
Abstract
Background
Cognitive impairments are well-documented in multiple sclerosis (MS), while speech impairments are often overlooked despite their significant effect on quality of life. For effective clinical management of multisystem conditions such as MS, consideration should be given to the interaction between deficits in multiple domains, such as speech and cognition. To evaluate speech rate measures of spontaneous and read speech, in people with MS and to examine the link between speech and cognition.
Methods
Forty-five people with MS and 25 controls underwent an extensive cognitive battery, including executive functioning, information processing and memory tasks, and completed two speech tasks: a reading task and a picture description task, from which speech rate measures were derived.
Results
The progressive MS cohort had reduced articulation (p < 0.04) and speech rate (p < 0.02) compared to controls and those with relapsing MS. Regression models also revealed information processing speed accounted for 18% to 30% of the variance of spontaneous speech rate measures, and 27% of read speech. Executive functioning accounted for a further 10% of the variance of speech rate in those with MS.
Conclusions
The present study suggests that speech production is contingent on cognitive ability, with information processing speed and executive functioning linked with speech timing patterns.
Introduction
Multiple sclerosis (MS) is a debilitating autoimmune condition of the central nervous system and a most common non-traumatic form of neurological disability in young adults. 1 MS affects diverse functional systems, including sensory, motor, and cognitive impairments. Cognitive impairment is a well-established symptom of MS with deficits observed in between 40% and 65% of people with MS (pwMS) and may present at the earliest stages of the disease. 2
Reduced information processing speed and efficiency are among the most common forms of cognitive dysfunction in MS.2–4 Deficits in executive functioning, often encompassing processes such as planning, organisation, reasoning, and attention are also commonly reported.2,3,5 Indeed, such cognitive domains have been utilised as disability metrics in MS clinical trials, due to the frequency and impact of cognitive dysfunction in this population.6,7
Additionally, speech abnormalities and language impairments are almost as pervasive as cognitive symptoms, with up to 50% of MS patients experiencing some form of speech disorder.8,9 Although speech and communicative ability are tightly linked with interpersonal relationships, work status, and quality of life, 10 impairments in these domains are among the least well-described manifestation of MS. Speech-motor conditions such as dysarthria are characterised by unclear articulation, for example, slurred, monotone or breathy speech, primarily resulting from muscle weakness. Conversely, speech and language production relies on multifaceted cognitive abilities involving message generation, word-finding, sentence structure as well as articulation, 11 and are the focus of this research.
Difficulty with word-finding has been reported as the primary cognitive complaint among pwMS and shown to discriminate pwMS from healthy controls, 12 while slowed articulation rate has repeatedly been linked with a decline in information processing speed.13–15 Swets et al. 16 reported the involvement of working memory in sentence planning, suggesting that sentence planning ability is limited by working memory capacity. Therefore, abnormalities or deficits in cognition may be reflected in the prosody of speech.13–15 While cognitive systems are a well-documented area of concern for pwMS, few studies explore the effect of cognitive impairment on speech and concerning the clinical management of multisystem conditions such as MS, consideration should be given to the interaction of deficits in different domains.
While measures of speech timing, such as speech rate and pause characteristics, have been linked with cognitive processing demands, the speech domain measured, and the method used to elicit speech may impact findings. Spontaneous speech has been reported to be more cognitively demanding than read speech due to the added dimension of planning, recalling content and monitoring.17,18 Many studies in MS, however, employ reading passages such as the Grandfather Passage13,19,20 or utilise speech prompts based on topics familiar to participants (e.g. ‘discuss your last holiday/favourite hobby’13,14). Like reading, familiar topics may require less cognitive engagement in the form of planning, idea generation and long-/short-term recall, due to frequent discussion, or rely on specific cognitive domains such as memory. Therefore, using unfamiliar images to probe extemporaneous speech generation may engage cognitive domains not employed by familiar topics.
A multitude of cognitive assessments, as well as reading and spontaneous speech tasks, were employed to investigate the relationship between cognition and speech in pwMS. It was hypothesised that self-generated spontaneous speech would result in longer, more frequent pauses, faster articulation and slower speech rates when compared to free speech and that these differences would be magnified in pwMS. It was also hypothesized that self-generated speech would require greater cognitive demand, as made apparent by cognitive variables explaining more variance in rate measures of spontaneous speech compared to read speech.
Methods
Participants
Forty-five pwMS were recruited through the outpatient MS clinic. Twenty-one had a diagnosis of relapsing MS (RMS), and 24 had progressive MS (PMS). Inclusion criteria were age 18 to 65 years, a diagnosis of MS as per the 2017 McDonald criteria 21 and MS phenotype based on the Lubin criteria. 22 For those in the RMS group, an expanded disability severity scale (EDSS) score <3.5 was required, or 3.5 to 6.5 for the PMS category. An EDSS score of 6.5 was used as a cut-off due to advanced symptom severity, which precluded people from completing aspects of the study. 23 At time of assessment, the MS cohort had a disease duration of 12.3 ± 10.3 years and 86% were taking disease-modifying treatments (DMTs). None had undergone speech therapy. Twenty-five age- and sex-matched controls were recruited also. Participants were excluded from the study if they had severe visual or cognitive impairment, neurodevelopmental disabilities impeding their capacity to provide informed consent, any evidence of clinically discernible dysarthria or experienced traumatic brain injury, uncontrolled neuropsychiatric, active malignancy or active MS relapse. Controls were also excluded if they had a history of neurological disease. All participants had normal or corrected vision and no participants reported difficulty viewing test stimuli at any stage. This study was approved by the Research Ethics Committee of the St. Vincent’s Healthcare Group, Dublin. Written informed consent was obtained from all participants.
Procedure
Clinical and cognitive assessments were administered over two 1-h sessions, with a 10-min break to reduce fatigue. A clinician retrospectively evaluated EDSS scores based on the most recent clinic letter within 3 months of participation in this study. Participants also completed the Hospital and Anxiety Depression Scale (HADS). All assessments were administered by a clinician or assistant psychologist and overseen by an experienced clinical neuropsychologist.
Cognitive battery
A cognitive battery was administered, assessing general intellectual ability (Wechsler Abbreviated Scale of Intelligence – Second Edition (WASI-II) and Vocabulary and Matrix Reasoning subtests 24 ); executive functioning (Delis-Kaplan Executive Function System (D-KEFS) Colour-Word Interference Test (CWIT) 25 ; named colour-word condition); attention (Wechsler Adult Intelligence Scale-IV (WAIS-IV) Forward Digit Span); information processing speed (Symbol Digit Modalities Test (SDMT)26,27); and verbal and visual learning and memory (California Verbal Learning Test-Second Edition (CVLT-II) 26 ; Brief Visuospatial Memory Test-Revised (BVMT-R) 26 ). Word-retrieval ability was assessed through Letter and Category Fluency tests (D-KFES 28 ). All tests were administered following standardised procedures.
Speech measures
Participants were provided with a typed script of the ‘Grandfather Passage’ 29 on a landscape-orientated A4 sheet of white paper using 20-point Times New Roman, black font. Participants were instructed to read the passage aloud at a comfortable pace. The spontaneous speech task involved describing ‘The Cookie Theft’ image, from the Boston Diagnostic Aphasia Examination 30 presented on a landscape-oriented A4 page. Participants described the image as fully as possible within 15 s. In both cases, the task commenced with the examiner indicating the recording had begun and ended when the participant indicated they had no more to say.
Speech data was recorded using a microphone (GXT 215, Trust International, Netherlands), placed 10 cm from the participant’s mouth. The speech was recorded at 44.1 kHz and quantised at 32 bits using Audacity (Free Software Foundation, Boston, USA). Anonymised recordings were annotated and transcribed using Praat software (Phonetic Sciences, Netherlands 31 ). Speech, pauses, and syllables were automatically extracted using a Praat script. Pause thresholds were set to 100 ms to distinguish pauses from silent plosives. Alignment of pauses and syllables were manually inspected and adjusted based on auditory and visual examination of spectrograms. Recordings were originally annotated by a neuroscientist, and 10% of files were repeated by a speech linguistic expert to assess inter-rater reliability. Both were blind to group status. A high degree of reliability was found between experimenters’ measurements. The average measure intraclass correlation coefficient was 0.973 with a 95% confidence interval from 0.822 to 0.953 (p < 0.001).
Global speech timing measures extracted from the speech recordings included speech and articulation rate, the number and duration of silent pauses, as well as the number of dysfluencies and the speech-task duration. Speech rates were calculated by dividing the total number of syllables by the total duration of the speech sample, including pauses. The articulation rate was derived similarly but excluded pause time. Dysfluencies included instances of non-lexical vocalisation or sound hesitation (e.g. um, eh 32 ), false starts, and repetitions.
Statistical analysis
Data analysis was carried out using SPSS-V27.0 (IBM Corp., IBM SPSS Statistics, Armonk, NY). The distribution of variables was assessed through Kolmogorov-Smirnov tests. Demographic and clinical measures were compared for descriptive purposes and were, therefore, not subject to correction for multiple comparisons.
All the cognitive tests were normalised to z-scores based on the mean and standard deviation of the control group. To reduce the number of variables used to test the hypotheses, composite scores were calculated from mean z-scores for cognitive tests as per Rodgers et al. 13 The intellectual ability composite consisted of the Vocabulary and Matrix reasoning subsets of the WASI-II. The memory composite included CVLT-II and BVMT-R z-scores.
Where appropriate, analyses of covariance (ANCOVA) assessed the interaction between three groups and speech tasks on global speech timing measures. Age, sex, years in education and depression were selected as covariates. For variables which violated the assumptions of an ANCOVA, non-parametric analyses were employed. Kruskal-Wallis tests were used to assess differences between groups and Wilcoxon tests explored differences between speech conditions. The resulting p-values of pairwise comparisons have been adjusted to account for multiple comparisons using Bonferroni corrections.
The second hypothesis that cognitive variables would explain variance in speech measures for pwMS was tested using stepwise regression models. To ensure assumptions of the regression analysis were met, the RMS and PMS groups were combined. Speech and articulation rates for spontaneous speech or read speech were set as dependent variables. Demographic characteristics, (age sex, years in education, and depression) were added as a block, and then each cognitive domain (intellectual ability, information processing speed, memory, attention, executive functioning, and word retrieval) was included using forward stepwise regression where cognitive domains were added in sequential order, with the domain accounting for most variance added first until no further significant domains remained (p > 0.05).
Results
Participant demographics
Demographic, clinical, and cognitive characteristics are shown in Table 1. There was no significant difference between groups in age, gender, handedness, or level of education (p > 0.05). More of the control group were in employment (88%) at the time of recording, compared to pwMS (55%; p = 0.002).
Demographic clinical and neuropsychological characteristics of the study population.

MS: multiple sclerosis; n: number; y: year; M: mean; SD: standard deviation; SE: standard error; IQR: interquartile range; n/a: not applicable; DMT: disease-modifying therapy; EDSS: expanded disability severity scale; WASI-II: Wechsler Abbreviated Scale of Intelligence Second edition; SDMT: symbol digit modalities test; CVlT: California Verbal Learning Test; BVMT-R: Brief Visuospatial Memory Test-Revised; WAIS: Weschler Adult Intelligence Scale; D-KEFS CWIT, Delis-Kaplan Executive Function System Color Word Interference Test; HADS: hospital anxiety and depression scale. Significant p-values are highlighted in bold.
Speech rate measures
Repeated measures ANCOVA were employed to assess articulation rate between the three groups (RMS vs. PMS vs. Control) and across both speech tasks (Read speech vs. Free speech). Controlling for age sex years in education and depression, there was no significant group×speech task interaction effect on articulation rate (F(2,63) = 1.008, p = 0.371, η2 = 0.03). However, there was a significant group effect (F(2,36) = 5.197, p = 0.008, η2 = 0.142). Pairwise comparisons revealed those with PMS have slower articulation rates than those with RMS (p = 0.04), and controls (p = 0.009). Similarly, there was no group × speech task interaction (F(2,63) = 0.259, p = 0.772, η2 = 0.008) for speech rate but the group effect (F(2630 = 4.99, p = 0.01, η2 = 0.137), revealed that speech rate was again reduced in those with PMS compared to RMS (p = 0.024), and the control group (p = 0.017).
Although pause duration remained consistent across tasks, the number of pauses recorded by each group was greater during the reading passage compared to spontaneous speech. Only the PMS group did not exhibit a greater number of dysfluencies during the spontaneous speech task. See Table 2 for a summary of the results.
Results of Wilcoxon signed rank test for between speech tasks.

Significant p-values are highlighted in bold.
Kruskal-Wallis H-test revealed that speech-task duration differed between groups for the spontaneous speech task (H(2) = 8.265, p = 0.016 η2 = 0.09), where those with RMS had significantly longer speech-task durations compared to those with PMS. However, for the reading passage, those with PMS has significantly longer speech-task duration compared to both controls (p < 0.001) and the RMS group (p = 0.045). The number of pauses differed between groups for both spontaneous speech passage (H(2) = 12.455, p = 0.002, η2 = 0.15) and read speech passage (H(2) = 9.740, p = 0.008, η2 = 0.12), such that those with PMS exhibited a significantly greater number of pauses than the control group for both tasks (spontaneous speech task: p = 0.001, read speech passage: p = 0.009). The frequency of dysfluencies and pause duration were comparable between groups for both tasks (p > 0.05). See Figure 1 for a summary.
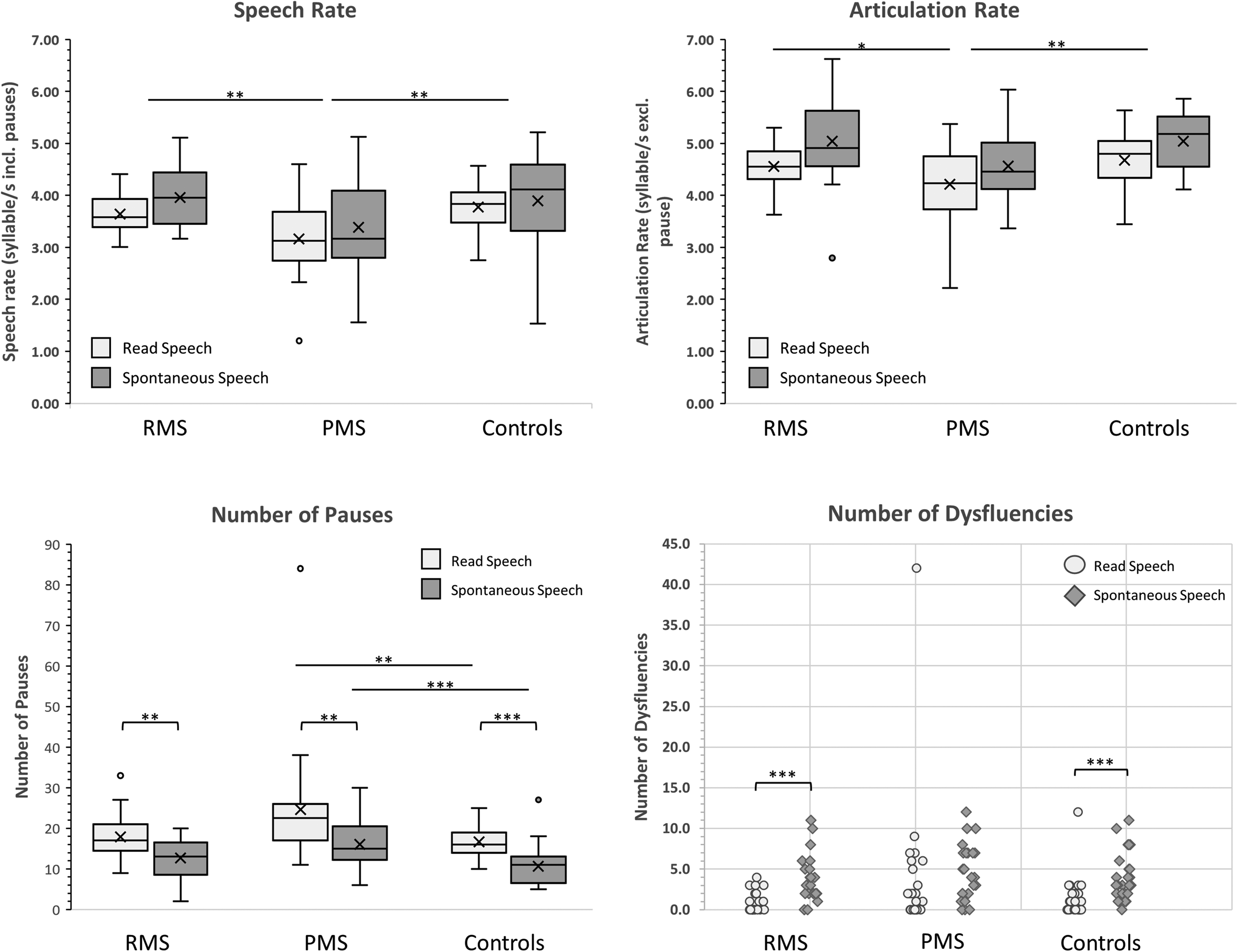
Speech measures by task. Brackets indicate differences between tasks, bars indicate differences between groups. * Denotes significance to the level of p < 0.05, ** signifies p < 0.01, ***indicates significance to the level of p < 0.001.
Regression
The results of the stepwise regression model for the MS cohort are reported in Table 3. Age, gender, and depression were not significant contributors to any model.
Results of stepwise regression analysis for speech rates and cognition.

The order of variables retained was determined by stepwise regression with a significance level set at p < 0.05. Variables were retained in the order which accounted for the most variance. Age sex and depression were entered as block 1.
The stepwise regression model for the self-generated, spontaneous speech task revealed that information processing speed accounted for a substantial proportion of the variance in speech rate (30%). Information processing speed was again retained in the model for articulation rate explaining 18% of the variance observed during spontaneous speech.
For the read speech passage, information processing speed accounted for 30% of the variance of speech rate while executive functioning (CWIT) accounted for a further 10%, bringing the total variance accounted for to 40%. Again, information processing explained 26% of the variance in the articulation rate of pwMS. Intellectual ability composites, attention, executive functioning, and memory composites provided an insignificant contribution to variance.
Discussion
This study aimed to compare speech measures of read and spontaneous speech and to examine the relationship between speech and cognition in those with MS. The hypothesis that all speakers would demonstrate slower speech rates, faster articulation rates and increased duration of pauses during the spontaneous speech was not supported. However, findings do support the hypothesis that differences in speech rates were magnified in pwMS, specifically within the PMS cohort. Regression models for predicting speech rate from cognitive abilities also added further evidence of the interdependence of cognitive functioning and speech-motor performance in MS.
As hypothesised, those with PMS consistently exhibited a greater number of pauses and slower speech rates during both speech tasks compared to the other cohorts. Such differences suggest that additional time is needed for cognitive-linguistic processing such as planning and formulating ideas. 20 Similarly, articulation rates were notably reduced in the PMS cohort which may reflect compensatory mechanisms to maintain speech intelligibility when reading or speaking aloud. 20 This, combined with the increased number of pauses, could also be reflective of greater overall cognitive impairment in those with PMS or offset slowed neural transmission of information. Speech-motor conditions such as dysarthria may also impact timings of speech production. While those with clinically noticeable dysarthria were excluded form participation in this study, some participants may have experienced subtle sub-clinical dysarthric symptoms. More thorough assessments of dysarthria may be necessary in future studies to rule out the potential impact of subtle oral-motor involvement.
Contrary to the hypothesis and previous reports, 20 each group exhibited a greater number and duration of pauses during the reading task than spontaneous speech. This may be due to the pause type. The syntactically complex reading passage contains improbable punctuation resulting in numerous grammatical pauses. However, due to the less formal structure of spontaneous speech, grammatical and ungrammatical pauses were not directly compared in this study.
The regression analysis did not support the hypothesis that self-generated, spontaneous speech requires greater cognitive demand than that of read speech. Information processing was, however, found to contribute significantly (18%–30%) to the variance in speech rate measures for both read and spontaneous speech. This is broadly in line with the results of Rodgers et al. 13 and Benedict et al., 4 who also report a link between information processing and measures of read and spontaneous speech. Similarly, a large-scale study carried out by Friedova et al. 14 linked reduced information processing speed with a slower articulation rate in those with MS. Therefore, our results reaffirm the role of information processing in speech generation.
However, contrary to previous studies, 13 memory composites added a negligible variance beyond that of information processing, during self-generated speech. A possible explanation for this is the use of the Boston Cookie Theft Image as a visual prompt to evoke speech. Perhaps the availability of the image throughout the task minimised demand on memory retrieval, instead concentrating cognitive resources on processing the image. The use of images to elicit speech provides a focus for participants, reducing ambiguity around the topic while also mitigating the use of memory.
Notably, executive functioning contributed significantly to the variance of read speech for pwMS. Combined, executive functioning and information processing explained 40% of the variance observed in read speech. Executive functioning encompasses processes such as attentional control and working memory and inhibition. Attentional control is needed to attend to relevant literacy information and suppresses irrelevant information while flexibly shifting between both, 33 while working memory is involved in storing and processing information 34 and so, executive functioning has long been associated with phonological awareness and literacy. 34 The engagement of information processing and executive functioning and the extent to which these cognitive domains explain variance in read speech, therefore, advocate for the reconsideration of the assumption that spontaneous speech necessitates greater cognitive-linguistic demand than read speech.
Such findings further highlight the importance of assessing information processing speed, executive functions and speech production as part of clinical monitoring in MS and that interventions targeting information processing speed may have a positive impact on speech production. Similarly, speech tasks grant non-intrusive, ecologically valid methods of assessing speech production, while picture description and reading tasks provide consistent stimuli for longitudinal studies, to monitor changes in speech or cognition across disease duration. Due to the ease of administration and richness of the data obtained, speech measures easily translate to clinical settings or familiar environments to monitor disease progression or treatment endpoints.
While this study benefited from the use of well-validated speech and cognitive measures, results must be interpreted with consideration of the constraints in which they were obtained. Although frequently employed, the administration of the Grandfather passage is rarely described in great detail. Font, size, spacing, delivery method, and participant ability may influence readability, 35 yet are rarely described in the literature. Without standardised administration, results must be compared with caution. Similarly, while the use of images to prompt speech has advantages, this method may rely on visual information processing specifically, which this study does examine. Differences in visual information processing may have underpinned or supplemented the effects of information processing speed on individual differences in speech timing due to varying times needed to process the image before planning and articulating the description. Pre-clinical dysarthric articulation may not have been detected during this study nor was there an assessment of respiratory problems which have previously been reported to affect speech in those with MS. 36
Another important issue to note is the potential effect of DMTs. As mentioned 86% of participants have been prescribed DMTs including fingolimod (22%), natalizumab (13%), rituximab (11%), peginterferon beta-1a (4%) dimethyl fumarate (7%), ocrelizumab (9%), glatiramer acetate (9%), cladribine (9%), and interferon beta-1a (2%). DMTs may affect cognition by reducing the progression of brain atrophy and relapse rates.37,38 Emerging research described early treatment with fingolimod as providing a cognitive advantage in those with RMS by allowing adaptive neuroplastic changes and providing anti-inflammation effects 38 while Mattioli et al. 37 reported that natalizumab-aided executive functioning and memory improvements through preservation of parahippocampal and frontal grey matter. However, there remains insufficient evidence of the efficacy of DMTs in the treatment of cognitive impairments in pwMS and no medication has been approved, specifically for these symptoms. 39
Future research should, where possible, consider the potential effects of respiratory issues on speech timing. Furthermore, sentence intelligibility scores may shed light on the influence of dysarthria on speech measures. Future research should also employ a combination of stimuli to elicit self-generated speech (e.g. familiar topics and conversational speech), as these may engage different cognitive processes, and provide a more sensitive delineation of the cognitive measures associated with speech.
Conclusion
The present study found that speech production is contingent on the cognitive ability of the speaker. Although the analysis did not support the hypothesis that read speech is less cognitively demanding than free speech, differences emerged in speech timing patterns of pwMS that are linked with information processing speed and executive functioning. Therefore, the relationship between speech and cognition in MS may provide a foundation for the introduction of speech-based technologies as a method of cognitive assessment and monitoring in pwMS. This study also reaffirms that reading passages and image prompts are easily administered tools to elicit speech and can provide an ecologically valid method of indirectly assessing cognition, whether in a clinical or familiar environment.
Footnotes
Acknowledgements
We would like to acknowledge Hugh Kearney for his assistance in conceptualisation of the research study. We would like to acknowledge Novartis for providing the funding for this study as part of SMY's clinical research fellowship. Novartis did not have any input into the conceptualisation and design of this study, nor the analysis of the results.
Data availability statement
Anonymised data will be shared on request with any suitably qualified investigator.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Novartis.