
Abstract
Background
Disease-modifying therapies benefit individuals with relapsing forms of multiple sclerosis, but their utility remains unclear for those without relapses.
Objective
To determine disease-modifying therapy use and costs in 2009, compare use in 2009 and 2000, and examine compliance with evidence-based guidelines.
Methods
We determined the extent and characteristics of disease-modifying therapy use by participants in the Sonya Slifka Longitudinal Multiple Sclerosis Study (Slifka) in 2000 (n=2156) and 2009 (n=2361) and estimated out-of-pocket and total (payer) costs for 2009. Two multivariable logistic regressions predicted disease-modifying therapy use.
Results
Disease-modifying therapy use increased from 55.3% in 2000 to 61.5% in 2009. In 2009, disease-modifying therapy use was reported by 76.5% of participants with relapsing-remitting multiple sclerosis, 73.2% with progressive-relapsing multiple sclerosis, 62.5% with secondary progressive multiple sclerosis, and 41.8% with primary progressive multiple sclerosis. Use was significantly associated with relapsing-remitting multiple sclerosis, shorter duration of illness, one to two relapses per year, non-ambulatory symptoms, using a cane, younger age, higher family income, and having health insurance. Average annual costs in 2009 were US$939–3101 for patients and US$16,302–18,928 for payers.
Conclusion
Use rates were highest for individuals with relapsing-remitting multiple sclerosis, but substantial for those with progressive courses although clinical trials have not demonstrated significant benefits for them.
Introduction
For over two decades, disease-modifying therapies (DMTs) have transformed treatment for relapsing forms of multiple sclerosis (MS). Clinical trials involving individuals with secondary progressive MS show reductions in relapse rates but, with few exceptions, 1 not in disability progression.2–6 In spite of their increasing prevalence as the MS population ages, 7 we know little about the efficacy of DMTs in older, non-ambulatory individuals because they are generally excluded from clinical trials.
The US Food and Drug Administration indicates and experts recommend DMTs for relapsing-remitting MS and secondary progressive disease with continuing relapses. In 2002, the American Academy of Neurology’s (AAN) clinical practice guideline additionally stated that the ‘effectiveness [of interferon beta] … [in secondary progressive MS] without relapses is uncertain … [and although glatiramer acetate [may be] helpful [in progressive disease], there is no convincing evidence to support this hypothesis.’ 2 The Paris Workshop Group took the same position. 8 Shortly thereafter, echoing the Royal College of Physicians of London, 9 the National Multiple Sclerosis Society (NMSS) stated that ‘it is the consensus of researchers and clinicians [that DMTs] can reduce future disease activity and improve quality of life for many individuals with relapsing forms of MS, including … secondary progressive disease [with] relapses.’ 10 In 2007, they strengthened ‘can reduce’ to ‘are likely to reduce’. 11
As early as 2002, MS experts registered concern about DMT use in patients without active disease: Vollmer and colleagues finding 28% of patients with primary progressive MS taking DMTs, despite the lack of data supporting such use, commented that ‘some treatment patterns … do not appear to be rational given studies and consensus guidelines for use of [DMTs].’ 12 Nevertheless, by 2004, use in this population had increased by 20–40%. 13
Without evidence to guide them, clinicians remain divided on whether to initiate DMTs for individuals with secondary progressive MS without relapses or continue treatment started for relapsing-remitting MS after relapses have ceased.14–17 Faced with side effects and increasing prices, patients and families remain unsure about the costs versus benefits.
Given these complexities, we asked: ‘What are the extent and predictors of DMT use in a representative sample of individuals with MS?’ and ‘What are consumer out-of-pocket (OOP) and total (payer) DMT costs?’ Using data from the Sonya Slifka Longitudinal Multiple Sclerosis Study (Slifka),18,19 we hypothesized that real-world DMT prescribing practices would diverge from evidence-based guidelines and that use would be associated with income and health insurance status. Although this is a health services and not a clinical or treatment study, it raises the most fundamental question clinicians, patients, and families should ask themselves: ‘Is DMT appropriate?’
Materials and methods
Data source
Initiated and funded by the NMSS, the Slifka Study collected data from 2000 to 2010. We recruited cohort 1 (N=2156) in 2000 and cohort 2 in 2007/2008 (N = 2478) by randomly selecting participants from the NMSS mailing lists and conducting nationwide outreach for under-represented groups, i.e., recently diagnosed (within 12 months), ages 18–24 years, African-American, and Hispanic. We stratified by census region and rural and urban location, and used fractional sampling intervals to select systematic samples. 18 We confirmed diagnoses with participants’ MS care providers or used proxy criteria (ever used a DMT and can report diagnosis date, course, and three typical MS symptoms). Comparison of cohort 1 to MS respondents in the National Health Interview Survey and the general population in the US Census demonstrated that participants generally represented the known demographic characteristics of the MS population. For the 2009 interview, we recruited all remaining cohort 1 and 2 participants achieving response rates of 62.5% and 41.4%, respectively, and a final sample of 2361.
We obtained institutional review board approval with waiver of written informed consent for community residents. At baseline, community residents provided verbal consent and nursing home residents signed written consent forms.
The Slifka computer-assisted telephone interviews used well-tested questions from federal surveys for sociodemographic characteristics; standard definitions of MS course, relapse, and progression; 20 and Disease Steps 21 for disability status. At the end of their 2007/2008 interviews, we asked participants to keep daily records of their use of and spending on medications and health services for complete and accurate reporting during their 2009 interviews: 84% reported doing so or having so little to report that recall was accurate. The ‘recall periods’ between individual participants’ 2007/2008 and 2009 interviews ranged from 13 to 27 months. We adjusted each participant’s recall period to a standardized 12-month interval to obtain comparable data on relapses, months of DMT use, and number of prescriptions, i.e., number of relapses/months/prescriptions*(12 months ÷ number of months in recall period).
We report utilization and costs for five of the six DMTs available in 2009: interferon beta-1a (Avonex®), interferon beta-1b (Betaseron®), glatiramer acetate (Copaxone®), interferon beta-1a (Rebif®), and natalizumab (Tysabri®). We excluded mitoxantrone (Novantrone®) because there were only 21 users.
Estimating costs
To determine the average annual OOP cost, we multiplied participants’ reported payments per prescription (standardized to a one-month supply) by the number of prescriptions or months of use if missing (adjusted for variation in recall periods).
Determining the average annual total cost to private and other payers is difficult because this information is not publicly available. However, Medicaid programs release retail transaction data for drugs, including quantities and total amounts paid to the pharmacy from any source. In 2009, Medicaid medication costs were similar to those of other payers because their reimbursements used comparable discounts off published list prices. 22 We therefore estimated the average annual total cost for each DMT by multiplying the number of prescriptions or months of use over patients’ adjusted recall periods by the average price per prescription in the national Medicaid drug utilization files. 23
Data analysis
We used data from the 2009 interview to determine the extent of DMT use overall and by drug, OOP and total costs, and significant differences in demographic and disease characteristics between users and non-users (chi-squared tests). We identified predictors of DMT use and tested our hypothesis regarding the impact of income and health insurance status using two multivariable logistic regressions: model 1 with only disease characteristics and model 2 with additional sociodemographic attributes and insurance status. We report adjusted odds ratios (95% confidence intervals) and use P values less than 0.05 for statistical significance. Finally, for 2009, we show how total and OOP costs compared by course. Analyses excluded missing data, generally less than 1% of responses.
To explore our hypothesis regarding the impact of evidence-based guidelines on real-world DMT practice, we used previously published data from the 2000 Slifka interview. 19 We compared the percentage of individuals using DMTs in 2000 and 2009 by disease characteristics and age ([number users/number in subsample]*100), calculated changes in use rates from 2000 to 2009, and assessed whether user characteristics were consistent with evidence-based guidelines.
Results
DMT use
Seventy per cent of participants in 2009 (n=1651) reported DMT use. Of these, 38.8% used glatiramer acetate, 28.7% interferon beta-1a (Avonex®), 18.2% interferon beta-1b, 17.9% interferon beta-1a (Rebif®), and 11.9% natalizumab. Eighty-six per cent of users (n=1417) took one DMT, with the remainder using two (n=212), three (n=21) or four (n=1) different DMTs over their recall periods. Of the one DMT users, 82.7% (n=1172) reported continuous use throughout their recall periods; others had complex patterns of starts, stops, and switches.
Tables 1 and 2 show participants’ demographic and disease characteristics. DMT use fell with increasing age from 93.8% of individuals aged 18–34 years to 28.8% of those aged 75 years and older (P<0.0001) (Table 1). Use was also associated with being married or never married compared to widowed or divorced, being employed, having higher family income (all P<0.0001), and being a student (P=0.005). Having health insurance (P<0.0017) and private health insurance (P<0.0001) were associated with DMT use as was living in the northeast census region (P=0.05).
Demographic characteristics associated with use of disease-modifying therapies (DMTs) during recall period (September 2007 to November 2009). a

aDemographic characteristics reflect status at the time of interview (end of recall period) except for health insurance status. DMT use covers the entire recall period.
bStudy sample n=2361. Two participants were excluded from analyses because of missing data.
cChi-squared tests. Statistically significant P<0.05.
dTotal combined income before taxes of all family members and from all sources during previous calendar year, including money from jobs, net income from business, farm or rent, pensions, dividends, interest, social security, retirement income, disability insurance, unemployment payments, public assistance, etc.
eHealth insurance types: ‘Private only’ includes commercial, Tricare, American Association of Retired Persons, drug plans; ‘Other public only’ includes any public insurance except Medicare, i.e. Medicaid, General Medical Assistance, Veterans Health Administration, Indian Health Service, Workers Compensation, other government plan; ‘Mixed coverage’ includes any combination of private plus public insurance.
Disease characteristics associated with use of disease-modifying therapies (DMTs) during recall period (September 2007 to November 2009). a
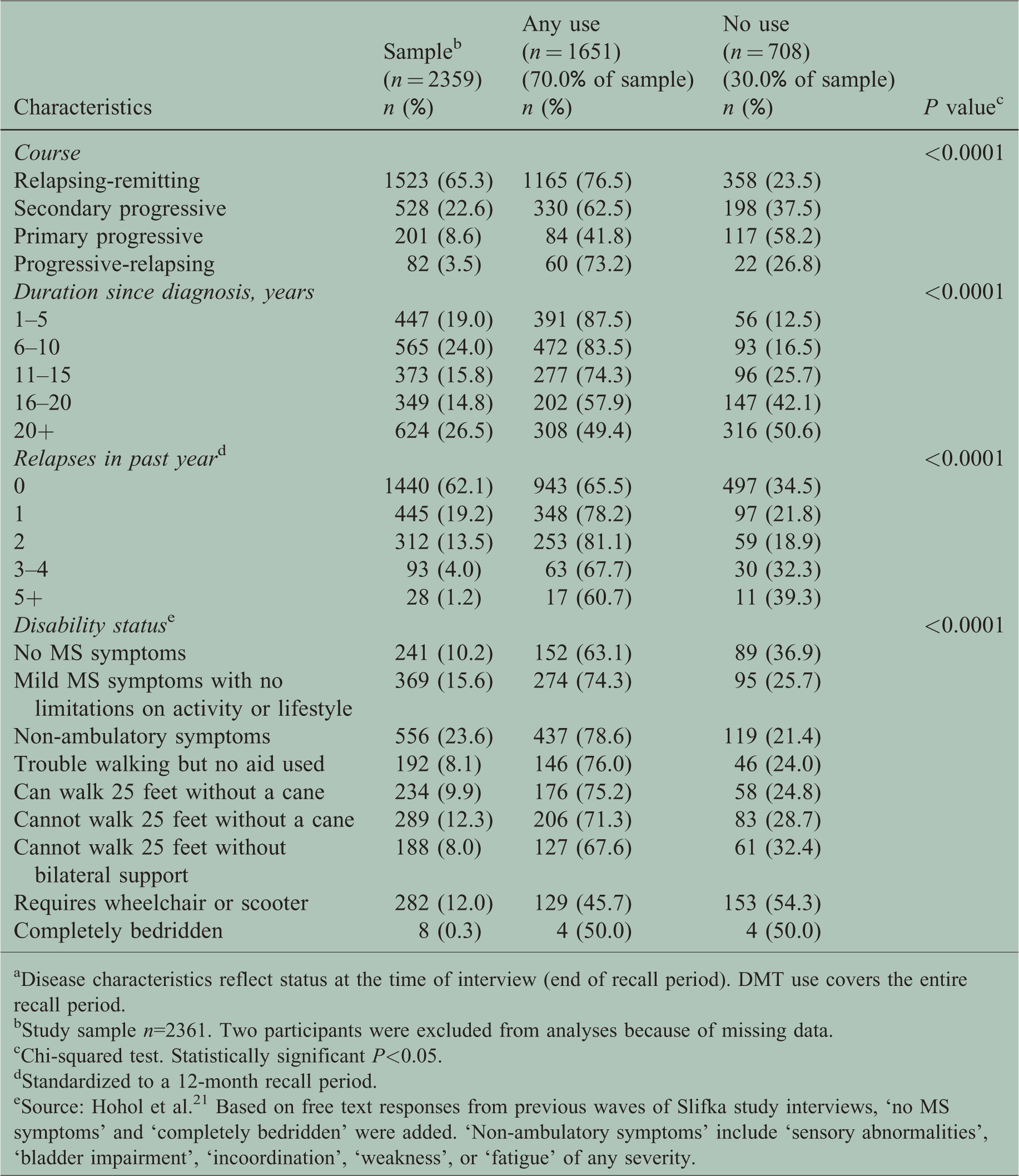
aDisease characteristics reflect status at the time of interview (end of recall period). DMT use covers the entire recall period.
bStudy sample n=2361. Two participants were excluded from analyses because of missing data.
cChi-squared test. Statistically significant P<0.05.
dStandardized to a 12-month recall period.
eSource: Hohol et al. 21 Based on free text responses from previous waves of Slifka study interviews, ‘no MS symptoms’ and ‘completely bedridden’ were added. ‘Non-ambulatory symptoms’ include ‘sensory abnormalities’, ‘bladder impairment’, ‘incoordination’, ‘weakness’, or ‘fatigue’ of any severity.
Table 2 shows DMT use during standardized recall periods by disease characteristics. Use rates differed significantly across all categories (P<0.0001). Among individuals with relapsing-remitting MS, 76.5% reported DMT use, compared with 41.8% with primary progressive MS. Use rates fell from 87.5% of individuals diagnosed within five years to 49.4% of those diagnosed 20 or more years earlier. Among those using wheelchairs or scooters, 45.7% used a DMT, as did half of those completely bedridden.
Comparing demographic and disease characteristics of DMT users in 2000 and 2009 shows for 2009 higher percentages of individuals who were aged 55 years and older, African-American, married, widowed, unemployed, needed a cane or bilateral support, and had postgraduate education and long durations of illness (see Supplementary Table 1).
Table 3 shows the multivariable models predicting DMT use. Adding sociodemographic characteristics (model 2) did not substantially change the adjusted odds ratios of use associated with disease characteristics (model 1). Participants with relapsing-remitting MS, non-ambulatory symptoms (e.g. sensory and bladder problems, fatigue), one to two relapses per year, shorter disease durations, or who needed a cane were significantly more likely to use DMTs than others. Significant sociodemographic characteristics associated with DMT use were aged less than 45 years and family income of US$100,000 or greater. Having health insurance increased the probability of use as did private coverage.
Adjusted odds ratios from multivariable logistic regression models predicting use of disease-modifying therapies (DMTs) (September 2007 to November 2009). a

aDisease and demographic characteristics reflect status at the time of interview (end of recall period). DMT use covers the entire recall period.
bStatistically significant P<0.05.
cStandardized to a 12-month interval.
dSource: Hohol et al. 21 Based on free text responses from previous waves of Slifka study interviews, ‘no MS symptoms’ and ‘completely bedridden’ were added. ‘Non-ambulatory symptoms’ include ‘sensory abnormalities’, ‘bladder impairment’, ‘incoordination’, ‘weakness’, or ‘fatigue’ of any severity.
eTotal combined income before taxes of all family members and from all sources during previous calendar year, including money from jobs, net income from business, farm or rent, pensions, dividends, interest, social security, retirement income, disability insurance, unemployment payments, public assistance, etc.
fHealth insurance types: ‘Private only’ includes commercial, Tricare, American Association of Retired Persons, drug plans; ‘Other public only’ includes any public insurance except Medicare, i.e. Medicaid, General Medical Assistance, Veterans Health Administration, Indian Health Service, Workers Compensation, other government plan; ‘Mixed coverage’ includes any combination of private plus public insurance.
AOR: adjusted odds ratio; CI: confidence interval.
DMT costs
Table 4 shows that in 2009, across the DMTs, the average monthly total price per prescription ranged from US$2056 to US$2536. For DMTs available in 2000, these prices ranged from US$781 to US$948. In 2009, average annual total costs per participant ranged from US$16,302 to US$18,928 with large standard deviations and ranges indicating high variability across individuals and costs as high as US$56,483. Average OOP costs ranged from US$130 to US$319 per prescription and US$939–3101 per year, with high variability and payments up to US$7495. Costs do not vary much by disease course, but do so within courses (Table 5). Forty-eight per cent of natalizumab users and 13.6–21.5% of other users had no OOP costs, mainly because of full coverage by their insurance, the Veteran’s Health Administration or state or other programs (see Table 6).
Total and out-of-pocket costs for users of disease-modifying therapies (DMTs) during recall period. a

aTotal cost is the amount paid by both insurers and patients to the pharmacy. Out-of-pocket (OOP) cost is the patient component of the total cost. Rebates and coupons are not accounted for due to data limitations. Costs are given in 2009 US dollars.
bStandardized to a 12-month interval.
cPrice per prescription = amount paid by both insurers and patients to the pharmacy per prescription estimated from 2009 State Drug Utilization Data. https://www.medicaid.gov/medicaid/prescription-drugs/state-drug-utilization-data/index.html. Accessed October 25, 2018. Prices per prescription in 2000 are available for interferon beta-1a (Avonex®) (US$784), interferon beta 1-b (Betaseron®) (US$948), and glatiramer acetate (Copaxone®) (US$781).
dTotal cost per year = price per prescription × number of prescriptions per year (or months of use if number of prescriptions missing).
eOOP cost per prescription and OOP cost per year = patient component of the applicable total costs. Excludes participants who paid zero.
Comparison of total and out-of-pocket costs per year by disease course for disease-modifying therapies (DMTs) during recall period (September 2007 to November 2009).a,b

aTotal cost is the amount paid by both insurers and patients to the pharmacy. Out-of-pocket cost is the patient component of the total cost. Rebates and coupons are not accounted for due to data limitations. Costs are given in 2009 US dollars.
bNumber of users by course: RRMS=1165, SPMS=330, PPMS=84, PRMS=60.
Percentage of users in course: RRMS=76.5%, SPMS=62.5%, PPMS=41.8%, PRMS=73.2%.
Percentage of users in sample: RRMS=49.3%, SPMS=14.0%, PPMS=3.6%, PRMS=2.5%.
OOP: out-of-pocket; RRMS: relapsing-remitting multiple sclerosis; SPMS: secondary progressive multiple sclerosis; PPMS: primary progressive multiple sclerosis; PRMS: progressive-relapsing multiple sclerosis.
Reasons for zero out-of-pocket costs for users of disease modifying therapies (DMTs) during recall period.

aFor percentages, denominators are the number of users of the particular DMT.
bFor percentages, denominators are the number of participants who provided reasons (101, 41, 97, 47, 93, respectively, from left to right).
OOP: out-of-pocket.
Change in DMT use: 2000–2009
DMT use by Slifka participants rose from 55.3% in 2000 19 to 61.5% in 2009 (Table 7), primarily among those with relapsing courses (relapsing-remitting MS by 5.2% and progressive-relapsing MS by 19.5% for a total of 24.7%). Use also rose for individuals aged over 54 years (by 15.8%) and those with long durations (by 20.7% for six to 15 years and 14.9% for over 16 years). Rates increased by 4.3% for individuals with secondary progressive MS, but decreased by 2.1% for those with primary progressive MS.
Comparison of use of disease-modifying therapies (DMTs) by Slifka study participants at the time of their interviews in 2000 and 2009. a

a2000 analyses: DMTs include interferon beta-1a (Avonex®), interferon beta-1b (Betaseron®), glatiramer acetate (Copaxone®). 2009 analyses: DMTs include the above plus interferon beta-1a (Rebif®), natalizumab (Tysabri®). Denominators do not exclude two subjects with missing data (as in Table 2).
bUnweighted percentage of users in sample or subgroup (number of users/number in sample or subgroup). Numerators are the number of users at time of interview (not over recall period as in Table 2).
cSource: Minden et al. 19
dOf the 528 patients in 2009 who reported a course of secondary progressive MS, 333 (63.1%) reported zero relapses and 195 (36.9%) reported one or more relapses in the preceding year.
eOf the 201 patients in 2009 who reported a course of primary progressive MS, 39 (19.4%) reported one or more relapses in the preceding year.
fSource: Hohol et al. 21 Based on free text responses from previous waves of Slifka study interviews, ‘no MS symptoms’ and ‘completely bedridden’ were added. ‘Non-ambulatory symptoms’ include ‘sensory abnormalities’, ‘bladder impairment’, ‘incoordination’, ‘weakness’, or ‘fatigue’ of any severity.
NA: category not included in 2000 interview.
Discussion
Utilization of DMTs by Slifka Study participants between 2000 and 2009 indicate a clear and persistent deviation from readily available scientific evidence. Even though higher use rates in 2009 for relapsing-remitting MS show conformity to evidence-based guidelines, and increased use from 2000 to 2009 for both relapsing courses suggests effective guideline dissemination, for other patients many prescribers seem to have paid little heed to the recommendations or were not educated in appropriate implementation. Despite the absence of data showing benefit for individuals with non-relapsing forms of MS presented in clinical guidelines carefully formulated by teams of experts, over one-third of participants with primary progressive MS and about one-half with secondary progressive MS received a DMT. Similarly, without evidence of benefit for more disabled and older individuals, over one-third of participants requiring a wheeled mobility aid used DMTs and use increased by nearly 16% among individuals over the age of 54 years, the median onset for secondary progressive disease. 24 We cannot tell from these data whether older individuals with long disease durations and progressive disabling courses were continuing therapy started when younger, less disabled, and still having relapses, or whether treatment was initiated more recently. However, given evidence of declining DMT persistence among patients with longer duration and greater disability, our results are likely to reflect non-evidence-based initiation of DMT. 25
For medicine as a whole, non-adherence to evidence-based guidelines varies widely from 10% to 80%,26,27 and many explanations have been proposed. Unintentional deviations may reflect lack of knowledge, error, or uncritical reliance on others’ opinions (‘herding’ behavior). 28 Intentional deviations, often valid, include contraindications, patient and physician preferences, absent or ambiguous cost-benefit data, and patient demographics. 26
In 2000 and certainly in 2009, there was repeated clinical trial evidence that DMTs do not work adequately in non-relapsing MS. Still, without positive evidence from purposefully designed clinical trials, there is controversy and uncertainty for clinicians and patients looking for guidance on treatment decisions. In 2013, the AAN advised clinicians to ‘not prescribe [DMTs] to patients with disability from progressive, nonrelapsing forms of MS’ because there was no evidence of benefit that outweighed potential adverse effects and financial burden, particularly for those over aged 54 years and no longer ambulatory. 14 Implicit in this statement is the requirement of adequate evidence for a treatment recommendation and a recommendation to follow published guidelines.
Other MS experts responded that this was ‘an oversimplified recommendation’ because ‘progressive patients who are on one of these agents and having no relapses are likely obtaining a partial treatment benefit and should remain on the agent’. 29 Implicit in this statement are two arguments. First, the ‘absence of evidence is not evidence of absence', 30 i.e., lacking evidence of benefit does not mean there is no benefit, simply that more research is needed. Second, patients cannot wait until we have the data. The ‘absence of evidence’ argument may justify treatment when outcomes are truly unknown, but when well-designed randomized clinical trials have been negative, the argument should be that further studies are required.
Fortunately, a randomized clinical trial is underway on the safety of discontinuing DMTs in individuals aged 55 years and older without relapses or MRI changes, but data will not be available until at least 2021. 31 Meanwhile, the field wants to know ‘What can we do now?’ First, patients and clinicians can read the latest guidelines 32 and research,33–38 discuss reasons for departures, and reach a shared decision despite the discomfort of having little clear and compelling evidence. Second, the MS community can engage in ‘unbiased discussion’39,40 that examines the full range of issues from patient and family preferences to societal costs due to increased healthcare expenditures, taking care not to present opinion as fact and to recognize the communal context 28 and external influences on treatment decisions. The 2018 guideline development process is noteworthy for its inclusion of people with MS and public reviews and emphasis on patient-doctor communication: as such, it sets an example for discussing its recommendation that ‘clinicians should assess the likelihood of future relapse’ and ‘may advise discontinuation of DMT in people with [secondary progressive MS] who do not have ongoing relapses (or … MRI activity) and have not been ambulatory … for at least 2 years. 32
Our study showed that annual total costs for first generation DMTs were three times higher in 2009 than in 2000. They have skyrocketed since then to over US$60,000,41,42 some even to US$86,000, 43 with annual increases seven times higher than average drug inflation. 44 We do not know, but should ask, whether use without evidence was contributory to the cost containment efforts discussed below. Escalating total costs inevitably increases the patient’s share: even in 2009 some individuals reported extraordinary OOP spending.
Our observation that people with high incomes and health insurance were more likely to use DMTs almost certainly indicates that low income and inadequate coverage limited access to these medications, reflecting well-known causes of healthcare disparity. Even though expansion of Medicaid with the Affordable Care Act provides coverage to many previously uninsured patients, their DMT utilization is lower than among the commercially insured. 45 Use is also lower among those with high cost-sharing plans. 46
Limitations
This study has limitations. First, the data do not include DMTs approved since 2009. However, a fundamental concern has not changed since 2000: in spite of clear and consistent guidelines, and no new evidence to the contrary, many patients are still newly prescribed or continued on DMTs without evidence of their effectiveness. Furthermore, from 2009 to 2014, injectable DMTs were still used by 93.7% of almost 9000 individuals with MS initiating and 60.6% of those switching DMTs. 47
Second, Slifka participants may not fully represent individuals with MS in the USA. Nevertheless, the sample includes patients receiving care in both academic and community settings and from MS specialists, general neurologists, and primary care physicians, thereby representing the full range of treatment practices. Because we followed participants over a critical nine-year period, from early adoption to established DMT use, we could show that prescribing DMTs for patients for whom there was no evidence of benefit continued in spite of consistent evidence-based guidelines.
Third, because information on private sector drug prices is unavailable, we had to rely on Medicaid payments to impute total DMT costs for patients mainly covered by private insurance and, without rebate information, we may have overestimated by an unknown amount. Still, Medicaid is the best available source of retail transaction costs, particularly for the years of our study. Because OOP costs were based on participants’ daily records, they are reliable.
Despite these limitations, our results have important implications for the present and for future studies of DMT utilization. Our findings can serve as benchmarks as prices rise and payers intensify efforts to control costs, producing ‘a cascade of negative effects’ on patients and families. 44 A recent survey of 59 health plans revealed that 93% require prior authorization and 58% use step therapy for DMTs, 48 and formulary restrictions have been shown to affect adherence negatively. 49 The overutilization of DMTs by patients unlikely to benefit will heighten insurers’ cost concerns and could lead to greater constraints on patient and clinician preferences. If patient-centered care is to become a certainty, decisions about DMT use ought to be driven by the evidence and further informed by the clinician’s medical judgment and the patient’s goals and values. Our data indicate that real-life decision-making is highly variable and that more evidence and education are needed to ensure the most appropriate treatments for the right individuals at the right time at the right cost.
Improving MS health outcomes and access to care while controlling escalating costs will require concerted efforts to adhere to the evidence-based guidelines we have now, while continually working to improve them, 26 study their implementation and acceptance, and remove barriers to prompt DMT initiation and equitable use. Guideline dissemination and education are essential, and should be free of pharmaceutical and payer influence.
Supplemental Material
Supplemental material for Use and cost of disease-modifying therapies by Sonya Slifka Study participants: has anything really changed since 2000 and 2009?
Supplemental Material for Use and cost of disease-modifying therapies by Sonya Slifka Study participants: has anything really changed since 2000 and 2009? by Sarah L Minden, R Philip Kinkel, Helene T Machado, Jonathan S Levin, Meredith B Rosenthal and Lisa I Iezzoni in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors are grateful to the National Multiple Sclerosis Society and its advisors for their vision in creating and providing ongoing support of the Sonya Slifka Longitudinal Multiple Sclerosis Study and the studies that have used its data. The authors particularly appreciate the wisdom, advice, and guidance of our project officer, Nicholas G LaRocca.
Conflict of Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SLM is receiving research grant support from Biogen, Inc. and has received honoraria for attending advisory meetings convened by Genentech, Inc., Novartis, EMD Serono, Inc, Pfizer, Inc, Avanir Pharmaceuticals. RPK is a scientific consultant for Cortechs Labs and Novoron Bioscience, Inc. and has received honoraria from Biogen, Genzyme, Genentech and Acorda for education programs. The remaining authors report no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Multiple Sclerosis Society, contract no.: HC 0107. The entire Slifka Study database (2000–2010) and related research materials can be accessed with permission of the National Multiple Sclerosis Society by contacting the corresponding author, Sarah L Minden.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.