early initiation of disease-modifying treatment (DMT) reduces relapses, hospitalizations, and the risk of disability. DMT is expensive with an annual cost exceeding $70,000 in the United States, but it is unclear if this high cost is offset by direct and indirect costs of untreated MS by reducing potentially avoidable healthcare utilization, lost earnings, and nonmedical expenses.5–8 Previous research has indicated that various factors, including education level, gender, race, employment status, and access to healthcare, can impact clinical outcomes related to MS and may influence prescribing decisions for the condition. However, there are still significant gaps in our understanding, and many studies that explore the relationship between social factors and MS outcomes have design limitations. 9 The impact of higher DMT costs, socioeconomic limitations, and insurance restrictions on MS outcomes requires further investigation.
DMT options are often limited by insurance policies forcing many patients to try modestly effective therapies first despite evidence that early initiation of highly effective therapy reduces disability. Unfortunately, the more effective therapies are often more expensive. 10 Private insurance plans are variable and difficult to compare, but single site studies suggest that Medicaid-insured patients are more likely to receive a denial for an MS medication compared to privately insured patients. 11 The initiation and adherence to DMT are also influenced by mental health conditions, demographic characteristics, and other socioeconomic factors, all of which contribute to disparities in MS outcomes.12–15
The objective of this study was to evaluate whether insurance type and socioeconomic factors affect DMT access and clinical outcomes in MS. We hypothesized the following: (1) patients with Medicaid are more likely to experience a clinical relapse and worsening Expanded Disability Status Scale (EDSS) over 18 months compared to patients with private insurance and (2) the relationships between insurance coverage and clinical outcomes (clinical relapse, worsening EDSS) are mediated by delay in accessing DMT. As a secondary objective, we examined the relationships between social risk factors, including gender, race, ethnicity, employment status, level of education, transportation difficulties, missed appointments, and clinical outcomes.
Methods
Enrollment
We performed a retrospective chart analysis of patients with MS treated at Rush University Medical Center (RUMC) between 1 January 2017 and 31 December 2022 using RUMC's electronic medical record.
We included adults aged 18 to 55 because most DMT were approved based on studies of patients 55 and younger. As people age, new clinical relapses and magnetic resonance imaging (MRI) changes become less frequent, with patients either stabilizing or experiencing slow, progressive neurological decline. We identified therapy-naïve relapsing-remitting MS patients. Patients lost to follow up before 2 years or unable to initiate DMT due to other medical conditions including pregnancy were excluded. Patients were classified by health insurance coverage (Medicaid vs private insurance). Demographic characteristics, baseline clinical information, and social risk factors were collected as the healthcare team documented them in the electronic medical record. Demographic characteristics included age, gender (male and female), race/ethnicity (Hispanic/Latino, non-Hispanic Black (Black), non-Hispanic White (White)), employment status (employed, unemployed, in school, not in labor force or school), and education level (high school degree or less, some college, college degree, or more). Baseline clinical characteristics included EDSS, the number of comorbid medical conditions such as hypertension, diabetes, asthma, epilepsy, hyperlipidemia, sleep apnea, and obesity (none, 1, 2, or more), and psychiatric comorbid conditions including depression, anxiety, and attention deficit hyperactivity disorder (ADHD). The EDSS is an ordinal clinical rating scale ranging from 0 (normal neurological examination) to 10 (death due to MS) in one or half-point increments. Social risk factors included transportation difficulty and missed appointments. Based on self-reports provided by patients, patients were classified as having transportation difficulties if a lack of transportation prevented them from attending clinical or treatment appointments. Any missed appointment was defined as not attending one or more follow-up appointments scheduled in the MS clinic.
Primary outcomes were number of clinical relapses, radiological activity, and EDSS score at 18 months. Clinical relapse was defined as new neurological symptoms persisting >24 hours preceded by neurological stability for at least 30 days and not attributable to another disease process.16,17 We determined the level of radiological activity by comparing the number of new MRI lesions at 18 months to those seen on the initial MRI. The grading system was as follows: grade 0 indicated no new lesions, grade 1 indicated 1 to 2 new lesions, grade 2 indicated 3 to 5 new lesions and grade 3 indicated more than 5 new lesions. Relapses were dichotomized as none versus ≥1 relapses. Changes on MRI were dichotomized as no new lesion versus ≥1 new lesions. We dichotomized change in EDSS based on clinically significant change. Disability progression was defined as (1) EDSS increase of 1.5 points if the baseline EDSS is 0 or (2) an increase of one point if the baseline is between 1 and 5.5 or (3) an increase of 0.5 points if the baseline is above 5.5.18,19
The secondary outcome was time to DMT initiation from the time of diagnosis. DMT delay was defined as initiation of DMT > 3 months after diagnosis. According to data analysis from three large MS registries, patients in the United States began DMT a median of 3 months after their diagnosis. 20 DMTs were categorized as none, modestly effective therapies (glatiramer acetate, interferon-beta, and teriflunomide), moderately effective therapies (fingolimod, siponimod, and dimethyl fumarate) and highly effective therapies (rituximab, ocrelizumab, and natalizumab).21,22
Statistical analysis
Patients’ characteristics were compared between patients with private insurance and patients with Medicaid. Continuous variables were compared with a two-sample t test or Wilcoxon rank sum test, and categorical variables were compared with a chi-square or Fisher's exact test. Clinical and imaging outcomes including new lesions in MRI, disability progression, and clinical relapses were compared between the two groups with Chi-square test.
We conducted a survival analysis using the Cox model to examine the time from diagnosis to the initiation of DMT in patients with Medicaid compared to those with private insurance. We tested whether DMT delay was a mediator between type of insurance and each clinical outcome following a causal mediation analysis. 23
Each binary logistic regression model included demographic characteristics (age, race/ethnicity), clinical factors (baseline EDSS, any psychiatric comorbid condition) and social risk factors (transportation difficulties, one or more missed appointments). Education was not included in the regression models due to missing data (n = 46). Additionally, employment status was highly correlated with type of insurance due to most individuals with private insurance being employed and therefore, we excluded employment status from the regression models. Model 1 tested the association between type of insurance and clinical outcome, model 2 tested the association between the type of insurance and the mediator DMT delay, and model 3 tested the association between type of insurance and clinical outcome after accounting for DMT delay in the same model. Model predictive accuracy was evaluated using the area under the receiver operating characteristic curve (AUC), and goodness-of-fit was assessed with the Hosmer Lemeshow Test. The predictive accuracy for model 3 compared to model 1 (with and without DMT delay) was compared using the DeLong test. 24
Results
A total of 160 patients were identified, including 119 with private insurance and 41 with Medicaid. There were no uninsured patients. The sample was predominantly female (71%) and White (49%). The Medicaid group had a higher proportion of Hispanic (27%) and Black (44%) patients compared to the private insurance group (Hispanic: 15%, Black: 27%) (p = .012). Medicaid patients were more likely to have a high school degree or less education, transportation difficulty and missed appointments compared to privately insured patients (Table 1).
Characteristics of sample.
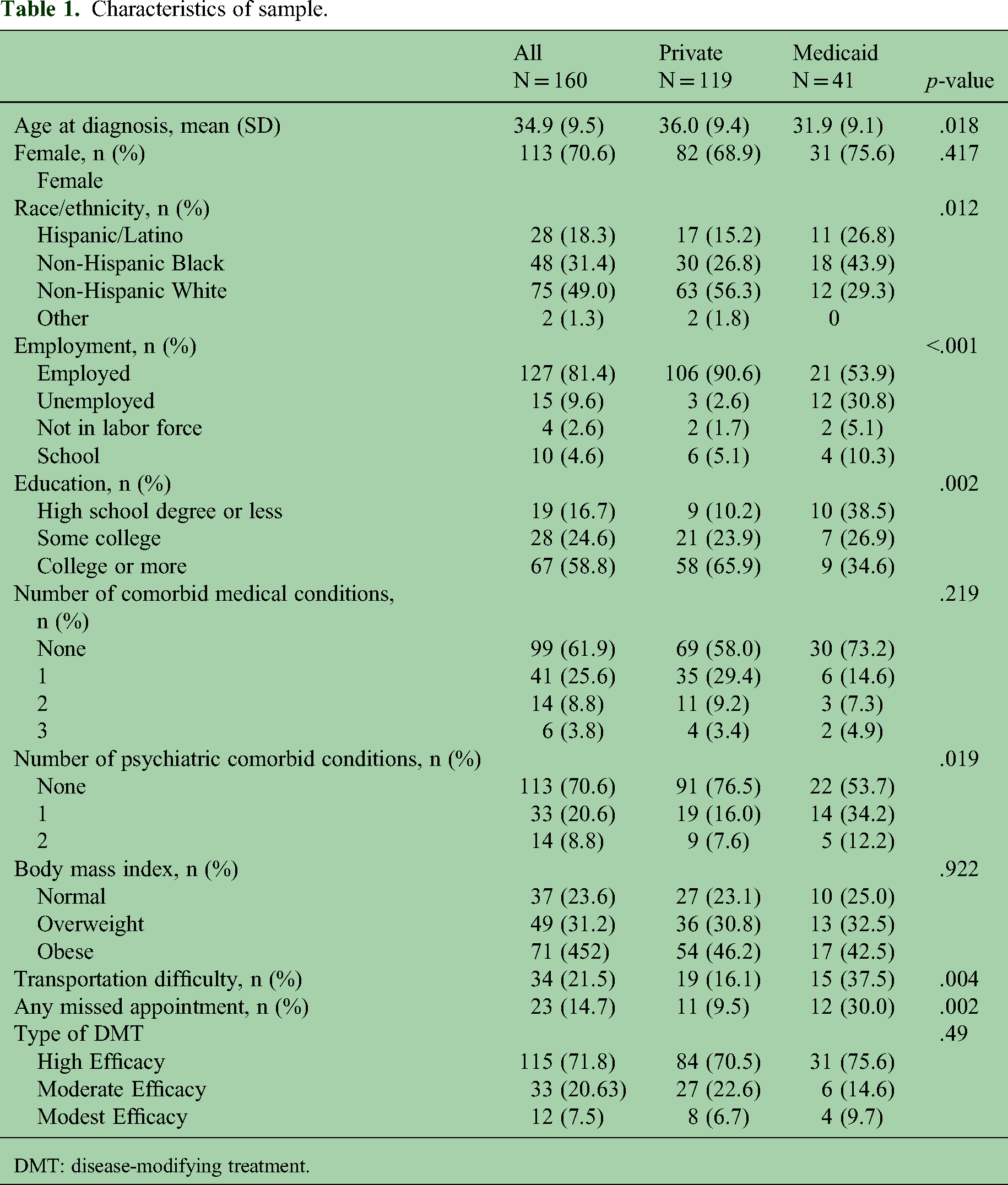
DMT: disease-modifying treatment.
Patients with Medicaid were more likely to have a delay in DMT initiation (p = .010), clinical relapse (p = .001), and disability progression measured by EDSS at 18 months (p = .002) (Table 2). The most common reason for DMT delay was patient preference in the private insurance group and insurance barriers in the Medicaid group. There was no significant difference in effectiveness level of DMT initiated between the two insurance groups (p = .49, Table 1) or imaging outcomes including new lesions at the first (9.8 months) and second average follow up (17.4 months) (Table 2).
Clinical and imaging outcomes.

Disability progress was defined as (1) an increase of 1.5 points in EDSS if the baseline EDSS is 0 OR; (2) an increase of 1 point if the baseline is between 1 and 5.5 OR; and (3) an increase of 0.5 points if the baseline is above 5.5.
Grade 0 indicated no new lesions, grade 1 indicated 1 to 2 new lesions, grade 2 indicated 3 to 5 new lesions, and grade 3 indicated more than 5 new lesions.
DMT: disease modifying treatment; EDSS: Expanded Disability Status Scale; MRI: magnetic resonance imaging.
Medicaid coverage was associated with increased odds of clinical relapse (odds ratio (OR) = 6.06 (confidence interval (CI) 1.35–27.30) and disability progression (OR = 4.56 (CI 1.44–14.45); Table 3). Our survival analysis using the Cox model examined the time from diagnosis to the initiation of DMT in patients with Medicaid compared to those with private insurance. The results did not show a significant difference between the two groups after adjusting for baseline covariates, including age at diagnosis, initial EDSS score, race/ethnicity, and transportation difficulties. The hazard ratio was 1.11 (95% confidence interval: 0.72–1.70, p = .647). We performed causal mediation analysis. We did not find any significant effects (Supplemental table), which could be due to the small sample.
Adjusted odds of clinical relapse, disability progression, and new lesions on the second MRI among Medicaid and privately insured patients with multiple sclerosis.

Covariates adjusted included: age at diagnosis, initial EDSS, at least one missed appointment, race/ethnicity, any psych comorbidities, and transportation difficulty.
CI: confidence interval; EDSS: Expanded Disability Status Scale; MRI: magnetic resonance imaging; OR: odds ration.
Discussion
In this retrospective study, Medicaid coverage was associated with delayed treatment initiation, increased relapses, and increased disability progression compared to patients with private insurance. However, the radiological outcomes between the two groups did not differ significantly. One possible explanation for this finding is that high-efficacy DMT in MS substantially reduces new MRI lesions. In this study, 75% of the Medicaid group received high-efficacy DMT, while 70% of the private insurance group also received these treatments. We hypothesized that the relationship between the type of insurance coverage and clinical outcomes was mediated by delay in accessing DMT, but we did not find evidence of this mediating relationship. Although more than twice as many Medicaid patients (32%) had a delay in DMT initiation compared to privately insured patients (15%), this was not statistically significant after adjusting for demographic characteristics, clinical factors, and social risk factors. This finding indicates access to DMT did not explain observed differences in clinical outcomes among Medicaid and privately insured patients. We speculate there may be other social factors that we could not measure in this study, where Medicaid could be a proxy for social risk. Hence, we require further prospective studies to gather more detailed data about this risk over time.
Although DMT delay was not significant after correcting for confounders, patients who experienced a DMT delay were four times as likely to experience a clinical relapse compared to those who did not experience a delay. One possibility is the variation in preferred MS therapy drugs among private insurance plans. A recent review examining health insurance access in patients with MS found that DMT initiation and adherence decreased as out-of-pocket costs increased. 25 We did not have access to information regarding out-of-pocket cost, prior authorization, or utilization management review requirements by private insurance plan for our sample of patients. Over the past decade, deductibles, copayments, and coinsurance requirements have increased particularly for people who purchase insurance through the Marketplace. To improve outcomes for patients with MS, the underlying drivers of DMT delay including financial considerations need to be pinpointed to remove these barriers through targeted interventions.26,27
Medicaid patients had more psychiatric comorbidities compared to the privately insured in our study. Untreated mental health conditions often can significantly impact medication compliance. Unfortunately, individuals with Medicaid especially in Black and Hispanic populations face even more barriers to receiving adequate psychiatric care.27,28 Implementing strategies that reduce racial and ethnic disparities in mental healthcare could have a positive impact on MS outcomes.
In our study, there was a higher proportion of non-White patients in the Medicaid group compared to the private insurance group. Unfortunately, inequities in healthcare access are still prevalent among marginalized communities in the United States. Previous studies have also shown disparities in outpatient neurological care in the country. 29 Access to DMT, timing of diagnosis, and access to specialty MS clinics could explain the differences in outcomes among racial and ethnic groups. Implementing virtual visits, providing educational materials in multiple languages, offering transportation assistance for necessary in-person appointments, connecting patients with social work or case management services, and linking patients to health psychologists can help reduce barriers to care for marginalized populations.30–32
The Medicaid group also had a longer time to DMT initiation (p < .001) than the privately insured group most commonly due to insurance barriers. Previous research indicates that early DMT initiation reduces long-term costs by slowing disability progression.33–35 Notably, we found that nearly twice as many patients with Medicaid experienced a delay in initiating DMT, however, source of health insurance coverage was not associated with DMT delays after controlling for other patient factors. Additionally, there was no significant difference in the type of DMT received between the Medicaid and private insurance groups (p = .49), indicating that both groups received equally effective treatments.
Our study had several limitations. The outcomes included in our study are only a fraction of potential factors affected by insurance coverage, but we chose clinical relapses and MRI activity as outcomes because they are important in disability progression and overall healthcare spending. Our power to detect changes in health outcomes was limited by the retrospective nature of our study. Although we had originally planned to compare hospitalizations between groups, few patients overall were hospitalized during the study period, and therefore, we did not include it in our analysis. Other limitations include the retrospective study design, potential for residual confounding, potential lack of generalizability of the findings since only a single center was involved, as well as being underpowered for mediation analyses.
Conclusions
In this retrospective study, patients with MS with Medicaid had worse clinical outcomes, including more clinical relapses, and higher EDSS progression compared to privately insured patients. Despite 15% to 32% of individuals experiencing a delay in accessing DMT, this delay was not significantly associated with EDSS progression. However, DMT delay was found to be linked with clinical relapses. Overall, this study highlights the need for further work to characterize and address insurance and socioeconomic barriers to care for people living with MS.
Supplemental Material
sj-docx-1-mso-10.1177_20552173251318034 - Supplemental material for Socioeconomic determinants of clinical outcomes in multiple sclerosis patients
Supplemental material, sj-docx-1-mso-10.1177_20552173251318034 for Socioeconomic determinants of clinical outcomes in multiple sclerosis patients by Fabian Sierra Morales, Bichun Ouyang, Augusto Miravalle, Allison Osen and Tricia Johnson in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chicago chronic condition equity network.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.