
Abstract
Background
Most multiple sclerosis patients on disease-modifying treatment at Umeå University Hospital are treated with rituximab and the prevalence of vitamin D supplementation has increased over time. Follow-up studies of these off-label treatments are needed.
Objective
To study inflammatory activity and adverse effects in rituximab-treated multiple sclerosis patients, and associations with 25-hydroxy-vitamin D levels.
Methods
Retrospectively collected data on repeated estimates of relapses, disability, side effects, magnetic resonance imaging, laboratory measures including 25-hydroxy-vitamin D levels and self-perceived health.
Results
In 272 multiple sclerosis patients with a mean follow-up of 43 months, we identified seven possible relapses during active rituximab treatment. On magnetic resonance imaging examination, new T2 lesions were seen in 1.3% (10 out of 792 scans), and 0.25% (two out of 785 scans) showed contrast enhancement. Adjusted 25-hydroxy-vitamin D levels in samples drawn close to all magnetic resonance images with new T2 lesions were lower compared to the remainder (62 vs. 81 nmol/l; P = 0.030). Levels of 25-hydroxy-vitamin D were associated with self-perceived health (r = 0.18, P = 0.041, n = 130) and C-reactive protein (r = –0.13, P = 0.042) but not with the risk of side effects.
Conclusion
The inflammatory activity in this rituximab-treated multiple sclerosis population that increasingly used vitamin D supplementation was extremely low. Higher 25-hydroxy-vitamin D levels were associated with beneficial outcomes.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease in which recurrent inflammations directed against the central nervous system (CNS) produce increasing neurological disability if untreated.
Treatment for MS includes a variety of disease-modifying therapies (DMTs) that all aim to reduce the inflammatory activity represented by either relapses, contrast enhancing lesions (CELs), or new/enlarged T2-weighted lesions on magnetic resonance imaging (MRI). Inflammation in MS was for long regarded to be mediated primarily by T lymphocytes. 1 The hypothesis that B lymphocytes play a key role in MS2 was the basis for the Helping to Evaluate Rituxan in Relapsing–Remitting Multiple Sclerosis (HERMES) trial. 3 Rituximab (Rituxan, Mabthera) is a chimeric monoclonal anti-CD20 antibody that selectively depletes B lymphocytes from the circulation. 4 The HERMES trial showed a marked reduction of inflammatory activity in relapsing–remitting multiple sclerosis (RRMS). 3 As a result of this trial, further supported by similar findings in inflammatory active primary progressive multiple sclerosis (PPMS), 5 MS patients at the Umeå University Hospital have increasingly been treated with rituximab since 2008, initially mainly in the form of a clinical trial. 6 In Umeå, rituximab has been the most common choice of DMT since 2010, and in 2013 rituximab was chosen for 85% (73 out of 86) of MS patients starting with DMTs (data provided by Leszek Stawiarz at the Swedish MS register; www.neuroreg.se). Mounting evidence of the efficacy and safety of rituximab has led to rituximab being the most commonly used DMT for MS since 2015 in Sweden,7,8 despite lacking formal regulatory approval (off-label use).
There is evidence that vitamin D plays a role in the immune system, 9 and several observational studies show an association between low circulating levels of vitamin D and an increase of inflammatory activity in MS.10,11 Serum vitamin D levels (25-hydroxy vitamin D; 25[OH]D) has also been linked to inflammatory activity in other autoimmune diseases such as rheumatoid arthritis. 12 A causal relationship in MS aetiology has been claimed based on data from prospective observational studies, and Mendelian randomisation studies,10,13 but the methodology used in the latter studies has been criticised. 14 Since 2011, MS patients from northern Sweden attending Umeå University Hospital have been informed about the possible benefits of vitamin D supplementation. Based on accumulating scientific support,10,15 this information has gradually shifted into a recommendation to use vitamin D supplements to decrease the risk of MS inflammatory activity.
A clinical observation at Umeå University Hospital is that among MS patients treated simultaneously with rituximab and vitamin D supplementation, inflammatory activity is extremely scarce. In order to investigate this systematically, we created a database with information on our MS patients treated with rituximab. The database encompasses information from yearly examinations including reported relapses, MRI results, clinical neurological examination using the Expanded Disability Status Scale (EDSS), reported adverse effects and laboratory parameters, such as flow cytometry of circulating lymphocytes, immunoglobulin G (IgG) and 25(OH)D levels in peripheral blood.
The two parallel aims of this study were: (a) To provide a long-term follow-up of a rituximab-treated MS population regarding safety and efficacy; and (b) to study the associations between 25(OH)D levels and these outcomes.
Methods
Patient cohort
This was a retrospective cohort study of all MS patients treated at Umeå University Hospital who had received at least one intravenous infusion of either 500 or 1000 mg rituximab from March 2008 to March 2015. Patients were identified through the Swedish MS registry and local medical records. For those who discontinued treatment, data were collected until one year after the last rituximab infusion. Patients who had a retreatment interval exceeding 18 months after June 2015 were considered to have discontinued treatment. Medical records and the MS registry were reviewed for all included patients to collect data on previous treatments, dose and interval of rituximab infusions, EDSS progression, MRI findings, vitamin D supplementation, self-perceived health, adverse events (AEs) and results from laboratory analyses described below.
Ethical statement
The project was approved by the ethics committee in Umeå (Dnr 2013/445-31).
Rituximab treatment
Beginning in 2008, patients were treated with rituximab according to the HERMES protocol. 3 Since 2013 this regimen was replaced by treatment with 1000 mg given every 6–12 months. From 2015 and onwards the standard retreatment dose was reduced to 500 mg, which was given every 6 months for 3 years, and then on a yearly basis.
Vitamin D
Yearly estimates of serum 25(OH)D levels started in 2012 as clinical routine and the available results were added to the database. Analyses were performed at the hospital laboratory with liquid chromatography–tandem mass spectroscopy. With regard to vitamin D supplementation, patients were categorised into three groups: those with a vitamin D supplement prescription; those using over-the-counter supplements; and those not taking supplements. Start of treatment and dose of supplementation were also recorded.
Clinical neurological evaluation
As a measurement of MS disability, the EDSS was used 16 at clinical examinations. This was performed at yearly intervals by an MS-specialised neurologist as a part of clinical follow-up, normally prior to treatment with rituximab. The last EDSS score following the last rituximab treatment was recorded for comparison with the EDSS score preceding treatment start. Any MS relapses – including those suspected by the patient or the MS nurse on the telephone – and the corresponding dates were also recorded.
MRI
A cerebral 1.5 or 3 Tesla MRI examination was performed routinely every 12 months, and if clinically indicated. The baseline MRI was defined as the most recent MRI investigation before rituximab treatment initiation. The presence and number of CELs, and new or enlarged T2-weighted lesions were recorded on all MRIs, including the baseline MRI. As new lesions on the first MRI on rituximab treatment may have occurred before the onset of treatment effect, the presence of new T2 lesions was restricted to MRIs performed later during rituximab treatment. Some MRI analyses were restricted to those performed during the time window over which rituximab was fully active: at least 6 months after start of rituximab treatment, and a maximum 18 months after the last infusion. This time window was decided on based on clinical experience using rituximab in patients with MS.6,7 Normally, MRIs were performed with intravenous gadolinium contrast to enable visualisation of active inflammation.
Immunological laboratory samples
Yearly samples for analyses of the white blood cell (WBC) count including differential blood count, C-reactive protein (CRP), 25(OH)D and IgG were drawn approximately 2 weeks before rituximab infusions. Lymphocyte subpopulations (including CD4+ T lymphocytes and CD19+ B lymphocytes) were analysed by flow cytometry on a yearly basis in blood samples typically drawn just before a rituximab infusion. The CD19+ cell counts were not used to trigger rituximab redosing. To study the association with the last 25(OH)D estimate, we recorded the last estimate of WBCs including differential blood count, CRP and lymphocyte subpopulations.
Self-perceived health
Information on self-perceived health was collected at clinical examination and was retrieved from the Swedish MS register (www.neuroreg.se), which contains the first question in the short form health survey (SF-36): ‘In general, would you say your health is:’ and the answer is rated on a five-point scale from poor to excellent = 1–5.
Adverse events
AEs occurring during rituximab treatment were recorded from medical records covering all departments at the university hospital and primary care healthcare centres within the country and were graded according to the common terminology for AEs v. 4.03, June 2010. The following AEs were recorded with date and grading: deaths, malignancies, autoimmune disorders and infections. Grade 1 AEs and grade 2 uncomplicated lower urinary and upper respiratory tract infections were not recorded because the sensitivity was expected to be low.
Statistical methods
IBM SPSS Statistics for Windows (v 23.0, 2015 Armonk, IBM Corp., NY, USA) and R (v 3.42, 2017, R Core Team, Vienna, Austria) were used for statistical analyses. Spearman’s rho was used to calculate correlations between immunological laboratory parameters, self-perceived health and 25(OH)D levels. The independent samples t-test was used to test differences between means. The Wilcoxon signed rank test was used to test the difference between the first (before treatment) and latest EDSS values. The yearly progression of 25(OH)D levels was estimated using a mixed effect model with a random intercept for individuals. The 25(OH)D levels were adjusted for seasonal variation 17 by estimating the seasonal trend, by a second order sinusoidal function, using patients not taking vitamin D supplements. Linear regression was used for modelling the effect of median adjusted 25(OH)D levels on the change in EDSS. The effect of median adjusted 25(OH)D levels on side effects was examined using a Cox proportional hazards model and the likelihood ratio test.
A P value of less than 0.05 was considered significant.
Results
A total of 272 MS patients were followed during the study period 2008–2016 for a mean (SD) of 43 (17) months of rituximab treatment, a total of 942 patient-years (Table 1). The prevalence of vitamin D supplementation increased during the study (Figure 1). In 2010, 2.2% of patients received vitamin D supplementation (average 2000 IU/day), at the end of the study period 80% of patients took supplementation (average 2250 IU/day). Treatment with vitamin D supplements in this population corresponded to a total of 608 patient-years. The median (range) 25(OH)D level was 76 (5–278) nmol/l (30.4 [2–111] ng/ml) with an individual estimated yearly increase of 25(OH)D levels of 3.9 nmol/l (P<0.001) (Figure 2). A total of 1109 25(OH)D level measurements were performed from 2011 and onwards.

Vitamin D supplementation among rituximab-treated multiple sclerosis (MS) patients by year. The number of patients active in the study (grey bar) each year and how many of them were receiving vitamin D supplementation (white bar) are shown. Vitamin D median dose (black line) was calculated using all MS patients from this study, even if they had not yet started rituximab treatment. IU: international units.

Median 25-hydroxy vitamin D (25(OH)D) levels among multiple sclerosis (MS) patients over time. The median serum 25(OH)D level and the number of analyses each year. The black lines represent the 25 to 75 percentiles of the samples.
Baseline characteristics and treatment data for 272 patients treated with rituximab at Umeå University Hospital.
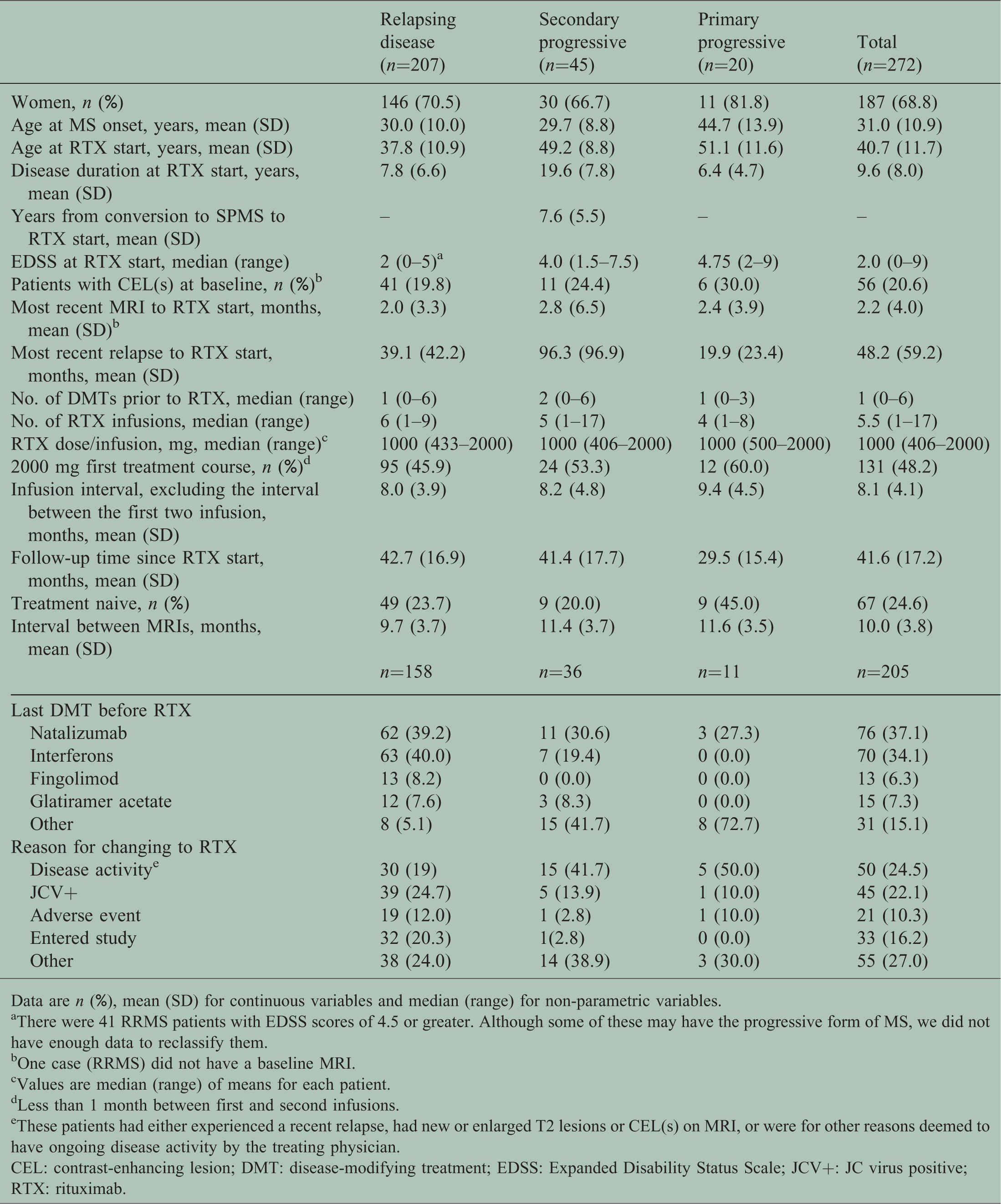
Data are n (%), mean (SD) for continuous variables and median (range) for non-parametric variables.
aThere were 41 RRMS patients with EDSS scores of 4.5 or greater. Although some of these may have the progressive form of MS, we did not have enough data to reclassify them.
bOne case (RRMS) did not have a baseline MRI.
cValues are median (range) of means for each patient.
dLess than 1 month between first and second infusions.
eThese patients had either experienced a recent relapse, had new or enlarged T2 lesions or CEL(s) on MRI, or were for other reasons deemed to have ongoing disease activity by the treating physician.
CEL: contrast-enhancing lesion; DMT: disease-modifying treatment; EDSS: Expanded Disability Status Scale; JCV+: JC virus positive; RTX: rituximab.
Rituximab treatment adherence
The most common reason for treatment discontinuation (59 out of 272) was that patients reached an age of 52–55 years, at which we usually stop DMTs because of spontaneously diminishing MS inflammatory activity with increasing age.18,19 In 21 patients in whom rituximab treatment was stopped before 52 years of age, the reason was: secondary progressive multiple sclerosis (SPMS) (median stop age 49 years) (n = 5), planned pregnancy (n = 4), AEs (n = 4), low IgG levels (3.3–5.7 g/l) (n = 3), patient wish (n = 3), inflammatory activity on spinal MRI 4 months after the first rituximab infusion (n = 1) and inflammatory inactive PPMS (n = 1). In addition, two patients continued rituximab treatment but with infusion intervals greater than 18 months, and six patients were lost to follow-up (all before age 52 years).
MRI
Excluding baseline MRIs, there were 1027 MRI examinations (1019 with gadolinium) performed during rituximab treatment. Out of these, 792 MRIs (785 with gadolinium) were made during the 6–18-month time window when rituximab was deemed active (see Methods). Only two of these MRIs showed gadolinium enhancement (two MRIs on different patients showed one gadolinium enhanced lesion). Thus, the prevalence of MRIs with CELs was 0.25% (two out of 785) in patients on active rituximab treatment. The low prevalence of CELs did not allow for comparison with 25(OH)D levels. Another three CELs were identified in 148 MRIs performed less than 6 months after treatment start.
In 1.4% (14 out of 1027) of MRI examinations, new T2 lesions were seen, 1.3% during the 6–18-month time window (10 out of 792). Fourteen adjusted 25(OH)D estimates performed closest in time (median 1.6 months) to these 14 MRIs were lower compared to the remaining adjusted 25(OH)D level estimates (62 vs. 81 nmol/l, respectively; P = 0.030). When restricted to the 10 new T2 lesions seen during the 6–18-month time window, there was no significant difference (72 vs. 80 nmol/l, P = 0.39).
Inflammatory markers
There was a significant negative correlation between CRP and 25(OH)D levels (r = –0.13, P = 0.042). This correlation was less pronounced and no longer significant when adjusted 25(OH)D levels were used. None of the other inflammatory markers in blood samples showed significant correlation with 25(OH)D levels (Table 2).
Association between immunological laboratory parameters and 25(OH)D levels.

*Statistically significant.
Relapses
New symptoms possibly representing relapses (n = 23) were recorded for 21 patients. Out of these, 14 occurred during the 6–18-month period after the most recent rituximab infusion. These medical records were scrutinised and only seven attacks, all with mild symptoms, were judged possibly to represent true relapses. Unscheduled consultations were made for four of these, either with a neurologist (n = 3) or an ophthalmologist (n = 1). In no case did MRI show a corresponding lesion either on an extra MRI (n = 2) or follow-up MRI (n = 7) (spinal MRI not performed in three cases with possible partial myelitis).
Perceived health
There was a significant correlation between self-perceived health and 25(OH)D levels (r = 0.18, P = 0.041, n = 130). This was also true in a multivariable linear regression analysis (β = 0.20, P = 0.024) adjusted for age, sex, EDSS (below or above median) and subtype (relapsing–remitting or progressive).
EDSS progression
Among all patients, there was no significant change in EDSS (before rituximab treatment compared to latest follow-up at median 38 months) during the study (median EDSS 2.0 both before and after, P = 0.59, n = 262). This was also true if only RRMS patients were analysed (median EDSS 2.0 before and 1.5 after; P = 0.13, n = 202). In patients with SPMS, there was a significant increase of median EDSS (from 4.0 to 5.5; P<0.001, n = 43). In PPMS there was a similar, however not significant, increase of EDSS (median EDSS 3.5 before and 6.0 after; P = 0.16, n = 17).
For all patients there was no association between individual median adjusted 25(OH)D levels and EDSS change. The estimated change in EDSS for a 50 nmol/l increase in median adjusted 25(OH)D levels was 0.058 (95% confidence interval (CI) –0.21–0.33; P = 0.68).
Side effects and their relation to 25(OH)D levels
In total, 105 non-infusion-related AEs as defined above were found in 77 out of 272 patients (Table 3). One patient experienced a grade 4 AE: a woman in her sixties was hospitalised for 4 days diagnosed with sepsis from Escherichia coli with onset 3 weeks after the first rituximab infusion. One patient died because of suicide without suspicion of any connection with rituximab treatment. 7 Four malignancies (all grade 2) were recorded, out of these clinical signs of one basalioma was present years before rituximab start, and one cervical cancer was known several years before rituximab start but led to conisation during rituximab treatment. A 50 nmol/l increase in median adjusted 25(OH)D levels was not associated with a significantly increased risk of side effects (hazard ratio (HR) 1.02, 95% CI 0.595–1.74; P = 0.95), which was true also if only infectious AEs were selected (HR 0.974, 95% CI 0.554–1.71; P = 0.93).
Non-infusion-related adverse events by severity, type, and frequency for 272 multiple sclerosis patients treated with rituximab at Umeå University Hospital.

Data are n (%).
aAdverse events as specified in the Methods section.
bCause of death judged to be unrelated to DMTs.
AE: adverse event; CTCAE: common terminology criteria for adverse events, version 4.03; DMT: disease-modifying therapies.
Discussion
The main finding was an extremely low occurrence of inflammatory activity in this MS population. Even if the number of new T2 lesions on MRI was indeed low during rituximab treatment, these measures may capture events that are not true signs of MS inflammatory activity, such as small vessel vascular disease on MRI. In addition, reported relapses would need confirmation from detailed neurological examination and/or MRI examination of the corresponding part of the CNS in order to be considered verified. In this real-life study, we were unable to confirm, although efforts were made, any of the reported possible relapses. The presence of CELs on MRI is a more specific measure of inflammatory MS activity, and the prevalence of just 0.25% in this study is to our knowledge unsurpassed when compared to other DMTs.
A significant association and a dose–response effect between vitamin D supplementation and health-related quality of life has been reported in MS patients. 20 These findings are supported by the present study in which we found better self-perceived health in MS patients with higher 25(OH)D levels. The association in the present study could not be explained by differences of disability.
As anticipated in treatment with monoclonal anti-CD20 antibodies, infections were the most common AE, with a panorama similar to that for ocrelizumab. 21 As the dosage regimen changed with time during the follow-up period, it is not possible to determine for how many cases the dosage regimen was changed because of infectious AEs. As B lymphocyte depletion in peripheral blood occurs after dosages much lower than those usually recommended in treatment with monoclonal anti-CD20 antibodies,22–24 a changed dosage regimen (lowered dose and/or an increased dose interval) appears to be a logical way to handle patients in whom infectious problems occur during rituximab treatment. At least three patients received repeated treatment with intravenous immunoglobulins at some point during rituximab treatment as a measure to prevent infectious side effects.
As for vitamin D supplementation, we found no association between 25(OH)D levels and the risk of AEs. With one exception, there was no significant correlation between 25(OH)D levels and the investigated laboratory markers. The negative correlation for CRP may indicate that high 25(OH)D levels are associated with a reduced risk of infection. Such a protective effect from vitamin D supplementation has been suggested. 25 However, we were unable to show any association between adjusted vitamin D levels and the risk of infectious AEs. An alternative explanation to this negative correlation with CRP could be that 25(OH)D exerts a direct anti-inflammatory effect manifesting in a reduction of CRP. 26
We found a significant increase of the EDSS in patients with SPMS, whereas in RRMS patients the EDSS was unchanged. This discrepancy may suggest that the treatment has its effect by way of decreased inflammatory activity and does not affect neurodegenerative mechanisms involved in MS progression. This is in line with a randomised controlled trial with rituximab in progressive MS patients aged up to 65 years (treatment arm mean 50.1 years). A planned subgroup analysis showed a 67% decreased risk (P = 0.0088) for EDSS progression in those aged less than 51 years with the presence of CELs at treatment start, but an opposite trend on EDSS progression among those without CELs and aged 51 years and older. 5 In the present study only six (out of 65) progressive patients were under 51 years at treatment start and had CELs, and for these median EDSS decreased non-significantly from 6.0 to 5.5. In a recently published study, treatment with ocrelizumab in PPMS patients aged up to 55 years (treatment arm mean age 44.7 years) delayed time to confirmed EDSS progression by 24% (P = 0.03), but data on the above subgroups were not provided. 27
One weakness with the present study is the observational design, which just enables us to identify associations between 25(OH)D levels or vitamin D supplementation and MS outcomes. Such associations may derive from confounding factors related to a healthier lifestyle in general among those taking vitamin supplements or having higher 25(OH)D levels.
In conclusion, this study was conducted to serve two purposes: to provide long-term follow-up data on all rituximab-treated MS patients at Umeå University Hospital since 2008, and to investigate whether 25(OH)D levels were associated with effect or AE outcomes. The main finding was an extremely low inflammatory activity. This was also a limitation as it reduced the statistical power to detect whether vitamin D supplementation added to the effect from rituximab treatment. The associations found between 25(OH)D levels and self-perceived health, and an inverse association to CRP, may together with the finding of lower 25(OH)D levels adjacent to MRI scans showing new T2 lesions, suggest that MS patients benefit from vitamin D supplements. Future follow-up studies of MS patients on this treatment at Umeå University Hospital will provide important data on these off-label treatments.
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.