
Abstract
Objective
Considering an increasing number of patients bring online health knowledge, as a key form of digital health, to discuss with their doctors, this study aims to construct a model to examine the relationship among perceived improved coping ability (PICA, reflecting patients’ self-efficacy) and physician-patient concordance (PPC), negative and positive doctor-patient trust, as well as doctor-patient relationship (DPR) in the context of diverse online information sources.
Methods
This cross-sectional survey was conducted online. Participants were recruited through convenience sampling among netizens across China. Through a convenience sampling method, an online survey was conducted among netizens in China. A total of 286 and 1041 valid questionnaires were distributed from May 6, 2022, to May 8, 2022 and February 27 to March 6, 2025, respectively. SPSS 26.0 was used for data analysis, while Smart PLS 4.0 was employed for both model building and testing.
Results
Compared with individuals utilizing content-sharing and short video platforms, all hypotheses were only supported in individuals utilizing social interaction platforms. PICA was positively correlated with PPC (β = .330; P < .001) and positive doctor-patient trust (PDPT) (β=.204; P = .030). Additionally, PPC was correlated with doctor-patient trust. PDPT significantly enhanced the DPR (β = .497, P < .001), while NDPT significantly undermined it (β = -.373, P < .001). PPC played a partial mediating role between PICA and doctor-patient trust. Doctor-patient trust played a mediating role between PICA and DPR. PPC and doctor-patient trust have a serial mediation effect between PICA and DPR.
Conclusion
All proposed hypotheses were confirmed only among individuals who primarily used social interaction platforms (such as WeChat, QQ, and Weibo) for health knowledge. The strict review mechanisms of these social media platforms may be crucial in ensuring the quality of health information.
Introduction
Background
After the outbreak of COVID-19, the Chinese government swiftly took action to address the crisis, which included the use of official social media for information dissemination. 1 This rapid organizational and information management capacity relies on China's centralized public health governance system, which coordinates resources through central leadership and local collaboration, while enforcing stringent review procedures for health information release to ensure accuracy and reliability. 2 Within this institutional framework, the processes of information review, dissemination, and updating are highly standardized, enabling official information to rapidly reach populations across regions, reduce distortion and delay, and strengthen public reliance on authoritative sources. 3 During this period, there was a significant enhancement in public health self-consciousness, accompanied by an increased focus on health knowledge. 4 Health knowledge related to COVID-19, as well as other health topics, proliferated rapidly. Despite the surge in health knowledge available on social media, the quality of it did not diminish. This achievement is partially attributed to the collaborative efforts of the Chinese government. In China, government agencies disseminated COVID-19 fact-checking information dynamically through their official social media accounts.5,6 Studies have shown that during the early stage of the COVID-19, official social media accounts played a crucial role in disseminating authoritative information about COVID-19, thereby mitigating public uncertainty. 7 In addition, studies have indicated that during the COVID-19, government agencies, independent media, civic organizations, social groups, social media platforms, and technology companies actively participated in fact-checking activities.5,8,9 Social media platforms such as Tencent and Facebook integrated fact-checking mechanisms into their systems.
Meanwhile, Chinese doctors played a central role in health information dissemination and in maintaining doctor–patient relationships. 10 Within China's centralized healthcare system, doctors not only undertook clinical responsibilities but also exerted significant influence in the dissemination of public health information. 11 During COVID-19 period, active participation by Chinese doctors in health communication and their efforts to debunk misinformation helped the public discern credible information, thereby enhancing the overall quality of the available content. For example, the program “News 1 + 1” adopted a dialogue format between hosts and experts to address the public's most pressing concerns about the COVID-19 on a daily basis; it played an important role in both knowledge dissemination and rumor refutation. 12 Accurate information provided by trusted clinicians and scientists helped curb the spread of misinformation that could be detrimental to public health. 12 Consequently, the overall quality of health knowledge on social media may have been generally high after the outbreak of COVID-19. Studies have shown that the dissemination of high-quality information through social media can effectively guide the public to adopt positive health behaviors. 13 It is likely that higher-quality online health information aligns with the knowledge and guidance provided by doctors, 14 helping the public better understand medical advice and enhancing their trust in doctor. A study has shown that high-quality online health information collected by patients correlates positively with their adherence to medical advice. 14
In addition, the COVID-19 pandemic placed both doctors and patients in a unique “exceptional” state. Within the framework of a nationally centralized and unified prevention and control system, Chinese healthcare professionals not only undertook overwhelming clinical treatment responsibilities, but also demonstrated extraordinary professional dedication, voluntarily placing themselves at risk and working under extreme pressure to treat COVID-19 patients. 15 Studies have shown that the professionalism of frontline healthcare workers has reshaped public perceptions of Chinese doctors. 16 At the same time, media reports and praise for frontline medical staff have further enhanced public understanding and support for healthcare professionals in the COVID-19 period. 16 During this period, both doctors and patients in China reported higher ratings of the doctor-patient relationship compared to before the COVID-19 period. 17 Consequently, built on doctor-patient trust, 18 the doctor-patient relationship rapidly evolved into a community with shared future for doctor-patient. 19 This relationship was characterized by patients having a deeper understanding of doctors, a greater willingness to adhere to medical advice, and increased solidarity with physicians.20–22 Therefore, in this environment of intergroup trust, there remains a lack of clear understanding of how health knowledge acquired by patients through social media affects the doctor-patient relationship.
Although doctors often prioritize rational and scientific communication within the doctor-patient relationship, overly specialized medical terminology can create gaps in public understanding and potential misconceptions. In the Chinese healthcare system, this issue is particularly pronounced. Due to limited consultation time and the traditional physician-centered communication model, doctor-patient interactions often lack adequate information exchange and bidirectional dialogue.23–25 Against this background, an increasing number of patients now seek health knowledge from social media in order to compensate for information asymmetry. 26 Nevertheless, the quality of online health information varies widely, 27 and the public has limited ability to discern the authenticity of information. It remains debated whether incorporating this information into shared decision-making is beneficial to the doctor-patient relationship.28–30 Our research group found that the public's enhanced health knowledge contributed to improvements in the doctor-patient relationship during the COVID-19 period. 17 Notably, the primary channels for accessing health knowledge during this period were the internet and, especially, social media. 31 Public adherence to home isolation and increased free time facilitated greater exposure to and effective acquisition of COVID-19-related health knowledge. 32 This phenomenon not only provides an opportunity to study how health information on social media affects doctor-patient relationships in this unique period, but also highlights its practical significance within the context of the Chinese healthcare system. Furthermore, using CiteSpace for scientometric analysis, our team identified that the uncertainties surrounding social media information, coupled with the unique characteristics of the COVID-19 pandemic, have made health communication on social media and doctor-patient relationship research emerging hotspots. 33 Based on the keywords and burst terms identified through the CiteSpace scientometric analysis, combined with descriptive analysis results from the survey questionnaire, our research group preliminarily proposes a potential pathway: social media health information quality (perceived source quality and information quality) → perceived information asymmetry → doctor-patient communication → physician-patient concordance → doctor-patient trust → doctor-patient relationship. 33 Notably, within this potential mechanism, the quality of information may not only influence patients’ expectations and experiences of doctor-patient communication but may also further shape the dynamics of doctor-patient relationships by affecting patients’ psychological preparation and self-efficacy prior to medical consultations.
Building on this, perceived improved coping ability with physicians was introduced as a relatively novel concept in our study to reflect patients’ increased confidence and competence to cope with physicians after accessing online health information prior to their medical consultations. 34 For a long time, the Chinese healthcare system has been characterized by structural issues such as professional knowledge asymmetry between physicians and patients and limited outpatient consultation time, leaving patients with insufficient voice and autonomy during clinical encounters.23–25 Against this backdrop, during the COVID-19 period, social media platforms served as major sources of health information, including WeChat, QQ, Weibo, Zhihu, Tieba, Xiaohongshu, Douyin, Bilibili, and Kuaishou. 35 They enable patients to proactively acquire relevant knowledge prior to medical consultations, 36 and may partially mitigate information asymmetry and enhance patients’ self-efficacy. However, the types of information disseminated via social media are complex and diverse in purpose, 35 and the quality of health information varies considerably across platforms. 35 Consequently, patients’ perceived improved coping ability may also differ depending on the platform from which they obtain information.
Therefore, this study aimed to evaluate differences among patients obtaining health knowledge from various social media platforms in terms of perceived improved coping ability with physicians, physician-patient concordance, doctor-patient trust (including positive and negative trust), and the doctor-patient relationship within the context of the COVID-19 pandemic in China. Using patients’ perceived improved coping ability with physicians as the central starting point, the study further investigated the potential pathways through which it may influence doctor-patient relationships via physician-patient concordance and doctor-patient trust. Moreover, during the exceptional circumstances of COVID-19, doctor-patient relationships were relatively harmonious; however, in future routine healthcare settings, such relationships may be less favorable and face greater challenges. This study thus not only contributes to understanding the potential of high-quality health information on social media to promote doctor-patient relationships during the COVID-19 pandemic but also provides insights for improving such relationships in routine healthcare contexts.
Theoretical framework
Asymmetric information theory refers to the situation in market economic activities that individuals with more information are at a relative advantage, while those with limited information are at a relative disadvantage. It suggests that sellers have more knowledge about the goods compared to buyers in the market, and the party with more information can benefit by providing reliable information to the party with limited information. 37 The doctor-patient relationship is an interpersonal relationship characterized by information asymmetry. 38 In traditional Chinese healthcare relationships, physicians typically possess greater medical knowledge and professional skills, while patients, as laypersons, are in a relatively disadvantaged position. This disparity in knowledge not only tends to undermine patients’ agency during clinical encounters but also contributes to a certain degree of estrangement in doctor-patient relationships. 39 Within the Chinese healthcare system, the problem of information asymmetry is particularly pronounced. Due to the concentration of medical resources in large cities and tertiary hospitals, physicians commonly face structural constraints such as limited consultation time and a disease-centered communication model, making it difficult for patients to receive adequate explanations and engage in bidirectional interactions within the limited consultation period,23–25 thereby exacerbating imbalances in doctor-patient relationships.
With the development of information technology, the long-standing pattern of information asymmetry in Chinese doctor-patient relationships is gradually being challenged. The mobilization of communication medium has created favorable technological conditions for health communication. The public's online searching for health information and demand for reliable health information are increasingly growing. 40 Compared with traditional media, social media offers distinct advantages in the dissemination of health information. For example, videos make health knowledge more visual and concrete, which can save patients’ reading time and facilitate their understanding. However, health information can be misinterpreted during the dissemination process. The misinterpretation can hinder the effective dissemination of health information and even create new barriers to doctor-patient communication. 41 In addition, information overload can result in adverse effects, such as fear or anxiety. 41 In the process of altering the traditional pattern of information asymmetry, health information on social media not only provides opportunities to improve doctor-patient relationships but also poses new challenges.
Notably, there is a positive correlation between the high quality of online health information collected by patients and their adherence to medical advice. Higher quality online health information is more likely to align with the doctors’ knowledge and guidance. 14 A study has shown that medical education and shared decision-making can reduce the information gap between doctors and patients. 42 Additionally, an increase in patients’ health knowledge levels may enhance their confidence and ability to engage in shared decision-making. Improved decision-making abilities enable them to participate in shared decision-making more effectively and to provide reasonable treatment recommendations. 43 Within the framework of this study, such enhancement in confidence and capability is conceptualized as “perceived improved coping ability with physicians,” referring to the increase in patients’ perceived ability to manage interactions with physicians and their self-efficacy in communication during medical consultations through the acquisition of online health knowledge. The enhancement of perceived coping ability with physicians not only reflects a reduction in information asymmetry but may also serve as a key psychological mechanism driving improvements in the quality of physician-patient interactions.
However, online health information does not always exert positive effects. Information overload, misinterpretation, and even false content may exacerbate patients’ anxiety and misunderstandings. 35 When online health information contradicts the advice given by doctors, patients may question their physicians. 44 Many patients tend to treat unverified online health information as gospel, leading to unrealistic expectations regarding treatment. 45 Within the context of Chinese medical culture, the authoritative status of physicians makes such conflicts particularly sensitive, as patients both respect physicians’ professional judgment and may develop unrealistic expectations due to excessive reliance on online information.
Against this backdrop, physician-patient concordance may serve as a key link between information asymmetry and doctor-patient relationships. It refers to patients discussing the treatment with their doctors equally and ultimately reaching an agreement on medical diagnosis and treatment with their doctors. 46 To some extent, physician-patient concordance is the opposite of information asymmetry. When patients’ perceived improved coping ability with physicians is enhanced through health information obtained on social media, they are more likely to actively express their views during consultations, understand physicians’ recommendations, and reach consensus with physicians. Accordingly, such consensus not only fosters patients’ trust in physicians but also provides a solid foundation for the improvement of doctor-patient relationships. Therefore, asymmetric information theory can better explain the role of physician-patient concordance between perceived improved coping ability and doctor-patient relationship after patients obtain online health information.
Research model and hypothesis development
Studies have shown that the quality of online health information positively influences physician-patient concordance. 14 Within the Chinese healthcare system, physicians commonly face structural constraints such as limited consultation time and a disease-centered communication model, making it difficult for patients to fully express their needs and comprehend physicians’ recommendations within the limited consultation period.23–25 On the one hand, when the quality of health knowledge on social media is high, patients can better understand their health conditions and treatment options prior to medical consultations, clarifying their purpose for the clinic visit and the questions they need to ask. This thorough preparation may help patients more readily reach a consensus with physicians during communication. On the other hand, by obtaining health information through social media, patients are able to articulate their health conditions and needs more clearly and accurately, thereby facilitating smoother communication with physicians and enhancing their ability to understand and follow medical advice. Therefore, hypothesis one (H1) proposes that perceived improved coping ability with physicians is positively correlated with physician-patient concordance.
Patients may acquire more health knowledge through social media. Patients who perceive themselves as adequately informed and who feel that their physicians have explained their condition tend to show higher levels of trust in their physicians. 47 Additionally, searching for health information online not only enhances patients’ health knowledge but also encourages patients’ greater involvement in health care and decision-making. 48 Within the context of China's unique medical culture, patients generally respect physicians’ professional authority; however, those with sufficient information and thorough preparation for consultations are more likely to understand physicians’ explanations, actively participate in treatment decisions, and exhibit higher levels of trust. Studies have shown that patients who engage in decision-making to the fullest extent possible are more likely to trust their physicians compared to those who do not participate in decision-making. 49 Therefore, perceived improved coping ability with physicians may positively influence positive doctor-patient trust. Therefore, hypothesis 2a (H2a) proposes that perceived improved coping ability with physicians is positively correlated with positive doctor-patient trust.
Positive and negative doctor-patient trust are not simple opposites, they also include neutral or uncertain attitudes. Lewicki et al. (1998) proposed that trust and distrust are independent yet related constructs. 50 Recent research further supports that trust and distrust are distinct constructs, not located at opposite ends of a continuum, and can exist simultaneously. 51 Trust is defined as a positive expectation regarding others’ behavior, whereas distrust reflects a negative expectation of others’ behavior, conceptualized as a form of negative trust.50,52 Accordingly, the present study distinguishes between positive doctor-patient trust and negative doctor-patient trust. Given the power asymmetry in doctor-patient relationships, doctor-patient trust is fragile.53,54 Patients with neutral or uncertain attitudes toward physicians are more likely to experience a decrease in trust if their healthcare encounters are unsatisfactory. Specifically, after acquiring health knowledge from social media, patients may bring this information into consultations. A lack of effective communication between physicians and patients can lead to a loss of doctor-patient trust. 55 The less health information patients obtain through social media, the less prepared and skilled they may be in communicating with physicians, which could reduce the quality of medical services, impacting their satisfaction with care and trust in their physicians. Therefore, hypothesis 2b (H2b) proposes that perceived improved coping ability with physicians is negatively correlated with negative doctor-patient trust.
The binary concordance in doctor-patient interactions refers to the degree of agreement between the physician's and patient's views on diagnosis and treatment, reflecting the extent to which mutual understanding has been achieved through communication. 56 Reaching a consensus between physicians and patients enhances interpersonal trust and group trust. 33 On one hand, a high level of consensus regarding disease understanding, treatment plans, and expected outcomes helps patients perceive the physician's professionalism and care, thereby strengthening the patient's positive trust in the physician. On the other hand, when the physician's treatment recommendations align with the patient's expectations, the patient feels a heightened sense of safety with the physician. Therefore, hypothesis 3a (H3a) proposes that physician-patient concordance is positively correlated with positive doctor-patient trust.
The factors influencing physician-patient discordance include the possibility that physicians may overestimate patients’ understanding of treatment plans, fail to accurately recognize patients’ health literacy levels, 57 or underestimate patients’ needs. 58 These cognitive biases may lead physicians to inadequately consider patients’ actual situations when formulating treatment plans and anticipating treatment outcomes, thereby affecting the attainment of physician-patient concordance. When patients disagree with or feel dissatisfied about the treatment plans or expected outcomes proposed by their physicians, they may perceive that the physician has not fully understood their conditions and needs, or they may doubt the physician's professional competence and decision-making. This disagreement and dissatisfaction can lead to negative evaluations of the physician by the patient. Therefore, hypothesis 3b (H3b) proposes that physician-patient concordance is negatively correlated with negative doctor-patient trust.
By obtaining more health information through social media, patients are better prepared for the medical process, leading to smoother communication with physicians. These changes may facilitate a higher degree of agreement between patients and physicians regarding disease understanding, diagnosis, and treatment decisions. The quality of physician-patient interactions is expected to foster trust. 59 Previous studies have also confirmed a strong and significant relationship between better physician-patient concordance and doctor-patient trust.33,60 When discrepancies or inconsistencies arise between patients and physicians, patients may experience dissatisfaction or skepticism towards their physicians. Therefore, hypothesis 4a (H4a) proposes that physician-patient concordance plays a mediating role between perceived improved coping ability with physicians and positive doctor-patient trust; hypothesis 4b (H4b) proposes that physician-patient concordance plays a mediating role between perceived improved coping ability with physicians and negative doctor-patient trust.
Building trust is a critical step in developing a high-quality doctor-patient relationship. 59 Physicians’ trust in patients and patients’ trust in doctors are intrinsically linked and essential to a collaborative healthcare partnership. 61 When patients have sufficient trust in their physicians, they are more likely to engage positively with them, cooperate with treatments, and maintain an optimistic attitude toward treatment outcomes. This positive interaction and attitude, in turn, enhance patients’ trust and satisfaction with their physicians, creating a virtuous cycle. Therefore, hypothesis 5a (H5a) proposes that positive doctor-patient trust is positively correlated with doctor-patient relationship.
When patients’ trust in doctors is low, they may question their physicians’ decisions and abilities, and they are more likely to attribute unsatisfactory medical outcomes to physicians’ mistakes or irresponsibility. Patients who distrust their physicians may doubt the motivations of physicians and could even act aggressively during interactions. 62 Consequently, negative doctor-patient trust may delay or hinder the development of the doctor-patient relationship. Therefore, hypothesis 5b (H5b) proposes that negative doctor-patient trust is negatively correlated with doctor-patient relationship.
Upon accessing online health information, individuals tend to take greater responsibility for their health and show interest in being more actively involved in health-related decisions. 63 When patients are willing to seek additional information from physicians to better understand treatment principles, they often build a stronger foundation of doctor-patient trust. 64 One study found that 85.2% of physicians believe that online health information can have both positive and negative impacts on the doctor-patient relationship. 65 A positive doctor-patient relationship is more likely to be established when patients’ perceived improved coping ability with physicians and positive doctor-patient trust increased during medical encounters. However, if the interaction around online health information in the consultation room is negative, such as when patients feel overlooked, misunderstood, or perceive information asymmetry, this may lead to an increase in negative evaluations of doctors, thereby strengthening negative doctor-patient trust. Therefore, hypothesis 6a (H6a) proposes that positive doctor-patient trust plays a mediating role between perceived improved coping ability with physicians and doctor-patient relationship; hypothesis 6b (H6b) proposes that negative doctor-patient trust plays a mediating role between perceived improved coping ability with physicians and doctor-patient relationship.
Physician-patient concordance is essential for mutual understanding and treatment satisfaction between patients and physicians. Specifically, physician-patient concordance affects the development of patients’ trust in doctors, which in turn influences the overall quality of the doctor-patient relationship. Conversely, significant differences between patients and physicians on critical issues may lead to patients’ negative evaluations of the physician, subsequently impacting the doctor-patient relationship adversely. Therefore, hypothesis 7a (H7a) proposes that positive doctor-patient trust plays a mediating role between physician-patient concordance and doctor-patient relationship; hypothesis 7b (H7b) proposes that negative doctor-patient trust plays a mediating role between physician-patient concordance and doctor-patient relationship.
The vast majority of patients believe that online health information can improve the doctor-patient relationship, particularly when they discuss this information with their physicians. After obtaining health information from social media, patients may enhance their capabilities of preparing for medical consultations, asking questions, explaining their needs, and confidently engaging in discussions with their physicians. When patients participate more actively in consultations, physicians are more likely to share additional information and adopt a more patient-centered communication approach. Through this process, patients may develop greater trust in their doctors and reduce doubts, ultimately fostering a stronger doctor-patient relationship. Therefore, hypothesis 8a (H8a) proposes that physician-patient concordance and positive doctor-patient trust have a serial mediation effect between perceived improved coping ability with physicians and doctor-patient relationship; hypothesis 8b (H8b) proposes that physician-patient concordance and negative doctor-patient trust have a serial mediation effect between perceived improved coping ability with physicians and doctor-patient relationship.
In conclusion, the research model and hypothesis have been shown in Figure 1.
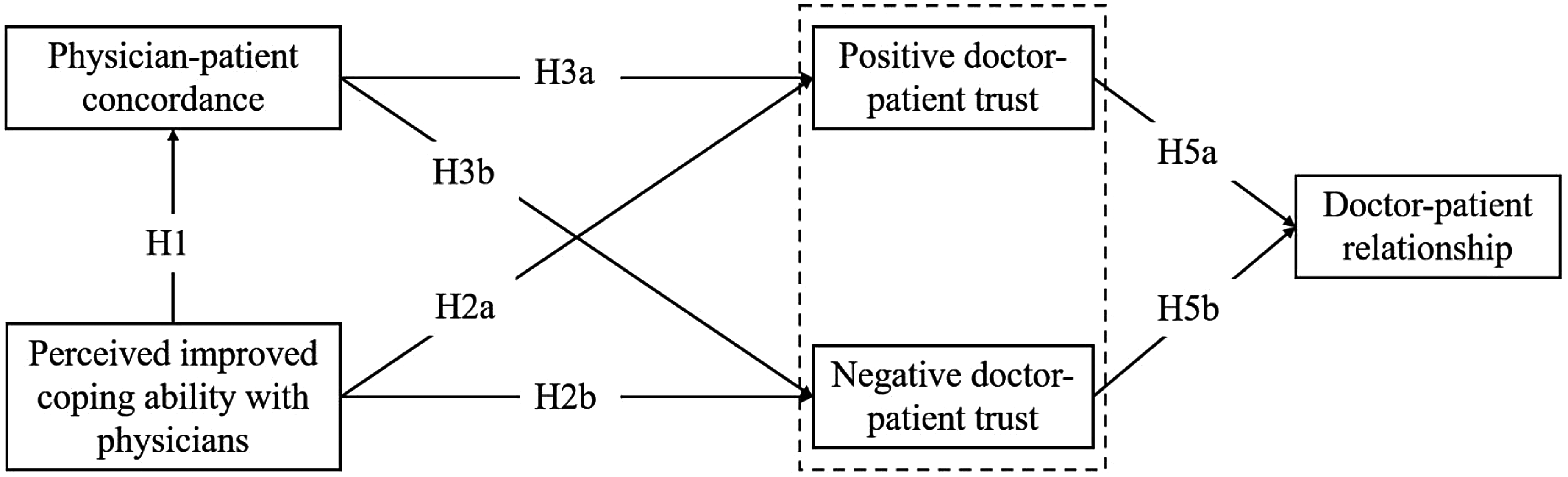
Research model and hypotheses.
Methods
Questionnaire composition
Existing validated scales were translated and modified to compose the questionnaire for this study by researchers, including doctors, nurses, university students, and administrative personnel. After conducting a pilot survey, the questionnaire was further refined based on the results. It consists of demographic items and several scales that were used to measure the respondents’ perception level. The questionnaire comprised 10 demographic items and four scales, totaling 41 items (Supplementary file 1). Due to the increased coverage of the internet and the rise of social media, traditional paper-based questionnaires have been replaced by online questionnaires. In addition, online questionnaires are not limited by the population and do not increase the risk of epidemic transmission. Therefore, in this study, an online questionnaire was created to conduct a nationwide survey on a Wenjuanxing online platform. 66 The formal cross-sectional survey was conducted from May 6, 2022, to May 8, 2022. The inclusion criteria were as follows: (1) age above 18 years, (2) ability to understand and read Chinese, (3) prior use of social media to obtain health information at least once in the past six months, (4) voluntary participation, and (5) willingness to provide informed consent. All eligible respondents were invited to participate in our online survey, while those not meeting any of the inclusion criteria were excluded. Convenience sampling survey was employed in this study. During the COVID-19 period, a total of 374 questionnaires were distributed. According to the standards of quality control, 286 questionnaires were valid and 88 questionnaires were invalid, resulting in an effective rate of 76.47%. To further validate the findings in a larger population, we conducted a nationwide survey on a Wenjuanxing online platform in China again from February 27 to March 6, 2025 after the COVID-19 period, based on the aforementioned inclusion and exclusion criteria. According to the standards of quality control, 1041 questionnaires were valid and 81 questionnaires were invalid, resulting in an effective rate of 92.78%.
The study protocol was approved by the Ethics Committee of Changzhou Maternal and Child Health Care Hospital (Approval No. 2022[22]). All participants provided informed consent electronically prior to participation in the online survey.
Quality control
The terms of informed consent, voluntary participation, and privacy protection were introduced before starting the questionnaire. An item about informed consent was included, and if the participant selected “disagree”, the questionnaire would be terminated. According to the outcomes of pilot survey, a minimum response time of 300 s (approximately 4 s per question) was established. Those questionnaires completed in less than 300 s were considered invalid. A personal identification number (consisting of the initials of the participant's Chinese name and the last four digits of their phone number) was used as the participant's identity credential. If the personal identification number, network IP address, and answers of a questionnaire were all consistent, and the filling time intervals for completion were close, the questionnaire would be determined as a duplicate. A common knowledge item (e.g., “Regarding emergency ambulance phone numbers, which one is correct?”) was included as a trap question, and questionnaires with incorrect answers were deemed invalid. Prominent reminders stating “… specifically targeting individuals who use social media for obtaining health information” were placed in the questionnaire's title and at the beginning of the informed consent section. During the distribution of the questionnaire, participants would be reminded again that they should have ever used social media to access health knowledge. Additionally, a trap answer option “Never use” was added to the item “What is the most frequently used social media platform when I want to acquire health information?”, and questionnaires filled with this option were considered invalid. Necessary instructions or examples were set to facilitate participants in filling out the questionnaire according to the correct format.
Classification of participants based on platform usage
Participants were categorized based on the frequency and type of social media platforms they used for health-related information. In practice, many social media platforms are gradually integrating multiple functions to meet users’ diverse needs. In China, similar to WhatsApp and Facebook, WeChat and QQ provide instant messaging services on smart devices. 33 Additionally, they also include content-sharing features. Zhihu is an online Q&A community akin to the American platform Quora, while Tieba is a topic-based discussion community that operates on keywords, both belonging to the category of Q&A platforms. 33 Xiaohongshu combines social media with e-commerce, often referred to as China's Instagram. 33 Profiles and characteristics of major Chinese social media platforms have been shown in Supplementary file 2 (Table S2). All three of these social media platforms function as online communities for knowledge sharing, communication, and discussion, possessing strong content analysis attributes alongside their social characteristics.
However, the content created on Zhihu, Tieba, and Xiaohongshu is predominantly based on users’ personal experiences and insights rather than health-related topics. Both QQ and WeChat exhibit strong social attributes, where shared content is filtered by “friends” acting as gatekeepers. Furthermore, WeChat users must apply for a subscription account before publishing content, which is subject to strict review prior to each release. Weibo, equivalent to Facebook in China, is an online platform for sharing, disseminating, acquiring, and sharing brief real-time information based on user relationships. 33 Although Weibo allows for content publication, discussion participation, and information acquisition like Zhihu, Tieba, and Xiaohongshu, it has a stronger social attribute, with a significant portion of health knowledge shared by non-health professional users being derived from reposts rather than original content. China's short video social media platforms include TikTok, Bilibili, and Kuaishou, which are also available in countries outside of China. 33 Therefore, this study categorizes WeChat, QQ, and Weibo as social interaction platforms, Zhihu, Tieba, and Xiaohongshu as content-sharing platforms, and TikTok, Bilibili, and Kuaishou as short video platforms.
Instruments
Perceived improved coping ability scale
The previous study measured perceived improved coping ability through the Perceived Stress Scale-4, assessing the extent to which an individual perceives stress in his/her life and their perceived ability to cope with stress. 67 In the medical field, patients now seek and use online health information increasingly to manage their own health more actively together with their physicians. 14 Online health information accessed from social media may reduce patients’ stress, increase their confidence when interacting with professionals, and increase their participation in the shared decision-making process. It has been defined as perceived improved coping ability under the influence of social media, abbreviated as perceived improved coping ability. Perceived improved coping ability scale was adapted from the Feeling more confident in the relationship with their physician scale developed by C.F. van Uden-Kraan et al. (Cronbach's α=.91). 34 The perceived improved coping ability scale used in this study consisted of 8 items. To enhance its applicability, the scenario-specific statement of each item in the original scale was replaced with “Through health information on social media…”. With this modification, the scale can reflect the increased confidence and capability of patients in communication with their physicians and participation in shared decision-making after accessing online health information. The scale was scored on a 5-point Likert scale, with response options ranging from ‘Strongly Disagree’, ‘Disagree’, ‘Neutral’, ‘Agree’ to ‘Strongly Agree’, scored as 1, 2, 3, 4, and 5, respectively. After exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), the KMO for perceived improved coping ability scale was .900. The Cronbach's α for it was .905, with the CR of .929, and AVE of .625. Additionally, it had good discriminant validity and model fit. The EFA and CFA results from the validation sample further confirmed them in Supplementary file 2 (Tables S3 to S8).
Physician-patient concordance scale
Physician-patient concordance regarding the patient's issues is related to the resolution of non-specific signs and symptoms. 68 When there is a lack of physician-patient concordance, the patient is less likely to return for further consultation. 69 Conversely, patients who exhibit a high concordance with their physicians are one-third more likely to take prescribed medications during the consultation. 46 The physician-patient concordance scale used in the study was adapted from the original physician-patient concordance scale developed by Ngaire Kerse (Cronbach's α=.87) and the adapted scale by John Laugesen,14,46 and the number of items in this physician-patient concordance scale was consistent with the five items in the adapted scale. Taking into consideration its applicability, the scale was contextualized. A scenario-specific statement was added to the scale, stating “The specific timeframe for these questions refers to the most memorable or relatively severe illness I have experienced recently.”. Thus, this scale can reflect physician-patient concordance in medical diagnosis and treatment during a specific episode of illness. The scale was scored on a 5-point Likert scale, with response options ranging from ‘Strongly Disagree’, ‘Disagree’, ‘Neutral’, ‘Agree’ to ‘Strongly Agree’, scored as 1, 2, 3, 4, and 5, respectively. respectively. After EFA and CFA, the KMO for physician-patient concordance scale was .891. The Cronbach's α for it was .897, with the CR of .897, and AVE of .637. Additionally, it had good discriminant validity and model fit. The EFA and CFA results from the validation sample further confirmed them in Supplementary file 2 (Table S3 to S8).
Doctor-patient trust scale
Trust is important in doctor-patient relationship and has positive effects on both parties involved. 70 The doctor-patient trust scale used in this study was adapted from the Chinese version of the Wake Forest Physician Trust Scale developed by Dong et al. 71 Taking into consideration its applicability, the scale was contextualized. A scenario-specific statement was added to the scale, stating “The specific timeframe for these questions refers to the most memorable or relatively severe illness I have experienced recently”. This modification allows the scale to measure doctor-patient trust during a medical consultation related to a specific illness. The doctor-patient trust scale used in this study consisted of two dimensions. Items 2, 3, 7, and 8 were negatively worded, representing negative doctor-patient trust. On the other hand, the remaining items were positively worded, representing positive doctor-patient trust. Given that prior studies treated items corresponding to different dimensions as separate latent variables, 72 doctor-patient trust scale was conceptualized as two independent dimensions-positive trust and negative trust-which were analyzed separately within the structural model in our study. Considering that the understanding of Chinese people towards different semantics may be quite different, this study tested the reliability and validity of Chinese version of the doctor-patient trust scale to determine the final items. The scale comprised a total of 10 items, and respondents are asked to rate their agreement on a five-point Likert scale ranging from ‘Strongly Disagree’, ‘Disagree’, ‘Neutral’, ‘Agree’ to ‘Strongly Agree’, scored as 1, 2, 3, 4, and 5, respectively. After EFA and CFA, the KMO for negative doctor-patient trust scale was .686. The Cronbach's α for it was .752, with the CR of .760, and AVE of .523. Additionally, it had good discriminant validity and model fit. The KMO for positive doctor-patient trust scale was .880.The Cronbach's α for it was .837, with the CR of .861, and AVE of .471. Additionally, it had good discriminant validity and model fit. The EFA and CFA results from the validation sample further confirmed them in Supplementary file 2 (Table S3 to S8).
Doctor-patient relationship questionnaire
The doctor-patient relationship is a complex psychosocial interaction within a professional environment, involving vulnerability, trust, and authority. 73 At the same time, doctor-patient relationship is an essential component for successful healthcare delivery. 74 Doctor-patient relationship questionnaire in this study was adapted from the original doctor-patient relationship questionnaire developed by Van der Feltz-Cornelis, Van Oppen. 75 In this study, a scenario-specific statement was added to the scale, indicating “The specific timeframe for these questions refers to the most memorable or relatively severe illness I have experienced recently.”. Thus, the scale can reflect the patient's perception of their relationship with the doctor when seeking medical care for a specific illness. This study tested the reliability and validity of the original scale doctor-patient relationship questionnaire-15 to determine the final items. The final questionnaire consisted of 8 items, scored on a 5-point Likert scale, with response options ranging from ‘Strongly Disagree’, ‘Disagree’, ‘Neutral’, ‘Agree’ to ‘Strongly Agree’, scored as 1, 2, 3, 4, and 5, respectively. After EFA and CFA, the KMO for doctor-patient relationship scale was .941. The Cronbach's α for it was .911, with the CR of .909, and AVE of .556. Additionally, it had good discriminant validity and model fit. The EFA and CFA results from the validation sample further confirmed them in Supplementary file 2 (Table S3 to S8).
Statistical analysis
Data analysis was conducted by SPSS 26.0, AMOS 24.0 and SmartPLS 4.1.0.0. Descriptive statistics were used to describe the participants’ demographic characteristics and medical consultation information, presented as frequencies and percentages. Continuous variables with normal distribution were presented as mean ± standard deviation (SD). Pearson correlation analysis was used to examine the correlations between pairs of variables. Reliability analysis was used to evaluate internal consistency, which is commonly assessed by Cronbach's α. A coefficient of it is greater than .7 indicates good consistency among items. Although all scales were derived from established measures, some modifications were made to original items to account for the unique Chinese context and healthcare system. Therefore, through the principal component analysis method, exploratory factor analysis (EFA) was conducted on all scales. Confirmatory factor analysis (CFA) was employed through AMOS 24.0. Our study randomly selected 143 samples out of 286 samples for EFA, and the remaining 143 samples were used for CFA. If the average variance extracted (AVE) is greater than .5 and the composite reliability (CR) is higher than .7, it indicates that the data has good convergent validity. Additionally, fit indices of all scales were tested, including CMIN/DF less than 2, GFI more than .9, CFI more than .9, SRMR less than .08, and RMSEA less than .07. SmartPLS, a specialized software, was used for Partial Least Squares Structural Equation Modeling (PLS-SEM). It is suitable for studying the relationships between multiple independent variables and multiple dependent variables. In this study, a model with 31 items was constructed, and the sample size exceeded 5 times the number of items, providing sufficient data support.
Confirmatory factor analysis for the multifactor model
As the model changes from a single-factor model to a model combining all factors, the χ2/df value gradually increases, while the GFI, CFI, and NFI values decrease, and the RMSEA and SRMR values increase, indicating a decline in model fit in Supplementary file 2 (Table S3 to S8). Therefore, the model without merging latent variables demonstrates the best model fit.
Common method bias
Through Harman's single-factor test, the presence of common method bias in the data was detected. All variables were entered into an exploratory factor analysis to determine the number of factors required to account for the variance in the variables. The results showed that the first principal component accounted for only 31.172% and 38.200% of the variance in the development and validation sample, respectively. They were both below the recommended threshold of 50%, 76 indicating that there is no significant common method bias in the data.
Results
Participants
In the development sample, the median age of participants was 35 ([P25, P75] = [29, 39]). 159 out of 286 participants (55.6%) were female. 188 out of 286 participants (65.7%) were married. 126 out of 286 participants (44.1%) had a junior college degree. When uncertain about their own health condition, all participants usually searched for relevant health knowledge on social media platforms. Specifically, 75 out of 286 participants (26.2%) primarily used WeChat or QQ to obtain health knowledge, followed by short video platforms such as TikTok, Bilibili, Kuaishou (16.8%), Weibo (15.7%), Zhihu or Tieba (14.0%), and finally Xiaohongshu (8.0%). In the validation sample, we have expanded the age range of the study population to enhance the model's applicability across different age groups. The median age of participants was 36 ([P25, P75] = [29, 53). 573 out of 1041 participants (55.0%) were female. 770 out of 1041 participants (74.0%) were married. 420 out of 1041 participants (40.3%) had a bachelor's degree. Specifically, 354 out of 1041 participants (34.0%) primarily used WeChat or QQ to obtain health knowledge, followed by short video platforms such as TikTok, Bilibili, Kuaishou (27.9%), Xiaohongshu (17.8%), Zhihu or Tieba (10.9%), and finally Weibo (3.7%).(Table 1).
Demographic characteristics of participants.

Correlation analysis
Considering that all study variables followed an approximately normal distribution, Pearson correlation analysis was used in this study. As shown in Table 2, based on the data from individuals primarily accessing health information through social interaction platforms, negative doctor-patient trust was significantly negatively correlated with doctor-patient relationship (r = −.758; P < .001), and there was a very strong positive correlation between positive doctor-patient trust and doctor-patient relationship (r = .775; P < .001). Perceived improved coping ability with physicians and physician-patient concordance showed a significant positive correlation (r = .314; P < .001), while perceived improved coping ability with physicians was significantly negatively correlated with negative doctor-patient trust (r = –.272; P = .003) and significantly positively correlated with positive doctor-patient trust (r = .269; P = .003). Physician-patient concordance was significantly negatively correlated with negative doctor-patient trust (r = –.295; P = .001) and positively correlated with positive doctor-patient trust (r = .269; P = .003). In other types of social media, negative doctor-patient trust was significantly negatively correlated with doctor-patient relationship, and there was a significant positive correlation between positive doctor-patient trust and doctor-patient relationship. Additionally, based on the data from individuals primarily accessing health information through other platforms, perceived improved coping ability with physicians had a significant negative correlation with negative doctor-patient trust in Supplementary file 2 (Table S9).
Pearson correlation analysis among variables based on individuals primarily accessing health information through social interaction platforms. a

: PICA: Perceived improved coping ability with physicians; NDPT: Negative doctor-patient trust; PDPT: Positive doctor-patient trust; DPR: Doctor-patient relationship; PPC: Physician-patient concordance.
Structural equation modeling
SmartPLS was employed to construct the initial SEM path diagram. Based on the data from individuals primarily accessing health information through social interaction platforms, the estimated model yielded the SRMR of .145 and the NFI of .656. Although these values did not reach the ideal standards, the model fit based on the data from individuals primarily accessing health information through social interaction platforms was the best after comparing with other groups (Table 3). Due to the small sample size, the fit results may be affected by limited statistical power, which somewhat restricts the accuracy of the model fit. Nonetheless, based on the current data, it has been decided to retain the existing model structure without further adjustments.
Fit indices of models based on individuals primarily accessing health information through different social media platforms.

Additionally, as shown in Table S10, the final outcome variable, doctor-patient relationship, exhibited the highest R2 (R2=.691) and substantial in-sample predictive relevance (Q2 = .456). The other endogenous variables, including negative doctor-patient trust, positive doctor-patient trust, and physician-patient concordance, showed moderate in-sample predictive relevance and demonstrated satisfactory out-of-sample predictive ability, with Q2_predict values greater than zero. Overall, the PLS predicts analysis suggested that the model maintains reasonable predictive stability, particularly for the core outcome variable, supporting the robustness of the hypothesized relationships (Supplementary file 2-Table S10).
In this study, a Bootstrap of 2000 was set to test the direct effects between variables in the model. As shown in Table 4, based on the data from individuals primarily accessing health information through social interaction platforms, perceived improved coping ability with physicians was positively correlated with physician-patient concordance (β=.330; P < .001) and positive doctor-patient trust (β=.204; P = .030), supporting H1 and H2a. Additionally, it was negatively correlated with negative doctor-patient trust (β=−.195; P = .051), supporting H2b. Physician-patient concordance was positively correlated with positive doctor-patient trust (β=.196; P = .024), supporting H3a. And it was negatively correlated with negative doctor-patient trust (β=–.239; P < .001), supporting H3b. Positive doctor-patient trust was positively correlated with doctor-patient relationship (β=.497; P < .001), supporting H5a. Negative doctor-patient trust was negatively correlated with doctor-patient relationship (β=–.373; P < .001), supporting H5b.
Standardized coefficients of models based on individuals primarily accessing health information through social interaction platforms. a
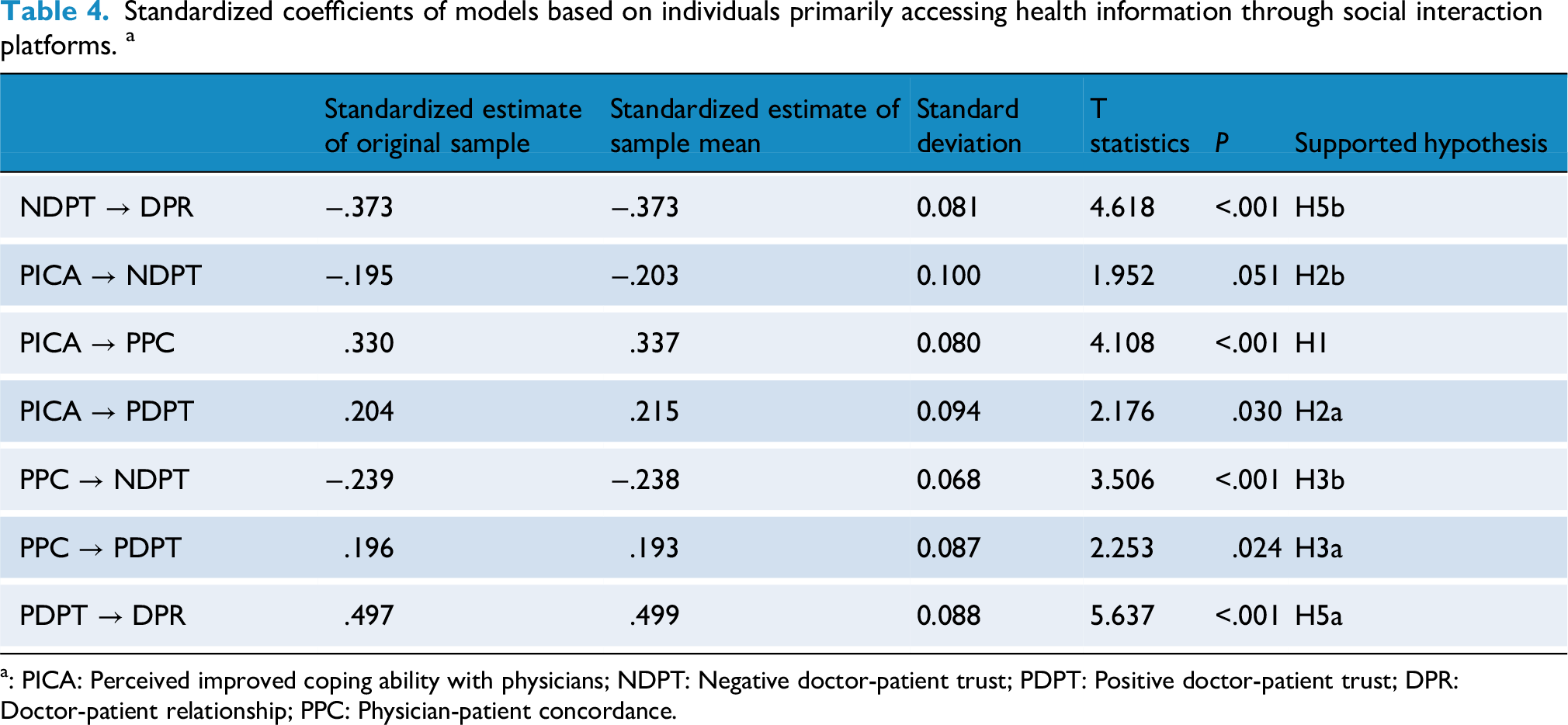
: PICA: Perceived improved coping ability with physicians; NDPT: Negative doctor-patient trust; PDPT: Positive doctor-patient trust; DPR: Doctor-patient relationship; PPC: Physician-patient concordance.
As shown in Table 5, based on the data from individuals primarily accessing health information through social interaction platforms, physician-patient concordance plays a partially mediating role between perceived improved coping ability with physicians and negative doctor-patient trust (β=−.079; P = .015), supporting H4b. Positive doctor-patient trust plays a fully mediating role between perceived improved coping ability with physicians and doctor-patient relationship (β=.101; P = .038), supporting H6a. Positive doctor-patient trust plays a fully mediating role between physician-patient concordance and doctor-patient relationship (β=.097; P = .044), supporting H7a. Negative doctor-patient trust plays a fully mediating role between physician-patient concordance and doctor-patient relationship (β=.089; P = .008), supporting H7b. Physician-patient concordance and negative doctor-patient trust have a serial mediation effect between perceived improved coping ability with physicians and doctor-patient relationship (β=.029; P = .040), supporting H8b. In addition, the indirect effect of perceived improved coping ability with physicians on positive doctor-patient trust via physician-patient concordance was positive but did not reach conventional significance (β = .065, P = 0.080), indicating a marginal trend. Therefore, H4a was not supported. The indirect effect of perceived improved coping ability with physicians on doctor-patient relationship through negative doctor-patient trust showed a marginal effect (β = .073, P = 0.057), approaching significance but not statistically significant, and H6b was not confirmed. All hypotheses have been shown in Figure 2.

Structural equation model diagram based on individuals primarily accessing health information through different social media platforms.
Hypothesis testing of direct, indirect, and total effects based on individuals primarily accessing health information through social interaction platforms. a

: PICA: Perceived improved coping ability with physicians; NDPT: Negative doctor-patient trust; PDPT: Positive doctor-patient trust; DPR: Doctor-patient relationship; PPC: Physician-patient concordance.
In the models based on the data from individuals primarily accessing health information through short video platforms and content-sharing platforms, positive doctor-patient trust was significantly positively correlated with doctor-patient relationship, and negative doctor-patient trust was significantly negatively correlated with doctor-patient relationship (Supplementary file 2-Table S10 and Figure 2). In the model based on the data from individuals primarily accessing health information through other platforms, positive doctor-patient trust was significantly positively correlated with doctor-patient relationship, perceived improved coping ability with physicians was negatively correlated with negative doctor-patient trust (Supplementary file 2-Table S11).
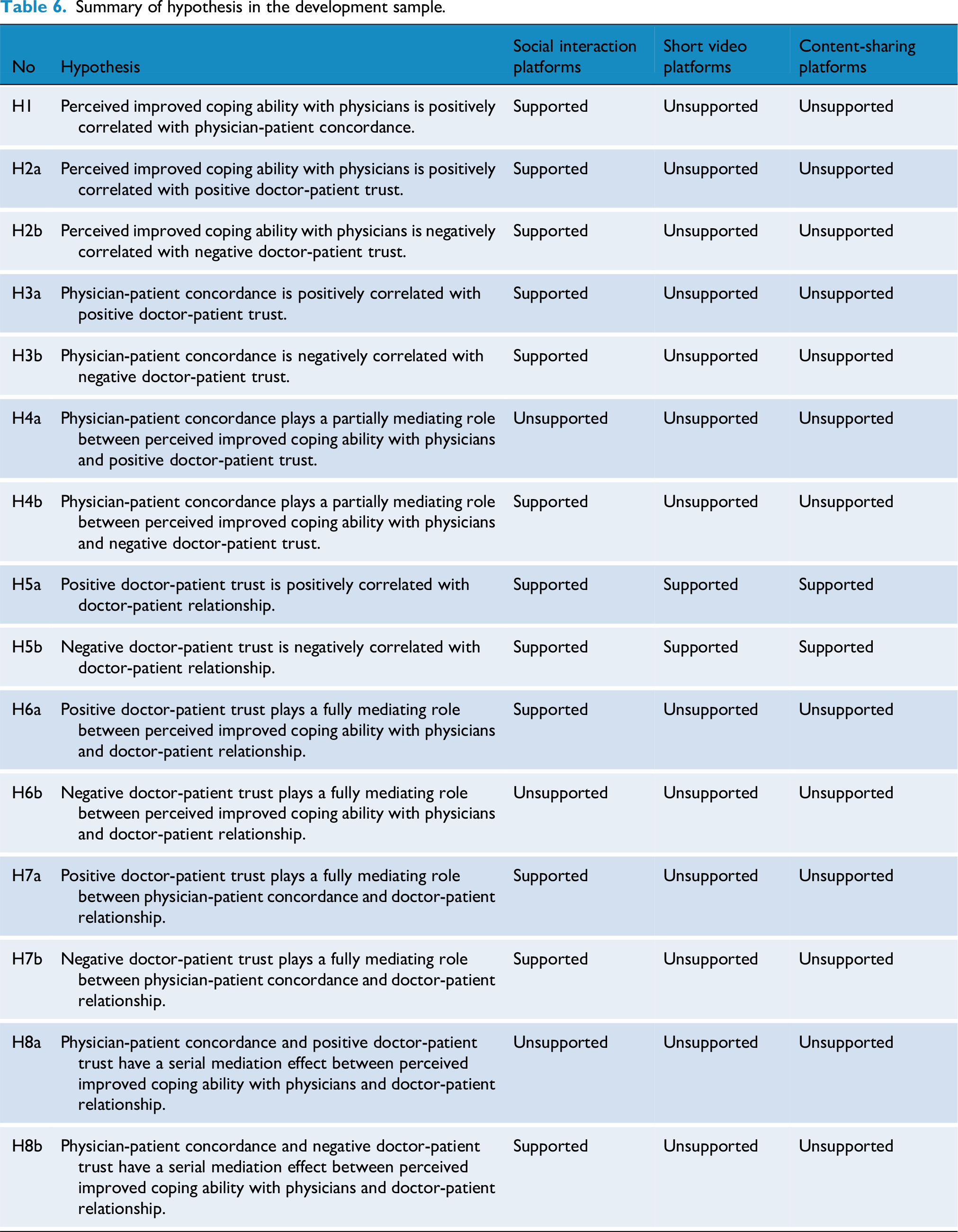
This study evaluated the relationship among perceived improved coping ability with physicians, negative doctor-patient trust, positive doctor-patient trust, doctor-patient relationship and physician-patient concordance based on individuals primarily accessing health information through social interaction platforms, short video platforms and content-sharing platforms. The test results are shown in Table 6.
Summary of hypothesis in the development sample.
Validation analysis
In the validation sample, the correlations among variables for users of social interaction platforms were consistent with those in the development sample (Supplementary file 2-Table S12). The results showed that the model fits of the validation sample based on the data from individuals primarily accessing health information through different social media platforms were better than those of the development sample (Supplementary file 2-Table S13). In addition, the model results based on the data from individuals primarily accessing health information through different social media platforms were similar with those based on the development sample. However, positive doctor-patient trust was positively correlated with doctor-patient relationship only in the models based on the data from individuals primarily accessing health information through content-sharing platforms (β=.274; P = .021), which was not supported in the models based on the data from individuals primarily accessing health information through social interaction platforms, short video platforms and other platforms. On the contrary, negative doctor-patient trust was negatively correlated with doctor-patient relationship only in the models based on the data from individuals primarily accessing health information through social interaction platforms (β=−.463; P < .001) and short video platforms (β=−.404; P<.001), which was not supported in the models based on the data from individuals primarily accessing health information through content-sharing platforms. The models based on the data from individuals primarily accessing health information through social interaction platforms and short video platforms were similar (Supplementary file 2-Table S14, Table S15 and Supplementary file 3- Figure S1).
Discussion
Principal findings
In our study, the model testing results based on different social media platforms were not entirely consistent. Overall, it has been primarily found that most research hypotheses were supported in the model constructed using data from individuals primarily accessing health knowledge through social interaction platforms, which has also been supported in the validation sample. However, in the models based on data from individuals utilizing content-sharing and short video platforms as their main sources of health knowledge, only H5a and H5b were validated, while the remaining research hypotheses were not supported. These have not supported in the validation sample.
During COVID-19 in the models constructed using data from individuals primarily accessing health knowledge through social interaction platforms, perceived improved coping ability with physicians was positively correlated with positive doctor-patient trust and negatively correlated with negative doctor-patient trust. H2a and H2b were supported. In the three models based on data from individuals utilizing short video platforms, content-sharing platforms, and other social media as their main sources of health knowledge, the positive correlations between perceived improved coping ability with physicians and positive doctor-patient trust, as well as perceived improved coping ability with physicians and negative doctor-patient trust, were not statistically significant. The mean value of perceived improved coping ability with physicians among individuals accessing information through social interaction platforms was slightly higher than that of content-sharing and short video platforms, although the differences in means were not statistically significant. These findings suggest that the characteristics of information on different platforms may alter the relationship between perceived improved coping ability with physicians and doctor-patient trust by influencing respondents’ perceptions of information usefulness, the extent of information adoption, and their capacity for doctor-patient interaction. In traditional healthcare settings, patients are generally at an informational disadvantage and lack sufficient understanding of physicians’ knowledge and judgments, resulting in information asymmetry in the doctor-patient relationship. 77 The rise of social media platforms, particularly social interactive platforms, provides patients with new channels to access health information, potentially mitigating this information asymmetry. This is consistent with the framework of the information adoption model. Based on the information adoption model, information quality and source credibility jointly influence the mediating variable of perceived usefulness, which in turn triggers information adoption behavior. 78 The data collected in this study were based on respondents’ evaluations of the social media platforms they most frequently use to obtain health knowledge. The choices made by respondents reflect their high perception of the credibility of information sources on these social media platforms. Therefore, under the premise that respondents have already formed clear evaluations of the credibility of these social media sources, the quality of information available on these platforms becomes one of the key factors influencing respondents’ perceived usefulness of the information, their information adoption, and even doctor-patient interactions. The core evaluation criteria for information quality mainly include accuracy, completeness, understandability, and relevance. 14 Among these, accuracy is the core element of information quality, while completeness ensures that users receive comprehensive information. Understandability refers to how easily the information can be understood, interpreted, and utilized by the target audience. Relevance is a key element that ensures the information is valuable to users.
All the social media platforms mentioned in this study utilize algorithmic recommendations and keyword search functions to provide users with information relevant to their needs. The diverse presentation forms of various social media ensure the comprehensibility of information. However, regarding accuracy, WeChat, QQ, and Weibo have strict authentication processes for accounts that publish information, along with rigorous review mechanisms for the content shared. Most health information is disseminated by medical institutions and professional health personnel, lending a high degree of credibility, although some non-professional or misleading information is also present on these platforms. In contrast to WeChat, Weibo, and QQ, content on Zhihu, Tieba, and Xiaohongshu is more frequently based on patients’ personal original health information. This information often stems from individual experiences and insights and may lack medical professionalism. Compared to WeChat, knowledge shared on Zhihu and Tieba mainly comes from reposts on other platforms and personal experiences of netizens, as well as suggestions from some netizens with medical expertise. 33 The process of waiting for answers on Zhihu and Tieba can reduce the time and costs associated with searching for knowledge, but the information is derived from others and tends to have lower credibility. 33 On platforms like Zhihu, Tieba, and Xiaohongshu, users are influenced not only by the content created by authors but also by the subjective discussions and opinions of other users, which may further diminish the accuracy of the information. In terms of completeness, health information on WeChat, QQ, and Weibo is typically presented in text, images, and videos, making the information relatively comprehensive. Conversely, on short video platforms, each video is brief, leading to a fragmentation of information dissemination that makes it challenging to provide a thorough introduction to all aspects of a disease within the limited time. Additionally, the effectiveness of video dissemination is affected by the presenter's expressive ability and knowledge base. In other words, the quality of information shared on the same health topic can vary significantly across different short videos. A study has shown that during participation in online patient support groups, patients’ perceived information exchange (including aspects such as comprehensibility, accuracy, usability, reliability, consistency, novelty, and applicability) may influence their confidence in coping with physicians. 34 Therefore, the quality of health information on social interaction platforms may enhance users’ preparedness and confidence when facing physicians. However, the fragility of doctor-patient trust may be linked to the existing power imbalance between them.53,54 Information asymmetry in the doctor-patient relationship signifies a power disparity. Under conditions of unequal power, patients’ perceived inadequate coping ability with physicians may diminish positive trust while potentially increasing negative trust.
During COVID-19 period, the Chinese government's unified organization of health communication and strict review mechanisms ensured the quality of health knowledge. The quality of online health information positively impacts physician-patient concordance. 14 High-quality health information from social interaction platforms may facilitate patients’ accurate understanding of their conditions and enhance their communication abilities, thereby fostering consensus between doctors and patients. Consequently, among individuals that primarily utilize social interaction platforms for health knowledge, a positive correlation exists between perceived improved coping ability with physicians and physician-patient concordance. H1 was supported. Moreover, the correlation coefficient between perceived improved coping ability with physicians and physician-patient concordance is greater than that between perceived improved coping ability with physicians and positive doctor-patient trust or negative doctor-patient trust. This suggests that health knowledge acquired through social interaction platforms has a more direct and significant impact on physician-patient concordance. This may be because when patients partially alleviate information asymmetry through high-quality health information, their understanding of the disease and treatment becomes more accurate, facilitating consensus with physicians regarding clinical decisions. In contrast, the formation of doctor-patient trust not only depends on information symmetry but is also influenced by external factors such as physician authority, patients’ prior experiences, and emotional considerations. 79 Therefore, the perceived improvement in patients’ ability to cope with physicians’ recommendations typically has a stronger direct effect on physician-patient concordance than on doctor-patient trust. However, on other social media, the positive correlation between perceived improved coping ability with physicians and physician-patient concordance is not statistically significant. This result indicates that the quality of health knowledge on social media may indirectly affect physician-patient concordance. Many patients may misinterpret unverified information they search for as a revelation, leading to information asymmetry and unrealistic expectations regarding treatment. 45 When physicians attempt to correct or adjust patients’ misconceptions about the information they have sought, it can often result in additional time expenditure. 80 These factors may contribute to an uncomfortable experience for patients seeking medical care. Therefore, even when patients obtain health information via social media, the quality of the information and the reliability of its sources remain critical factors in alleviating information asymmetry and promoting physician-patient concordance and doctor-patient trust.
Among all the social media involved in this study, physician-patient concordance was positively correlated with positive doctor-patient trust and negatively correlated with negative doctor-patient trust. H3a and H3b were supported. Physician-patient concordance is an effective outcome of communication and a direct product of alleviating information asymmetry, with a more central and immediate role. Previous research has confirmed that high-quality communication is positively correlated with trust. 81 Conversely, a lack of effective communication between physicians and patients may lead to a loss of trust. 55 When a physician's treatment recommendations, attitudes, and behaviors align with the patient's expectations, disease perceptions, and treatment plans, patients are more likely to develop positive doctor-patient trust. In contrast, when online health information is inconsistent with the physician's advice, patients may begin to question the physician's credibility. 82 Furthermore, the absence of complex conflicts of interest between physicians and patients objectively alleviated antagonistic sentiments during COVID-19 period.22,83 This led to increased patient compliance and greater mutual trust and respect. 84 Such a positive intergroup trust environment makes it easier for both parties to reach a consensus.
Only among individuals who primarily use social interaction platforms to obtain health knowledge does physician-patient concordance play a partial mediating role between perceived improved coping ability with physicians and negative doctor-patient trust. H4b was supported. The doctor-patient relationship is inherently characterized by information asymmetry. 38 When patients acquire high-quality health knowledge through social interaction platforms, it may enhance their preparedness for medical consultations and their communication skills with physicians. These changes can not only directly impact doctor-patient trust but may also reduce information asymmetry, facilitating higher physician-patient concordance, thereby alleviating doubts about the physician and enhancing doctor-patient trust. In other words, patients with higher perceived improved coping ability with physicians are better able to understand physicians’ recommendations and engage in discussions with them, which may help reduce the emergence of negative trust even in cases where there are inconsistencies in certain issues. However, we found that physician-patient concordance did not have a significant mediating effect on positive doctor-patient trust, which may be related to the psychological mechanisms underlying trust formation. Positive doctor-patient trust not only depends on the degree of information symmetry but is also influenced by patients’ overall evaluations of physicians’ expertise, attitude, and prior experiences, 79 factors that do not change immediately even with the intervention of high-quality information. Therefore, the quality of health knowledge on social media platforms that include patients in medical decision-making is particularly crucial for the effects of information adoption and application.
Among all the social media platforms involved in this study, positive doctor-patient trust was positively correlated with doctor-patient relationship, while negative doctor-patient trust was negatively correlated with doctor-patient trust. H5a and H5b were supported. Trust is a core factor that facilitates the doctor-patient relationship, especially the trust that patients place in physicians. 85 When patients have a high level of positive trust in their doctors, they tend to evaluate the overall quality of the doctor-patient relationship more favorably. Additionally, during the response to COVID-19, physicians demonstrated commendable dedication and professional competence, which were recognized by the public. 4 These factors help ensure that doctor-patient trust evolves into a stable and enduring relationship. Conversely, patients with lower levels of trust in their doctors often expend more time and resources to verify that their physicians’ actions genuinely align with their best interests. 86 Such protective behaviors resulting from diminished trust not only increase the burden on patients but may also introduce additional tension and unnecessary complexity into the doctor-patient relationship. These negative emotions can undermine collaboration between doctors and patients.
Only among individuals who primarily use social interaction platforms to obtain health knowledge, positive and negative doctor-patient trust played a fully mediating role between physician-patient concordance and doctor-patient relationship. H7a and H7b were supported. In the binary relationship between doctors and patients, the information asymmetry leads to an imbalance of power. In this process, the binary concordance between doctors and patients plays a crucial role, as it signifies effective communication of information and the establishment of mutual consensus during interactions, particularly in enhancing doctor-patient trust, boosting patients’ confidence in coping with physicians, and promoting patients’ understanding of health knowledge. 56 Therefore, positive and negative doctor-patient trust act as bridges and links in the relationship between physician-patient concordance and doctor-patient relationship.
Only among populations that primarily use social interaction platforms to acquire health knowledge did positive doctor-patient trust play a fully mediating role between perceived improved coping ability with physicians and doctor-patient relationship. H6a was supported. In other words, perceived improved coping ability with physicians does not directly impact the doctor-patient relationship. According to information asymmetry theory, the doctor-patient relationship inherently involves an imbalance of information and power, with physicians possessing professional knowledge and clinical experience, while patients are comparatively information-poor. 77 Even if patients acquire health knowledge through social media and enhance their ability to cope with physicians, such improvements primarily occur at the cognitive and skill levels and are still insufficient to directly establish a stable doctor-patient relationship. After obtaining health knowledge through social media, patients may undergo a series of cognitive and behavioral changes. However, these changes alone are insufficient to establish a stable doctor-patient relationship directly. The key lies in the need for these changes to be accompanied by effective interactions with the physician, where trust is established during the interaction, thus potentially reinforcing and developing the doctor-patient relationship further. Many physicians believe that the impact of online health information on the doctor-patient relationship has both advantages and disadvantages. 65 Conflicts or disputes may arise when patients’ online health knowledge is inconsistent with physicians’ diagnoses or treatments. 33 Therefore, it is only when patients perceive improved coping ability with physicians and develop positive doctor-patient trust that they can also perceive a favorable doctor-patient relationship.
Only among populations that primarily use social interaction platforms to acquire health knowledge did physician-patient concordance and negative doctor-patient trust have a serial mediation effect between perceived improved coping ability with physicians and doctor-patient relationship. H8b was supported. The verification of information is bidirectional; it can occur either by searching the internet to validate the information provided by physicians or by consulting medical staff to verify the health information available online. 87 Correct bidirectional verification of information may facilitate consensus between patients and physicians. Once patients and physicians reach an agreement, both their satisfaction levels and the satisfaction gap between them are likely to improve. 88 Moreover, during the process of information verification and consensus formation, patients’ negative suspicion and distrust toward physicians are effectively reduced. The reduction of such negative trust directly improves the doctor-patient relationship, making patients more receptive to physicians’ recommendations and facilitating positive interactions. Therefore, physician-patient concordance serves as a crucial link connecting perceived improved coping ability with physicians and doctor-patient relationship. Additionally, this study reaffirms the significant role of fostering trust and eliminating doubts in promoting doctor-patient relationship.
In the validation sample, we found that among individuals who acquired health knowledge through social interaction platforms and short video platforms, all hypotheses were supported except for positive association between positive doctor-patient trust and the doctor-patient relationship. In contrast, for individuals obtaining health information via content-sharing platforms, all hypotheses were supported except for negative association between negative doctor–patient trust and doctor–patient relationship. These results may be interpreted from three perspectives: the unique context of the COVID-19, the differing characteristics of each platform, and sample size. During the COVID-19 period, the health information disseminated across various social media platforms primarily focused on COVID-19-related topics - a trend that may have been more pronounced on short videos and content-sharing platforms. Existing research indicates that COVID-19 was the most frequently discussed health condition on non-Twitter social media platforms. 89 Even when these platforms provided information on other diseases, such content was often associated with COVID-19. Algorithm-driven push mechanisms and user search behavior further prioritized COVID-19 content, making it difficult for users to access or prioritize health knowledge unrelated to the COVID-19. As a result, individuals relying on short videos and content-sharing platforms may have found it challenging to comprehensively enhance perceived improved coping ability with physicians and physician-patient concordance.
As epidemic control measures evolved, public understanding of COVID-19 on social media platforms became more transparent, and the generation of new COVID-19-related content declined. Concurrently, the heightened public awareness of health during the COVID-19 period, along with China's strong promotion of science-based health communication, led to a surge in high-quality, visually engaging health information covering a wide range of diseases. According to data released by Douyin Medical in 2024, the platform gained 13,000 new medical science content creators and 3.7 million new science popularization videos over the past year. 90 These developments may have facilitated the establishment of doctor-patient trust, allowing users to assess physicians’ professionalism and credibility from multiple dimensions. This, in turn, could enhance physician–patient concordance, build doctor-patient trust, and ultimately improve the doctor–patient relationship.
Furthermore, our findings suggest that differences in user characteristics across platforms may also account for these results. Social interaction and short video platforms tend to attract younger users and “follower-type” audiences who often search for health information in a more spontaneous and unstructured manner. Consequently, in addition to accessing health education content, they may also encounter negative news about medical professionals during their browsing. Younger users are generally more emotionally reactive to negative content. Coupled with the immersive design and “illusion of control” inherent to these platforms, they may struggle to disengage from use even after experiencing negative emotions, 91 leading to sustained emotional distress and cognitive bias. This emotional contagion may foster negative perceptions of physicians and thus adversely impact the doctor-patient relationship. By contrast, users of content-sharing platforms may exhibit more rational or goal-oriented behavior and possess stronger critical thinking abilities. In other words, they are more likely to search directly for specific information they need and are better equipped to evaluate negative online information about physicians with a critical lens. This allows them to avoid forming negative doctor-patient trust and instead facilitates the development of a constructive doctor-patient relationship through mechanisms of positive doctor-patient trust.
Limitations
First, this study was conducted during COVID-19 period. The Chinese government imposed strict reviews and unified organization of health knowledge dissemination on social media, and the overall doctor-patient relationship improved during this period. Outside of this “exceptional” context, the proposed hypotheses need further validation. Second, the study employed a cross-sectional survey methodology, making it impossible to draw clear inferences about the causal relationships among the variables. Future research should consider implementing longitudinal studies. Thirdly, although all hypotheses have been supported by the validation sample, the significant time gap between the two data collection periods introduced temporal bias and background changes, meaning the validation sample does not accurately reflect the situation during the COVID-19 period. Fourth, this research utilized only quantitative analysis; future investigations could delve deeper into other factors influencing perceived improved abilities coping with physicians, physician-patient concordance, doctor-patient trust, and doctor-patient relationships through qualitative analysis. Finally, all core variables were measured via self-report based on participants’ recall of a “most memorable illness,” which may introduce recall and social desirability bias.
Conclusion
Despite the Chinese government's unified organization and strict review of health knowledge dissemination during COVID-19 period, all the proposed hypotheses were validated only among individuals who primarily used social interaction platforms (such as WeChat, QQ, and Weibo) as their main sources of health knowledge. The rigorous review mechanisms of social interaction platforms may serve as important measures to ensure the quality of health knowledge. Although patients’ improved coping ability with physicians acquired from health knowledge on other social media platforms may not influence physician-patient concordance or doctor-patient trust, the intergroup trust and common goals between physicians and patients during COVID-19 period in China may promote physician-patient concordance, thereby increasing doctor-patient trust and fostering harmony in doctor-patient relationships. Additionally, by promoting the use of social interaction platforms, physicians can effectively share valuable information on health management and coping strategies with patients, thereby empowering them, strengthening their coping abilities, and fostering better physician-patient concordance and doctor-patient relationship.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251411210 - Supplemental material for The association between perceived improved coping ability and the doctor-patient relationship among patients accessing health knowledge via social Media: A cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251411210 for The association between perceived improved coping ability and the doctor-patient relationship among patients accessing health knowledge via social Media: A cross-sectional study by Renjie Lu, Jing Zhou, Jiaying Ge, Xiyang Xia, Shenyu Zhao, Yu Chen, Yang Chen, Juan Wen and Lingmin Hu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251411210 - Supplemental material for The association between perceived improved coping ability and the doctor-patient relationship among patients accessing health knowledge via social Media: A cross-sectional study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251411210 for The association between perceived improved coping ability and the doctor-patient relationship among patients accessing health knowledge via social Media: A cross-sectional study by Renjie Lu, Jing Zhou, Jiaying Ge, Xiyang Xia, Shenyu Zhao, Yu Chen, Yang Chen, Juan Wen and Lingmin Hu in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251411210 - Supplemental material for The association between perceived improved coping ability and the doctor-patient relationship among patients accessing health knowledge via social Media: A cross-sectional study
Supplemental material, sj-docx-3-dhj-10.1177_20552076251411210 for The association between perceived improved coping ability and the doctor-patient relationship among patients accessing health knowledge via social Media: A cross-sectional study by Renjie Lu, Jing Zhou, Jiaying Ge, Xiyang Xia, Shenyu Zhao, Yu Chen, Yang Chen, Juan Wen and Lingmin Hu in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
Not applicable
Ethical approval
The study was approved by the ethics committee of Changzhou Maternal and Child Health Care Hospital (No.2022[22]).
Consent to participate
All participants’ informed consent was obtained online before the survey.
Consent to publish
All authors have read and approved the final version of the manuscript and consent to its publication in this journal.
Author's contributions
The conceptualization was carried out by Lingmin Hu, Juan Wen, Renjie Lu. The methodology was carried out by Lingmin Hu, Juan Wen, Renjie Lu. The investigation was carried out by Renjie Lu, Shenyu Zhao. Formal Analysis was carried out by Renjie Lu and Jing Zhou. Funding Acquisition was carried out by Lingmin Hu and Renjie Lu. Writing-Original Draft was carried out by Jiaying Ge, Jing Zhou, Renjie Lu. Writing -Review & Editing was carried out by Renjie Lu, Jing Zhou, Yang Chen, Yu Chen, Shenyu Zhao, Xiyang Xia, Jiaying Ge. Data Curation was carried out by Jing Zhou. Validation of the study was carried out by Juan Wen and Jing Zhou. Visualization of this study was carried out by Jiaying Ge. The supervision of this study was carried out by Lingmin Hu and Juan Wen. All authors reviewed and provided edits for the final manuscript.
Funding
This research was supported by Open Research Fund Program of Changzhou Institute for Advanced Study of Public Health, Nanjing Medical University [CPHS202303], the 2024 Medical Quality (Evidence-Based) Management Research Project of the National Institute of Hospital Administration, National Health Commission of the People's Republic of China [YLZLXZ24G031], and the Hospital Management Innovation Research Project of Jiangsu Hospital Association in 2023 [JSYGY-3-2023-247], and the Research Project on Policy of Traditional Chinese Medicine for Deepening Reform of Healthcare System in 2024 of the Monitoring and Statistical Research Center of the National Administration of Traditional Chinese Medicine [YGZXKT2024124], and Jiangsu Province Hospital Association Special Research Project on Hospital Pharmaceutical Administration in 2024 [JSYGY-2-2024-YS41], and Jiangsu Pharmaceutical Association - Aosaikang Hospital Pharmacy Research Fund Project in 2024 [A202426], and the 2024 Hospital-level Research Project of Changzhou Third People's Hospital [SY202433], and Changzhou Soft Science Research Project in 2024 [CR20241102], and Changzhou Hospital Association Practical Research Project on “Improving Medical Experience and Enhancing Patient Experience” in 2025.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Guarantor
Lingmin Hu is the guarantor of this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.