
Abstract
Background
Children with congenital heart disease (CHD) require long-term home care. Mobile health apps offer a new approach for home care support, but they face challenges of low user engagement and insufficient sustained usage rates.
Purpose
Identify and analyze the essential functional features of mobile health apps supporting home care for children with CHD; examine their design strategies based on the Persuasive System Design (PSD) model.
Methods
Based on the framework of Arksey and O'Malley’s scoping review and the PRISMA-ScR guidelines, a systematic search was conducted in major domestic and international databases. The search scope encompassed studies published between 2010 and 2026 concerning mHealth apps supporting home care for children with CHD. The app design features were coded based on the 28 principles of the PSD model.
Results
A total of 22 studies were included. Patient–provider communication and Health education delivery were the most common functions, followed by Physiological data monitoring. Motivational incentive mechanisms were severely underdeveloped. The credibility and reduction principle were widely employed. The social support pillar was the most underutilized. Motivational principles were entirely absent. The rewards principle was implemented in only 6.7% of the apps.
Conclusion
Apps for CHD family care performed adequately in information delivery and credibility support but showed significant deficiencies in motivational incentives, social support, and emotional connection. Theories from behavioral science should guide the development of future apps. All PSD pillars should be used in a balanced way, and the principles of dialog support and social support should be strengthened, enhancing parental engagement and long-term use.
Keywords
1. Introduction
Congenital Heart Disease (CHD) refers to structural or functional defects of the heart caused by abnormal development of the heart and major blood vessels during the embryonic period, and it represents the most common type of congenital malformation in children. 1 The rising survival rate of CHD signifies that a growing number of children with CHD require long-term, even lifelong, medical management and family care. Traditional hospital-based follow-up models are limited by infrequent sessions, geographical and time constraints, and high costs, making it difficult to meet families’ continuous needs for information, guidance, and support in daily care. 2 The rapid development of mobile health (mHealth) presents new opportunities for improving chronic disease management and family care, with mobile health applications (apps) being a form of this technology that is convenient, low-cost, and highly accessible. The cardiac rehabilitation management for children after CHD surgery requires sustained health monitoring and consistent patient-provider communication, areas where mobile health apps demonstrate their unique advantages. 3 Mobile health apps for CHD family care vary considerably in their functional design, technical implementation, and application outcomes, offering diverse solutions to support the home care of children with CHD. However, despite the promising prospects of mHealth technology, a core challenge lies in user adherence, which encompasses both the depth of engagement with app features and the long-term retention of users. It indicated that health apps generally exhibit low user retention rates, with a majority of users discontinuing use shortly after download. 4 Parents of children with CHD often face practical challenges including time constraints, limited energy, and significant psychological stress while managing complex care tasks.5,6 Since sustained adherence is a prerequisite for apps to deliver effective support, their intended supportive value cannot be realized without successfully attracting and maintaining parental engagement.
PSD framework elements.
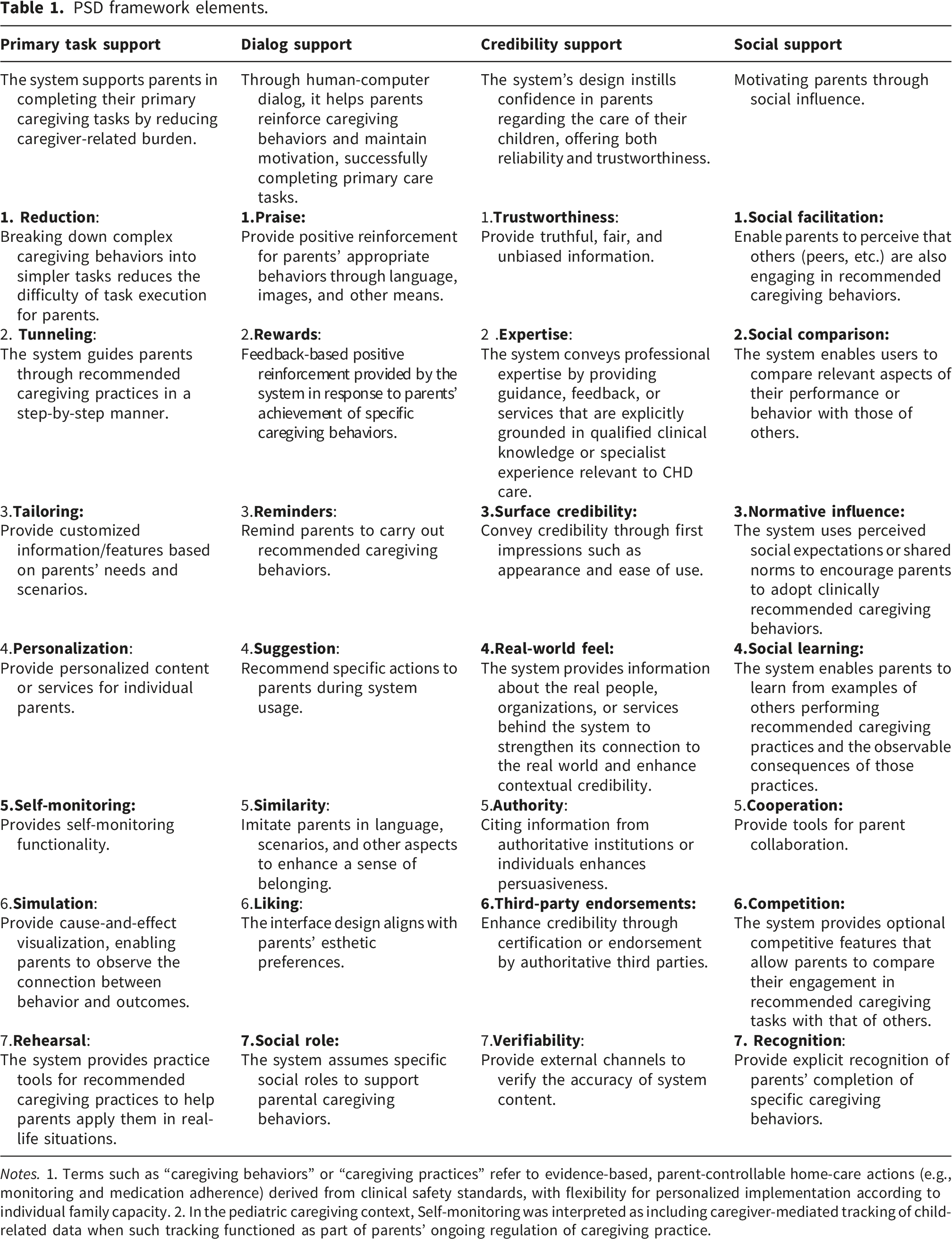
Notes. 1. Terms such as “caregiving behaviors” or “caregiving practices” refer to evidence-based, parent-controllable home-care actions (e.g., monitoring and medication adherence) derived from clinical safety standards, with flexibility for personalized implementation according to individual family capacity. 2. In the pediatric caregiving context, Self-monitoring was interpreted as including caregiver-mediated tracking of child-related data when such tracking functioned as part of parents’ ongoing regulation of caregiving practice.
Existing research focuses on the development or evaluation of individual CHD family care apps, lacking a comprehensive understanding of the overall landscape of apps in this field. Studies often treat apps as a “black box,” concentrating on outcome changes pre- and post-intervention, but fail to thoroughly examine the “black box” interior, the apps’ functional and design features. Although the PSD model has been applied in adult chronic disease management apps, its application in pediatric contexts, where parents act as primary caregivers for medically fragile children with complex needs, remains scarce. This scoping review aims to identify and analyze mobile health apps designed to support family care for children with CHD, with a focus on their functional features and design strategies based on the PSD theory, to explore how optimized design can improve usage rates and engagement among parents of children with CHD. In doing so, it fills a key gap in the application of persuasive technologies to CHD family care by clarifying how PSD principles are translated into concrete system features and synthesizing them into actionable, theory-informed design recommendations to tackle persistent problems of user attrition and poor adherence and to support the development of more sustainable digital tools for home care of children with CHD.
2. Methods
2.1. Design and reporting guidelines
This study followed the scope review framework of Arksey and O'Malley 11 and was reported according to the PRISMA-ScR 12 guidelines. As this review aimed to rapidly synthesize existing evidence on the topic, registration of the protocol in PROSPERO was not required.
2.1.1. Defining research questions
The following research questions guide this review: (1) What are the functional characteristics of apps designed to support home care for children with CHD? (2) Based on the PSD framework, what design strategies do these apps employ? (3) What are the shortcomings of existing app designs, and what potential for optimization exists?
2.1.2. Literature search and retrieval
We conducted a comprehensive literature search. The following databases were systematically searched: China National Knowledge Infrastructure (CNKI), Wanfang Data, China Science and Technology Journal Database (VIP), PubMed, Web of Science, Embase, Cochrane Library, Scopus, and CINAHL. The search period lasted from 2010 to March 4, 2026. Literature retrieval was restricted to studies published in 2010 or later, as the PSD framework was proposed in 2009. A combination of controlled vocabulary and free-text terms was employed to ensure comprehensive retrieval. Search terms included congenital heart defect/congenital heart disease/complex congenital heart disease/congenital heart malformation; telemedicine/ehealth/mhealth/telehealth/smartphone/mobile health/electronic health/digital health/tablet computer/iPad/iphone/mobile application/app/mobile platform/digital intervention/mobile app/telerehabilitation/smartphone app/health app. Detailed search strategies, using PubMed as an example, are provided in the Appendix. To identify further relevant studies, we reviewed the reference lists of all included studies, examined relevant review studies to identify their original research, and tracked study protocols for their full results.
2.1.3. Study selection
Inclusion Criteria Based on Population, Concept, and Context Principles: 1. Population (P): Studies involving parents or primary caregivers of children with CHD aged 0–6 years were eligible. This review focused on early childhood because this period encompasses the peak stage of surgical treatment, intensive home monitoring, and high caregiving dependency.13,14 Studies involving child–parent dyads were also considered when the intervention was designed to support home care primarily through caregiver use. 2. Concept (C): Eligible studies described mobile health interventions for children with CHD or their parents that were delivered through a user-facing software interface accessible on mobile devices, such as mobile apps or app-like interactive platforms. Interventions were included when they supported interactive digital functions for home-care support. 3. Context (C): This review focuses on the home-care support environment, encompassing interventions initiated during the transition from hospital to home or provided entirely in a home-based setting. Studies were included if they described the characteristics, implementation, feasibility, use, or outcomes of eligible mobile health interventions. This study is limited to peer-reviewed original journal articles, papers, and theses published in Chinese or English.
Exclusion criteria and rationale.

2.1.4. Literature screening and data extraction
A comprehensive literature search was conducted to ensure no potentially eligible studies were overlooked. Reference lists of relevant systematic reviews and scoping reviews were also screened. All retrieved studies were imported into Zotero 7.0, and duplicate studies were removed. Two researchers independently reviewed the titles and abstracts of retrieved papers, resolving disagreements by consulting a third researcher. Full-text screening was then conducted based on predefined inclusion and exclusion criteria, with the final study collection confirmed through cross-checking.Data were systematically extracted and organized using a pre-designed table, including author, country of publication, study type, research objective, app name, study population, sample size, research content, intervention duration, and design participants. During data extraction, we relied solely on information available in published literature. The basis for data extraction was the app itself, not the individual studies. This means that for certain apps, data were drawn from multiple published articles.
2.1.5. Data analysis
Data analysis was conducted in three stages: descriptive summarisation, qualitative coding, and integrative interpretation. First, descriptive numerical summaries were used to synthesise the basic characteristics of the included studies extracted in Section 2.1.4. All extracted data were recorded in a predesigned Microsoft Excel spreadsheet. Second, a mixed analytic approach was used, combining inductive thematic development of app functions with deductive coding of design features based on the PSD model. Functional descriptions were analysed inductively through open coding, followed by comparison and grouping of codes with semantic or logical similarity into broader categories. Through iterative reading and constant comparison across apps, overarching functional categories relevant to CHD family care support were developed from the data. To enhance rigour, functional coding involved independent reading, preliminary coding, comparison of codes, and discussion between the first and second authors until agreement was reached.
Design features were analysed deductively using the 28 PSD principles as a predefined coding framework. Two reviewers independently examined the full-text descriptions of each app and coded a PSD principle only when explicit textual evidence supported its presence. Consistent with established PSD methodology, our coding focused exclusively on system features rather than the content of human-delivered messages mediated by the platform. For instance, system-triggered praise (automated messages generated by the app’s logic following task completion) was coded as a persuasive feature. In contrast, praise delivered manually by healthcare professionals through a chat was excluded, as it reflects the quality of clinical service rather than the inherent design of the persuasive system. Each PSD principle was coded dichotomously as present or absent, regardless of whether the original study explicitly described it as a persuasive design component.
Operational definitions and decision rules for both functional categorisation and PSD coding were discussed before formal analysis. Data extraction and coding were completed independently by the first and second authors and verified by the third author. Disagreements were resolved through re-examination of the original papers and discussion until consensus was reached. Inter-rater reliability for the deductive PSD coding, assessed using Cohen’s kappa, was 0.90, indicating good agreement.
The quantitative and qualitative findings were integrated at the apps level to address the review questions. The inductively derived functional categories were used to describe what kinds of support current CHD family-care apps provide, while the deductive PSD coding was used to examine how those functions were designed and delivered. Frequencies of functional categories and PSD principles were then summarised and interpreted alongside the thematic findings to characterise both the functional profile and the design orientation of current apps. This analysis was based on the researchers’ assessment of the alignment between the literature’s descriptive content and PSD principles, a methodology widely adopted in prior studies applying PSD analysis to existing systems.15–17
3. Results
3.1. Research selection
The initial search retrieved a total of 3156 studies. Two researchers screened the remaining 1253 titles and abstracts using the Zotero software program to determine eligibility after removing 1903 duplicate documents. After removing 1183 ineligible documents through title/abstract review, the first and second authors reviewed the remaining 70 full-text documents. Until they reached a consensus, both authors discussed discrepancies and disagreements. When consensus could not be achieved, the third author’s opinion was sought. A total of 17 documents were retained. By tracing the references of the aforementioned documents, 5 additional studies meeting the inclusion criteria were identified, resulting in 22 documents ultimately included for subsequent analysis (Figure 1). PRISMA flowchart for study selection and assessment.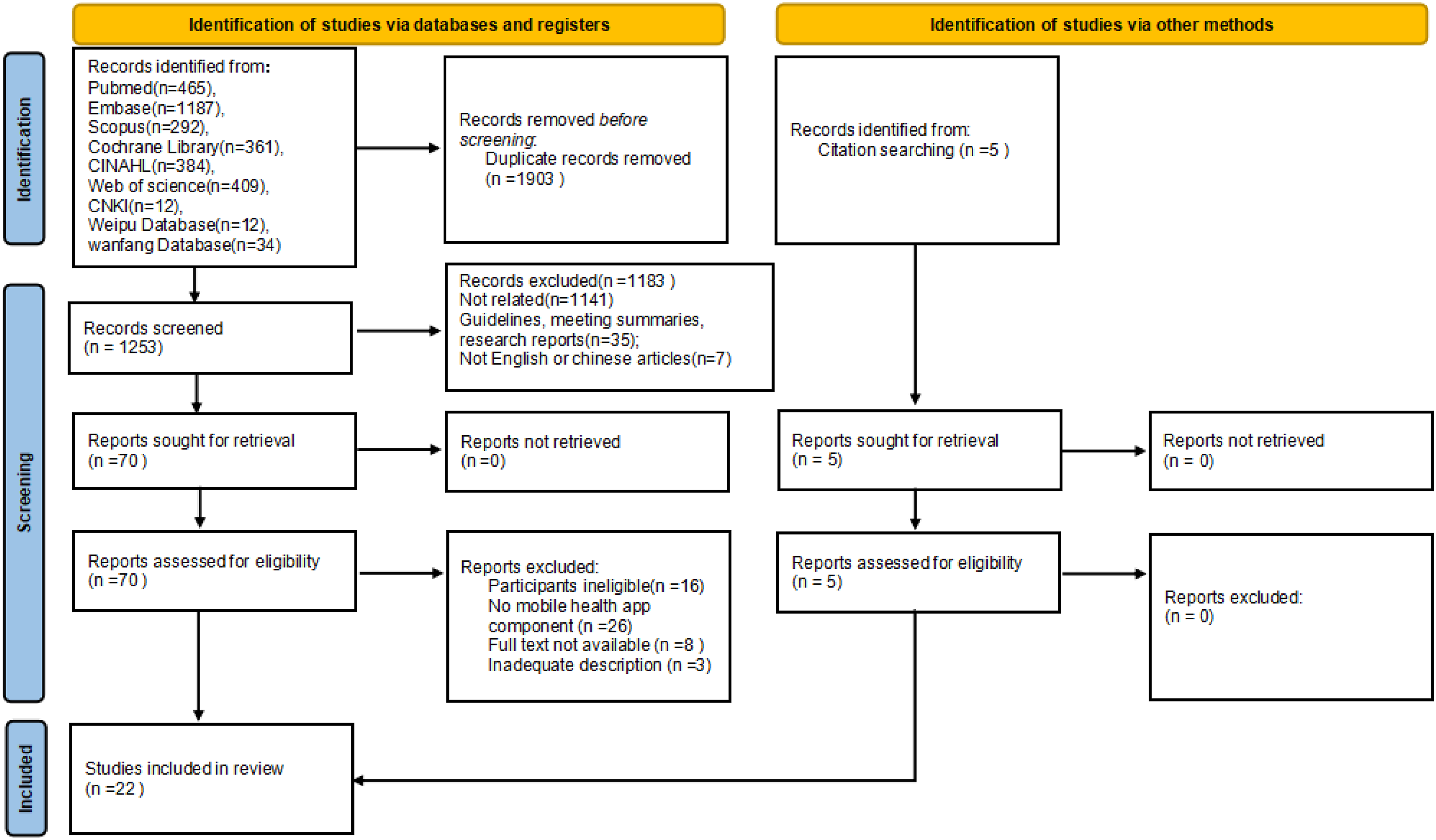
3.2. Included studies overview
This review included 22 studies18–39 either unnamed or not explicitly identified. The geographic distribution of included studies was as follows: United States (n = 12),21,23,25–34 China (n = 5),18,36–39 Norway (n = 2),19,22 Colombia (n = 2),24,35 and Iran (n = 1)20. Quantitative studies (n=16; 72.7%) were the most prevalent, including RCTs (n=6),20,28,30,36,38,39 non-randomized controlled trials (n=2),18,19 feasibility studies (n=4),21,25,29,35 and retrospective study (n=3).26,31,33 The sample also comprised qualitative studies (n=2)23,24 and mixed-methods studies (n=5) 22,27,32,34,37 sample sizes of the included studies varied considerably, ranging from 10 to 130 participants, with a total of 1323 enrolled. Parents used the apps for periods ranging from 4 weeks to 6 months. Only 6 apps or studies18,23,25,30,34,39 explicitly stated that they were designed and developed based on theory. Most of studies involved multidisciplinary team collaborations, but only 7 apps19–23,25,31 included parents or family members of the children in their design process (Supplementary File S1).
3.3. Functional composition and distribution of the apps
The mobile health apps or mobile health programs described in the included studies encompassed 12 functional categories. Each app contained between 1 and 9 functions, with an average of approximately 6 functions per app. The frequency of occurrence for these 12 functional categories varied significantly across the 15 included apps (Supplementary File S2). For analytical purposes, this study categorized functions into three tiers based on frequency: high-frequency functions (≥60%), medium-frequency functions (40–59%), and low-frequency functions (<40%) (Figure 2). Prevalence of features in mobile applications for family caregivers of children with CHD.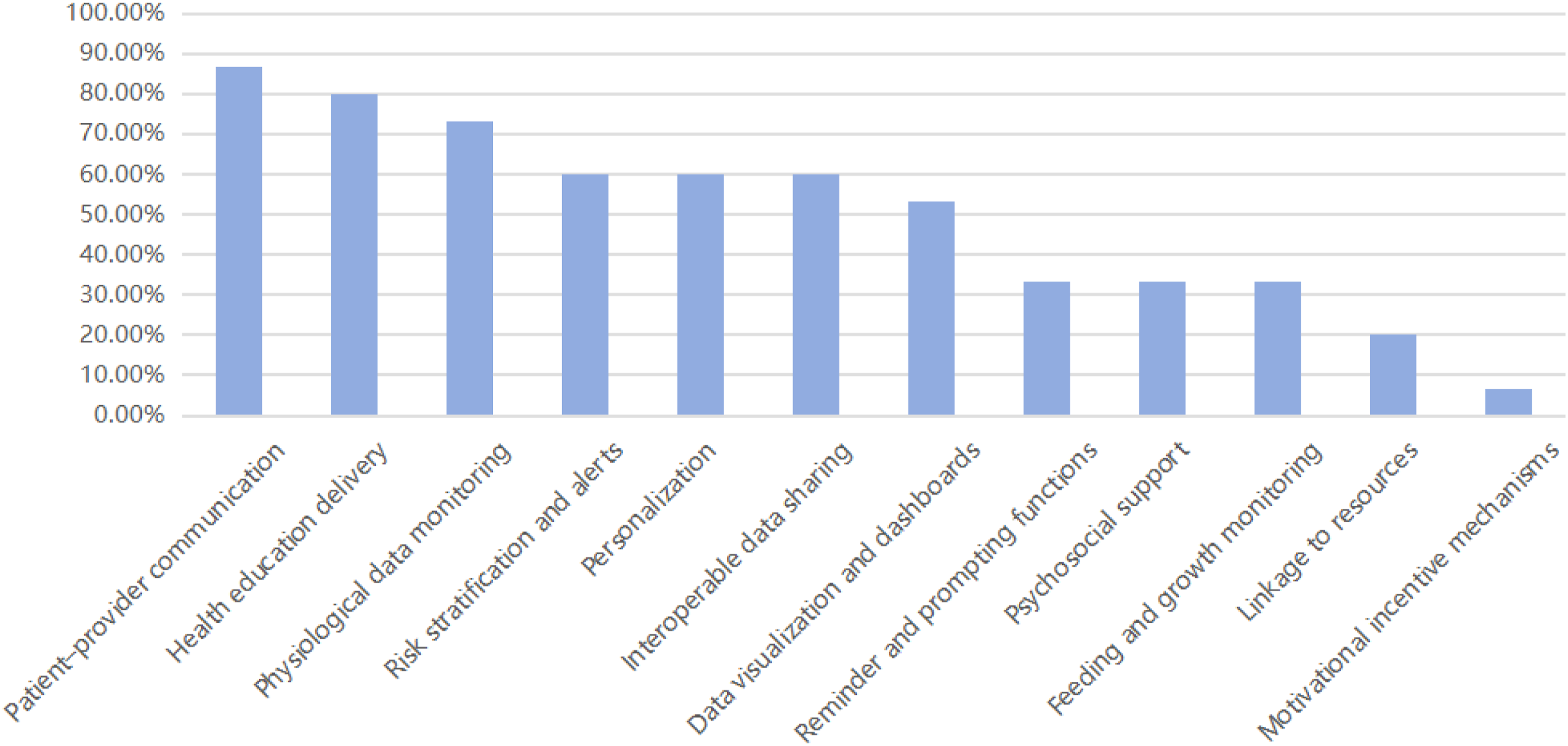
Patient–provider communication18,19,21–24,26–39 was the most commonly implemented feature, appearing in 13 apps and projects (86.7%), while health education delivery18–22,24,25,27,30–39 was also highly prevalent, appearing in 12 (80%). Physiological data monitoring19,21–29,31–33,35,36,39 is the third most frequent feature, implemented in 11 apps (73.3%),serving as a foundational tool for home care. It enables parents to track their child’s health status and provides a data foundation for doctor-patient communication and assessment alerts. Patient–provider communication features include text chat, video consultations, and photo or video sharing. Health education delivery utilizes video, text, and images to cover topics such as CHD diagnosis knowledge, postoperative care, feeding guidance, symptom recognition, follow-up management, medication guidance, and psychological adjustment. The physiological data monitoring function reports parameters including body weight, blood oxygen saturation, heart rate, food intake, excretion volume, and oxygen flow rate. Risk stratification and alerts,21,23,24,27–29,31–33,35–39 personalization,18,19,22,26–30,32,34,36–39 interoperable data sharing23,24,27–30,32–39 and data visualization and dashboards19,21–24,26–29,31,32,35,37,38 appear with moderate frequency as an auxiliary tool for family care management. Most apps achieve risk stratification and alerts through structured symptom checklist evaluation and automated threshold triggering. Most apps achieve risk stratification and alerts through structured symptom checklist evaluation and automated threshold triggering. Personalization is achieved by tailoring content to match diagnoses, establishing personalized thresholds, and setting individual baseline parameters. Interoperable data sharing encompasses real-time assessment by medical teams, electronic medical records accessible to medical teams, and sharing with family members. Data visualization and dashboards feature chart types such as trend graphs, statistical charts, and visual assessment scales. Reminder and prompting functions21,23,24,30,31,34,35,37,38, psychosocial support18,24,25,30,34,35,39, linkage to resources,21,22,25,31 feeding and growth monitoring21,24,26,31,35,37–39 and motivational incentive mechanisms21,31 are low-frequency functions. Reminder and prompting functions include data entry reminders, medication reminders, and follow-up appointment reminders. Psychosocial support is delivered through peer support and assistance in managing negative emotions. The linkage to resources function connects to external websites, aggregates healthcare provider access methods, and provides assistance channels. Feeding and growth monitoring provides specialized feeding behavior tracking and real-time adjustment of feeding plans. Only one app21,31 describe the implementation of motivational incentive mechanisms to enhance user compliance and engagement.
3.4. Mapping of mobile health app design features to PSD principles
This study evaluated the application of 28 design principles from the PSD model across 15 apps (Supplementary File S3). The results show varying degrees of reflection for all four pillars, but there were significant differences in the depth and breadth of their implementation (Figure 3). Distribution of PSD support categories across the included mobile applications.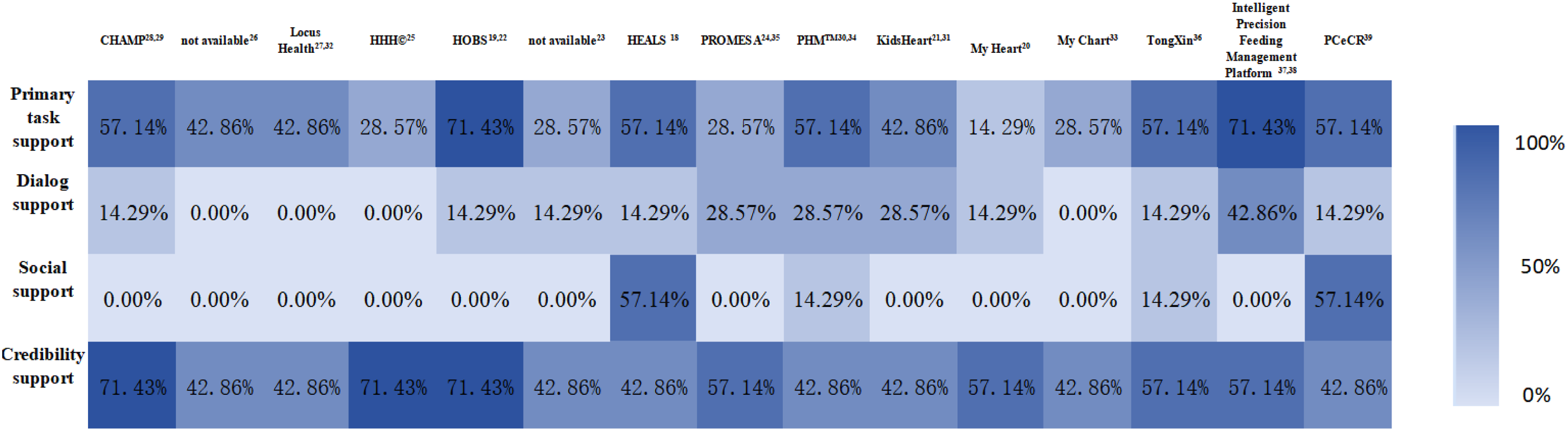
3.4.1. Application status of the four pillars
The credibility support principle had the highest adoption rate, with all apps implementing at least some principles within this pillar, achieving 100% app coverage. The adoption rates for principles under primary task support were 71.4%. The adoption rates for principles under dialog support and social support were comparable (both 57.1%). In contrast, dialog support features were implemented in 73.3% of apps, whereas social support features were implemented in only 26.7%. All apps integrate multiple PSD principles, with none relying solely on a single pillar. The 15 apps incorporate between 5 and 12 PSD principles, averaging 9 principles per app.
3.4.2. Application frequency and characteristics of each PSD principle
3.4.3. Analysis of PSD principle balance
The credibility support principles achieved 100% application, with all seven principles being implemented. The three core principles, trustworthiness (100%), expertise (100%), and real-world feel (100%) were extensively implemented, indicating that all apps prioritized establishing a foundation of trust. The primary task support principles achieved a 71.4% implementation rate, with five of them being applied. Reduction (100%) and self-monitoring (80%) served as the core components. However, simulation and rehearsal were completely absent. While the apps performed well in lowering usage barriers, they lacked support for advanced learning. The dialog support principles achieved a 57.1% implementation rate. It exhibited significant internal variation. Suggestions (40%) and reminders (33.3%) were relatively well applied, whereas rewards, praise and social role were severely underutilized. The social support principles had a 57.1% implementation rate. The three core motivational principles, social comparison, competition and recognition, were entirely absent, largely overlooking group dynamics and peer support.
4. Discussion
This review systematically summarizes the current application status of mobile health apps in supporting home care for children with CHD. It analyzes the characteristics of 15 apps from functional configuration and PSD design strategies, revealing the developmental trends and potential challenges in this field. Research indicates that while mobile health technologies show promising potential in home care for children with CHD, significant room for improvement remains in areas such as design philosophy and user engagement strategies.
4.1. App feature configuration
This study found that existing apps supporting CHD family care perform well in information access and care coordination. Patient-provider communication and health education delivery were the most widely implemented functions, with risk stratification and alerts and physiological data monitoring also demonstrating high coverage. These functions partially alleviate the temporal and spatial constraints inherent in traditional follow-up models. They help enhance information accessibility, strengthen care continuity, and provide parents with an “always-accessible professional support channel.” This finding aligns with previous studies 40 where parents commonly reported information gaps and an ongoing need for professional guidance, indicating that the apps have, to some extent, addressed the core care needs of families with CHD.
However, this study also found that motivational incentive mechanisms were implemented in only a few apps, representing the functional category with the lowest adoption rate. Many apps primarily remain in a passive management mode of providing information and reminders, paying insufficient attention to enhancing proactive parental engagement through methods like goal setting, progress tracking, and reward feedback. The absence of incentive mechanisms reflects a misunderstanding among developers regarding the nature of “user engagement,” as many seem to assume that parents will spontaneously and consistently use an app simply because it provides sufficiently comprehensive and accurate information. Consequently, most apps function at the level of “information providers” rather than “behavior facilitators. Substantial evidence indicates that merely providing information and tools does not necessarily lead to behavioral change or sustained engagement.41–43 Technology adoption and sustained use are two distinct processes. 44 Initial adoption may rely on users’ perceived usefulness and ease of use, but long-term engagement requires systematic motivational maintenance. 45 From the theoretical perspective of behavioral persistence, Deci and Ryan’s Self-Determination Theory 46 distinguishes between extrinsic motivation (acting for external outcomes) and intrinsic motivation (where the action itself is satisfying).The initial motivation for parents of children with CHD to utilize mHealth apps stems from a complex interplay of intrinsic and extrinsic factors. Although the child’s medical condition acts as an external trigger, parental commitment to the child’s well-being represents a highly internalized form of motivation. This state is conceptualized as “identified regulation” within Self-Determination Theory, a process through which individuals recognize and consciously accept the personal importance of a specific behavior. However, even with strong internal commitment, parents face significant practical constraints like time pressure and psychological stress. Without immediate positive feedback or a sense of “small wins,” the intense caregiving tasks can feel like an external burden, potentially leading to burnout and diminished engagement over time. Incentive mechanisms, such as rewards and praise, serve to help parents experience a sense of accomplishment, recognition, and control during app use. It enhances their intrinsic motivation, thereby promoting sustained use behavior through the synergy of strengthened intrinsic and extrinsic motivation. 47 Previous research suggests that digital interventions incorporating motivational elements often demonstrate superior effectiveness in improving usage frequency, adherence rates, and behavior change.48–52 Therefore, the incentive mechanism gap identified in this study, while not simplistically viewed as the direct cause of user attrition, undoubtedly highlights a priority area for optimization in future design.
Furthermore, the functional distribution reveals another significant phenomenon: general-purpose functions, such as patient-provider communication, health education delivery,and physiological data monitoring, dominate the landscape, while more targeted care functions like feeding and growth monitoring are less frequently implemented. Feeding difficulties and malnutrition are significant concerns in the prognosis management of infants and young children with CHD. Monitoring and feedback during the feeding process help improve the nutritional status and growth outcomes of pediatric patients. 53 The app 26 included in this study, which incorporated feeding and growth monitoring, reported improvements in weight-for-age z-scores. This suggests that beyond general functions, developing deeply tailored functions addressing key care challenges may hold greater potential for enhancing both the prognosis of children with CHD and their families’ care experience.
4.2. Application characteristics of the PSD principle
Analysis based on the PSD framework revealed that credibility support principles were applied to all included apps (100%), with trustworthiness (100%) and expertise (100%) approaching universal adoption. This indicates that developers place high importance on the professionalism, reliability, and safety of healthcare apps, which forms the essential foundation for trust and adoption by parents of children with CHD. 54 The reduction principle under primary task support was widely adopted (100%). Simplifying complex care tasks through technological design is crucial for ensuring initial adoption by parents and integration into daily routines. 55 The frequent application of the self-monitoring principle (80%) is primarily operationalized through physiological data monitoring, which serves as a proxy-monitoring mechanism in this pediatric context. This underscores the central role of technology-driven feedback in facilitating caregivers’ management of their home-based care tasks.
The partial absence of dialog support is particularly noteworthy. Although 40% of apps provided suggestions and 33.3% offered reminders, only 6.7% incorporated rewards, and none delivered praise feedback, indicating a lack of dynamic interaction based on parental behavior, emotional state, or phased care goals. This means parents primarily receive rule-based, one-way information pushes rather than a continuous interactive experience of being seen and accompanied. Caregiving is both emotionally and mentally taxing, and the additional strain of feeling unappreciated may exacerbate mental health issues.56,57 Parents of children after CHD surgery endure significant psychological stress, and the lack of recognition and encouragement may exacerbate their caregiving fatigue. 58 Recognizing and appreciating parents can serve as a powerful source of motivation, particularly when they face caregiving responsibilities and challenges. 59 However, current family care app designs for CHD have failed to address this emotional need adequately.
The marked underutilization of social support principles represents one of the most significant findings of this study. The social support pillar was addressed by only 26.7% of the apps,18,30,34,36,39 with a mere 20% offering limited forms of peer communication or experience sharing through social learning; principles of social comparison, competition, and recognition were entirely absent. This finding aligns with research on mobile health interventions for adults with coronary heart disease. 16 Furthermore, Villinger et al. 60 found that apps designed to support cancer patients also lacked emotional social support and informal support from peers.The intense and prolonged nature of caregiving often prevents parents/caregivers of children with CHD from engaging in normal social interactions, which can lead to feelings of loneliness and isolation over time.61,62 In the field of chronic disease management, peer support has been demonstrated to significantly reduce caregiver burden, enhance treatment adherence, and improve mental health outcomes.63–65 However, this study found that only a small subset of apps applied any principles from the social support pillar, and these were mostly confined to vertical parent-provider interactions, with peer-to-peer interaction among parents being almost entirely absent. From a practical perspective, the absence of social support may largely reflect developers’ practical concerns. Children’s health data is highly sensitive, and social features could increase the risk of data breaches.Furthermore, the low utilization of social support features may be related to their potential to trigger strong negative emotions and emotional backlash.66,67 For instance, given the wide variation in CHD severity, social comparison might induce parental anxiety and self-blame rooted in perceptions that “my child is not as good as others.” Additionally, features like parent communities require content moderation, conflict mediation, and misinformation correction, which entail significant human resource costs. 68 However, these concerns are not insurmountable, and appropriate design is crucial. When comparisons focus on effort level, task completion, or behavioral adherence rather than behavioral outcomes, they can be motivating rather than discouraging.69,70 A social comparison approach focusing on caregiving behaviors rather than child health outcomes, comparing parent-controlled actions like “monitoring frequency” or “courses completed” rather than uncontrollable physiological indicators like “weight gain” or “oxygen saturation levels”, can mitigate most ethical risks. Furthermore, future research should promote the development of ethical frameworks for mHealth apps, explore new privacy-preserving technologies, and establish dynamic regulatory frameworks that can keep pace with rapid innovation, effectively managing risks through technical and administrative measures such as anonymization, optional participation, and professional moderation. 71
4.3. From “tools” to “care partners”
The findings indicate that most CHD family care apps are primarily designed as information and task management tools, rather than as “partnership-based” support systems that actively engage in the care process. Virtually none of the apps included in the study explicitly adopted the social role principle; human-computer interactions were predominantly functional operations, lacking personified, empathetic communication or contextualized engagement. From the perspective of the care experience, the challenges faced by CHD families extend beyond information gaps and management complexity to include emotional distress from prolonged uncertainty, role-related stress, and adjustments in family dynamics.61,62 This study identified a notable neglect of these emotional dimensions, as only 33.3% of the apps incorporated psychosocial support features. Parental mental health is not merely a personal issue but a fundamental determinant of the child’s clinical outcomes. 72 Standardized care is unlikely to meet the diverse needs of families, and parents have expressed a desire for tailored mental health support. 73 Relying solely on “task lists and reminders” is inadequate to address these deeper psychosocial needs. Moderate anthropomorphic design, a warm communication style, and emotionally sensitive support during key milestones (e.g., pre-/post-surgery, follow-ups) can enhance users’ emotional connection to the digital intervention and their willingness for sustained engagement.74,75
Based on our findings, the following design implications are proposed: while ensuring information accuracy and security, appropriately incorporate emotional support elements, such as sending caring messages at key milestones and providing positive reinforcement for parents’ consistent recording and caregiving efforts. Introduce structured peer support modules, such as professionally moderated parent discussion forums and experience-sharing storybanks. Design context-aware “micro-pathways” for critical CHD care scenarios (e.g., feeding management, post-operative recovery) to assist parents in making step-by-step decisions in complex situations. These design strategies can help transition apps from mere information carriers into more interactive and companion-like care partners.The transition from “tools” to “partners” is being catalyzed by generative artificial intelligence (AI). 76 Recent studies show that large language models can achieve, and in some dimensions exceed, physicians in perceived empathy in medical contexts, with generated responses demonstrating clear advantages in emotional validation and supportive communication.77,78 Generative AI-based systems can move beyond static, template-driven scripts to provide real-time, context-sensitive, and human-like emotional validation tailored to parents’ affective states, thereby fulfilling the “social role” emphasized in this study. 79 In addition, AI agents are evolving from simple prompt-driven tools into autonomous entities capable of processing complex clinical narratives and offering personalized recommendations.In line with the “micro-pathway” decision support proposed in this study, AI agents are increasingly used in perioperative rehabilitation management, where they can reason over real-time health data to anticipate complication risks and guide families through stepwise care pathways. 80 Thus, integrating the deep conversational capabilities of LLMs with the proactive coordination mechanisms of AI agents into CHD family-care apps could operationalize the PSD principles of “dialogue support” and “social role” with genuine interactional depth and, through companion-like intelligent collaboration, help alleviate parents’ caregiving burden and enhance long-term adherence.
It is important to note that excessive anthropomorphism may induce an “uncanny valley” effect or foster unrealistic expectations of the system’s capabilities. 81 Therefore, we recommend designing apps as “complementary partners”: on the one hand, encouraging a sense of community through appropriate emotional expression, personalized feedback, and responsiveness to care rhythms; on the other hand, clearly defining their boundaries, ensuring they are perceived as a “supplement” to professional care teams and family support networks in any context. Furthermore, the foundation of this “partnership” rests upon trust. A systematic review highlights that perceived data privacy and security are decisive factors for the sustained use of mHealth apps. 82 Consequently, the design of a “complementary partner” must include transparent data management and robust privacy protocols, establishing clear boundaries of information access to transition these apps from mere monitoring tools into reliable care partners.
4.4. Implications for practice
Among existing apps for CHD family care, only a minority were explicitly guided by theoretical frameworks during design and development, with systematic reporting of their application process being limited. In paediatric family care, the value of theory lies not simply in strengthening parents’ willingness to provide care, but in identifying the barriers that prevent caregiving intentions from being translated into sustained behaviours, thereby informing more targeted intervention design. 83 In practice, this means translating theoretical constructs into clinically meaningful functions. For example, a parent empowerment perspective may inform stepwise assessment and decision-support features for postoperative warning signs and home management uncertainty, thereby enhancing parents’ participation in care-related decision-making. 84 Similarly, the Family Management Style Framework may guide the development of family-sharing and information-synchronisation functions by drawing attention to how family members understand the child’s condition, organise management tasks, and integrate care into everyday family life. 85
Future CHD family-care apps may also benefit from a more balanced use of PSD principles. While many existing apps are already strong in task support and system credibility, dialogue support and social support remain relatively underdeveloped. Dialogue support should move beyond reminders or superficial rewards and provide clinically meaningful feedback embedded in daily care tasks. For instance, when parents consistently complete demanding monitoring activities, the app could provide explanatory feedback on the value of those records for postoperative assessment, rather than relying solely on symbolic rewards. Social support features should also be developed cautiously and in ways that reflect the realities of postoperative family care. Parent experience-sharing and peer exchange may be valuable, but these features require professional moderation, content screening, and appropriate risk communication to reduce misinformation and unhelpful comparison.
Although most apps were described as family- or parent-centred, relatively few studies involved families directly in the co-design process. Future development may therefore benefit from experience-based co-design approaches that engage parents early in needs identification and solution development. 86 Evaluation should also extend beyond short-term engagement or usability outcomes to include clinically meaningful and family-relevant endpoints.
4.5. Limitations
This study has several limitations that should be considered when interpreting the results. First, the coding of PSD principles was based on the researchers’ judgment in matching app functions and design descriptions found in the literature, rather than on developers’ explicit statements of design intent. Some included studies provided only general descriptions of app structure and interface. To maintain coding consistency, a PSD principle was only recorded as “applied” if it was explicitly described in the literature. While this strategy reduced subjective speculation, it may have introduced information reporting bias, whereby some designs actually present in the apps were underreported and thus misclassified as “not used” in this review. Consequently, the application frequencies of PSD principles reported here are likely conservative estimates, and the actual implementation level, particularly for esthetically oriented or system-level default features, may be higher. The studies included in this review primarily originated from high-income countries like the United States, resulting in a sample with relatively concentrated geographical distribution, healthcare systems, and cultural contexts. Factors such as healthcare systems, family structures, digital literacy, and patterns of trust in professional authority may all influence the acceptance and usage patterns of apps among CHD families. The limited reporting of these contextual factors in existing studies makes it difficult to assess the applicability of certain design patterns in other cultural or resource settings. Therefore, future work should involve designing and evaluating CHD family care apps across more diverse regions and populations, systematically reporting medical and social contexts, and integrating cultural sensitivity and accessibility into design considerations.
5. Conclusion
This scoping review mapped the functional characteristics of mHealth apps designed to support family care for children with CHD and examined their design features through the PSD framework. It offers a more detailed picture of how current apps are designed and where the field remains underdeveloped. Current mHealth apps for CHD family care are strongest in supporting information delivery, monitoring, communication, and credibility, but remain less developed in dialogue support and social support. This uneven design profile suggests that most existing apps still operate mainly as tools for care management, with more limited capacity to support the relational, emotional, and sustained work of family caregiving. Rather than simply expanding functional scope, future development may therefore need to focus on how digital tools can better evolve into care partners for families.
Supplemental material
Supplemental material - Mobile health apps for home care support of children with congenital heart disease: A scoping review based on persuasive system design models
Supplemental material for Mobile health apps for home care support of children with congenital heart disease: A scoping review based on persuasive system design models by Jiajia Li, Jiajia Zhu, Xiaomin Tang, Weihong Jiang, Mengyi Chen, Xia Kong, Yiting Gong, Aining Zhang and Jihua Zhu in DIGITAL HEALTH.
Supplemental material
Supplemental material - Mobile health apps for home care support of children with congenital heart disease: A scoping review based on persuasive system design models
Supplemental material for Mobile health apps for home care support of children with congenital heart disease: A scoping review based on persuasive system design models by Jiajia Li, Jiajia Zhu, Xiaomin Tang, Weihong Jiang, Mengyi Chen, Xia Kong, Yiting Gong, Aining Zhang and Jihua Zhu in DIGITAL HEALTH.
Supplemental material
Supplemental material - Mobile health apps for home care support of children with congenital heart disease: A scoping review based on persuasive system design models
Supplemental material for Mobile health apps for home care support of children with congenital heart disease: A scoping review based on persuasive system design models by Jiajia Li, Jiajia Zhu, Xiaomin Tang, Weihong Jiang, Mengyi Chen, Xia Kong, Yiting Gong, Aining Zhang and Jihua Zhu in DIGITAL HEALTH.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of our institutional librarians and peer reviewers who provided guidance on search strategies and manuscript preparation. This work was supported by ZJU-GENSCI CHILDREN'S HEALTH RESEARCH & DEVELOPMENT CENTER.
Consent for publication
All authors agree to submit the manuscript to the journal.
Author contributions
Jiajia Li contributed to conceptualization, data curation, methodology, paper screening, and writing original draft. Jiajia Zhu and Xiaomin Tang contributed to conceptualization and methodology and paper screening.Weihong Jiang and Mengyi Chen contributed to supervision and validation.Xia Kong, Yiting Gong and Aining Zhang contributed to writing—review and editing. Jihua Zhu contributed to conceptualization, methodology, validation, writing—review and editing.
Funding
This work was supported by the 2024 Research Program of the ZJU-GENSCI CHILDREN'S HEALTH RESEARCH & DEVELOPMENT CENTER (Grant No. ZJU-GENSCI2024YB006).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No data was generated in this study, and data availability is not appropriate for this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.