
Abstract
Background
Uterine contraction is a meaningful indicator for labor onset and appropriate hospital admission. Inaccurate self-assessment may lead to premature admission, unnecessary interventions, and higher healthcare resource use. Traditional monitoring devices have limited portability and comfort, restricting home-based use.
Objective
This study developed and validated a wearable system integrating flexible sensors, a data acquisition platform, and machine learning models to monitor uterine contractions and identify labor onset, focusing on late pregnancy and the pre-labor period.
Methods
A flexible sensor-based device was developed and validated against hospital toco. Contraction data from 82 participants (104 recordings) were preprocessed and segmented, and features were extracted for model training. Hospital admission was classified into recommended admission (RA), deferred admission (DA), and selective admission (SA). Several ML models were trained and evaluated via 10-fold stratified cross-validation using accuracy, precision, recall, F1-score, and area under the curve. Shapley Additive Explanations (SHAP) analysis interpreted feature contributions.
Results
A total of 82 participants were enrolled, and 104 uterine contraction recordings were collected, ranging from 10 to 70 min (mean 20.3). Two hundred and seventy-seven processed segments were obtained for analysis. Contraction signals were generally consistent with toco measurements (r = 0.85–0.95). XGBoost achieved accuracy of 0.87 for RA classification, and SHAP identified kurtosis, signal energy area, and standard deviation as key features.
Conclusion
The system enabled accurate monitoring of uterine contractions, improved estimation of hospital admission timing, reduced premature admission risk, and demonstrated high wearability, offering a feasible solution for home obstetric monitoring.
Keywords
Introduction
Uterine contractions, as the direct physiological indicator of uterine excitability, are widely used to assist in assessing labor progression. 1 The WHO Labour Care Guide 2 recommends monitoring key indicators, including contraction frequency and duration, cervical dilation, and fetal descent, to guide hospital admission and intervention decisions. According to Chinese clinical consensus, 3 labor onset is characterized by regular and progressively stronger uterine contractions, each lasting at least 30 s and occurring every 5‒6 min, and is typically accompanied by cervical effacement, cervical dilation, and fetal descent. When these signs are present, hospital admission is warranted. This idea highlights that identifying regular contractions provides a quantifiable temporal target for admission.
Determining whether primigravidas experiencing contractions are in active labor and require hospital admission remains challenging. 4 Women in late pregnancy who are awaiting the onset of labour often experience irregular Braxton Hicks contractions, which are not indicative of true labour. 5 In clinical practice, professionals usually assess uterine contractions by manual palpation or with specialized devices, such as intrauterine pressure catheters (IUPC), tocodynamometers (toco), and electrohysterography (EHG). 6 Manual palpation, a traditional method, was widely used in the past. However, its accuracy largely depends on the examiner's experience and lacks objective quantitative standards, leading to high subjectivity and low repeatability. 7 With advances in monitoring technology, the independent use of palpation has gradually declined and is increasingly employed only as a supplementary method alongside instrument-based measurements. 8
Toco is the most commonly used external uterine contraction monitoring tool in clinical settings. Nevertheless, because toco is usually integrated into large fetal monitoring systems, its connection with bulky components limit its use in home settings. 9 In contrast, IUPC involves inserting a flexible catheter with a micro-sensor at its tip through the cervix into the uterine cavity to measure intrauterine pressure changes. This method provides much higher measurement accuracy than external monitoring, but its invasive nature increases the risk of infection. 10 EHG, a novel non-invasive technique, measures uterine electrical activity to reflect contraction status, 11 It offers real-time monitoring and potentially higher accuracy. Based on this principle, many manufacturers have developed wearable patches. However, EHG signals are easily affected by maternal movement, breathing, and fetal activity, and proper electrode placement is required. Although these devices emphasize comfort and can accommodate different BMIs, key technical parameters and clinical validation data are rarely reported. Therefore, EHG has not yet been widely adopted in routine clinical practice. 12
Outside clinical settings, however, pregnant women relying solely on self-perception without professional instruments find it difficult to accurately differentiate contractions. Primigravidas, in particular, due to safety concerns and heightened anxiety, frequently present to the hospital earlier than necessary. 13 Early admission does not efficiently improve the childbirth experience. In contrast, it increases maternal stress, strains healthcare resources, and often leads to interventions rather than allowing natural labor progression. 14 These interventions, including analgesia and labor induction, raise the likelihood of cesarean delivery and related postoperative risks. 15 Early admission can trigger the “Domino effect” amplifying resource use and potentially affecting maternal and neonatal outcomes, as well as future pregnancy safety.
Medical uterine contraction monitoring devices are limited by signal stability and size, restricting their use outside clinical settings. 16 Advances in artificial intelligence and flexible wearable technologies have enabled perinatal health management to extend from hospitals to the home. 17 Although some wearable contraction monitors for remote surveillance have emerged, systematized solutions for labor onset identification and admission time determination still remain scarce. 18 Based on this situation, we developed a portable and accurate wearable device designed for home use. Our system integrates flexible sensors with ML algorithms to help primigravidas identify regular contractions, assess labor onset, and support appropriate admission time.
Furthermore, this study aims to develop and evaluate a flexible wearable system for monitoring uterine contractions, assessing its feasibility and discussing potential for home use. The main contributions of this work are as follows: focusing on admission timing for primigravidas by identifying the onset of labor through contraction patterns; comparing data from our device with hospital-based tocodynamometers that operate on the same technical principles; proposing lightweight signal processing methods and time-domain feature extraction; developing a home-use prototype; and exploring the relationship between extracted signal features and clinical judgment.
Method
Overview
We designed a flexible wearable monitoring system that enables continuous and non-invasive monitoring of uterine activity when attached to the maternal abdomen. Although intended for home use, the prototype requires clinical validation to ensure its safety and stability. To this end, we conducted a validation study in a hospital setting, where contraction data were simultaneously collected from both the wearable system and the standard toco monitor for comparison. After validating the device's performance, the clinical data were used to extract features and develop a ML model for further analysis.
This study was conducted in a tertiary hospital in Shanghai, China. Maternity care in Shanghai is highly medicalised, with most antenatal assessments, including ultrasound, laboratory tests, and Cardiotocography (CTG), performed in hospitals by obstetricians and midwives. Community services provide always basic follow-up, and home self-monitoring is also limited by medical resource. Consequently, outside the hospital, women often rely on subjective assessment to judge contraction intensity and determine the timing of hospital admission.
The study focuses on low-risk primigravidas, who generally have less accurate perception of uterine contractions and longer labor duration compared with multiparous women. Our device is designed for low-risk women to provide quantitative home monitoring and support timely admission decisions. High-risk pregnancies still require hospital-based surveillance. In these cases, the device is not intended as the primary monitoring tool but may be used as a supplementary aid under professional guidance.
Guided by obstetric consensus and existing guidelines, the model identifies labor onset from contraction patterns and provides admission recommendations. The study comprises three core components: (a) Contraction monitoring system, (b) Clinical data collection experiment, and (c) Machine learning model for admission.
Contraction monitoring system
We developed a wearable uterine contraction monitoring device. As shown in Figure 1, the device is a compact 50-mm disc that incorporates a nine-channel flexible pressure sensor array with a sampling frequency of 10 Hz. The integration of flexible sensors allows for improved comfort and biocompatibility, enhancing both user experience and safety during monitoring.

Photograph of the wearable uterine contraction monitoring device and the 9-channel flexible pressure sensor array.
Figure 2 shows the 3D model of the device. The exploded view (Figure 2(a)) illustrates the internal components, including a 3D-printed resin shell, a printed circuit board (PCB) with a microprocessor and Bluetooth Low Energy (BLE) module for data preprocessing and transmission, a rechargeable battery, a pressure sensor, and a silicone pad for stable skin contact. The BLE module transmits data to a lightweight acquisition platform on the terminal, which supports real-time waveform visualization. The Overall view of the device (b) includes a fixed part, which can be secured to the participant's abdomen using a belt, a switch, and an indicator light. The light emits a soft blue glow to indicate device operation and has been shown to help reduce anxiety, as demonstrated in several other studies. 19 The bottom of the device (c) serves as the sensing area and consists of a flexible sensor array and a silicone pad. It detects uterine contractions from the abdomen, while the biocompatible silicone pad cushions pressure to ensure a comfortable data collection process.

3D model of the device. Exploded view of the device (a) illustrating the internal components. Top view of the device (b). Bottom of the device (c) is the sensing area.
We also developed a visual data collection app (Figure 3) to receive and display real-time data from the device during experiments. This allowed researchers to evaluate multi-channel uterine contraction signals and their feasibility.

The mobile data acquisition platform.
The mobile app was developed in Android Studio, using Java, Kotlin, and XML as the main programming languages. For communication, we used the stable FastBLE framework to enable low-power Bluetooth communication between the device and the phone. For data storage, we used Room with SQLite, which allows efficient and lightweight data reading and writing.
Inclusion and exclusion criteria
Participants were recruited on-site at Fudan University Obstetrics and Gynecology Hospital from admitted primigravidas with suspected labor. Eligible participants were 20‒50 years of age, had a singleton cephalic pregnancy, and were at least 37 weeks’ gestation. Individuals were excluded if they had pregnancy-related complications or severe underlying diseases that could affect normal participation. Participants with psychiatric disorders or impairments in cognition or language were excluded. These conditions may reduce the ability to understand instructions, correctly wear the device, or cooperate during monitoring, which could compromise the validity of the collected data, although they do not directly affect the technical accuracy of the device. After providing written informed consent, trained data collectors placed the wearable uterine contraction monitoring device and recorded real-time contraction signals using a mobile application.
Clinical data collection experiment
To evaluate the feasibility of the system for monitoring uterine contractions, the wearable device is secured to the maternal abdomen with a belt (Figure 4) to record contraction signals, which are simultaneously compared with signals from the standard hospital toco monitor. Pearson correlation coefficients are calculated to assess agreement between the two modalities (Figure 5). To minimize external influences on uterine activity, no medical interventions are performed during data collection, including cervical examinations, intravenous oxytocin administration, and epidural anesthesia. Each participant undergoes a minimum of 10 min of monitoring to capture at least one complete contraction cycle.

Clinical collection of uterine contraction signals, wearable device is fixed to the abdomen via a belt to monitor contractions.
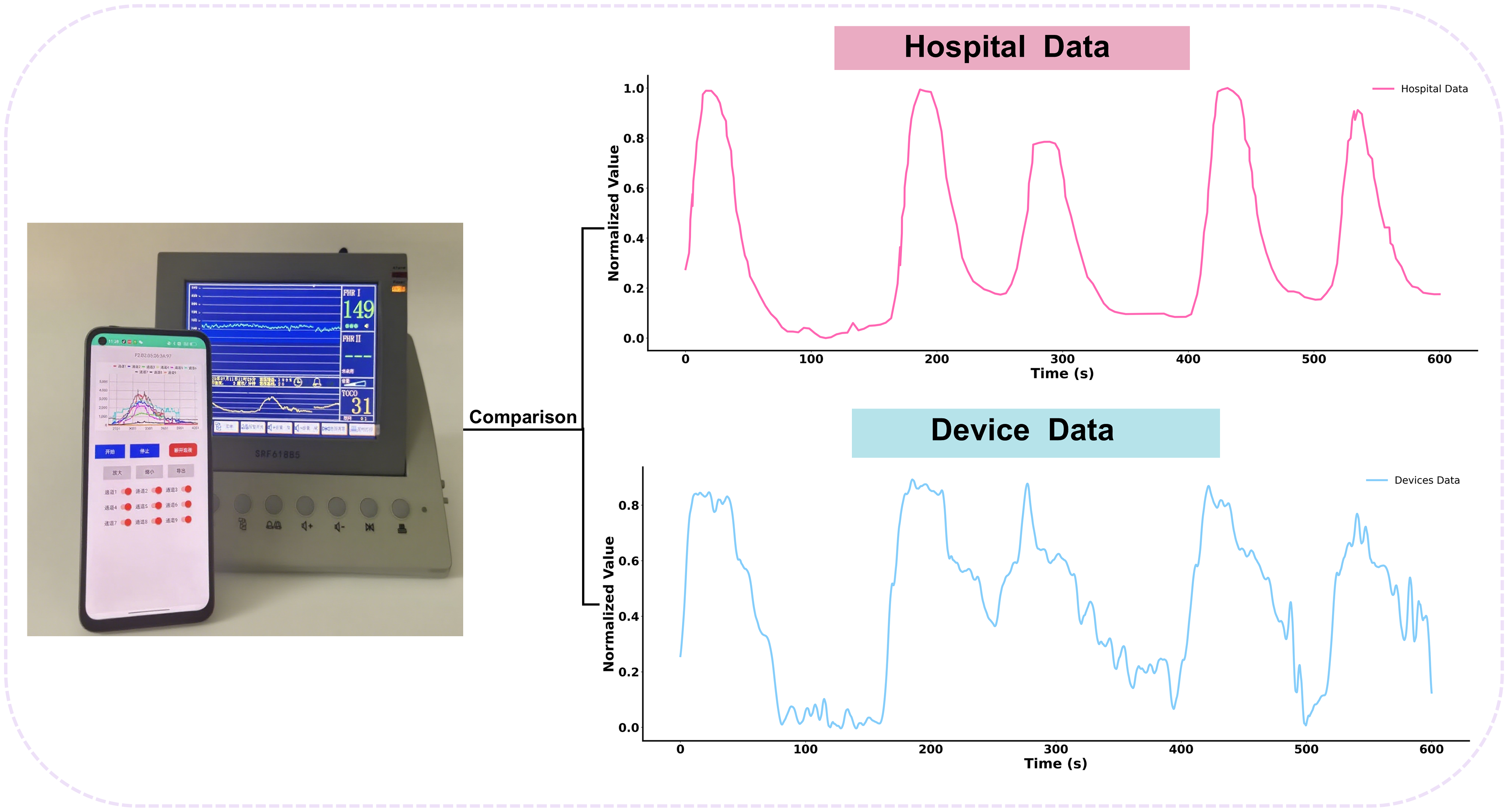
Comparison between hospital and device data with Pearson correlation coefficients.
Based on clinical experience and professional judgment, contractions occurring three or more times within 10 min, each lasting at least 30 s, or two contractions with markedly increased intensity indicating progressively regular patterns, are classified as recommended admission (RA). Contractions that do not meet these criteria, such as fewer than two contractions within 10 min, durations of less than 30 s, or low intensity without noticeable discomfort, are classified as deferred admission, as women in this group typically do not require immediate hospitalization. In clinical practice, some women present atypical contraction patterns. These include two to three or more contractions within 10 min with insufficient intensity, or fewer than two contractions accompanied by significant self-reported discomfort or a strong preference for hospital admission. To account for these cases, a selective admission (SA) category is defined for women with intermediate contraction patterns. Ultimately, all contraction data are categorized into three groups: RA, SA, and Deferred Admission.
Machine-learning model for admission
In the current system, the wearable device is responsible only for signal acquisition and basic preprocessing. Model inference is carried out on a local computer using Python. The end-to-end delay of the system, including acquisition, transmission, and processing, is at most about 1 s. This delay is acceptable for uterine contraction monitoring, as the rise, peak, and fall of a contraction usually change over tens of seconds and do not require millisecond-level feedback. Therefore, the present system architecture meets the real-time needs for prototype validation. Time-domain features were extracted for model training. Several traditional machine learning classifiers, including Random Forest (RF), Support Vector Machine (SVM), Extreme Gradient Boosting (XGBoost), Logistic Regression (LR), K-Nearest Neighbors (KNN), and Gradient Boosting Machine (GBM), were developed for contraction signal classification. In addition, deep learning models, including one-dimensional convolutional neural network (1D-CNN) and bidirectional long short-term memory network (BiLSTM), were implemented for comparison. All models were evaluated using 10-fold stratified cross-validation. Performance metrics, including accuracy, recall, precision, F1-score, and Area Under the Curve (AUC), were calculated. Feature importance for the traditional machine learning models was assessed using SHAP to identify the variables contributing to classification.
Ethical considerations
The study is conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of the Obstetrics and Gynecology Hospital of Fudan University (Approval No. [2022] 186). Written informed consent was obtained from all participants, and collected data and personal information were strictly protected.
Results
Participant condition
This study enrolled 82 low-risk primigravidas, aged 23‒38 years (mean = 29.8), with gestational weeks ranging from 37+3 to 40+1 weeks (mean = 39). A total of 104 uterine contraction recordings were obtained for subsequent analysis. The monitoring duration ranged from 10 to 70 min (mean = 20.3, SD = 10.7). Table 1 presents the demographic data of the participants.
Participants’ demographics.

Comparison of contraction signals with hospital monitors
This study compares the signals collected by the system with those obtained from the hospital toco, which is a Sunray fetal monitor (SRF618B5), and also uses a pressure sensor to record uterine contractions, with a measurement range of 0 to 100 mmHg and a sampling rate of 4 Hz. Due to differences in measurement ranges between the two devices, all raw signals are normalized using Min-Max normalization, mapping values to a range of 0 to 1. This procedure eliminates interference caused by differences in signal amplitude scales.
The normalized contraction signals from both systems are one-dimensional time-series signals, making the Pearson correlation coefficient an appropriate metric for evaluating signal similarity. This metric reflects the degree of linear correlation between two variables by calculating the covariance ratio to the product of their standard deviations. The coefficient ranges from −1 to 1, where values close to ±1 indicate a strong linear correlation, and values near 0 indicate weak correlation. The formula is as follows:
The six groups of samples were randomly selected from the overall dataset, each containing 10 min of uterine contraction monitoring data. The statistical results are reported in Table 2, showing a Pearson correlation coefficient range of 0.85-0.95 and an average correlation coefficient of 0.90. Key waveform features included a contraction onset time deviation of ≤0.83 s (95% CI −6.55 to 5.22) and a mean relative error of peak intensity below 15.8% (95% CI −4.2% to 35.8%). These results further confirm the equivalence of the uterine contraction monitoring device with hospital monitoring equipment. In Figure 6, the two contraction waveforms are consistent in overall pattern, particularly during the active phases of labor. The timing of contraction onset, peak, and duration is generally aligned between the wearable device and the hospital toco, demonstrating that the device can accurately capture both the temporal and amplitude characteristics of uterine contractions. Minor differences in signal amplitude are observed, but they do not significantly affect the overall waveform.

Correlation curve between wearable equipment and hospital toco data.
Correlation between wearable equipment data and toco data.

Preprocessing of uterine contraction data
The collected uterine contraction data underwent systematic preprocessing (Figure 7). Raw data were first sorted and deduplicated by timestamps, and missing values were imputed using the mean of three neighboring points. Signal segments separated by more than 60 s were considered interruptions and were automatically segmented. Uterine contraction signals are characterized as low-frequency, high-amplitude, rhythmic signals, with a typical duration of 30–90 s. 20 Early contractions are often irregular, gradually becoming more regular as labor approaches. 21 Because the signals are weak and may be affected by maternal and fetal movement, noise suppression is essential. The main energy of contraction signals is concentrated in the 0–0.1 Hz range, whereas respiration and other high-frequency components introduce interference. 22 Previous studies have shown that wavelet threshold denoising effectively reduces high-frequency noise while preserving the waveform integrity of uterine electrical activity 23 and other biometric signals. 24 In this study, discrete wavelet transform is applied for multiscale decomposition and reconstruction of the contraction signals. The uterine contraction pressure signal is decomposed into five levels using the Daubechies 3 (db3) discrete wavelet transform. High-frequency detail coefficients are denoised, with the threshold calculated from the median absolute deviation of each coefficient and dynamically adapted to the signal length. The low-frequency approximation coefficients are retained. The denoised signal is then reconstructed via the inverse wavelet transform.

Comparison of the signal with each step of processing: (a) raw data, (b) data denoising and (c) data detrending and baseline wandering removal.
To remove baseline drift and slow trends, Locally Estimated Scatterplot Smoothing (LOESS) 25 is applied with a window width parameter of frac = 0.1, and the signals are subsequently rescaled to have zero minimum values. During data augmentation, overlapping sliding windows of 10 min with a step size of 5 min are used. This coarse-grained segmentation aligns with clinical practice, more than 3 effective contractions within 10 min is a criterion for labor assessment, while ensuring that each sample preserved waveform variability.
In total, 104 contraction recordings were collected, with durations ranging from 10 to 70 min (mean 20.3). After preprocessing and window segmentation, 277 signal segments were obtained. Each segment was resampled to 1 Hz using linear interpolation, resulting in 600 points per 10-min window. Based on waveform characteristics and prior literature, 26 11 time-domain features were extracted: mean, standard deviation (std), skewness, kurtosis, maximum value (max_val), root mean square (rms), amplitude range, signal energy area, peak amplitude, peak count, and active duration. All features were standardized using Z-score normalization to ensure comparability for model training and evaluation.
Significant differences were observed among the machine learning models in this study (Table 3). Ensemble models (XGBoost, RF, GBM) generally outperformed traditional linear models (LR) and instance- or kernel-based models (KNN, SVM) across multiple metrics. XGBoost achieved the highest performance, with an accuracy of 0.78, precision of 0.77, recall of 0.75, F1-score of 0.74, and AUC of 0.89. Its gradient boosting and regularization mechanisms likely contributed to stable performance when handling high-dimensional nonlinear features and imbalanced classes. RF showed similar results (accuracy = 0.77, F1 = 0.73, AUC = 0.89), with a modest trade-off between precision and recall, while GBM performed slightly lower (accuracy = 0.75, AUC = 0.88), possibly due to parameter sensitivity and handling of sparse features. LR showed moderate performance (accuracy = 0.71, AUC = 0.86), and SVM (accuracy = 0.70, AUC = 0.85) and KNN (accuracy = 0.66, AUC = 0.84) performed less well, likely reflecting challenges in high-dimensional space and sensitivity to noise.
Performance evaluation of the classification model.

For deep learning models, 1D-CNN outperformed BiLSTM on all metrics (Table 4), suggesting that convolutional networks are more effective at capturing local temporal patterns. BiLSTM did not fully learn long-term dependencies with the current dataset and short time-series segments, likely causing undertraining or underfitting. Although 1D-CNN showed slightly higher performance than KNN and LR on some metrics, its overall performance remained lower than that of tree-based models (Table 3), likely due to limited sample size and class imbalance. The input features, processed using statistical and frequency-based methods, captured key information, which tree models could exploit more efficiently. Overall, traditional machine learning models performed better on engineered features, and 1D-CNN was superior to BiLSTM. However, as the study progresses and the dataset grows in size and becomes more balanced, deep learning models may achieve superior performance.
Deep learning model results.

In Figure 8, Radar Plot 27 was employed to compare the performance of different machine learning models across multiple evaluation metrics. Each model was represented as a polygon, with its vertices corresponding to the respective metric values. The plot showed that all models performed similarly in accuracy, precision, recall, and F1-score, with no substantial differences observed. In contrast, AUC values were consistently higher across all models. Accuracy, precision, and recall are calculated using a specific threshold to determine whether a uterine contraction is considered positive, and their values can be influenced by the choice of threshold and the sample distribution. 28 In contrast, AUC reflects the model's ability to discriminate between different types of uterine contractions across all possible thresholds, providing an overall measure of discriminative performanceFigure 9. 29
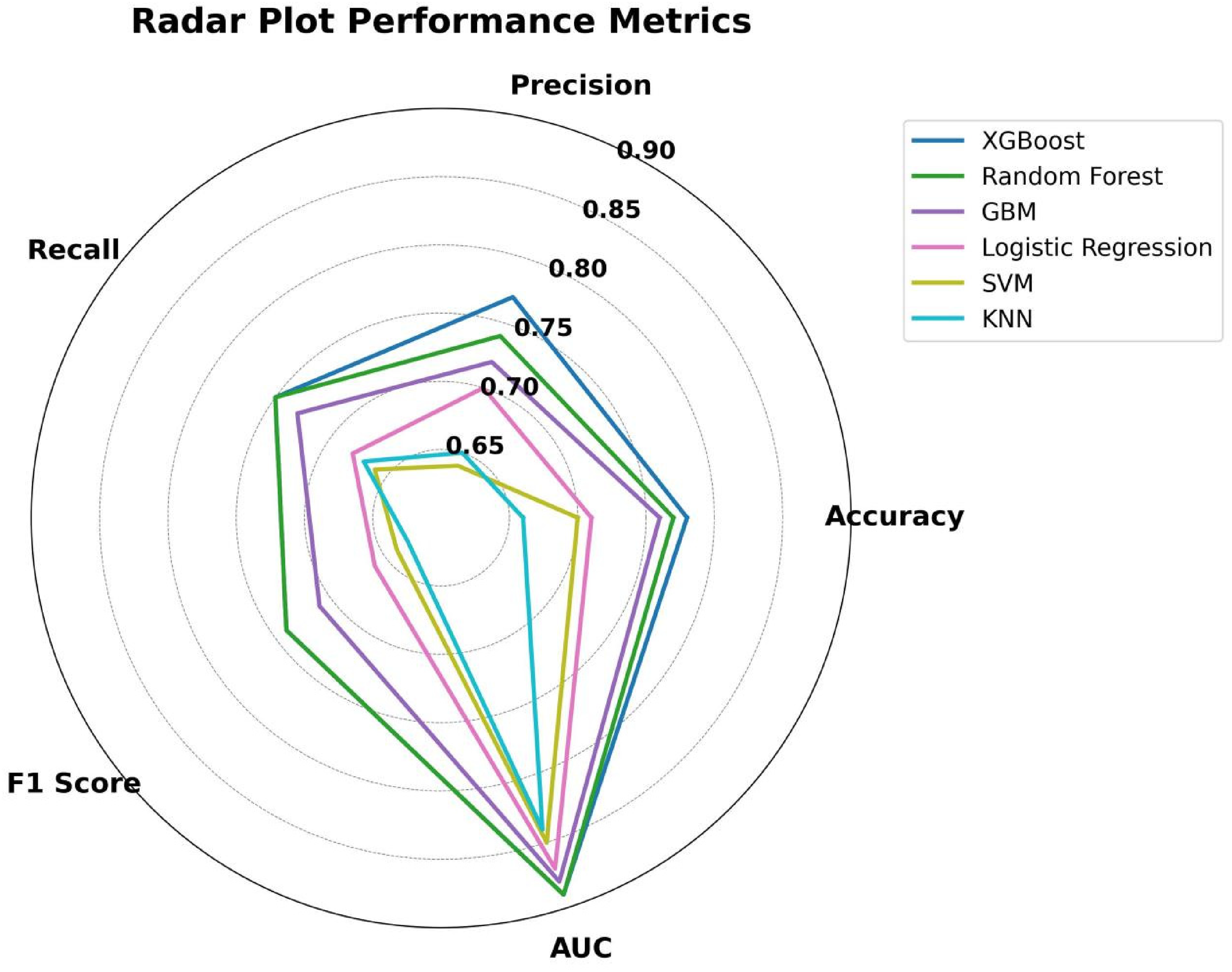
Radar Plot of ML Performance Metrics.

Confusion matrices of different models, 0 represents RA, 1 represents SA, 2 represents DA: (a) confusion matrix of the GBM, (b) confusion matrix of the KNN, (c) confusion matrix of the LR, (d) confusion matrix of the RF, (e) confusion matrix of the SVM and (f) confusion matrix of the XGBoost.
The classification performance of the XGBoost model (Table 5) indicated that the RA achieved the highest performance, with an accuracy of 0.87, a recall of 0.84, and an F1-score of 0.85, suggesting that the model can reliably identify participants requiring immediate hospital admission. The DA also performed robustly, with an accuracy of 0.74, a recall of 0.78, and an F1-score of 0.75. In contrast, the SA showed relatively lower performance, with an accuracy of 0.70, a recall of 0.63, and the lowest F1-score of 0.62. The confusion matrix further illustrated the prediction distribution of the model across different classes (Figure 9(f)). For the RA, most predictions were correct (n = 123), although 16 cases were misclassified as DA. For the SA, 29 cases were correctly identified, while 18 cases were misclassified, indicating that this category was relatively more challenging to classify. For the DA, 65 cases were correctly predicted, with eight misclassified as RA and 10 as SA.
Classification results of XGBoost for each class.

SHAP-Based feature contribution
Accurate recognition of uterine contractions requires identifying four characteristic phases of the contraction waveform: ascending, peak, descending and interval phases. 30 Time-domain features, such as mean, standard deviation, amplitude, and duration, are used to quantify the signal morphology of these phases.
To enhance the model's reliability and interpretability, we used the SHAP method to identify the key features that distinguish different contraction categories and linked them to the core physiological indicators that obstetricians use to assess contractions.
In Figure 10, SHAP analysis based on the XGBoost model ranked features according to their mean absolute SHAP values, providing insight into each feature's contribution to the classification. Each point represents a single sample's SHAP value, with red indicating high feature values and blue indicating low values. The horizontal position of each point reflects the feature's positive or negative influence on the model's output.

SHAP bee-swarm plot of the XGBoost.
Different contraction categories are influenced by distinct key features. The analysis showed that the feature combinations for each category are consistent with clinical diagnostic logic. Specifically, the RA category was mainly driven by features such as kurtosis and signal energy area, which reflect the waveform sharpness and overall energy that clinicians often observe. The key features for the SA category include kurtosis, std, and rms These features correspond to how clinicians assess contraction rhythm, amplitude, and effective working time to judge whether the labor has entered the active phase. The DA category was primarily based on mean, rms, and std, focusing on amplitude features. The SHAP-identified features linked to the clinical diagnostic criteria used by obstetricians, ensure that our model is not just a predictive tool but also an analytical tool that helps doctors quickly locate and interpret key physiological changes.
Discussion
Main results
This study proposed and validated the Flexible Wearable System, and also developed a machine learning-based classification model using the collected contraction data. The system enabled accurate acquisition and visualization of contraction signals, while running a contraction classification model that linked the recorded signals to clinically recognized contraction features and hospital admission categories.
In a clinical setting, signals collected by the device were compared with those from a toco, and normalized comparison curves were generated. Results from six random samples showed Pearson correlation coefficients ranging from 0.85 to 0.95 (mean r = 0.90). Further visual inspection revealed that the two contraction waveforms were generally consistent in overall fluctuation patterns, particularly during active contraction phases, with key features such as onset time, peak, and duration closely aligned.
The time deviation of the contraction onset points in specific waveforms was controlled within ≤0.83 s (95% CI −6.55 to −5.22), indicating that the device captures the onset of contractions nearly synchronously with hospital-based fetal monitoring, meeting the temporal precision required for labor management. In addition, the mean relative error of peak intensity was below 15.8% (95% CI −4.2% to 35.8%), suggesting that although signal amplitude differences existed, this error range was insufficient to substantially affect clinical interpretation of contraction strength.
To ensure clean and stable signals, the raw signals were preprocessed using wavelet threshold denoising and baseline correction. Wavelet denoising suppressed high-frequency noise through multi-scale time—frequency decomposition while preserving key signal features. Baseline correction was applied to eliminate signal drift and improve signal stability for subsequent analysis. 31
In the third stage of the study, time-domain features of the contraction waveform were used to build multiple machine learning models, including common traditional algorithms and two representative deep learning models, for a three-class classification task. Evaluation results indicated that the XGBoost model performed best overall (accuracy = 0.78; recall = 0.75; precision = 0.77; F1-score = 0.74; AUC = 0.89), demonstrating not only improved overall classification accuracy but also a balanced performance across different risk categories. Specifically, the recall was higher in the high-risk RA category, indicating the model's ability to capture most patients who required timely admission and thus reduce the risk of missed cases. In the low-risk DA category, precision was higher, suggesting fewer false positives when identifying patients who did not urgently require admission, thereby avoiding unnecessary medical interventions.
The RF model ranked closely behind XGBoost, with slightly lower performance across most metrics, yet still demonstrated strong classification capability. Notably, although both XGBoost and RF exhibited excellent AUC values, other specific metrics such as accuracy, precision, and recall were slightly lower due to overlapping class distributions and sample imbalance. Relying solely on AUC is insufficient for comprehensive evaluation of multiclass clinical decision models; interpretation should also consider confusion matrices and class-specific performance metrics. 32
LR and SVM faced challenges in handling contraction waveform features. In this study, multiple time-domain features with complex nonlinear relationships were extracted. Under such conditions, the linear assumptions of logistic regression limited its ability to capture intricate patterns. 33 Although SVM maps features into a high-dimensional space via kernel methods, its classification performance can still be affected by complex nonlinear relationships and limited samples. 34 In contrast, ensemble learning methods such as XGBoost can more effectively model these nonlinear relationships, improving both the accuracy and robustness of multiclass classification. Overall, these findings align with existing literature demonstrating XGBoost's advantages in handling class-imbalanced data, complex signal features, and nonlinear relationships. 35
Comparison with previous work
Existing wearable contraction monitors, such as Novii, 17 Bloomlife, 36 and Keyar CM, 37 primarily rely on electrodes to capture EHG signals for monitoring uterine activity. 38 This study applies a pressure-sensing principle and focuses on admission timing, representing a transition from signal acquisition to clinical decision support. We previously explored contraction-based decision support and developed corresponding monitoring devices. Compared with previous study, 39 this study introduces a multichannel flexible thin-film sensor array, enabling distributed sensing of uterine tension and providing a real-time visualization interface to facilitate rapid verification of signal quality by clinical personnel. The sensing and processing modules are integrated into a portable circular device, enhancing wearability and feasibility. In addition, a SHAP interpretability framework is applied to address imbalance class and complex contraction patterns, clarifying the contribution of key features such as rms, std, and kurtosis. The study also identified a limitation in the classification task, with the SA category showing a relatively low recall, primarily due to signal instability and the ambiguous waveform boundaries of this class. These limitations reflect the inherent constraints of both the hardware and signal characteristics, including the finite sensitivity and resolution of wearable sensors, potential signal noise and artifacts, and variability in signal acquisition due to differences in maternal body habitus or fetal positioning. These factors are largely unavoidable and stem from intrinsic physiological and technological conditions. 40
Limitations
This study is a single-center validated study with several obvious limitations. Due to the limited sample size, the study may be subject to information bias and center-specific effects. 41 Specifically, although the device used in this study was primarily designed for home and community settings, the experiment was conducted in a hospital environment to allow for an initial evaluation of device function and model performance. For a home-use device, multi-center studies are essential, as they can cover different home conditions, user operation habits, and individual differences such as BMI, gestational age, and fetal position. These factors may influence signal quality and model performance. Therefore, future studies will focus on experiments conducted in diverse home or community environments, collecting more representative data and performing comparative analyses to further improve the model's applicability and stability.
In addition, the clinical labels were based on manual interpretation and subjective recording by clinicians, and the labeling was cross-sectional. As a result, it did not capture the full dynamics of uterine contractions from admission to delivery. The limited sample size also constrained the performance of more complex deep learning models. Although XGBoost achieved moderate accuracy, it is still not sufficient for time-based predictions, such as estimating safe waiting time at home. Moreover, the study did not integrate multimodal information, including fetal heart rate, fetal movement, electrical uterine signals, or maternal physiological and behavioral data. This limits the model's ability to consider all factors related to contraction monitoring.
Finally, this study did not include the development of a complete mobile application, and the system remains in an early validation stage. Future work will focus on building a mobile application that integrates data collection, processing, and result presentation, ultimately forming a more complete home monitoring system for pregnant women.
Conclusion
This study presented a flexible wearable system for monitoring uterine contractions. The system provided real-time data that could assist doctors in evaluating labor progression and support clinical decisions, potentially reducing reliance on subjective assessments. For midwives, it offered additional information for monitoring labor, which may help in routine workflow management. For pregnant women, the device enabled home-based monitoring, offering supplementary data to consider when deciding on hospital admission. Overall, the system served as an additional tool to support clinical observation and decision-making.
Footnotes
Abbreviations
Acknowledgments
The authors wish to express their appreciation to their colleagues and research partners for their valuable collaboration, as well as the participating pregnant women for their trust and contribution to this study. We also express our gratitude to the medical staff who provided support and assistance.
Consent for publication
All authors have approved this manuscript for publication. This manuscript has not been previously published.
Contributorship
Study objectives: Xin Xu, Li Gong. Data collection: Li-hua Xu, Huan Liang. Data analysis: Xin Xu, Li Gong, Ji-Chao Leng. Critical review and approval of manuscript: Yan Ding, Zhuo Zou. All authors have read and approved the final manuscript. Professor Ding and Professor Zou are the corresponding authors and guarantors of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Medical Engineering fund of Fudan University (yg2025-general-23). As part of funding support for the Medical-Engineering Interdisciplinary Program, which aims to promote deep integration between medicine and engineering and to foster multidisciplinary innovation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data generated or analyzed during this study are included in this published article.