
Abstract
Background
Fingolimod is a sphingosine 1-phosphate receptor modulator for the treatment of patients with relapsing forms of multiple sclerosis (RMS). Fingolimod sequesters lymphocytes within lymphoid tissue thereby reducing the counts of circulating lymphocytes. However, fingolimod’s effects on the innate and adaptive components of the immune system are incompletely understood.
Objective
The FLUENT study will investigate temporal changes in circulating immune cell subsets in patients with RMS treated with fingolimod. Secondary objectives include examining the association between anti-John Cunningham virus (JCV) antibody status/index and phenotypic changes in innate and T and B cell subsets in patients on fingolimod therapy, and the association between serum neurofilament levels and clinical outcomes.
Methods
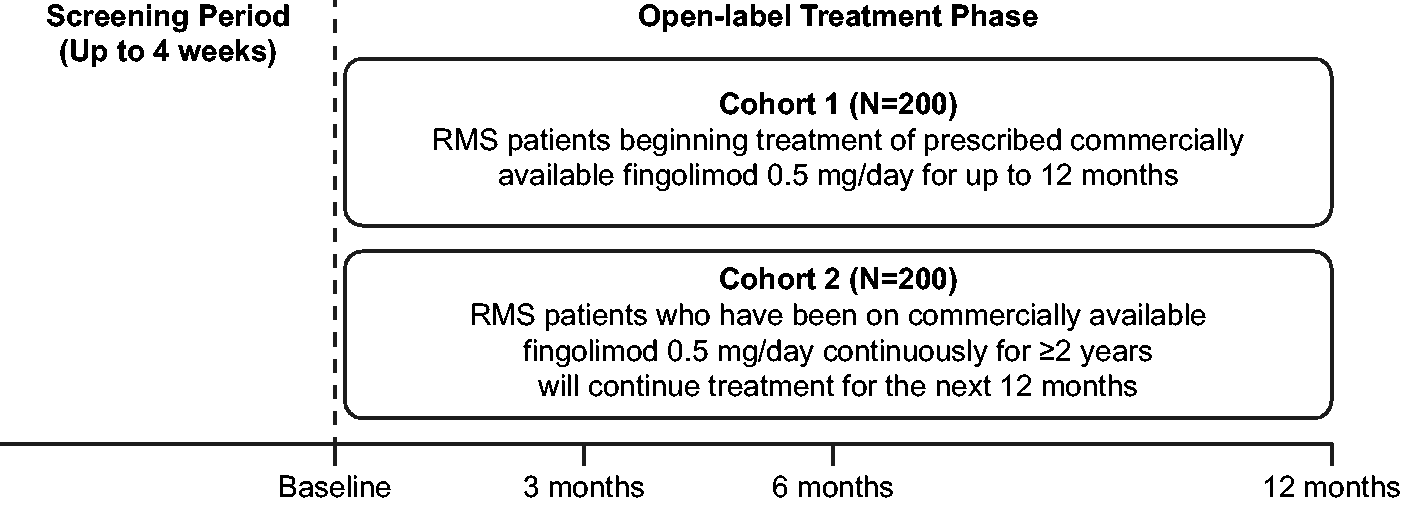
FLUENT is a prospective, multicenter, two-cohort, nonrandomized, open-label Phase IV study. Cohort 1 will include fingolimod-naïve patients and Cohort 2 will include patients who have received fingolimod 0.5 mg/day continuously for ≥2 years. Changes in the cellular components of the innate and adaptive immune system will be characterized over 12 months.
Results
The study is ongoing.
Conclusion
FLUENT may provide evidence for the use of immunologic profiling in predicting efficacy and risk of infection in patients with RMS treated with fingolimod.
Introduction
Fingolimod is a sphingosine 1-phosphate receptor (S1PR) modulator for the treatment of patients with relapsing forms of multiple sclerosis (RMS). 1 Dose-dependent reductions in peripheral lymphocyte counts to 20–30% of baseline values are observed in patients treated with fingolimod, due to reversible sequestration of lymphocytes in lymphoid tissues. 1 Fingolimod reduces the number of CD4+ and CD8+ T cells in peripheral blood, the effect being more pronounced for the CD4+ T cell subset. 2 Fingolimod differentially affects immune cell subsets; modulation of S1PRs, principally S1PR1, favors retention of CCR7-expressing naïve and central memory T cells, including Th17 cells, in lymph nodes, thereby reducing the egress of potentially pro-inflammatory autoreactive lymphocytes and limiting their infiltration into the central nervous system. 3 Effector memory T (TEM) cells, which lack CCR7, 4 do not regularly circulate through lymph nodes and are largely unaffected by fingolimod.3,5 This could be important in maintaining immune surveillance during fingolimod therapy.
However, phenotypic changes in the innate and adaptive components of the immune system are incompletely understood and were not investigated in pivotal trials. Further, the relationship between anti- John Cunningham virus (JCV) antibody status and index and immune cell subsets during fingolimod treatment has not been explored. The Biobank study (NCT01310166) and its extension (NCT02720107) investigated the effect of fingolimod treatment on major immune cell populations over 48 months in patients with MS. A limited number of immune subsets were analyzed, and no assessments were made between 6 months and 48 months, restricting information on when specific cellular changes occur. In addition, no relationship with clinical efficacy or therapeutic risk was explored.
Levels of serum neurofilaments (sNfL) are increased in patients with MS with recent relapse or disability worsening, and therefore may have a role as biomarker of disease activity and effects of treatment. 6 In patients with MS, sNfL levels correlate strongly with CSF NfL, 7 which decrease substantially in patients treated with fingolimod. 8
Clinical studies did not demonstrate an increased risk of infectious adverse events (AEs) compared with placebo, 9 and no new safety signals were identified in longer-term studies.10,11 However, rare occurrences of opportunistic infections associated with fingolimod therapy have been reported in the post-marketing setting, including cases of progressive multifocal leukoencephalopathy (PML), as well as herpes virus, cryptococcal infection, and atypical mycobacterial infections.1,12
T and B cells participate in a wide range of cellular and humoral host defense responses, and it is now widely accepted that both lymphocyte subsets contribute to the pathogenesis of multiple sclerosis. The FLUENT study (NCT03257358) was designed to investigate temporal changes in these immune cell subtypes in fingolimod-naïve patients with RMS and in those receiving chronic fingolimod therapy (0.5 mg/day) continuously for ≥2 years. The association between sNfL levels and clinical relapse, magnetic resonance imaging (MRI)-based variables, and patient-reported outcomes of disability status will also be explored. In addition, the association between JCV antibody status and index and phenotypic changes in immune cell subsets during short- and long-term fingolimod therapy will be assessed. JCV antibody status is an exploratory outcome of the FLUENT study because PML can only occur with JCV infection, and PML has been reported in fingolimod-treated MS patients in the post-marketing setting.
Materials and methods
Study design
FLUENT is a prospective, multicenter, two-cohort, nonrandomized, open-label Phase IV study in adult patients with RMS to investigate changes in immune cell subsets and biomarkers during treatment with fingolimod. Patients will be stratified into two cohorts: Cohort 1 will include fingolimod-naïve patients; Cohort 2 will include patients who have received fingolimod 0.5 mg/day continuously for ≥2 years, thereby providing data on both short-term (Cohort 1) and longer-term (Cohort 2) changes in immune cells subsets during fingolimod therapy. Following a screening period of up to 4 weeks, eligible patients will enter a treatment period and will take fingolimod 0.5mg/day orally, as prescribed per the Gilenya US prescribing information (Figure 1). 1
Study design.
The study was designed, and shall be conducted and reported, in accordance with the International Conference on Harmonisation Guidelines for Good Clinical Practice (as well as applicable local regulations), and the ethical principles laid down in the Declaration of Helsinki., The study protocol will be approved by each center’s independent ethics committee.
Study Population
Inclusion and exclusion criteria are listed in Table 1. Contraindications to treatment according to the Gilenya prescribing information will be adhered to. 1
Inclusion and exclusion criteria.
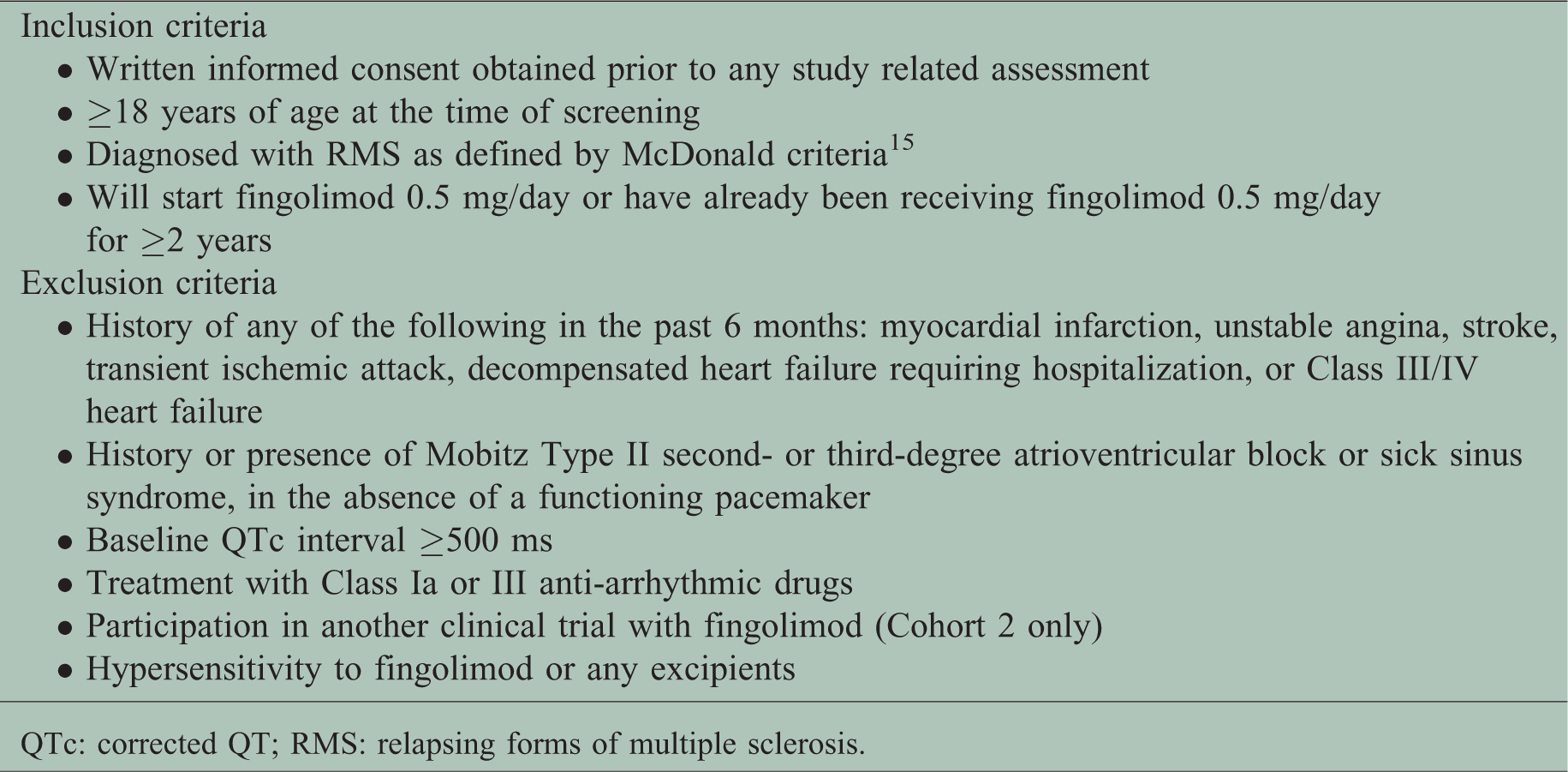
QTc: corrected QT; RMS: relapsing forms of multiple sclerosis.
The target for enrollment is 400 patients (approximately 200 in each cohort) from up to 125 centers in the USA. As a 25% screening failure rate is expected, approximately 533 patients will be screened. Patients who discontinue following enrollment will not be replaced.
Study treatment
Patients will receive commercially available oral fingolimod 0.5 mg/day, prescribed by the treating physician. Patients in Cohort 1 will undergo first-dose observation, which, according to the Gilenya prescribing information, 1 may occur at a site capable of managing any symptoms that may arise. Following completion of the first-dose observation, fingolimod will be self-administered. In Cohort 2, all doses of fingolimod will be self-administered. Both treatment cohorts will remain on treatment with fingolimod 0.5 mg/day from baseline (Day 1) for a period of 12 months.
Study objectives and endpoints
The primary objective of this study is to characterize phenotypic changes in peripheral blood cellular components of the innate (monocytes, neutrophils and NK cells) and adaptive (T cells, B cells) immune system, including their subsets. Change from baseline to Month 6 in surface markers representative of different immune cell subsets and biomarkers to be assessed are listed in Table 2.
Immune cell subsets and biomarkers to be assessed.
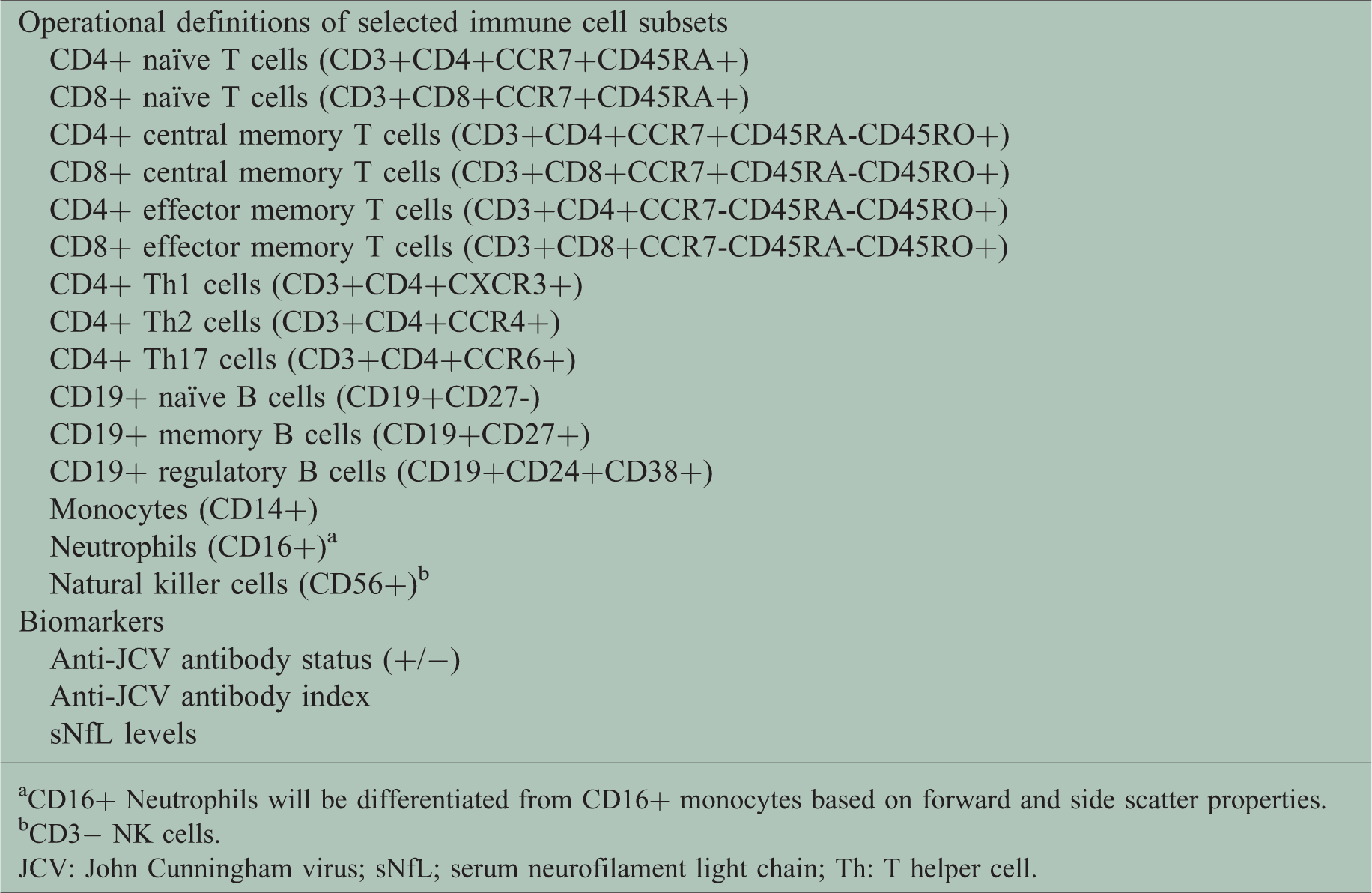
CD16+ Neutrophils will be differentiated from CD16+ monocytes based on forward and side scatter properties.
CD3− NK cells.
JCV: John Cunningham virus; sNfL; serum neurofilament light chain; Th: T helper cell.
The secondary objectives are to investigate the association between anti-JCV antibody status and index, and phenotypic changes in T and B cell subsets. Anti-JCV antibody status, and change from baseline in anti-JCV antibody index, will be measured at Months 3, 6, and 12. Change from baseline to Months 3 and 12 will be assessed for immune cell subtypes and biomarkers listed in Table 2.
sNfL levels at Months 3, 6, and 12, as well as any relationship between these levels and clinical outcomes, will be assessed as an exploratory objective.
Study assessments
Table 3 lists the procedures to be undertaken during the study. Patients should be seen for all visits on the designated day, or as close as possible thereafter.
Study flow chart.

Patients who discontinue study participation should return for a study discontinuation visit, as soon as possible, or at least within 14 days of, the last dose of fingolimod.
First date of treatment, dosage, and frequency will be recorded for all patients in Cohort 2.
At Baseline visit, blood sample collection must be taken before administration of the first fingolimod treatment in all patients in Cohort 1.
MRI to be reviewed if performed as part of routine standard of care.
Blood samples (up to 80 mL) will be taken for biomarker and hematology assessments. Hematology assessments include RBC count and morphology, WBC absolute and differential counts (basophils, eosinophils, lymphocytes, monocytes, neutrophils and segmented neutrophils), platelet count, hemoglobin and hematocrit. All specimens collected will be analyzed by a central laboratory.
MRI: magnetic resonance imaging; MS: multiple sclerosis; PDDS: patient determined disease steps; RBC: red blood cell; SDC: study discontinuation completion visit; WBC: white blood cell.
Efficacy assessments
Disability will be assessed using the Patient Determined Disease Steps (PDDS) scale, a patient-reported outcome measure that correlates strongly with Expanded Disability Status Scale scores.16
For patients with MRI data obtained as part of routine standard care, change from baseline in T2 lesion burden and new gadolinium-enhancing T1 lesion counts will be assessed.
Safety monitoring
AEs will be recorded by the treating physician at each visit, and will be followed until resolution or until the event is judged to be permanent. Assessments will be made of any changes in severity, the suspected relationship to the study drug, the interventions required to treat it, and the outcome. Every serious AE (SAE), regardless of causality, occurring after the patient has provided informed consent and until 30 days after the last visit/dose of fingolimod, will be reported to Novartis safety within 24 h of learning of its occurrence. All follow-up information for the SAE will be reported within 24 h of the Investigator receiving the information. After this 30-day period, SAEs with a suspected causal relationship to fingolimod should be reported to Novartis safety. Any SAE experienced during pregnancy and unrelated to the pregnancy will be reported as an SAE to Novartis safety.
Any pregnancy occurring after providing informed consent will be reported to Novartis within 24 h of learning its occurrence. Should a patient become pregnant, physicians will be encouraged to enroll them in the fingolimod pregnancy registry as referenced in the Gilenya prescribing information. 1
Statistical analysis
The population size of 200 patients in Cohort 1 will detect an effect size of 0.30 with 89% power at a significance level of 0.05, after adjusting for multiplicity of testing changes in 15 variables. For both cohorts, effect size will provide estimates within 0.14 of corresponding standard deviation of variables.
Analyses will be conducted by cohort for the full analysis set, which will include all enrolled patients who received at least one dose of fingolimod during the study. Three analyses are planned. The first interim analysis of Cohort 2 will assess safety and will be conducted once 50% of patients (n = 100) have completed the Month 6 visit. A primary analysis of Cohorts 1 and 2 will be performed when all patients have completed the Month 6 visit, and a final analysis of both cohorts will be conducted when all patients have completed the 12-month follow-up visit.
Descriptive statistics (sample size, mean, standard deviation, standard error of mean, minimum, first quartile, median, third quartile, interquartile range, and maximum) will be calculated, with 95% confidence intervals determined for mean values. For the primary outcome (change from baseline to Month 6 in immune cell subtypes), analyses will be performed with respect to the actual value of the primary variables by employing an analysis of covariance (ANCOVA) model, with gender as a factor and duration of disease and corresponding baseline as covariates. The unadjusted as well as the adjusted least squares means will be determined together with a p-value. The percentage change from baseline mean will also be reported.
For secondary outcome measures, correlation coefficients between changes in immune cell subtypes (T cells, B cells, monocytes, neutrophils, NK cells), efficacy (MRI variables and PDDS), and safety outcomes (anti-JCV antibody status and index) will be computed. Descriptive statistics and 95% confidence interval for the mean will be provided for the efficacy assessments. In addition, the association between sNfL levels and relapse, MRI outcomes, and disability progression will be explored.
For safety variables, AEs will be summarized by number and percentage of patients experiencing an AE, system organ class, and each individual AE by cohort and the overall population. Any suspected relationship to fingolimod will be recorded.
Results
The first patient was enrolled on 19 September 2017, with last patient last visit estimated to be 1 July 2019. As of August 2018, 384 patients have been enrolled into the study; 167 to Cohort 1 and 217 to Cohort 2. Seventy-eight sites have been activated.
Upon study completion and finalization of the report, the study results will be submitted for publication and/or posted in a publicly available clinical trials database.
Discussion
FLUENT is a comprehensive immune-profiling study in patients with RMS treated with fingolimod in a real-world setting. This investigation will expand upon the previous biobank studies to provide longitudinal data on cellular changes in the innate and adaptive immune cell populations in fingolimod-treatment naïve patients, as well as those who have been on continuous treatment for at least 2 years.
Previous investigations into the effects of fingolimod treatment on phenotypic changes in T and B cell subsets in patients with MS have demonstrated reductions in CD4+ and CD8+ T cell counts by approximately 80% and 60%, respectively, compared with control subjects. 3 Blumenfeld et al. examined changes in lymphocyte subsets over 3 months following initiation of fingolimod therapy, and observed significant reductions in the percentages of peripheral CD3+CD4+ T cells and CD19+ B cells compared with baseline, and an increase in the proportion of CD14+ monocytes.17 Fingolimod exposure was also found to reduce the percentage of memory B cells and increase the proportions of naïve B cells as well as regulatory B cell subsets, within total CD19+ B cells. Similar observations were reported following a study to examine immune cell subtypes over the course of 12 months. Percentages of CD4+ T cells CD19+ B cells decreased 1 month after treatment with fingolimod before reaching steady-state proportions at 3 months.18
In addition to compositional changes in the phenotypes of immune cell subsets, differential expression of functional molecules relating to cytokine production, migration and immunosurveillance, and antigen-presenting activity, including T cell activation and T helper subset differentiation, have been associated with S1P1 signaling and fingolimod exposure.17-24
Changes in immune cell subsets during treatment with fingolimod may be associated with its therapeutic efficacy. Alterations in T cell phenotypes might be related to relapse during fingolimod treatment.25 null The percentages of central memory CD4+ T cells in peripheral blood samples collected from a small cohort of patients with RRMS correlated with occurrence of relapse within the first year of fingolimod treatment. 25 Patients determined to have stable disease, defined by clinical and MRI criteria, following treatment with fingolimod for ≥ 12 months were found to have significantly higher proportions of peripheral regulatory B cells than those with active disease,19 suggesting that determination of the proportions of these cells in patients might be a method to evaluate efficacy of fingolimod therapy.
The FLUENT study will expand upon these previous investigations and will also assess immune cell subtypes in relation to safety outcomes, particularly infections, including PML. The association between cell subtypes and clinical outcomes will also be investigated. The inclusion of sNfL levels as an exploratory endpoint allows investigation of this promising biomarker for its association with disease activity and response to therapy. Elevated levels of sNfL have been associated with lesions on MRI, relapses and disability progression in patients with MS, as well as increased risk of future relapses and disease worsening as measured by the Expanded Disability Status Scale score. 6 The FLUENT study will assess the association over time between sNfL levels and relapse, MRI based variables, and disability progression.
FLUENT may provide evidence for the use of immunologic profiling in predicting efficacy and risk of infection in patients with RMS treated with fingolimod.
Footnotes
Acknowledgements
The PDDS is provided for use by the NARCOMS Registry (![]() ). NARCOMS is supported in part by the Consortium of Multiple Sclerosis Centers (CMSC) and the CMSC Foundation. The authors acknowledge Marina Ziehn, PhD, of Novartis Pharmaceuticals Corporation, who reviewed the article during the early stages of development; and Philip Chapman of Indicia Medical Ltd, a member of the Fishawack Group of Companies, Abingdon, UK, who provided editorial and medical writing support, which was funded by Novartis Pharmaceuticals Corporation.
). NARCOMS is supported in part by the Consortium of Multiple Sclerosis Centers (CMSC) and the CMSC Foundation. The authors acknowledge Marina Ziehn, PhD, of Novartis Pharmaceuticals Corporation, who reviewed the article during the early stages of development; and Philip Chapman of Indicia Medical Ltd, a member of the Fishawack Group of Companies, Abingdon, UK, who provided editorial and medical writing support, which was funded by Novartis Pharmaceuticals Corporation.
Conflict of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JAC reports personal compensation for consulting for Adamas, Convelo, EMD Serono, Novartis, and Pendopharm, speaking for Mylan, and serving as a Co-Editor of Multiple Sclerosis Journal – Experimental, Translational and Clinical.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The FLUENT study is funded by Novartis Pharmaceuticals Corporation, East Hanover, NJ, United States. Editorial and medical writing support of the manuscript and the journal’s article processing charges were funded by Novartis Pharmaceuticals Corporation.