
Abstract
Background
The rising prevalence of chronic diseases and the widespread use of smartphones have led to a surge in preventive health mobile applications (mHealth apps) for corporate wellness. However, user retention and the intention to continue using these apps remain suboptimal. This study examines factors influencing corporate employees’ intention to continue using a preventive health mHealth app in Thailand, using the Health Belief Model (HBM) as the guiding framework.
Methods
A cross-sectional survey was conducted among a sample of corporate employees in Thailand. The survey questionnaire measured constructs from the HBM, including perceived severity of disease, perceived benefits of using mHealth apps, cues to action, and self-efficacy in using mHealth apps. Structural equation modeling (SEM) was employed to analyze the relationships between these constructs and the intention to continue using preventive health mHealth apps.
Results
Perceived benefits were the strongest predictor of intention to continue using the app. Cues to action and self-efficacy were also significant predictors, whereas perceived severity was not a significant factor.
Conclusion
The findings underscore the importance of highlighting the benefits of mHealth apps and leveraging cues to action and user confidence in the intention to continue using. Strategies in corporate wellness should focus on these factors to enhance engagement. However, because this study evaluated a single wellness app among pre-selected users already engaged with the app, the results should be interpreted with caution and may not be generalizable to other settings or populations.
1. Introduction
Non-communicable diseases (NCDs), such as cardiovascular diseases, cancer, diabetes, and chronic respiratory diseases, represent the most significant global health threat, accounting for over 74% of global mortality. 1 Every year, 18 million people aged 30 to 69 years die prematurely due to NCDs, with 82% of these deaths occurring in low- and middle-income countries. 2 In Thailand, with a population of 71.7 million, NCDs are responsible for 68% of total mortality, and 15% of Thai citizens face a heightened risk of premature death from one of the four major NCDs.1,2 Premature deaths and prolonged illnesses caused by NCDs exert a substantial toll on economic growth by diminishing labor force contributions and individual earning potential. Those living with chronic diseases are not only more likely to experience increased absenteeism but may also exhibit reduced productivity while present at work, a phenomenon known as presenteeism. 3 Studies reveal that the financial impact of employee absenteeism and presenteeism due to poor health far exceeds direct healthcare costs alone.4,5 The primary risk factors leading to NCDs include tobacco and alcohol consumption, physical inactivity, obesity, excessive fat and salt intake, insufficient fruit and vegetable consumption, raised blood pressure, elevated glucose, and high cholesterol levels. 6 Among the most effective preventive strategies are those that promote lifestyle modifications, such as healthier diets, increased physical activity, smoking cessation, and managing metabolic disorders. 7
The rapid growth of mobile technology has transformed health promotion strategies. Mobile health (mHealth) applications are increasingly used to support preventive health behaviors by providing users with tools to track physical activity, monitor health indicators, and receive personalized health education. These platforms are especially useful in workplace wellness programs, where they can reduce health-related absenteeism and improve productivity. However, while adoption of mHealth tools has expanded, the intention to continue using them remains a challenge. Many users discontinue use after initial onboarding, limiting the impact of these programs. In Thailand, corporations have begun integrating mHealth apps to support employee well-being. 8 Understanding the intention to continue using these tools is essential for ensuring sustained participation and impact.
This study investigates the intention to continue using the “i-Live Well” app, a preventive health application implemented across multiple corporations in Thailand. Distinct from adoption studies, our research focuses specifically on post-adoption behavior, which motivates existing users to continue engaging with the app over time. This approach recognizes that the psychological drivers of intention to continue using may differ from those influencing initial uptake.
To explore these behavioral drivers, we applied a modified version of the Health Belief Model (HBM), a widely used framework for understanding health-related behaviors. 9 While the traditional HBM includes six constructs: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy, this study focuses on four: perceived severity, perceived benefits, cues to action, and self-efficacy. Perceived susceptibility and perceived barriers were excluded based on both theoretical considerations and empirical evidence from prior research, which suggests that these constructs often have diminished relevance in post-adoption contexts where users have already overcome access hurdles and committed to preventive actions. 10 Our adaptation reflects a contextual application of HBM tailored to the intention to continue using rather than a theoretical extension.
Compared to technology-centered models such as the Technology Acceptance Model (TAM) and the Theory of Planned Behavior (TPB), which emphasize perceived usefulness, ease of use, and intention based on social norms, the HBM offers a health-specific lens. Its focus on health motivation, risk perception, and confidence is especially relevant for understanding the behavioral drivers behind preventive health actions, such as using an app to reduce disease risk.
This research contributes to the underrepresented literature on mHealth intention to continue using behavior in Southeast Asian workplace settings. By examining psychological determinants in a real-world corporate wellness context, the study provides evidence on how employees interact with digital health tools beyond the point of adoption.
Based on the literature and the HBM framework, we proposed the following hypotheses:
Cues to action positively influence the intention to continue using the app.
Perceived benefits positively influence the intention to continue using the app.
Perceived severity positively influences the intention to continue using the app.
Self-efficacy positively influences the intention to continue using the app.
Ultimately, the study seeks to generate insights that can inform the design of effective workplace wellness strategies and support intention to continue using mHealth technologies in culturally relevant ways.
2. Background
2.1. Mobile health (mHealth) applications
mHealth apps leverage mobile devices to deliver home healthcare services, playing a pivotal role in providing feedback, setting goals, and facilitating self-monitoring. 11 These technologies, encompassing smartphones, tablets, and wearables, enable users to track physical activity, diet, sleep patterns, and physiological metrics such as heart rate and blood pressure. 12 Studies have demonstrated that mHealth apps are effective in managing chronic conditions, promoting healthy behaviors, and improving health outcomes. Their role in preventive health is particularly valuable, as they support early detection and timely intervention, significantly alleviating the burden on healthcare systems. 13
In corporate environments, where sedentary lifestyles and stress often contribute to health problems, mHealth apps serve as valuable tools for empowering employees to proactively manage their health. Through corporate wellness programs, employees gain access to mHealth technologies, which can enhance productivity and reduce absenteeism by supporting their health and well-being. 14 However, the intention to continue using (willingness to keep using the app over time) remains low in corporate settings. 15 Understanding the psychological and environmental factors that influence sustained app usage is critical to maximizing the long-term impact of mHealth technologies.
In this study, all participants are corporate employees who had already adopted the “i-Live Well” application, an AI-powered employee well-being platform implemented by a limited number of partner companies in Thailand. The application includes key features such as personalized health missions (e.g., nutrition and exercise), IoT health tracking (e.g., sleep habits, steps, calorie intake), AI-recommended personalized meal plans, entertainment activities (e.g., mini-games and rewards), a company mission feature that promotes engagement between the company and employees, social media communication, and a corporate health dashboard that displays an overview of company well-being based on employee assessments as shown in Figure 1. The example of the user interface for the i-Live well application is from the employee’s perspective.
2.2. Health Belief Model (HBM)
The Health Belief Model (HBM) is a well-established framework for predicting and explaining health-related behaviors. It posits that an individual’s decision to engage in a health action is shaped by their appraisal of health risks (threat) and the evaluation of the effectiveness of taking preventive measures (coping). While the HBM was originally designed to explain one-time health behaviors or initial adoption, recent literature increasingly applies it to the intention to continue using phase (post-adoption) of mHealth usage.
Research adapting the HBM to mHealth intention to continue using often finds that traditional factors undergo a shift in predictive power after initial adoption. Perceived susceptibility (belief in one’s risk of illness) and perceived barriers (obstacles to using the technology) frequently exhibit limited influence on the intention to continue using among existing users.16,17
This phenomenon occurs because users who have already integrated a health app into their routine have typically overcome initial barriers, such as technical complexity or setup costs, especially within supportive corporate environments. Furthermore, because active users generally possess a high baseline acknowledgement of their health risks, there is often insufficient variance in perceived susceptibility to drive ongoing behavioral intention.
Consequently, this study utilizes a modified HBM framework that explicitly excludes susceptibility and barriers to maintain theoretical precision for a post-adoption context. We position this as a contextual application of HBM rather than a novel theoretical contribution, acknowledging that our adaptation is guided by behavior patterns specific to continued digital engagement in workplace health environments.
The four remaining constructs in this model are defined as follows: 1. Perceived Severity refers to beliefs about the seriousness of a health problem and its potential impact. For employees, this construct involves their assessment of the consequences of ignoring health management through digital tools. 2. Perceived Benefits pertain to the advantages employees associate with using mHealth apps, such as better health outcomes and more efficient health tracking. 3. Cues to Action serve as prompts that encourage employees to take health-related action. This could include reminders from the app itself or workplace health campaigns. 4. Self-efficacy involves employees’ confidence in their ability to successfully use mHealth apps and maintain engagement with their health management routines.
While HBM is a health-specific model, this study also recognizes insights from post-adoption literature, such as Expectation-Confirmation Theory (ECT) and habit formation frameworks. ECT suggests that continued use is driven by how well the app meets users’ expectations and satisfaction. 18 Habit formation has emerged as a powerful explanation for sustained engagement with mHealth apps and wellness tools. Habit theory suggests that as users repetitively perform a behavior in stable contexts, it can become automatic, continuing not because of a conscious decision, but because it’s ingrained in routine. 19 Including these perspectives supports a more comprehensive understanding of the intention to continue using the process, particularly in digital health settings.
2.3. Corporate wellness programs
Corporate wellness programs aim to enhance employee well-being by offering initiatives like health screenings, fitness challenges, and wellness workshops. Integrating mHealth apps into these programs adds value by offering personalized health recommendations, tracking health metrics, and providing real-time feedback. 20 These tools can make health management more engaging, fostering long-term behavioral changes that benefit both employees and employers.
However, most existing studies on corporate mHealth engagement have been conducted in Western contexts. There is limited research exploring how organizational structure, health culture, and employee motivation influence mHealth use in non-Western corporate settings like Thailand. Thai workplace environments, often hierarchical and collectivist, may influence how employees respond to digital health prompts, especially when these prompts come from organizational leaders or peer networks.
This study aims to address that gap by examining the psychological, behavioral, and contextual factors shaping the intention to continue using mHealth apps among corporate employees in Thailand. By applying a modified HBM and drawing from relevant post-adoption literature, this research provides a theory-informed understanding of intention to continue using digital health in the workplace. The findings are expected to inform more culturally and organizationally tailored wellness strategies, both within Thailand and in similar settings globally.
3. Method
3.1. Study design
This study employs a quantitative research design to investigate the psychological factors influencing the intention to continue using a preventive health mobile app among corporate employees in Thailand. The research was grounded in a modified version of the Health Belief Model (HBM), which has been widely used to explain health-related behavior but was adapted in this study to address the distinct context of existing users’ intentions to continue using the application.
3.2. Instrument and measures
A structured questionnaire was developed based on validated HBM scales and adapted to the Thai corporate context. Items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). Sample items include: 1. 2. 3. 4. 5.
The original Thai questionnaire was translated into English using a forward–back translation method, followed by pretesting and cognitive interviews with 10 corporate employees to ensure clarity and cultural appropriateness.
The questionnaire consisted of four sections: 1. Demographics and Work Profile: age, gender, education, income, job role, organizational type, and health history. 2. mHealth App Usage: general use patterns and awareness of different health apps. 3. HBM Constructs: perceived severity, benefits, cues to action, and self-efficacy. 4. Behavioral Intention: intention to continue using the health app. (Recommendations from coworkers, social media promotions)
3.3. Participants and sampling
The target population consisted of corporate employees from 11 Thai companies that had already implemented the i-Live Well preventive health application as part of their workplace wellness programs. Since all respondents were current users, the study focuses on continuation intention, not initial adoption. This context was essential for evaluating intention to continue using mHealth tools.
A purposive sampling approach was used, specifically selecting companies and employees actively using the i-Live Well app. The sample aimed to capture variation across sectors and organizational roles. This selective strategy allowed in-depth analysis of continued use behavior but may limit the generalizability of findings to other contexts or non-users.
The required sample size was calculated using Cochran’s formula for an unknown population proportion, targeting 250 participants to ensure adequate power for Structural Equation Modeling (SEM). A total of 500 surveys were distributed, and 285 complete responses were received, yielding a response rate of 57%. While nonresponse bias was not formally assessed, the sample reflects a diverse cross-section of private sector employees across different industries and roles.
3.4. Data collection
Data were collected via an online survey platform between January and March 2024. The survey link was disseminated through email and corporate HR channels. The study followed ethical practices: all participants were informed about the purpose of the research, assured of confidentiality and anonymity, and informed that participation was voluntary.
To improve clarity and consistency, the study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies. A completed STROBE checklist has been included as a supplemental file.
3.5. Data analysis
The collected data were analyzed using Structural Equation Modeling (SEM) with the help of SmartPLS software. SEM was chosen for its ability to examine complex relationships between observed and latent variables, offering a comprehensive analysis of the factors influencing mHealth app intention to continue using.
The analysis procedure consisted of the following steps: 1. Data Screening: Raw data were screened for missing values, outliers, and inconsistencies. Responses with significant missing data (more than 10%) or outliers significantly deviating from the sample distribution were excluded. 2. Descriptive Statistics: Descriptive statistics were calculated to summarize demographic characteristics and survey item responses. 3. Reliability and Validity: The reliability and validity of the constructs were assessed using Cronbach’s Alpha, Composite Reliability (CR), and Average Variance Extracted (AVE). Constructs with an AVE greater than 0.50 and a CR greater than 0.70 were considered to demonstrate acceptable reliability and convergent validity. 4. Structural Model Assessment: The structural model was evaluated by examining path coefficients, t-values, and p-values to determine the significance of the relationships between HBM constructs and behavioral intention. The model’s explanatory power was assessed using the coefficient of determination (R2), with a higher R2 indicating stronger explanatory power. Variance Inflation Factor (VIF) to assess multicollinearity. Bootstrapped confidence intervals (using 10,000 resamples) for estimating precision.
3.6. Ethical considerations
The study obtained ethical approval from the lead researcher’s affiliated institution’s Institutional Review Board (IRB). Informed consent was obtained from all participants, who were informed of their right to withdraw from the study at any time without consequence. The research adhered to ethical guidelines, ensuring the confidentiality and anonymity of participant data throughout the study.
4. Results
4.1. Descriptive statistics
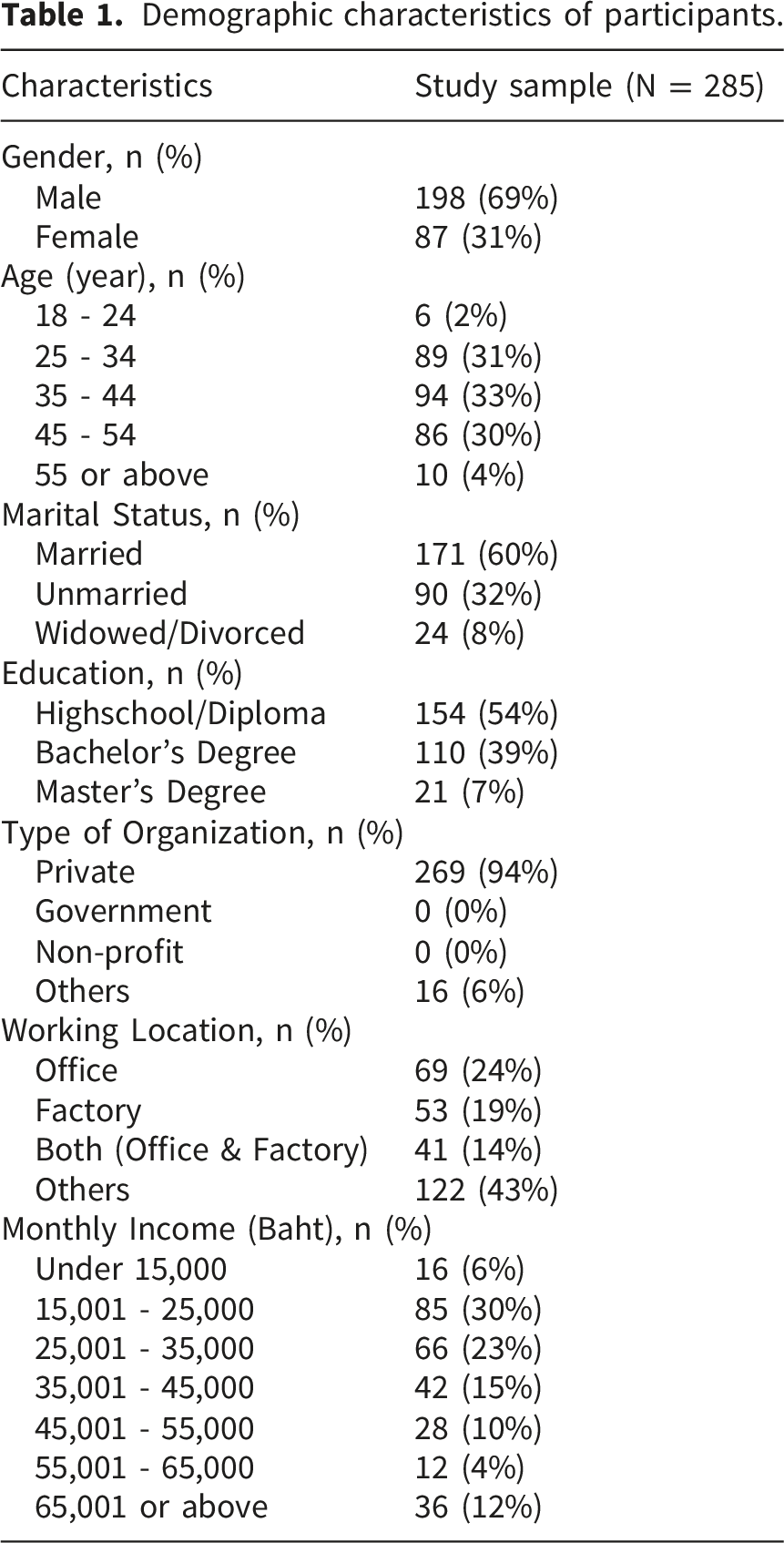
Data screening, including item-level missing data, was examined before model estimation. As shown in the descriptive data screening, the proportion of missing responses for all measurement items ranged from 0% to 6.7%, which is below the commonly accepted thresholds for SEM-based survey research (5–10%). The missing data did not display any systematic pattern, indicating that the data were likely missing at random. SmartPLS applies listwise deletion for missing values; therefore, all subsequent analyses were conducted using the complete and cleaned dataset.
Demographic characteristics of participants.
4.2. Measurement model assessment
Measurement model results: Outer loadings, AVE, CR, and VIF.

Comparison of reliability and validity before and after removing CA3.

Multicollinearity was assessed using the Variance Inflation Factor (VIF). All indicators had VIF values below 7.0, with most under 5. Three items in the Perceived Benefits construct exceeded 5 (PBE1 = 5.14, PBE3 = 6.59, PBE4 = 5.98) but were retained based on high outer loadings and the reflective nature of the construct.
4.3. Discriminant validity
Cross-loadings matrix for discriminant validity.

4.4. Model fit assessment
Structural model fit indices.

4.5. Explanatory power
R2 and adjusted R2 for endogenous variable.

4.6. Structural path estimates and hypothesis testing
Hypothesis testing results.
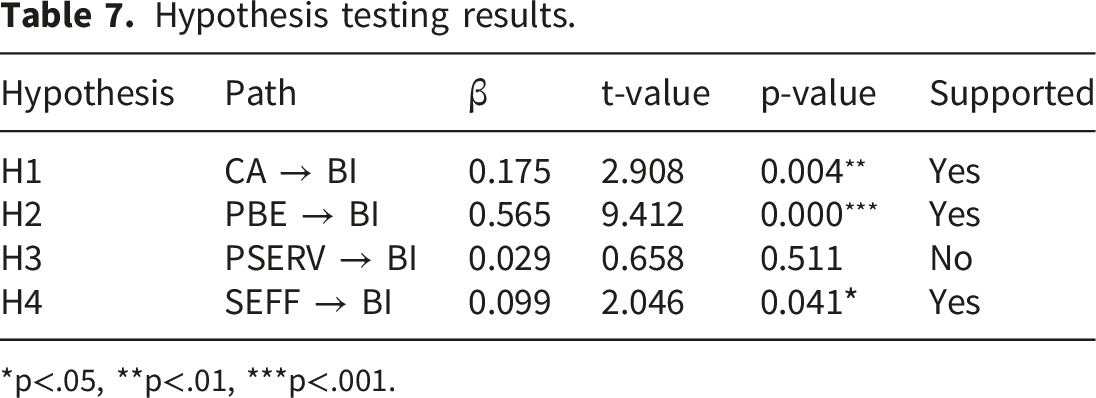
*p<.05, **p<.01, ***p<.001.
The unsupported hypotheses, related to perceived severity, suggest that these factors may not play a crucial role in the intention to continue using preventive health mobile apps in Thailand’s corporate context. These findings underscore the importance of perceived benefits in driving the intention to continue using mHealth apps, while cues to action and self-efficacy also play a moderate role.
4.7. Final SEM diagram
The results in Figure 2 show that the perceived benefits (PBE) variable had the highest t-value, indicating the strongest influence on behavioral intention (BI). Cues to action (CA) and self-efficacy (SEFF) also demonstrated significant effects, ranking second and third, respectively, in terms of t-values. In contrast, perceived severity (PSERV) had a relatively low t-value, suggesting a weaker influence on behavioral intention. Final structural equation model for intention to continue using.
5. Discussion
5.1. Theoretical reframing: A modified HBM for intention to continue using
This study examined factors associated with corporate employees’ intention to continue using a preventive mHealth application in Thailand. Although the Health Belief Model (HBM) is classically used to explain health behavior initiation, we applied a modified HBM to a post-adoption context. We emphasize that this modification should be understood primarily as a contextual application of existing mHealth intention to continue using literature rather than a novel theoretical extension. Specifically, the exclusion of perceived susceptibility and perceived barriers has been reported in prior mHealth studies and is consistent with the notion that, once users are already active, entry barriers (e.g., access, installation, onboarding) are largely resolved and perceived susceptibility may show limited variability among continuing users. 10
Accordingly, the modified HBM in this study is intended to improve stage fit (intention to continue using vs. adoption). In the intention to continue using settings, determinants may shift from threat appraisal to the perceived value of ongoing use, reinforcement mechanisms, and emerging routines. This is conceptually aligned with post-adoption perspectives (e.g., expectation confirmation and habit formation) that emphasize satisfaction, perceived usefulness/value, and repeated behavior as drivers of ongoing engagement.
5.2. Perceived benefits: Instrumental vs. affective drivers
Perceived benefits emerged as the most powerful predictor of continued app use. To deepen this analysis, these benefits can be categorized into instrumental and affective dimensions.
5.2.1. Instrumental benefits (utility/value)
Practical functions such as progress tracking (steps, activity streaks), access to personal health metrics, and actionable feedback. These features help users see measurable outcomes and support goal-oriented behavior in workplace contexts. This aligns with recent findings that emphasize perceived usefulness as a cornerstone of post-adoption stability. 21
5.2.2. Affective benefits
The inclusion of gamified points and social rewards suggests that emotional satisfaction and joy of use also sustain engagement. 22
This distinction helps explain why perceived benefits outperformed perceived severity: users may be motivated more by immediate, tangible value and positive experience than by abstract disease threat, particularly in a corporate wellness setting where engagement competes with time constraints and work priorities. Practically, program communication should therefore emphasize concrete, near-term value (e.g., easier monitoring, clear progress feedback, rewards) rather than relying primarily on risk-based messaging.
5.3. Cues to action: Managerial and organizational endorsement
Cues to action significantly influenced behavioral intention, reflecting the importance of environmental or social prompts in sustaining digital engagement. In this study, cues were more effective when embedded in organizational routines (e.g., HR communications, manager encouragement, team challenges) rather than relying on purely app-driven nudges.
The low performance of CA3 (“shared the app with coworkers”) suggests that informal peer diffusion may be less influential than formal endorsement in this corporate context. One possible explanation is that in hierarchical workplaces, employees may interpret managerial endorsement as a signal of legitimacy and priority. Importantly, this interpretation is hypothesis-generating rather than definitive, as cultural norms were not directly measured. This aligns with recent occupational health literature emphasizing that in collectivist and hierarchical settings, employees often look to leadership to validate the legitimacy of wellness initiatives. 23
These findings support the view that effective workplace mHealth programs require upstream prevention support, for example, structured onboarding, leadership participation, and clear alignment with wellness goals, so that app prompts are perceived as legitimate and relevant rather than intrusive.
5.4. Self-efficacy, health literacy, and the path to habit formation
Self-efficacy had a moderate but significant association with intention to continue using. In post-adoption contexts, self-efficacy may reflect more than technical confidence; it also relates to whether users feel capable of using app feedback to guide health actions. In that sense, self-efficacy is closely connected to functional health literacy: users must not only operate the app but also understand what the metrics imply and how to respond (e.g., interpreting a low activity score and choosing feasible corrective steps). This aligns with recent research, which demonstrates that baseline health literacy is a prerequisite for meaningful engagement in digital interventions. 24
This suggests that workplace wellness initiatives should include literacy-oriented onboarding (brief explanations of key metrics, examples of what to do next, short guided challenges) and user support (tutorials, peer ambassadors, or help channels). Such supports may help translate app interaction into meaningful preventive behaviors, thereby strengthening the pathway from self-efficacy to the intention to continue using.
5.5. Perceived severity and cultural context
Perceived severity did not significantly predict intention to continue using. In a post-adoption setting, this pattern is plausible: users who already engage with a preventive tool may be less influenced by disease threat and more by value, reinforcement, and routine. This result is consistent with prior findings in post-adoption contexts, where users may no longer be motivated by disease threat but instead by ongoing utility or habit. 25 In addition, corporate wellness participation may be shaped by institutional practices (e.g., annual checkups, HR initiatives), potentially reducing the motivational role of perceived severity.
One possible cultural explanation, such as hierarchy or collectivism influencing responsiveness to leadership cues, should be treated as an interpretative hypothesis rather than empirical conclusions. Future research could measure workplace culture constructs directly (e.g., perceived organizational support, leadership endorsement, collectivism/power distance) and use qualitative methods to test these mechanisms.
5.6. Recommendations for practitioners
Based on the observed pattern of associations, organizations aiming to strengthen intention to continue using may consider: 1. Make benefits tangible and immediate: emphasize progress dashboards, personalized feedback, and clear short-term wins. 2. Design structured cues to action: combine app notifications with HR messaging and manager-supported challenges. 3. Use onboarding for early success: e.g., a 7-day guided mission to establish routine and early reinforcement. 4. Support self-efficacy through health literacy: simple explanations of metrics, action suggestions, tutorials, and peer ambassadors. 5. Build trust through privacy protection: clearly communicate data boundaries (what employers can/cannot see) to reduce concern and encourage engagement.
5.7. Limitations and interpretative constraints
Several limitations warrant emphasis. First, the primary outcome is self-reported intention to continue using, which is a proximal and subjective measure and should not be interpreted as actual long-term usage, adherence, or health outcomes. The cross-sectional design also limits causal inference and may be susceptible to social desirability bias, ceiling effects, and post-hoc rationalization among active users.
Second, the study is context-specific: examined a single application implemented in partner companies and used purposive sampling of active users. Findings should therefore be interpreted as most applicable to workplace settings with comparable implementation conditions (e.g., similar wellness program structure, communication channels, and incentive arrangements), rather than generalized to all corporate mHealth tools.
Third, the study was funded by the app, and several authors were affiliated with partner companies. These relationships were transparently disclosed and may be associated with potential selection effects (e.g., higher participation among more engaged users) and response tendencies (including social desirability) in an employer-linked survey context. In addition, company-level implementation features, such as HR communications and managerial endorsement, may shape perceived benefits and cues to action and thereby influence reported intentions. To mitigate these risks, the study employed standardized survey procedures, anonymous data collection, and independent analysis; nevertheless, residual bias cannot be fully excluded.
Future studies should incorporate objective usage logs, longitudinal designs, and broader samples (including non-users and public-sector contexts) to evaluate whether intention to continue using translates into sustained behavior and health impact.
6. Conclusion
This study examined psychological and organizational factors associated with employees’ intention to continue using a preventive corporate wellness mHealth app in Thailand. Using a modified Health Belief Model as a context-appropriate approach for post-adoption behavior, the findings indicate that intention to continue using is primarily associated with perceived benefits (instrumental and affective), cues to action, and self-efficacy, while perceived severity was not significant in this setting.
These results suggest that the intention to continue using in workplace mHealth programs is more likely to be supported by immediate, tangible value (e.g., progress tracking, feedback, incentives) and positive user experience (e.g., gamification), rather than fear-based messaging about disease consequences. In addition, the significance of cues to action underscores that workplace mHealth tools are most effective when paired with organizational infrastructure, such as HR-led campaigns, managerial endorsement, and structured wellness activities, rather than relying solely on informal peer diffusion.
Practically, organizations should provide literacy-oriented onboarding that helps employees interpret health metrics and translate app feedback into actionable steps. Early quick wins (e.g., a guided 7-day challenge), meaningful incentives (e.g., health points or gym subsidies), and consistent prompts (e.g., push notifications integrated with workplace communication) may strengthen continued engagement. Clear privacy communication, including separation of individual health data from employer access, remains essential for trust.
The findings should be interpreted considering key limitations. The study assesses self-reported intention, not objective long-term usage or health outcomes, and is based on purposive sampling of active users of a single app implemented in partner companies. In addition, funding and organizational affiliations may introduce potential selection or response biases despite anonymized procedures. Future research should incorporate longitudinal designs and objective usage data to examine whether intention to continue using translates into sustained behavior and measurable health impact across a broader organizational setting.
Supplemental material
Supplemental Material - Intention to continue using corporate wellness mHealth apps in Thailand: A health belief model approach
Supplemental Material for Intention to continue using corporate wellness mHealth apps in Thailand: A health belief model approach by Kittipoom Supamontri, Natcha Limtrakun, Benjaphon Limphonyan, Piroonrat Wangprakob and Thipwadee Krumram in Digital Health.
Supplemental material
Supplemental Material - Intention to continue using corporate wellness mHealth apps in Thailand: A health belief model approach
Supplemental Material for Intention to continue using corporate wellness mHealth apps in Thailand: A health belief model approach by Kittipoom Supamontri, Natcha Limtrakun, Benjaphon Limphonyan, Piroonrat Wangprakob and Thipwadee Krumram in Digital Health.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to all participating organizations and employees who contributed their time and insights to this study. We are also thankful to the Human Resources departments of the 11 participating companies for facilitating the data collection process. Special thanks to Ajinomoto Co., (Thailand) Ltd. for their collaboration and support throughout the project. We also acknowledge the Medical Innovation team at Invitrace Company Limited for their valuable assistance in distributing the online survey, collecting responses, and supporting data analysis.
Ethical considerations
The ethics committee for human research of the Bangkok University approved this study (Reference number: 416702007).
Consent to participate
Written informed consent to participate was obtained from all participants.
Author contributions
Kittipoom Supamontri designed the study and was involved in the development of the study protocol and gaining ethical approval. All authors were involved in data collection and analysis as well as the write-up of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Invitrace Company Limited, a health technology company, funded this study.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure and declare: Kittipoom Supamontri, Phd, received research funding from Invitrace Company Limited. No other conflicts of interest are declared.
Supplemental material
Supplemental material for this article is available online.