
Abstract
Objectives
Artificial intelligence (AI) is increasingly transforming healthcare delivery and health professions education, creating a need for future healthcare professionals to develop adequate knowledge, practical skills, and ethical awareness. However, many students remain exposed to AI tools without receiving structured academic preparation. This study aimed to assess knowledge, attitudes, practices, and perceived barriers toward AI among nursing and health sciences students.
Methods
A descriptive cross-sectional study was conducted among 242 undergraduate students at a public university in Palestine between January and February 2025. Data were collected using a structured self-administered questionnaire adapted from previous literature and refined through expert review and pilot testing. The survey assessed sociodemographic characteristics, AI-related knowledge and exposure, attitudes, practices, and perceived barriers. Descriptive statistics were used to summarize the data, while Mann–Whitney U and Kruskal–Wallis tests examined subgroup differences.
Results
Participants had a mean age of 20.4 ± 2.28 years, and 77.3% were female. Most students reported using AI tools (83.1%), whereas only 31.0% had received formal AI training. Overall knowledge/exposure scores were moderate (2.78 ± 1.12), attitudes were generally positive (3.64 ± 0.61), and practice levels were moderate (3.18 ± 0.72). No significant differences in knowledge or practice scores were observed across demographic variables (p > .05). Students with formal AI training demonstrated significantly higher attitude scores (p = .019). The most frequently reported barriers were ethical and privacy concerns (44.2%), limited curriculum integration (42.6%), and lack of knowledge or expertise (38.4%).
Conclusions
Students demonstrated substantial exposure to AI technologies but limited structured preparedness for their effective and ethical use. Positive attitudes toward AI suggest readiness for educational adoption; however, moderate knowledge and practice levels indicate the need for formal curriculum integration, faculty development, and competency-based training. Addressing ethical concerns and institutional barriers is essential to support responsible AI implementation in nursing and health sciences education.
Keywords
Introduction
Artificial intelligence (AI) is rapidly transforming both healthcare delivery and health professions education, introducing new paradigms in clinical decision-making, diagnostics, and learning environments. AI encompasses a range of computational techniques including machine learning, natural language processing, and predictive analytics that enable systems to perform complex cognitive tasks traditionally requiring human intelligence.1,2 In clinical contexts, AI has demonstrated potential to enhance diagnostic accuracy, optimize workflow efficiency, and support personalized care, thereby reshaping modern healthcare systems. 3 Parallel to these developments, AI is increasingly integrated into educational settings, where it supports adaptive learning, simulation-based training, and automated feedback systems.
However, it is important to distinguish between three related but conceptually different domains: AI in healthcare delivery, AI in health professions education, and generative AI tools used for academic support. AI in healthcare primarily focuses on clinical applications such as diagnosis and decision support, whereas AI in education emphasizes learning enhancement through simulation and intelligent tutoring systems. In contrast, generative AI tools (e.g., ChatGPT) are widely used by students for academic assistance, including writing, idea generation, and information retrieval. 4 Recent evidence indicates that generative AI has introduced new educational and psychological dynamics, influencing students’ learning behaviors, engagement, and academic integrity. 5 Failure to differentiate these domains may lead to conceptual ambiguity and limit the interpretation of AI readiness in educational contexts.
Within nursing and health sciences education, AI presents both opportunities and challenges. Evidence suggests that AI-supported learning can enhance clinical reasoning, decision-making, and student engagement when appropriately integrated into curricula. 6 However, concerns remain regarding ethical accountability, data privacy, overreliance on automated systems, and potential erosion of critical thinking issues particularly relevant to patient-centered disciplines such as nursing. 7 These concerns highlight the need for balanced educational strategies that integrate technological competence with professional and ethical standards.
Despite increasing exposure to AI technologies, the literature consistently demonstrates a gap between students’ awareness and their formal preparedness to use AI effectively. International studies indicate that although many health sciences students are familiar with AI concepts, structured curricular integration and competency-based training remain limited.8,9 In Middle Eastern contexts, including Palestine, students frequently rely on informal learning sources such as online platforms and peer interactions, resulting in fragmented understanding. 10 Notably, recent research in Palestine has primarily examined students’ attitudes toward AI without providing a comprehensive assessment of knowledge, practices, and barriers, limiting the applicability of findings for curriculum development. 11
Students’ attitudes toward AI are generally positive, reflecting optimism regarding its future role in healthcare. Several studies report that health sciences students recognize AI as essential for professional development and healthcare advancement. 12 However, these favorable attitudes coexist with concerns about ethical implications, data security, and potential job displacement. 13 This duality reflects cautious optimism rather than unconditional acceptance, emphasizing the complexity of AI adoption in healthcare education.
In terms of practice, AI use among students is often limited to low-stakes academic activities, such as assignment preparation, grammar checking, and idea generation, rather than advanced clinical or decision-support applications. 14 This pattern suggests that access to AI tools does not necessarily translate into meaningful or competency-based utilization, particularly in the absence of structured educational guidance.
Multiple barriers further hinder effective AI use in health sciences education. These include limited curriculum integration, lack of faculty expertise, insufficient training opportunities, and unresolved ethical and regulatory frameworks. 15 In resource-constrained and conflict-affected settings such as Palestine, these challenges may be further exacerbated, contributing to disparities in AI readiness and digital health literacy. 16
Given the rapid expansion of AI in healthcare and education, there is a clear need for comprehensive, context-specific assessments of students’ readiness for AI. While previous studies have explored individual aspects such as attitudes or general awareness, few have examined knowledge, attitudes, practices, and barriers simultaneously within a single framework, particularly in Palestinian settings. Addressing this gap is essential to inform evidence-based curriculum development and policy initiatives. The present study aims to comprehensively assess knowledge, attitudes, practices, and perceived barriers toward artificial intelligence (AI) integration among nursing and health sciences students in Palestine. Specifically, the study seeks to evaluate students’ level of knowledge regarding AI concepts and applications, examine their attitudes toward the role of AI in healthcare and education, and assess their patterns of AI use in academic and professional contexts. In addition, the study aims to identify the key barriers that hinder effective AI adoption among students, including educational, ethical, and structural challenges. Furthermore, it explores potential differences in knowledge, attitudes, and practices based on demographic and educational characteristics, particularly formal exposure to AI training. Through this multidimensional approach, the study intends to generate evidence that can inform curriculum development, faculty preparedness, and policy initiatives to support the safe, ethical, and effective integration of AI into health professions education.
Methods
Study design
This study employed a quantitative descriptive cross-sectional design to assess knowledge, attitudes, practices, and perceived barriers toward artificial intelligence (AI) integration among nursing and health sciences students. A cross-sectional approach is appropriate for examining perceptions, behaviors, and educational readiness at a single point in time, particularly for emerging technologies such as AI where baseline evidence is limited. This design has been widely used in similar studies investigating AI readiness among health professions students in diverse educational settings.
Study setting
The study was conducted at Palestine Polytechnic University (PPU), located in Hebron, Palestine. PPU is a public higher education institution offering undergraduate programs in nursing and multiple health sciences disciplines. The setting was selected due to its diverse student population and the presence of digital learning platforms that may facilitate exposure to AI-related tools. Only contextual information relevant to the study environment and potential AI exposure was included to maintain methodological clarity.
Population and sampling
The target population consisted of undergraduate students enrolled in nursing and health sciences programs, including nursing, medicine, dentistry, nutrition, physical therapy, occupational therapy, optometry, and medical laboratory sciences. Eligible participants were students registered in any academic year during the data collection period and able to read and respond to the questionnaire in English, which is the primary language of instruction for health sciences programs at the institution.
Students enrolled in non-health-related programs, academic staff, and those who declined participation were excluded. Additionally, questionnaires with more than 20% missing responses were considered incomplete and excluded from analysis to ensure data quality and consistency.
A non-probability quota sampling technique was used to achieve proportional representation across academic programs and year levels. Although quota sampling carries a risk of selection bias, it was considered appropriate due to logistical constraints and its common use in cross-sectional educational research conducted within defined institutional settings. The required sample size was calculated using the Raosoft® sample size calculator based on a population of approximately 3,034 students, a 95% confidence level, and a 5% margin of error, yielding a minimum sample of 342 participants. However, a final sample of 242 students completed the survey. While lower than the calculated sample, this size remains acceptable for descriptive analysis and nonparametric comparisons, although it may reduce statistical power for detecting small effect sizes.
Study period
Data collection for this study was conducted over a six-week period between January and February 2025. During this time, eligible undergraduate nursing and health sciences students were invited to participate through official university communication channels, including institutional email and the learning management system. Two reminder notices were distributed at two-week intervals to enhance participation rates.
Instrumentation
Data were collected using a structured, self-administered questionnaire adapted from a previously published instrument assessing AI-related knowledge, attitudes, and practices among health professions students. 15 The questionnaire was administered in English, consistent with the language of instruction at the study institution.
The instrument consisted of four domains: 1. Sociodemographic characteristics, including age, gender, academic year, discipline, and prior exposure to AI tools. 2. AI knowledge and exposure, comprising items assessing awareness of AI concepts, familiarity with applications in healthcare, and prior exposure to AI-related learning (e.g., courses or training). Given reviewer concerns, this domain was treated as a combination of knowledge and exposure indicators rather than strictly objective knowledge, acknowledging that some items reflect self-reported familiarity rather than factual correctness. 3. Attitudes toward AI, measured using a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), evaluating perceptions of AI’s usefulness, ethical implications, and role in healthcare and education. 4. Practices related to AI use, assessed using a 5-point Likert scale (1 = never to 5 = always), capturing frequency of AI use in academic, research, and personal contexts. 5. Perceived barriers, including predefined items related to ethical concerns, curriculum limitations, lack of expertise, technological constraints, and system complexity. Participants were allowed to select multiple responses.
Validity and reliability
Content validity was established through structured expert evaluation by four specialists in nursing, medicine, pharmacy, and health education. Experts assessed each item for relevance, clarity, and representativeness. Based on their feedback, minor modifications were made to improve wording and conceptual alignment with study objectives.
A pilot study was conducted with 30 students to assess clarity, feasibility, and completion time. Pilot participants were excluded from the final analysis.
Internal consistency reliability was assessed using Cronbach’s alpha for Likert-scale domains. The attitude domain demonstrated good reliability (α = 0.87), while the practice domain showed very high reliability (α = 0.95). The high alpha value for the practice domain may indicate some redundancy among items and should be interpreted with caution.
For the knowledge/exposure domain, internal consistency estimates should be interpreted cautiously due to the heterogeneous and partially dichotomous nature of items. Although Cronbach’s alpha was calculated (α = 0.82), alternative measures such as Kuder–Richardson Formula 20 (KR-20) may be more appropriate for dichotomous items in future studies.
Data collection procedure
Data were collected using an online survey platform. The questionnaire link was distributed through official university channels, including institutional email lists and the learning management system used for course communication. Students received an invitation explaining the study purpose, voluntary nature of participation, and confidentiality assurances.
Data collection was conducted over a six-week period. Two reminder messages were sent at two-week intervals to enhance response rates. No incentives were provided for participation. To maintain anonymity, no personally identifiable information was collected.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS). Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize participant characteristics and study variables.
The normality of continuous variables was assessed using the Kolmogorov–Smirnov test, which indicated non-normal distribution. Accordingly, nonparametric tests were applied. The Mann–Whitney U test was used to compare differences between two groups (e.g., gender, formal training), while the Kruskal–Wallis test was used for comparisons across multiple groups (e.g., academic year). Statistical significance was set at p < .05.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board of Palestine Polytechnic University (Approval No. EA-2025-123). The study adhered to the principles of the Declaration of Helsinki and relevant international ethical standards for research involving human participants.
Participation was voluntary, and electronic informed consent was obtained prior to data collection. Participants were informed of their right to withdraw at any time without penalty. Confidentiality and anonymity were ensured by not collecting identifying information and restricting data access to the research team.
Results
Participant characteristics
A total of 242 undergraduate students participated in the study. The mean age was 20.4 ± 2.28 years. The majority of participants were female (77.3%, n = 187), while males accounted for 22.7% (n = 55). Participants were distributed across academic years, with the highest proportion in the fourth year (40.9%), followed by third year (25.2%), second year (19.8%), and first year (14.0%).
Most participants reported using artificial intelligence (AI) tools (83.1%, n = 201), whereas only 31.0% (n = 75) had received formal AI training. Missing responses for training status (n = 7) were excluded from subgroup comparisons.
Sociodemographic characteristics and differences in knowledge, attitudes, and practices (N = 242).

*Note. Mann–Whitney U test and Kruskal–Wallis test were used. P < .05 indicates statistical significance.
Overall knowledge, attitudes, and practices scores
Responses to AI knowledge and exposure items (N = 242).

Attitudes toward artificial intelligence
Attitudes toward AI (N = 242).
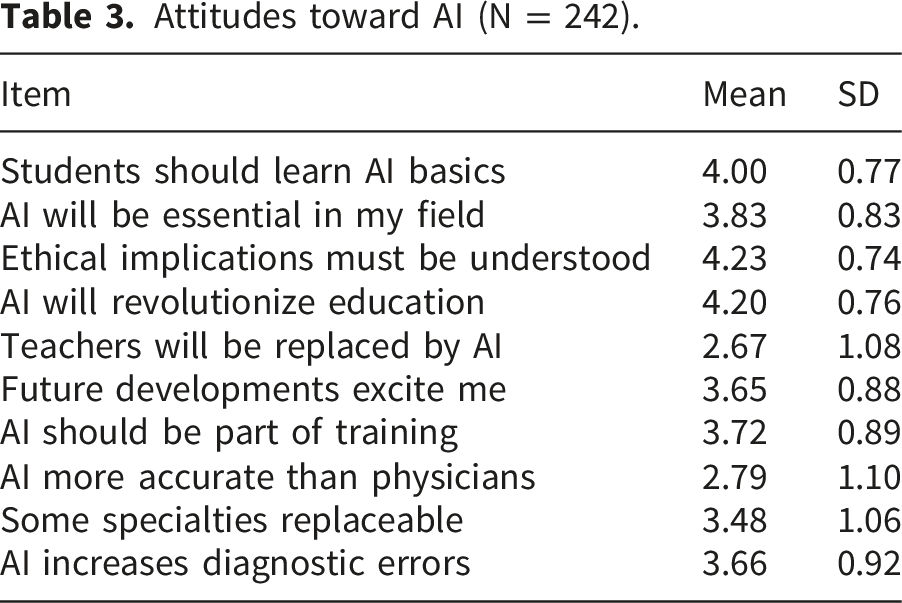
Moderate scores were reported for perceptions related to AI replacing healthcare professionals (mean = 2.67 ± 1.08) and AI accuracy compared with physicians (mean = 2.79 ± 1.10).
Practices related to artificial intelligence use
Practices related to AI use (N = 242).

Perceived barriers to artificial intelligence adoption
Perceived Barriers to AI Adoption (N = 242, multiple responses allowed).

Discussion
This study examined knowledge, attitudes, practices, and perceived barriers toward artificial intelligence (AI) integration among nursing and health sciences students in Palestine. The findings indicate moderate levels of knowledge and practice, alongside generally positive attitudes toward AI. However, these findings should be interpreted cautiously, as the study assessed self-reported perceptions and behaviors rather than objective competency or performance.
The results demonstrated that students possessed limited foundational understanding of AI concepts, particularly in areas such as machine learning and core AI principles, while showing higher awareness of AI applications and barriers. This pattern is consistent with studies conducted among health sciences students in Jordan and Saudi Arabia, where awareness of AI applications was relatively high, but conceptual knowledge remained limited due to insufficient curricular integration.15,17 Similarly, regional studies have reported that students often acquire AI-related knowledge through informal sources rather than structured education, leading to fragmented understanding.14,16 These findings suggest that the observed knowledge profile reflects exposure rather than comprehensive educational preparation.
Attitudes toward AI were generally positive, with students recognizing its importance in healthcare and education and expressing strong agreement regarding the need for ethical awareness. This aligns with findings from international and regional studies, which consistently report favorable attitudes toward AI among nursing and medical students.18,19 However, moderate scores for items related to AI replacing healthcare professionals and concerns about diagnostic accuracy indicate the presence of uncertainty and skepticism. This pattern reflects cautious acceptance rather than unconditional endorsement, which has been similarly reported in studies examining AI perceptions among healthcare students. 20
Despite high levels of reported AI use, practice scores remained moderate and were primarily associated with academic support activities, such as research, assignments, and idea generation. This finding is consistent with previous research indicating that students tend to use AI tools for low-stakes academic tasks rather than for clinically relevant or decision-support applications.15,21 It is important to note that self-reported frequency of use does not necessarily reflect the quality, depth, or appropriateness of AI utilization. Therefore, the results should not be interpreted as evidence of competency or proficiency in AI use, but rather as indicators of usage patterns.
One of the key findings of this study is that formal AI training was associated with more positive attitudes but not with significant differences in knowledge or practice. This finding warrants careful interpretation. Several explanations may account for this pattern. First, the content and duration of training may have been insufficient to produce measurable changes in knowledge or behavior. Second, the measurement of knowledge in this study included both awareness and exposure items, which may have limited sensitivity to detect differences. 22 . Third, the sample size may not have been adequate to detect small effect sizes. Finally, variability in the quality and structure of training experiences may have contributed to inconsistent outcomes. Similar discrepancies between attitudes and measurable competencies have been reported in prior studies, suggesting that attitudinal readiness does not necessarily translate into practical skills.12,13
Perceived barriers to AI were commonly reported and included ethical and privacy concerns, limited curriculum integration, and lack of knowledge or expertise. While these findings are consistent with previous studies conducted in both high- and low-resource settings,12,23 it is important to interpret them within the scope of the data. The study measured perceived barriers rather than objectively assessed institutional or systemic constraints. Therefore, although educational and structural challenges were frequently reported, it cannot be conclusively determined that these barriers are primarily systemic rather than attitudinal. Instead, the findings suggest that multiple factors educational, ethical, and resource-related—coexist and may collectively influence AI adoption. 24 .
The findings of this study should also be interpreted in the context of the Palestinian educational environment. Resource limitations, variability in curriculum design, and restricted access to advanced technologies may influence both exposure to AI and opportunities for structured learning. However, the current study did not directly measure institutional readiness or infrastructure, and therefore conclusions regarding contextual constraints should remain cautious.
Implications for education and practice
The findings highlight the need for structured integration of AI into nursing and health sciences curricula, with a focus on foundational knowledge, ethical considerations, and applied competencies. Educational interventions should move beyond exposure and aim to develop critical appraisal skills and responsible use of AI technologies. Faculty development and institutional support are also essential to ensure effective implementation. However, these implications should be considered as recommendations based on observed patterns rather than definitive conclusions.
Strengths and limitations
This study provides a comprehensive assessment of AI-related knowledge, attitudes, practices, and perceived barriers within a single framework, contributing to the limited body of research in Palestinian and similar contexts. The use of a structured instrument and appropriate statistical analyses enhances the methodological rigor.
Nevertheless, several limitations should be acknowledged. The cross-sectional design precludes causal inference. Data were self-reported, which may introduce response bias. The use of non-probability sampling limits generalizability. Additionally, the knowledge domain included both exposure and awareness items, which may not fully capture objective knowledge. The study also did not assess actual AI competency or institutional readiness, which are important areas for future research.
Conclusion
Artificial intelligence is increasingly relevant to healthcare education, yet students in this study demonstrated a mismatch between high exposure and limited structured preparedness. Although attitudes toward AI were generally positive, foundational knowledge and applied competencies remained moderate, while ethical concerns, insufficient curricular integration, and limited expertise were commonly perceived barriers. Formal AI training was associated with more favorable attitudes, suggesting that educational exposure can positively influence readiness. These findings underscore the urgent need for structured curriculum reform, faculty capacity building, and ethical governance frameworks to ensure safe, evidence-based, and professionally responsible AI within nursing and health sciences education. Future multicenter and longitudinal studies are recommended to evaluate competency-based interventions and long-term educational outcomes.
Footnotes
Acknowledgement
The authors would like to thank the nursing student who participated in this study for their time and valuable contributions. Special appreciation is extended to the University for facilitating data collection. Gratitude is also due to Palestine Polytechnic University for their ethical oversight and support throughout the research process.
Ethical considerations
Ethical approval for this study was obtained from the Institutional Review Board of Palestine Polytechnic University (Approval No. EA-2025-123). The study was conducted in full accordance with the ethical principles outlined in the
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions related to participant confidentiality and institutional regulations but are available from the corresponding author upon reasonable request.
Data guarantor
corresponding author accepts full responsibility for the integrity of the data, accuracy of the analysis, and decision to submit the manuscript for publication.