
Abstract
Background
Natalizumab (NTZ) is a highly effective disease modifying treatment for relapsing multiple sclerosis (RMS), but it increases risk of progressive multifocal leukoencephalopathy (PML) in patients with serum anti- John Cunningham virus (JCV) antibodies.
Objective
To assess the safety and efficacy of rapid transition, from NTZ to teriflunomide (TFM) in RMS patients.
Methods
Clinically stable NTZ-treated, anti-JCV antibody positive RMS patients were switched to TFM 28 ± 7 days after their last dose of NTZ. The primary endpoint was proportion of relapse free patients at 24 months.
Results
Median [IQR] age of the 55 enrolled patients was 47 [40.7, 56.3] years, 76% were female. The median [IQR] number of prior NTZ treatments was 34 [18, 64]. annualized relapse rate (ARR) was 0.07 and 77% of the patients were relapse free at 24 months. Mean time to first GAD + lesion was 19.6 months, and to new/enlarging T2 lesion was 19.2 months. Mean time to 3 month sustained disability worsening (SDW) was 22 months and proportion free of 3-month SDW was 0.87. There were no cases of PML.
Conclusions
The washout-free transition of NTZ to TFM was an efficacious and safe strategy for patients at risk of developing PML.
ClinicalTrials.gov Identifier: NCT01970410
Keywords
Introduction
Multiple Sclerosis (MS), a degenerative disease of the central nervous system (CNS), largely resulting from cell-mediated inflammation that contributes to neurological impairment, has prompted the development of disease modifying therapies (DMTs) that destroy, suppress, sequester, or alter the pro-inflammatory behaviour of cells, including lymphocytes, macrophages, microglia, and astrocytes. While the mechanisms underlying MS pathogenesis remain unclear, evidence suggests that MS results from a complex interaction of genetic, environmental and infectious agents, causing an alteration of adaptive immunity, although there is increasing awareness that alterations of the innate immune system also play an important role in the disease process.1–3 The monoclonal antibody natalizumab (NTZ), a highly effective therapy for relapsing MS (RMS), 4 inhibits migration of pro-inflammatory autoreactive cells into the CNS 5 but also increases risk of developing progressive multifocal leukoencephalopathy (PML) in patients infected by John Cunningham virus (JCV). 6 PML risk in JCV-infected patients is approximately 3/1000 between 2 and 4 years of NTZ use, 6/1000 between 4 and 6 years of use, and 12-13/1000 in patients who also had past treatment with cytotoxic or chemotherapeutic agents. 7 Cases of PML also have been reported in a small number of patients treated with fingolimod (FGM), 8 rituximab (RTX) 9 and dimethyl fumarate (DMF),10–12 as well as in a single patient with prior exposure to NTZ who was subsequently treated with teriflunomide (TMF). 13
Potential PML risk has prompted discontinuation of NTZ in many patients, but there may be heightened risk of recurrent MS disease activity after NTZ withdrawal, including increased relapse frequency, increased activity on MRI,14–20 and increased severity of relapses.14,15,19,20
Increased disease activity was reported in patients switched from NTZ to glatiramer acetate, interferon β-1a or methylprednisolone. 16 A post-hoc, cross-sectional analysis indicated that initiating DMF within 90 days of discontinuing NTZ was associated with lower risk of relapse. 21 In a retrospective chart review study, 61% of patients switching to FGM sustained a relapse after discontinuing NTZ, 48% of whom had a relapse while being treated with FGM. Most of the relapses occurred within 13–24 weeks of NTZ washout 15 In a prospective study of patients switching from NTZ to FGM, 11.5% of patients had a relapse within 6 months. 17 The odds ratio for a relapse was 7.2 for patients with washout of 8–12 weeks compared to those with a washout of ≤4 weeks. In a blinded, placebo-controlled prospective study of FGM, there was a 9–12% relapse risk following a NTZ washout of up to 12 weeks and 16% for a washout of up to 16 weeks. There was also reduced MRI evidence of disease activity in patients in whom FGM had been initiated within 8–12 weeks of stopping NTZ.22,23 Comparable results have been obtained in patients transitioned to RTX 24 and alemtuzumab. 25 In aggregate, these studies suggest that longer duration of post-NTZ washout increases risk of reactivation of MS disease activity.8,9,13
In this prospective, interventional cohort study, we examined TFM as replacement therapy for clinically stable RMS patients being taken off NTZ because of prior JCV exposure. TFM is an approved oral medication for RMS treatment that inhibits de novo pyrimidine synthesis by blocking mitochondrial dihydroorotate dehydrogenase, 26 and was selected because of its safety profile,27,28 including low risk of PML, evidence of rapid onset of activity, 29 and potential anti-viral properties. If TFM treatment could control MS disease activity safely, and without rebound activity, it could serve as a useful therapeutic strategy for patients being withdrawn from NTZ.
Patients and methods
Study design
This was a prospective, interventional cohort study conducted at two comprehensive MS care centres. Initial key eligibility criteria included age of 21–60 years, but a waiver was subsequently granted to include patient ages 19–64 years, inclusive. The patients were also required to have a diagnosis of RMS, be relapse-free for 12 months prior to the screening visit, have a baseline (Expanded Disability Status Scale (EDSS) of 1.0–6.0, have no evidence of significant cognitive limitation or psychiatric disorder, and have stable brain MRIs in the 12 months prior to the screening visit, which was defined as no new or enlarged T2 or gadolinium enhancing (GAD + ) lesions. Patients had to have received at least 12 consecutive months of NTZ treatment over the previous year and have a positive serum anti-JCV IgG titre. After providing informed consent and completing study screening, patients started oral TFM treatment 14 mg a day 28 ± 7 days after their last NTZ infusion.
Physical examination, EDSS, adverse events (AEs), laboratory assessments, and concomitant medication review were performed at screening and baseline, monthly for 6 months, then at 9, 12, and 24 months. A brain MRI was completed at screening, monthly for 6 months, and at 12 and 24 months. Symbol digit modality test (SDMT) and Beck depression inventory-II (BDI-II) were completed at baseline, 6, 12, and 24 months. The baseline through month 12 results have been previously reported. 30
All patients at each site were studied on the same 3 tesla MRI scanner throughout the study. MRI sequences included axial and sagittal T2 FLAIR, axial T1, axial T2, axial diffusion-weighted images, and axial spin-echo T1 following gadobutrol (GAD) 0.1 nmol/kg administration. Axial and sagittal T2 FLAIR 3D images were contiguous non-gapped, 1 mm thick sections. All other images were contiguous non-gapped, 3mm thick. GAD T1 images were obtained after a 10-min post-GAD infusion delay, with 1mm 3DT1 MPRAGE sequences and 3mm axial Spin Echo T1 weighted sequences. Scans were reviewed by neuroradiologists at each centre, each with extensive experience in MS diagnosis.
Study approval was obtained from each site’s institutional review board (IRB), and written informed consent was obtained from all participating patients. All study AEs were reported according to International Conference of Harmonization and local IRB guidelines.
Trial endpoints
This paper is a report of baseline to 24-month TFM treatment outcomes which include the previously reported 30 interim analysis of baseline to 12-month results.
The primary study endpoint was the proportion of relapse-free patients at 24 months of TFM treatment. The proportion of relapse-free patients at 12 months was previously reported. 30
The secondary endpoints were 1) Mean time in months to first appearance of radiological evidence of MS activity with new GAD + T1 lesions and/or new or enlarging T2 lesions on cranial MRI between baseline and 24 months; 2) The proportion of patients free of GAD + T1 lesions on cranial MRI at 24 months; 3) Mean number of new or enlarging T2 lesions per patient between baseline and 24 months, and the proportion of patients free of new or enlarging T2 lesions on brain MRI at 24 months; 4) Mean time to 3-month sustained disability worsening (SDW) between baseline and 24 months.
The exploratory endpoints included median SDMT and BDI-II at 24 months and changes in median SDMT and BDI-II between baseline and 24 months, and proportion of relapse-free patients correlated with age (<50 vs ≥50) and with disease duration (≤15 years vs >15 years) between baseline and 24 months.
Post-hoc analyses included annualized relapse rate (ARR), proportion of patients free of SDW, and no evidence of disease activity (NEDA 3) at month 24, the latter defined as no relapses, no change in EDSS, 31 no new T2/GAD + or enlarging lesions on brain MRI and the risk of relapse for patients who had experienced a relapse during the 12 months prior to starting NTZ.
A relapse was defined as new or worsened neurologic symptoms, unassociated with fever or evidence of infection, lasting at least 24 hours, with an increase in one or more points in two or more EDSS FS scores, or a two or more point increase in one FS score. 31 All patients reporting suspected relapse symptoms were evaluated within 7 days of onset by their study treating neurologist. All relapses were confirmed by the principal investigators (KE, SC). SDW was defined as an increase of ≥ 1 point for patients with EDSS of 1.0–5.0, and ≥ 0.5 points for patients with an EDSS of 5.5–6.0, sustained for 3 months. Patients with ≥ 1 point increase in EDSS in whom a second measure was not obtained 3 months later were not included as SDW.
Statistical Analysis
Analysis was based on an intention-to-treat model and included all enrolled patients who received at least one dose of TFM. Patient characteristics were summarized as percentages, means and standard deviation (SD) or medians and interquartile range [IQR], as appropriate. Kaplan Meier analysis was used to estimate the proportion of relapse-free patients at the end of 24 months, and the proportion of patients with no new or enlarging T2 lesions and no GAD + lesions.
Wilcoxon signed-rank tests were used to analyse changes in EDSS, BDI-II, and SDMT from baseline to 24 months. R Packages survival, survminer, and ggplot2 were used for the survival analysis analyses and Kaplan-Meier plots.
Results
Sixty-two patients were screened; 55 were enrolled and completed baseline procedures. The median [IQR] age was 47.0 [40.7, 56.3] years; 53 (96.4%) were white, 2 (3.6%) were African American, and 42 (76.4%) were female (Table 1). The median [IQR] number of NTZ treatments prior to treatment with TFM was 34 [18.0, 63.5] (Table 1).
Baseline demographic and clinical characteristics.

IQR: interquartile range; ARR: Annualized Relapse Rate; EDSS: Expanded Disability Status Scale; NTZ: natalizumab; SD: standard deviation; SDMT: symbol digit modalities test; BDI-II: Beck depression inventory-II.
Twenty-eight (51%) patients completed 24 months. The proportion (also known as cumulative survival probability) of patients free of relapse at 24 months based on survival analysis was 0.77 (95% CI 0.61, 0.87) (Table 2) (Figure 1).
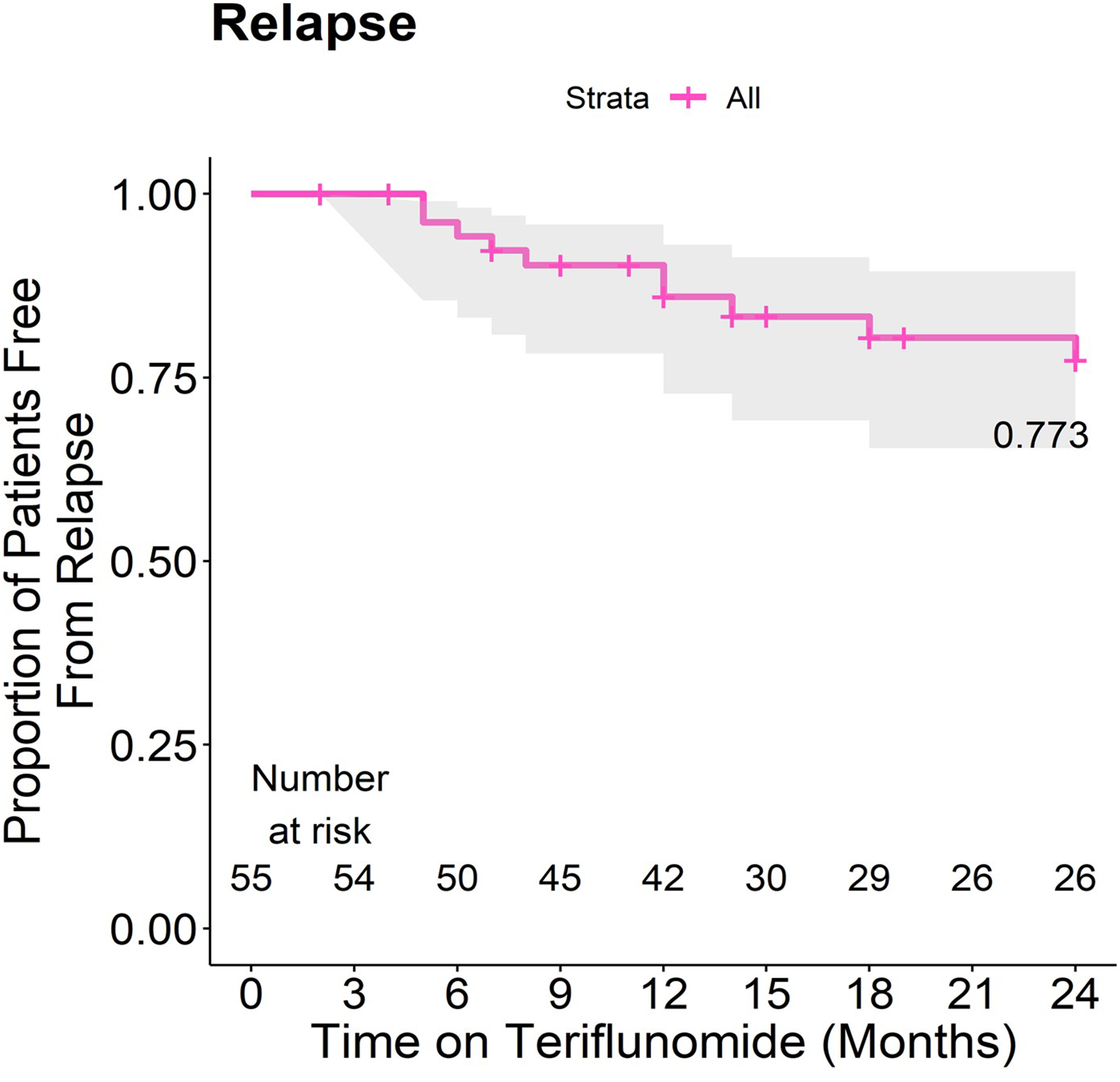
Survival analysis. Results indicate the proportion of patients free of relapse. Solid lines denote Kaplan-Meier estimates and shaded areas denote the 95% confidence intervals.
Study outcomes at month 24.

Proportion estimated from Kaplan-Meier Survival Analysis.
Total number of relapses including all enrolled patients.
Restricted mean with upper limit of 24 months estimated from Kaplan–Meier survival curve.
Wilcoxon signed rank test for difference in medians.
ARR: annualized relapse rate; BDI-II: Beck Depression Inventory-II; GAD + : gadolinium enhancing; SE: standard error; SDMT: Symbol Digit Modalities Test; NS: not (statistically) significant; CI: confidence interval; IQR: interquartile range; SDW: sustained disability worsening; NEDA 3: no evidence of disease activity; RR: Relative Risk.
Of the secondary outcome measures, mean time to 3-month SDW was 22 months (SE 0.7) (Table 2).
The mean time to first GAD + T1 lesion was 19.6 months (SE 1.1) and mean time to new and/or enlarging T2 lesions was 19.2 months (SE 1.1) (Table 2). The proportion of patients free of GAD + T1 lesions at 24 months was 0.62 (95% CI 0.45, 0.75), and the proportion of patients free of new and/or enlarging T2 lesions at 24 months was 0.55 (95% CI 0.8, 0.69) (Table 2) (Figures 2(a) and 2(b)).

a & b. Survival analysis. Results indicate the proportion of patients free from new gadolinium-enhancing lesions and new or enlarging T2 lesions. Solid lines denote Kaplan-Meier estimates and shaded areas denote the 95% confidence intervals.
Of the exploratory outcome measures, the median SDMT at 24 months was 50 [IQR 44, 59.5] and change from baseline to month 24 was −0.64 (-3.7, 2.4) p = 0.9 (Table 2). The median BDI [IQR] at 24 months was 7 [1, 14.5], which is a 2.2 [-2.4, 6.8] (p = 0.34) increase from baseline, but the change was not statistically significant (Table 2). The median [IQR] EDSS at baseline was 2.5 [2.0, 4.0] (Table 1), and the median [IQR] EDSS for those patients completing 24 months was 2.5 [2.0, 4.0] (p = 0.540). There was also an effect of age upon the proportion of relapse free patients, at 0.61 (CI 0.38, 0.78) for those < 50, and 0.96 (CI 0.73, 0.99) (p < 0.014) for those ≥50 years of age (Table 2).
Of the post hoc analyses, the annualised relapse rate (SD) was 0.07 (0.31), the proportion of patients free of 3-month SDW was 0.87 (95% CI 0.74, 0.94), the proportion of patients with NEDA 3 at 24 months was 0.39 (95% CI 0.29, 0.54). Although the relative risk of relapse for patients who relapsed 12 months prior to starting NTZ compared to those who did not was 3.75 (95% CI 0.53, 26.6), this difference was not statistically significant (Table 2).
Twenty-seven patients discontinued TFM before 24 months, 4 of whom had a relapse, 5 experienced new MRI activity, and 4 experienced both clinical worsening and evidence of disease activity on MRI. In addition, 5 patients discontinued TFM due to AEs, 2 were discontinued by the investigators due to non-compliance, 1 was lost to follow up and 6 patients discontinued TFM as a personal choice but provided no explanation (Table 3). None of the relapses that resulted in TFM discontinuation necessitated hospitalization, and none in which their neurological status was worse than before starting or during NTZ treatment.
Reasons for discontinuing TFM.

From baseline through month 24 of TFM treatment, fifty-one patients (93%) reported AEs (Table 4). The most reported AEs were hair thinning/loss (36.4%), diarrhea/loose stool (34.5%), headache (23.6%), and nausea/vomiting (21.8%) (Table 4). More than 95% of the AEs were mild to moderate in severity, and most AEs occurred in the first 12 months following the initiation of TMF treatment. No additional SAEs occurred after those previously reported in the 12-month interim analysis. 30 There were no cases of PML, other opportunistic infections, or deaths.
Adverse events.

Percentages are based on total # of enrolled patients (N = 55). All AEs (N = 386) reported for those who experienced AEs during the study period (N = 51). Relapse and progression of MS were not reported as AEs, as these were categorized separately for reporting in table 2.
One patient discontinued due to severe empyema, severe pleural effusion, and mild-moderate lymphopenia.
One patient discontinued due to mild diarrhea.
One patient discontinued due to severe diarrhea.
One patient discontinued due to mild loose stool.
One patient discontinued due to mild-moderate leukopenia, abscessed tooth and dental infection.
AEs collected between July 2013 and August 2017 are included and have been previously reported. 1 .
Discussion
Because of the risk of developing PML, a disorder associated with a high mortality rate and significant disability in patients who survive, 6 in NTZ treated patients who have been exposed to JCV, strategies are needed for transitioning such patients to other therapeutic agents that can maintain neurological stability with minimal risk of serious AEs. There has been understandable concern for potential risks of rapidly substituting another DMT while NTZ is still therapeutically active. Based upon pharmacodynamics, clinical and MRI data, NTZ appears to retain therapeutic activity up to 3 months after the last dose,32–34 leading some clinicians to employ post-NTZ washout periods of 3 months or longer. However, return of MS disease activity correlates with longer post-NTZ washout durations.15,16,21 Analyses of immune cell populations during NTZ therapy suggest potential mechanisms to explain the timing of returned, and in some cases, heightened MS disease activity following NTZ discontinuation. Sustained NTZ treatment was associated with increased circulating T-cells, B-cells and monocytes,35–37 possibly from impaired cell migration into the CNS, and elevated mobilization of T- and B-cell stem cells. 38 Return to baseline levels of circulating lymphocytes and sub-therapeutic alpha 4-integrin saturation required up to 16 weeks after the last NTZ dose. 32
A number of previous reports and studies suggest that first six months is a time interval of high risk of post-NTZ relapse.14–18 We had previously reported that initiating TFM at the time patients were due for their next NTZ infusion, and thus employing no washout, was associated with low 12-month relapse risk (proportion of relapse-free patients = 0.94), and only 2 patients (4%) experienced SDW, 30 which was in contrast to higher risks of relapse previously reported in patients with more prolonged post-NTZ washout durations.14–16,19,20 There was a statistically significant impact of age in our cohort, with patients under age 50 having greater risk of relapse while being treated with TFM. The impact of relapse occurring in the 12 months prior to starting NTZ on risk of relapse while on TFM was not significant. It was not possible to assess the relationship between disease activity on NTZ to that observed when patients were switched to TFM because disease activity or MRI changes while on NTZ were exclusion criteria for the study. While no direct outcome comparisons to other reported studies of post-NTZ DMT use would be entirely valid, the low risks of relapse we observed in our patients may provide potential guidelines for transitioning patients off NTZ.24,25,39 The safety and side effect profile in our study were similar to the results of TFM controlled clinical trials with larger cohorts,27,28 Furthermore, no cases of PML or other opportunistic infections were observed over the two-year observation period. To date there has been only one case of PML reported in a patient being treated with TFM. 13 Our safety data supports the absence of increased risk of initiating TFM without a prior NTZ washout period.
Potential shortcomings of this study include its open-label design, the absence of a comparator agent, the relatively small number of patients, and the absence of examiner blinding. The previously reported proportion of relapse-free patients in our patient population at 12 months of 94% compares favourably with results published utilizing other agents,16,30 but the conclusions that can be drawn by such non-head to head comparisons are very limited. Although the sample size was relatively small, the sensitivity of the study was strengthened by the study design, which utilized a high frequency of MRI scanning and neurological examinations. We may have introduced selection bias by excluding patients with enhancing MRI lesions at screening, which would not likely occur in routine clinical practice and did not occur in the TFM placebo-controlled trials.27,28
Strengths of this study include high frequency, consistency and quality of MRI scanning, and the reading of all MRIs by pre-designated neuroradiology MS experts. All patients at each site were studied on the same 3T scanner throughout the study. Each patient was clinically assessed at every visit by the same neurologist, each of whom had Level C Neurostatus EDSS certification and extensive experience in MS patient care evaluation and clinical research, using pre-specified criteria for relapses and disability progression.
Our results suggest that TFM, when used without a washout period for NTZ is an effective therapeutic strategy to employ for patients being taken off NTZ, with a comparatively low risk of post-NTZ relapses, especially for the first year, 30 and an acceptable safety profile. This is the first prospective study of TFM as follow-up therapy after NTZ cessation for a 2-year period, and specifically addresses issues associated with the risks of NTZ withdrawal upon MS activity risk. These results may prompt further investigation of “no withdrawal” strategies with other DMTs in the post-NTZ setting.
Footnotes
Author contributions
The study protocol was conceived, developed, and supervised by KE and SC, data management by TGF, statistical analysis by AK and EB, and all the listed authors participated in the writing and editing of the manuscript.
Declaration of conflicting interests
SC has served on advisory boards or steering committees for Biogen, Novartis, Sanofi Genzyme, AbbVie, and EMD Serono and received research support from Biogen, Novartis, Sanofi Genzyme, MedDay, and Roche Genentech, and speaker honoraria from Biogen, Novartis, Sanofi Genzyme, Bristol Myers Squibb, and Roche Genentech. KS has received research support from AbbVie, Biogen, Roche Genentech, and EMD Serono and consulting fees from Bristol Myers Squibb, Janssen, Acorda, Biogen, EMD Serono, Sanofi Genzyme, Roche Genentech, Novartis, and Teva. KE has received honoraria for speaking and consulting from Biogen and EMD Serono and research/grant support from Biogen, Sanofi Genzyme, F. Hoffmann-La Roche and Genentech, EMD Serono, and Novartis.
AK, TGF, VK, EB, and CC have no disclosures.
Role of funding source
Sanofi Genzyme provided funding to support the conduct of the study and cover the expenses of the procedures that were not part of routine care but had no influence in the design of the study, the analysis and interpretation of data, or the writing of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SC has served on advisory boards or steering committees for Biogen, Novartis, Sanofi Genzyme, and Pear Therapeutics and received research support from Biogen, Novartis, Sanofi Genzyme, MedDay, and Roche Genentech, and speaker honoraria from Biogen, Novartis, Sanofi Genzyme, and Roche Genentech. KS has received research support from AbbVie, Biogen, Roche Genentech, and EMD Serono and consulting fees from Bristol Myers Squibb, Janssen, Acorda, Biogen, EMD Serono, Sanofi Genzyme, Roche Genentech, Novartis, and Teva. KE has received honoraria for speaking and consulting from Biogen and EMD Serono and research/grant support from Biogen, Sanofi Genzyme, F. Hoffmann-La Roche and Genentech, EMD Serono, and Novartis. AK, TGF, VK, EB, and CC have no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by theSanofi Genzyme