
Abstract
Background
Neuromyelitis optica spectrum disorder (NMOSD) primarily affects women of childbearing age.
Objectives
Studying the potential relationship between NMOSD and pregnancy characteristics and outcomes.
Subjects and methods
This is a retrospective cohort study that was conducted on 66 married female patients diagnosed with NMOSD. All patients underwent a thorough review of their demographic and clinical history through their medical records and personal interviews. Additionally, a complete neurological examination was performed, along with the expanded disability status scale (EDSS) and a pregnancy registry questionnaire.
Results
After comparing married patients before and after disease onset, there was a significant increase in the number of abortions and the percentage of cesarean sections, as well as a decrease in the percentage of breastfeeding after disease onset. The p values were .02, <.001, and <.001, respectively, with odds ratios of 2.03, 5.13, and 6.17. Additionally, there was a rise in the occurrence of postpartum relapses, which accounted for 66% of all relapses after the disease onset. Most of these relapses (88.7%) occurred within the first 3 months postpartum.
Conclusion
Presence of NMOSD increased the percentage of miscarriage, delivery by cesarean section, and decreased the chance of breastfeeding. In addition, pregnancy increases NMOSD relapse and subsequent disability.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a severe, recurrent, inflammatory demyelinating disorder of the central nervous system (CNS) that is mediated by autoantibodies against the water channel aquaporin-4 (AQP4). It is primarily characterized by optic neuritis (ON) and longitudinally extensive transverse myelitis (LETM). These autoantibodies can also affect other areas of the CNS, such as the area postrema of the medulla and the hypothalamus. 1
NMOSD is more prevalent in women than men with a ratio of 9:1 in relapsing NMOSD.
The average age of onset for NMOSD is typically between 30 and 40 years, subsequently, many women are diagnosed during their active childbearing years. It is crucial to thoroughly examine all aspects of the disease during the pre-, intra-, and postpartum periods, as well as its impact on fertility and vice versa. 2
It is well-established that pregnancy can have a modulatory effect on autoimmunity. 3 This is also true for NMOSD, as large-scale studies have shown that the relapse rate is significantly higher during the first 3 months after giving birth compared to before or during pregnancy.4,5
Like other autoimmune diseases, NMOSD may also increase the risk of spontaneous abortion and other complications during pregnancy. This could be due to the transfer of AQP4 antibodies through the placenta, which can have a significant impact on the infant's neurological health. 6
In this study, we thoroughly examined the potential interactions between pregnancy and NMOSD and suggested further research on reproductive management strategies for patients with NMOSD. This includes preconception counseling and postpartum supervision.
Materials and methods
Study population
This retrospective cohort study involved 66 married Egyptian female patients who were diagnosed with NMOSD according to the NMOSD international consensus diagnostic criteria (2006, 2015). 1 The patients were recruited from the Kasr Alainy Multiple Sclerosis Unit (KAMSU) between June 2013 and June 2019. Patients with a history of gynecological disorders that could potentially cause miscarriage, such as uterine deformity, tumors, uterine or tubal adhesions, cervical incontinence, polycystic ovary syndrome, metabolic disorders, or those using chronic medications that could affect their menstrual cycles, were excluded. Patients with clinically isolated syndrome (CIS) or other autoimmune disorders that did not meet the diagnostic criteria for NMOSD were also excluded.
Clinical data collection
Informed consent was obtained from all participants, and detailed demographic and clinical data were collected. This included current age, age at onset of disease, family history, comorbidities, duration to diagnosis, total duration of disease, annualized relapse rate, lab and imaging results, anti-aquaporin 4 antibodies status, and treatments received.
This information was gathered from clinical records and personal interviews with patients.
Additionally, a detailed history was obtained from all patients, including symptoms at the onset and during the course of the disease. Physical examinations, including the expanded disability status scale (EDSS), were also conducted.
Our self-constructed NMOSD pregnancy questionnaire was used to collect pregnancy details, such as age at pregnancy, whether it was planned or not, number and timing of relapses during pregnancy, treatments received, complications during pregnancy, method of delivery and any complications, the outcome of the pregnancy, number and timing of post-partum relapses, and method of lactation.
Statistical analysis
This was an exploratory study without adjustment for multiple comparisons.
Chi-square test or Fisher's exact test was used to examine the relationship between qualitative variables.
For normally distributed quantitative data, a comparison between two groups was done using the Student's t-test, for not normally distributed quantitative data, a comparison between two groups was done using the Mann–Whitney test. All tests were two-tailed, and a p-value < .05 was considered statistically significant. The Pearson correlation coefficient was used to test the correlation between different variables. Odds ratios were used to present the strength of the association between risk factors and outcomes.
Results
Our study included 66 patients, with a total of 277 pregnancies. Of these, 211 pregnancies occurred before the onset of the disease, while 66 occurred after (see Figure 1).

Flow chart showing the relation between pregnancies and the onset of NMOSD among our population.
Clinical data of patients with NMOSD
The average age of our population was 36.5 ± 7.2 years, with a median EDSS of 5 at the time of the questionnaire. The mean annualized relapse rate (ARR) was 2.3 ± 1.9. The majority of patients (71.2%) had a monosymptomatic onset, with optic neuritis being the most common initial symptom (52.2%). The most commonly prescribed medications were rituximab (31.8%) and azathioprine (25.4%). A large proportion of patients (83.3%) had a history of long segments myelitis. For additional demographic and clinical data, please refer to Table 1.
Demographic and clinical data of our study population.
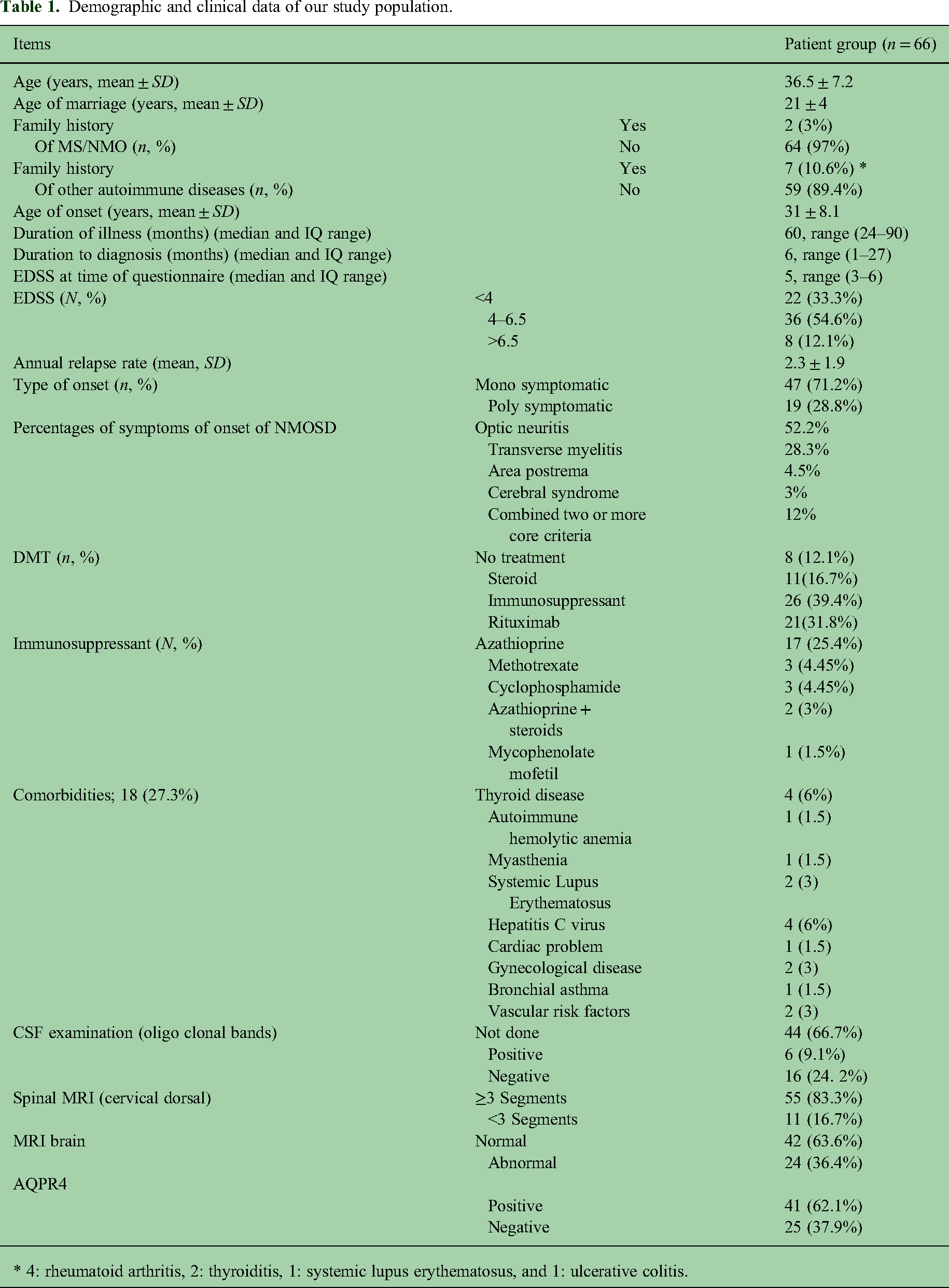
* 4: rheumatoid arthritis, 2: thyroiditis, 1: systemic lupus erythematosus, and 1: ulcerative colitis.
Post-NMOSD pregnancy characteristics
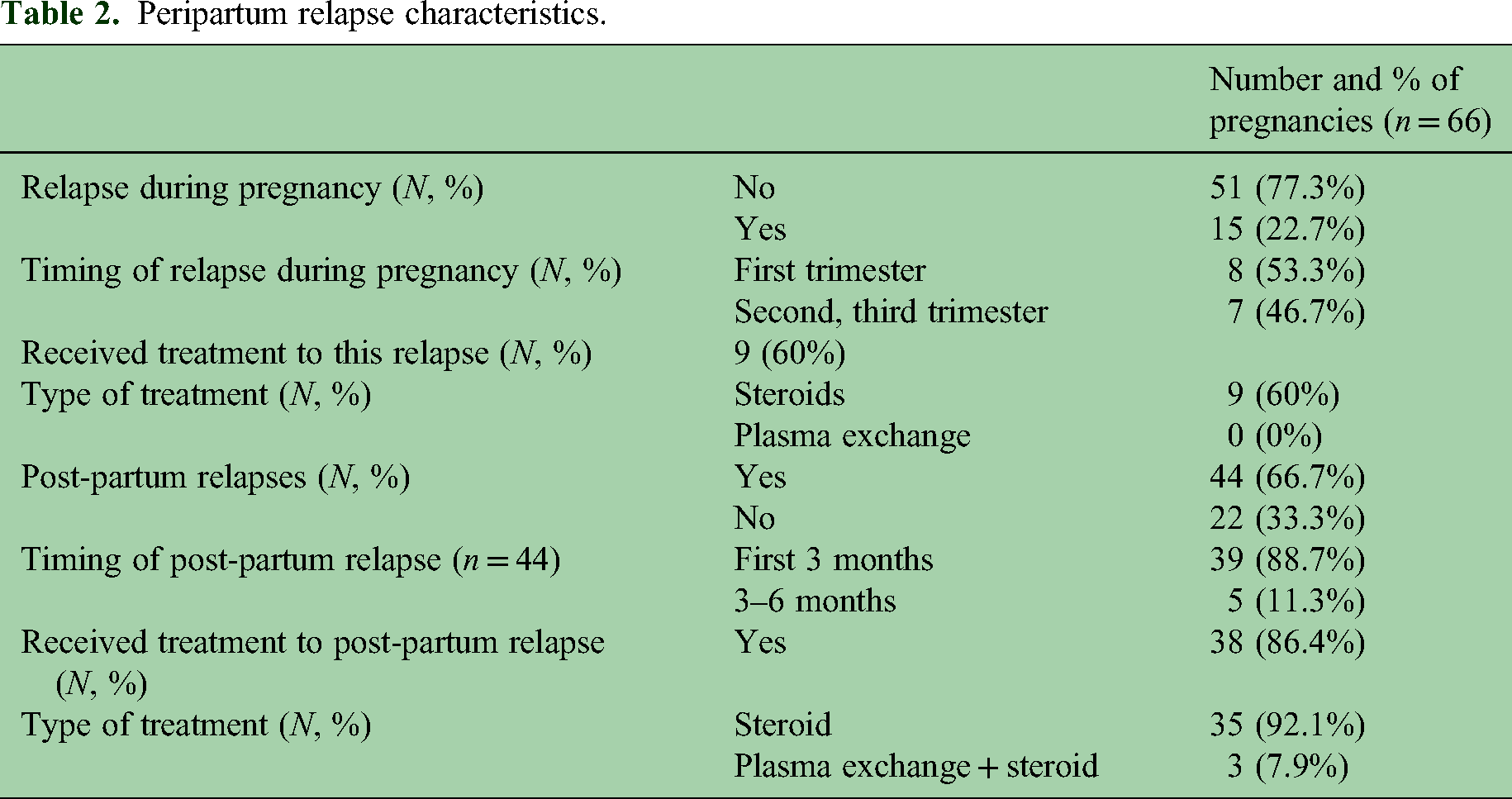
After the onset of NMOSD, there were a total of 66 pregnancies, with a median time of 4 years from onset to pregnancy. The range of time varied from 1 to 13 years, with an interquartile range (IQR) of 3–7 years. Out of these pregnancies, 59 out of 66 (59/66) were complicated by peripartum relapses. Of these, 15 out of 66 (15/66) (22.7%) experienced relapses during pregnancy, with more than half (53.3%) occurring in the first trimester. Among these relapses, six (40%) were not treated. Three participants had transverse myelitis and three had optic neuritis. Although these attacks resolved spontaneously, they resulted in residual disability. The reasons for not receiving treatment were inaccessibility to healthcare providers for four participants and fear of fetal complications for two participants. Additionally, out of the 66 pregnancies, 44 (66.7%) resulted in postpartum relapses, with the majority (88.7%) occurring within the first 3 months after delivery (refer to Figure 2). The decision to stop taking immunotherapy medication was made by all patients to conceive, except two who continued taking rituximab without any complications.

Temporality of attacks in relation to trimesters/post-partum periods.
After giving birth, all patients resumed their use of immunotherapy within an average of 3.09 ± 0.58 months. Therefore, it can be concluded that the majority of postpartum relapses occurred before the patients resumed their immunotherapy treatment. Table 2 presents the characteristics of these peripartum relapses.
Peripartum relapse characteristics.
Comparison between pregnancies before and after NMOSD onset
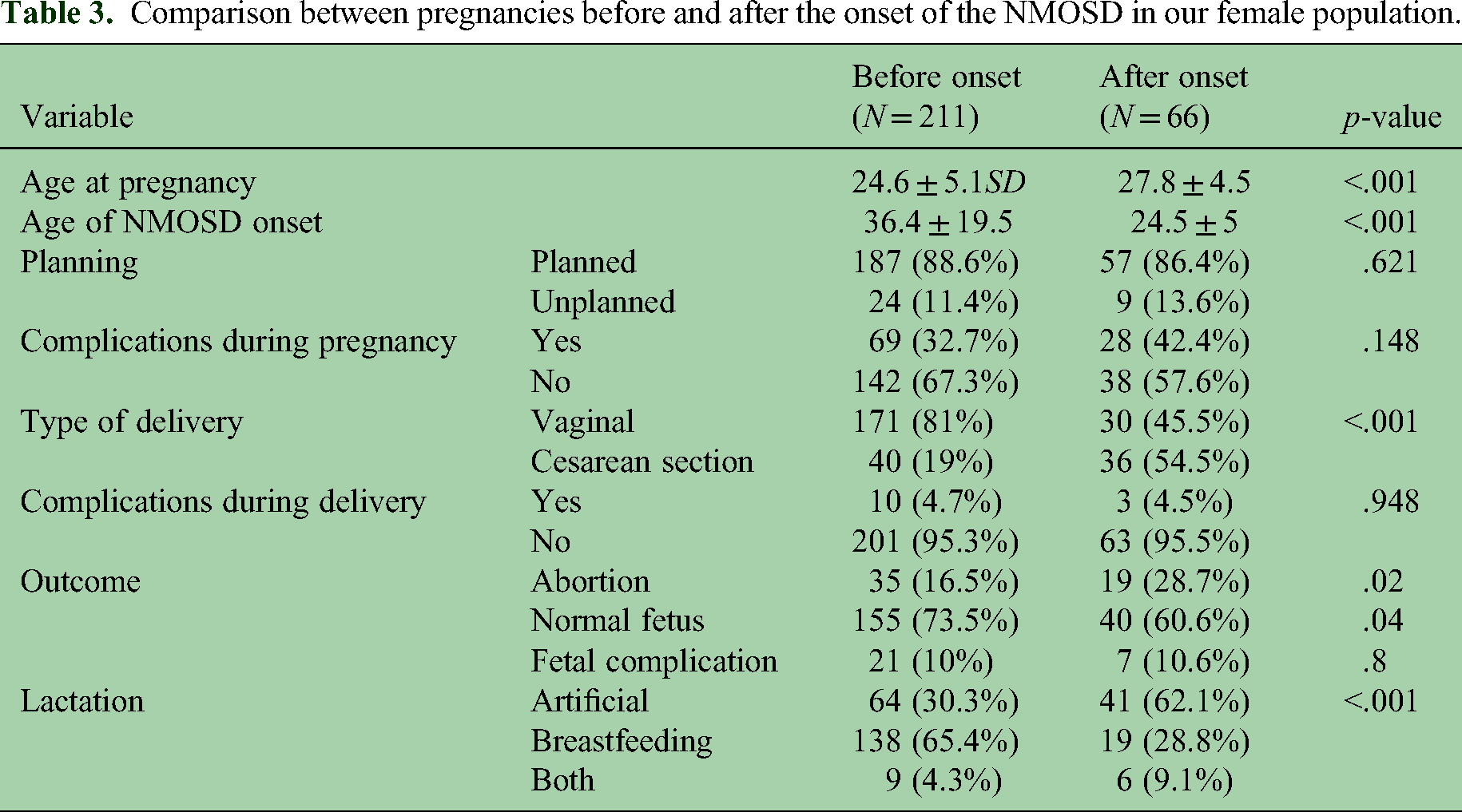
After the onset of NMOSD, most pregnancies were planned, with 86.4% being intentional. However, there was a higher incidence of complications during pregnancy, occurring in 42.4% of cases. These complications included bleeding, premature labor, anemia, hyperemesis gravidarum, preeclampsia, and gestational diabetes. Although this increase in complications was not statistically significant when compared to pregnancies before the onset of NMOSD, it is still worth noting. Only 4.5% of post-NMOSD pregnancies experienced complications during delivery, such as obstructed labor, puerperal sepsis, and bleeding. Out of the 66 post-NMOSD pregnancies, 19 (28.7%) ended in abortion, 7 (10.6%) had fetal complications (such as low birth weight, jaundice requiring NICU admission, and intrauterine fetal death), and 40 (60.6%) resulted in normal, healthy babies. Interestingly, patients who became pregnant after the onset of NMOSD had a higher rate of abortions compared to those who became pregnant before the disease began. Additionally, more than half of the post-NMOSD pregnancies resulted in cesarean section deliveries and the babies were artificially fed, in contrast to those who became pregnant and delivered before the onset of the disease (as shown in Table 3). Most of the cesarean deliveries were performed due to medical indications related to pregnancy and delivery complications, rather than being a patient's personal preference.
Comparison between pregnancies before and after the onset of the NMOSD in our female population.
Comparison between aquaporin-positive and aquaporin-negative patients in terms of pregnancies occurring after the onset of NMOSD
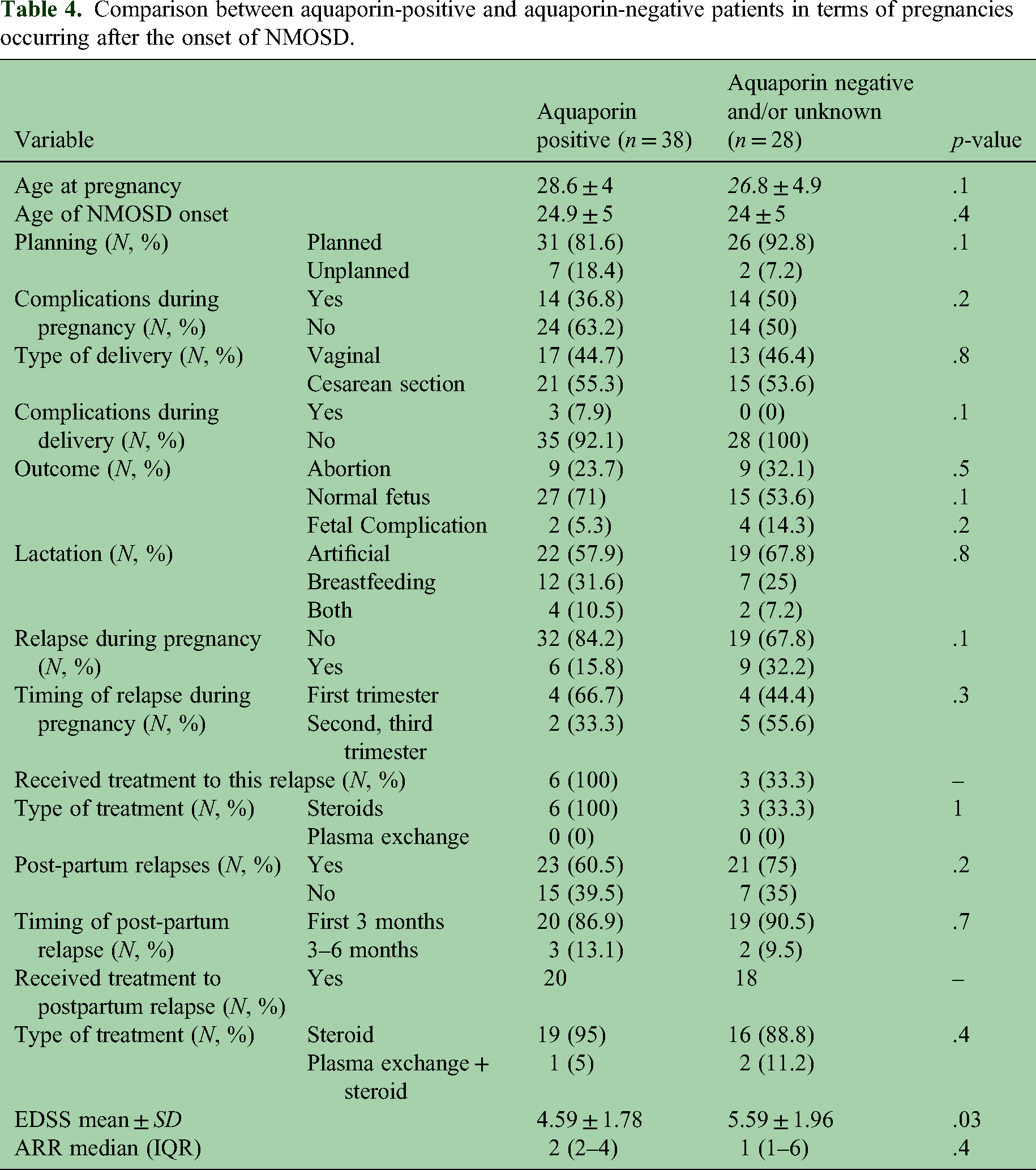
Comparison between patients with positive and negative aquaporin status in terms of pregnancies occurring after the onset of NMOSD revealed that the EDSS was significantly higher in aquaporin-negative patients (5.59 ± 1.96) compared to aquaporin-positive patients (4.59 ± 1.78), with a p-value of .03. However, there were no significant differences between the two groups in terms of pregnancy-related complications, attack rate, or abortions. Please refer to Table 4 for further details.
Comparison between aquaporin-positive and aquaporin-negative patients in terms of pregnancies occurring after the onset of NMOSD.
Comparison between aquaporin-positive and aquaporin-negative patients in terms of pregnancies occurring before the onset of NMOSD
Comparison between patients with positive and negative aquaporin in terms of pregnancies occurring before the onset of NMOSD revealed that complications during delivery were significantly higher in aquaporin-positive patients (38.4%) compared to aquaporin-negative patients (21.9%). Additionally, cesarean deliveries were significantly higher in aquaporin-negative patients (31.5%) compared to aquaporin-positive patients (12.3%) with a p-value of .01 and .0007, respectively. However, there were no significant differences between the two groups in terms of delivery-related complications, lactation, or abortions. Please refer to Table 5 for further details.
Comparison between aquaporin-positive and aquaporin-negative patients in terms of pregnancies occurring before the onset of NMOSD.

Correlations
Significant positive correlations were found between the EDSS and the age of the patients, total duration of disease, and ARR (r = .3, .27 and .311, respectively; p values = .003, .012, and .004). Please refer to Figure 3 for a visual representation. Additionally, the ARR showed significant correlations with the total duration of disease and the number of abortions after disease onset (r = .276 and .247, respectively; p values = .01 and .04).

Correlation between ARR and EDSS at time of the study.
Odds ratios
Odds ratios were calculated for the significant comparative results (Table 6), showing that abortion is two times, cesarean section is five times and artificial feeding is six times more common in pregnancies after disease onset compared to those before disease onset.
Odds ratio for pregnancy parameters that are affected by NMOSD.

Discussion
A significant number of female patients experience the onset of NMOSD during their childbearing years (15–40 years). The presence of NMOSD can have an impact on pregnancy outcomes, while pregnancy itself carries the risk of increased postpartum relapse rates and potential disability. Therefore, it is important for treating neurologists to consider how the disease and its treatment may affect peripartum aspects and make necessary modifications to therapeutic approaches based on this information.
This retrospective cohort study was designed to determine the impact of NMOSD on pregnancy and postpartum outcomes among female patients who underwent treatment at our Kasr Alainy Multiple Sclerosis Unit (KAMSU).
Our research revealed that NMOSD is frequently accompanied by other autoimmune diseases, including organ-specific conditions such as thyroiditis (6%), autoimmune hemolytic anemia, and myasthenia gravis, as well as non-organ-specific conditions like SLE. This is in line with previous studies, which have identified the most commonly associated autoimmune diseases with NMOSD to be autoimmune thyroiditis and primary Sjogren's syndrome (in organ-specific cases) and SLE (in non-organ-specific cases).7–11
At the time of this study, the majority (64%) of patients had an EDSS score of more than four, with a median EDSS of 5 and an interquartile range of 1–3. This, in contrast to previous studies, which reported a median EDSS of 3.5 and a range of 0–10, with the majority (62.2%) having an EDSS score of less than 4.12,13
The difference may be attributed to a delay in disease diagnosis, ranging from 1 to 24 months, and subsequent delayed management, resulting in increased disability. This is also reflected in the higher annualized relapse rate (2 ± 2) compared to the study by Sepúlveda and colleagues, who reported a mean ARR of 0.9 ± 1.5. 13
In our study population, we found a low pregnancy rate after the onset of NMOSD. Out of 277 pregnancies, only 66 (23.8%) occurred after the onset of the disease, while 211 (76.2%) occurred before the onset. This could be due to NMOSD typically presenting at a later age, with a mean onset of 31 ± 8.1 years. Additionally, it is possible that NMOSD patients consciously choose to avoid pregnancy, potentially due to existing disabilities or a desire to prevent them.
In terms of pregnancy outcomes, there was a 2.03 times higher likelihood of miscarriage in patients who became pregnant after the onset of NMOSD, compared to those who became pregnant before the disease onset (OR = 2.03, 95% CI 1.03–3.87). This finding is consistent with previous studies that have shown an increased risk of miscarriage in NMOSD patients, particularly during the first trimester.3,14–16 Animal studies have also demonstrated that AQP4 antibodies can cross the blood–placenta barrier and bind to placental AQP4, resulting in inflammatory changes, placental necrosis, and a higher rate of miscarriage. 6 Furthermore, Chang and colleagues found evidence of AQP4 immunoreactivity, inflammation, and damage in placentas from pregnancies that were terminated in the first and second trimesters, but not in term placentas. 17
The current study did not find a significant difference in fetal complications between pregnancies that occurred before and after the onset of the disease (10% vs. 10.6%). Although AQP4 antibodies have been shown to cross the blood–placental barrier and can be detected in the blood of newborns of NMOSD patients after birth, an elevated AQP4 antibody level in these infants does not typically result in neurological symptoms or other fetal complications. Additionally, their development was normal, and the antibody level returned to normal within 3–6 months after birth.4,18
On the other hand, our study focused on the effect of pregnancy on the course of NMOSD disease. Our findings showed that 66.7% of pregnancies that occurred after the onset of the disease were followed by a postpartum relapse. Additionally, 88% of these relapses occurred within the first 3 months postpartum. These results align with previous studies that have also observed a rise in disease activity during the first 3 months after delivery in NMOSD patients, whether it was the initial onset of the disease or a relapse.15,16,19
The observed fluctuations in disease activity during pregnancy may be attributed to the upregulation of AQP4 during pregnancy and the postpartum period. In addition to being expressed in astrocytes, AQP4 is also present in the placenta and may play a crucial role in maintaining ion homeostasis and water balance throughout pregnancy. The expression of AQP4 in the placenta is highest during the second trimester and gradually decreases toward the end of pregnancy. This could potentially contribute to adverse pregnancy outcomes. 6
One possible explanation for the rise in pregnancy-related attacks in NMOSD could be linked to the discontinuation of steroids and other immunosuppressant drugs during pregnancy. This may be due to patients’ concerns about potential complications for the fetus. 4
Previous studies have shown that patients who continued taking high doses of immunosuppressive drugs, such as prednisolone and azathioprine, were able to remain free of relapses. This suggests that adequate and relatively safe immunosuppression can prevent pregnancy-related attacks. 4 Azathioprine can be transferred through the placenta to the fetus. However, due to the fetus lacking the enzyme necessary for producing active metabolites, the concentrations of these metabolites are typically lower in the fetus compared to the mother. 20
In this study, more than half of the patients (54.5%) chose to have a cesarean section delivery after the onset of the disease, compared to only 19% of pregnancies before the disease onset. This finding is consistent with a study by Klawiter et al., 19 which also reported a high rate of cesarean section (55.9%) after the onset of the disease. There is no evidence to suggest that the method of delivery, epidural administration, or breastfeeding has any impact on the activity of NMOSD disease. 21 In a cross-sectional study, it was found that more than half of the surveyed women believed that cesarean delivery was safer for the mother, while nearly two-thirds believed it was safer for the baby. Additionally, around two-thirds of the participants perceived cesarean delivery to be associated with less pain and bleeding compared to vaginal delivery. 22 However, in our study, most of the cesarean deliveries were performed due to medical indications related to pregnancy and delivery complications, rather than being a patient's personal preference. Recent recommendations from the French Multiple Sclerosis Society state that the indications for cesarean delivery for the general population should also apply to women with NMOSD, regardless of their level of disability (Expert opinion). 23
The choice of breastfeeding after disease onset was also lower (28.8%) compared to (65.4%) before disease onset. This could be explained by the high post-partum relapse rate, also due to difficulty in coping with symptoms such as fatigue, and the need to restart DMDs and symptomatic treatment.
The limitations of the current study include its retrospective design and failure to address the relationship between DMD and pregnancy profiles in women with NMOSD. However, it is the first study to address this issue in Egypt.
In conclusion, research has shown that having NMOSD increases the risk of miscarriage and cesarean delivery and decreases the likelihood of successful breastfeeding. On the other hand, pregnancy has been linked to a higher rate of NMOSD relapse and potential disability.
More prospective studies are needed to examine the impact of changing or stopping immunosuppressant treatment during pregnancy on both the pregnancy and the disease. Additionally, further research is necessary to understand the connection between sex hormones, anti-mullerian hormone (AMH), and fetal aquaporin 4 antibody levels and pregnancy complications and outcomes.
Footnotes
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Medical Ethical Research Committee of Neurology Department, Faculty of Medicine in Cairo University. Informed consent to collect and use anonymized clinical data was obtained from each patient before the study.