
Abstract
Objective
This study investigates how technical features of hospital self-service systems influence patients’ organizational trust and treatment adherence through trust transfer mechanisms in the Chinese digitally integrated healthcare context.
Methods
A cross-sectional survey was conducted with 310 patients in China who had used hospital self-service systems in the past three months. Structural equation modeling using SmartPLS 4.0 assessed the effects of Technical Convenience and Technical Safety and Information Quality on Perceived Systems Reliability, Global Trust in Healthcare Providers, and barriers to treatment adherence.
Results
Both Technical Convenience and Technical Safety and Information Quality significantly enhanced Perceived Systems Reliability, which subsequently increased Global Trust in Healthcare Providers. Technical Convenience had a stronger direct effect on organizational trust, while Technical Safety and Information Quality exerted more influence through Perceived Systems Reliability. Global Trust significantly reduced both Uncertainty and Doubts about Therapy and Practical Barriers to treatment. Moreover, Digital Distrust negatively moderated the effect of Technical Safety and Information Quality on Perceived Systems Reliability.
Conclusion
This study conducted in China demonstrates that hospital self-service systems significantly influence patient trust and treatment adherence through system reliability perceptions. Technical Convenience directly enhances organizational trust, while Technical Safety and Information Quality work indirectly. Hospitals can optimize trust by simplifying interfaces, providing real-time security prompts, and maintaining staff support. For patients who are less comfortable with digital technology, additional staff support may enhance their experience.
Keywords
Introduction
Digital healthcare transformation has positioned hospital self-service systems as increasingly important tools for improving efficiency and optimizing resource allocation in healthcare services,1–3 Self-service systems refer to digital service platforms that allow patients to independently complete tasks such as registration, payment, information inquiries, and report retrieval through self-service terminals, mobile applications, or internet platforms without assistance from medical staff. 3 These systems not only enhance service convenience and patient experience but also help alleviate medical resource shortages, reduce operational costs, and decrease the workload of front-desk staff under specific conditions.4–6
Within China's hospital system, patients’ interactions with self-service systems span the entire care process around the hospital.7–9 On arrival, patients first use self-service kiosks to complete registration and select physicians.10,11 During the visit, they use mobile applications to view test results and manage medical records.12,13 Meanwhile, digital payment systems provided to patients integrate Alipay, WeChat Pay, and medical insurance cards, allowing payment via mobile devices or kiosks and streamlining the billing process.14–16 After the visit, patients can obtain electronic reports and receive follow-up reminders through the same platform.17–19 This systematized service model has redefined the patient experience in hospitals.20,21
As self-service systems play increasingly critical roles in healthcare service processes, their operational quality and user experience have begun to significantly influence patients’ subjective judgments of overall service quality and institutional capabilities, 22 When patients’ medical experiences become increasingly dependent on digital technology system performance, their positive perceptions of system reliability, convenience, and security not only influence their judgments of service efficiency and quality but may also foster trust in the system, which can then be transferred to trust in the healthcare institution as a whole through trust mechanisms,23–26 This trust not only shapes patients’ overall perception of the healthcare system but also significantly influences their behavioral responses to treatment recommendations, 27 Hallet al. 28 and Stivers and Timmermans 29 indicate that patients’ trust in healthcare institutions not only significantly reduces resistance to treatment plans but also enhances their willingness to accept recommendations and adhere to treatment.
Related research has increasingly focused on trust in healthcare technology. Immonen and Koivuniemi 30 found through empirical research on the adoption of medical self-service technologies that system convenience, security, and information quality are key technical features influencing patients’ intention to use the system. Xieet al. 31 developed a framework of factors influencing trust beliefs in medical self-help systems based on an enhanced trust model, finding that constructs such as situational normality, structural assurance, cognitive reputation, perceived ease of use, and self-efficacy have significant positive impacts on patients’ technical trust. Catapan et al. 32 conducted a systematic review of digital healthcare trust and confirmed that 40.8% of studies found trust to have significant predictive effects on the intention to use digital healthcare technology.
However, these studies remain limited to technical-level adoption or trust issues, lacking a patient-centered research perspective that uses technical adoption and trust as starting points to explore institutional trust formation. Similarly, while existing healthcare trust research examines patients’ trust in healthcare institutions, it primarily focuses on direct patient-provider interactions and considers the role of digital system interactions.33,34 Therefore, how technical trust transfers to institutional trust and influences treatment adherence remains underexplored. As digital healthcare expands, technological interactions have become important touchpoints in patients’ institutional trust formation. 35 However, the mechanisms through which technical trust transforms into institutional trust currently lack systematic theoretical explanation and empirical testing.
To address this research gap, this study poses the following research questions: (1) How do Technical Convenience (TC) and Technical Safety and Information Quality (TSIQ) of hospital self-service systems influence patients’ trust in healthcare institutions? (2) How does patients’ trust in healthcare institutions influence their treatment adherence? (3) How does patients’ Digital Distrust (DD) moderate the influence of TSIQ on trust formation?
To address these questions, this study constructs a theoretical framework based on the Organizational Trust Model 36 and Trust Transfer Theory. 24 This framework explains the mechanism through which patients form Perceived Systems Reliability (PSR) through their technical experiences with self-service systems, which then translates into Global Trust in Healthcare Providers (GTHP), and ultimately reduces Uncertainty and Doubts about Therapy (UDT) and Practical Barriers (PB). Additionally, the framework incorporates the moderating effect of DD. This study employs structural equation modeling to empirically test this theoretical framework.
Theoretically, this study is the first to integrate organizational trust theory and trust transfer theory to construct a trust formation framework in the context of digital healthcare, identifying PSR as the key mediating mechanism in the transformation from technological trust to organizational trust, and revealing the moderating role of DD in the trust pathway, thereby expanding the applicability of trust theory in high-tech dependency scenarios. Practically, this study provides scientific evidence and implementation pathways for healthcare institutions to optimize self-service system design, develop differentiated trust management strategies, and improve patient treatment adherence.
Literature review
Self-service system and digital trust
Public trust is the cornerstone of successful health systems, and the lack of accessible and trustworthy digital healthcare applications has become a key barrier to digital health advancement.37,38 In hospital self-service systems, objective performance advantages do not automatically translate into preference and sustained adoption, with the crux lying in digital trust.39,40 Cross-national evidence shows that the relationships between perceived security, perceived risk, and trust are nonlinear, with significant pathway differences across different groups. Healthcare practitioners in developed countries demonstrate greater trust sensitivity and risk awareness toward technology, highlighting institutional and contextual heterogeneity. 41 From a health equity perspective, the digital divide in the Global South is more pronounced, with technology designs dominated by developed countries often misaligned with the actual needs of developing regions, and this structural inequality directly affects the generation patterns of digital healthcare trust. 42 Empirical research in Chinese communities found that even when self-service digital healthcare services approached or reached the level of human services in objective indicators such as image quality, efficiency, security, and convenience, residents’ preferences still significantly favored human-operated modes. Distrust of self-service results was significantly associated with refusal to use. 43 Thus, patient adoption of self-service systems requires not only sufficient demonstration of system advantages in efficiency and convenience but also active trust-building efforts by healthcare providers.44,45 Meanwhile, existing research frameworks still show obvious gaps: Systematic reviews indicate that 73.5% of studies used unidimensional measurements, 42.9% failed to clearly define trust, and scales were mostly transplanted from non-healthcare fields, making it difficult to capture the complexity of digital trust. 32 Digital health research has also long overlooked patient perspectives and participatory design, further limiting the explanatory power for trust formation mechanisms. 44
Theoretical foundation
The Organizational Trust Model proposed by Mayer et al. 36 explains the cognitive mechanisms underlying trust formation. According to this theory, trust represents the psychological state in which the trustor willingly assumes corresponding vulnerability based on expectations of the trustee's behavior. This process depends on the trustor's perception of the trustee across three key dimensions of ability, benevolence, and integrity, which reflect the trustee's competence, goodwill, and adherence to acceptable standards, respectively. In subsequent research, the three-dimensional structure of Organizational Trust Model is often flexibly applied, and focusing on certain dimensions in specific contexts is also an acceptable approach.46–48
Additionally, Mayer et al. 36 highlights Propensity to Trust as a stable, cross-situational tendency to trust others or systems that shapes initial trust when specific information is scarce and conditions sensitivity to trustee attributes; this tendency varies with developmental experiences, personality, and culture along a continuum from blind trust to universal suspicion. In digital settings, individual differences in technology acceptance and trust tendencies are specific manifestations of Propensity to Trust.49,50 Organizational trust theory also emphasizes the behavioral consequence of trust as risk taking in relationships: Once trust is formed, actors accept greater relational risk, cooperate more, and show fewer defensive reactions. 36 In healthcare services, patients who trust a provider reduce skepticism and resistance toward treatment plans, which improves cooperation.28,51
Organizational trust theory has begun to be applied in the digital healthcare field,52–54 but these applications are relatively new, and the theory faces important considerations in digital environments. First, the theory's original authors acknowledge that their model represents a cognitive trust approach, while emotions do indeed affect the perception of trust antecedents. 55 From a user psychology perspective, when patients face technological interfaces that cannot provide emotional feedback, their emotional states may be amplified and influence their perceptual judgments of system capabilities,56,57 while traditional cognitively oriented models may underestimate such emotional influences. Second, trust research reviews indicate that early studies, including organizational trust theory, tend to study trust statically as a state at a single point in time. 58 In digital healthcare environments where system functions are frequently updated, this static perspective has difficulty fully capturing the dynamic characteristics of trust. 59 Despite these considerations, organizational trust theory still provides an important foundation for understanding trust dynamics in digital healthcare environments, particularly having expansion value in specific technological contexts and cross-cultural applications.55,58
To complement the understanding of trust attribution mechanisms, this study introduces Trust Transfer Theory, 24 The theory suggests that when individuals encounter two objects with structural or brand-related associations, they may extend the trust formed toward one object to the other, particularly in situations where direct experience with the latter is lacking.24,60 The trust transfer mechanism posits that trust is not only derived from direct contact experiences but can also be transferred through associations between objects, and this extension of trust typically follows certain patterns. 24 For example, patients may trust a system because they trust the doctor who uses it.61,62 In healthcare service research, this theory has been used to explain how patients extend their trust in self-service platforms, remote platforms, or frontline staff to the entire healthcare institution,63–65 In digital contexts, a strictly one way linear view is questionable because constructs such as perceived usefulness and attitude can be both antecedents and outcomes of trust, and PSR may both reflect and reshape evaluations of technical features.66,67 Despite these considerations, trust transfer remains a useful basis for understanding how technical trust becomes organizational trust.
Therefore, Organizational Trust Theory, together with Trust Transfer Theory, provides a framework for understanding patient trust formation and its behavioral implications in digital healthcare environments. It explains how technological characteristics shape cognitive trust and how that trust transfers from the technical system to the organizational level through a transmission effect, shaping patient behavior. Figure 1 presents the research framework.

Research framework.
Hypothesis development
TC reflects the operational capability and service efficiency of self-service systems.4,5 In organizational trust theory, Ability denotes the skills, knowledge, and capabilities a trustee uses to complete domain-specific tasks. 36 When patients use hospital self-service systems for appointments, payments, and inquiries, usability, response speed, and functional completeness directly signal capability. 68 Patients judge capability by whether the system is user-friendly, fast, and convenient. 69 Ng et al. 12 found that intuitive interfaces, simple operations, and smooth interactions significantly enhance patients’ trust and satisfaction, improving their evaluations of system reliability. Hou et al. 70 further confirmed that when users perceive processes and interactions as convenient, they are more likely to develop trust in the system and form positive views of its professionalism and reliability.
TSIQ correspond to the core of the Integrity dimension.4,71 Mayer et al. 36 point out that Integrity concerns alignment between actions and commitments and adherence to standards acceptable to the trustor. 36 In self-service system design, hospitals assume responsibilities for information security, accurate data transmission, and reliable service provision.72,73 Patients’ perceptions of whether these responsibilities are fulfilled shape views of system stability. 74 Information security and quality are foundational to system reliability, 75 and the security of technical systems and information quality significantly predict users’ trust in the system. 76 This fit between stated commitments and actual performance informs judgments of Integrity and, in turn, overall perceptions of system reliability.
Based on this, the present study proposes the following hypothesis:
H1: TC has a positive impact on PSR
H2: TSIQ have a positive impact on PSR
According to Trust Transfer Theory, when individuals establish relationships between two objects that are structurally or brand-related, their trust in one party can be transferred to the other, particularly in situations where there is a lack of direct interaction experience, and this transfer effect is even more pronounced.24,77 In digital hospital service contexts, patients typically use self-service systems as their first point of contact with healthcare institutions, the performance of these systems not only influences users’ judgments about the systems themselves but also subtly shapes their perceptions and evaluations of the hospital's overall service quality. 5 Specifically, patients view the operational stability, functional reliability, and information processing capabilities of self-service systems as direct indicators of a hospital's technical capabilities and service standards. 65 Existing research indicates that the reliability of technical systems significantly enhances patients’ overall trust in healthcare providers. 25 Furthermore, in the absence of face-to-face interaction with healthcare providers during the service process, patients are more likely to infer the overall credibility of healthcare providers based on their experience with self-service systems, thereby completing the trust transfer process. 78
Based on this, the present study proposes the following hypothesis:
H3: PSR has a significant positive impact on GTHP
According to organizational trust theory, trust is not merely a cognitive evaluation state but also serves as a behavioral motivator, with its core function lying in mechanisms that promote risk-taking and reduce defensive reactions. 36 In the high-uncertainty, high-professional-barrier context of healthcare services, patients often face treatment decisions that exceed their knowledge base, making trust a crucial psychological foundation for accepting treatment recommendations and cooperating with medical procedures.79,80 Specifically, when patients develop a high level of trust in healthcare providers, their recognition of medical professionalism is stronger, thereby reducing uncertainty and skepticism toward the treatment process. 81 Additionally, trust not only helps alleviate psychological hesitation but also enhances patients’ subjective motivation and actual behavioral performance in overcoming practical obstacles such as time conflicts, complex procedures, or operational difficulties. 82 Previous studies have indicated that patients with strong trust are more likely to proactively adjust their personal schedules to accommodate medical arrangements, thereby improving treatment adherence.83,84
Based on this, the following hypotheses are proposed:
H4: GTHP has a significant negative impact on UDT
H5: GTHP has a significant negative impact on PBs
Research shows that convenient technological experiences significantly enhance patients’ perceptions of providers’ service philosophy and management standards, which underpin trust formation. 85 Chen et al. 86 further confirmed that technological convenience directly predicts patients’ trust in healthcare providers. Patients interpret technological convenience as evidence that providers prioritize patient needs and pursue service efficiency. 87 Perceptions of TSIQ directly affect patients’ trust evaluations. 88 Robust data security and high-quality information services are indicators of provider professionalism and responsibility. 89 Daraz et al. 90 found that the quality of institutional information is a key factor in patients’ overall assessment of provider credibility.
Additionally, trust transfer theory suggests that individuals can extend trust from one entity to structurally related entities through cognitive inference processes. 24 Applied to healthcare, when patients treat the digital system and the hospital as a single system of responsibility and capability, trust in the system generalizes into trust in the hospital as a whole.91–93 Patients’ perceptions of TC and TSIQ not only generate direct trust effects but also form more stable organizational-level trust judgments through the cognitive mediation of PSR. 94 This indirect pathway transforms trust based on specific functions into systematic evaluations of providers’ technical capabilities and service standards.95,96 Research by Barua et al. 97 suggests that perceived reliability can function as a mediating mechanism through which technical features shape users’ trust in technology-driven services. Groves et al. 98 also noted that patients’ perceptions of system technical reliability significantly enhance their trust judgments at the organizational level, particularly when encountering automated or telemedicine mechanisms.
Based on the direct and mediating effects of technical characteristics, this study proposes:
H6: TC has a direct positive impact on GTHP
H7: TSIQ have a direct positive impact on GTHP
H8: PSR mediates the impact of TC on GTHP
H9: PSR mediates the impact of TSIQ on GTHP
Individual differences in trust propensity may significantly influence technological trust formation processes.99,100 This study therefore introduces DD as a moderating variable. Organizational trust theory holds that propensity to trust shapes how people attend to and interpret trustee characteristics. 36 DD denotes negative expectations about the stability and information control of digital systems and can be viewed as the inverse manifestation of trust propensity in digital contexts.101,102 In healthcare, DD is most evident around privacy, data security, and system reliability.103–106 Some patients also report skepticism about information accuracy, the dependability of technological systems, and institutional intentions.107–109
When DD is high, even self-service systems with good information security and technical quality may still be judged as unreliable by risk-sensitive users.94,110 Liu and and Wang 111 found that trust attribution is shaped by users’ internal interpretations of system explanations, regardless of the underlying technical mechanism, indicating that negative predispositions such as DD can undermine the effectiveness of otherwise trustworthy features. Therefore, DD is expected to weaken the positive effect of TSIQ on PSR, reflecting the moderating role of trust orientation in digital healthcare. This moderating effect is expected to be less pronounced for TC and strongest for TSIQ, because DD is driven by concerns about opaque system processes, whereas convenience is directly experienced and readily evaluated.4,112
Based on this, the present study proposes the following hypothesis:
H10: DD negatively moderates the effect of TSIQ on PSR
Method
Measurement tools
Following established methodological requirements for structural equation modeling and validated approaches from previous research, this study employed scales adapted from previously validated instruments for measurement.113,114 TC and TSIQ were measured using scales adapted from Ganguli and Roy 115 and Zhang et al, 4 comprising 6 items each (TC1-TC6, TSIQ1-TSIQ6) to assess the convenience, safety, and information quality of hospital self-service systems. DD was measured using the scale from Ezeudoka and Fan, 102 which includes 3 items (DD1-DD3) to assess patients’ level of distrust toward digital technology. PSR was measured using the scale from Barua et al., 97 which includes 5 items (PSR1-PSR5) to assess patients’ perception of the reliability of hospital self-service systems.
GTHP was measured using the scale from Richmond et al., 116 which includes three items (GTHP1-GTHP3) to assess patients’ trust in healthcare providers’ delivery of medical services. PBs and UDT were measured using scales from Kirby et al., 84 which include 4 items (PB1-PB4) and 5 items (UDT1-UDT5), respectively, to assess the PBs patients encounter when using healthcare services and their uncertainty and doubts about treatment.
A pilot test was conducted with 64 participants prior to the main data collection to ensure item clarity and preliminary reliability, exceeding recommended sample sizes for pilot studies. 117 The pilot test confirmed adequate reliability (all Cronbach's α > 0.70) and comprehensibility of all measurement items. 114 All scales employed a 7-point Likert scale ranging from “1 = Strongly Disagree” to “7 = Strongly Agree” to enhance measurement reliability and validity.118–120 The full set of 32 measurement items employed in this study is presented in Table 1.
Measurement items and constructs.

Note. All items were measured on a 7-point Likert scale ranging from “1 = Strongly Disagree” to “7 = Strongly Agree”. TC: technical convenience; TSIQ: technical safety and information quality; DD: digital distrust; PSR: perceived systems reliability; GTHP: global trust in healthcare providers; PB: practical barriers; UDT: uncertainty and doubts about therapy.
Research design and data collection
This cross-sectional study was conducted from June 1 to June 9, 2025. The study employed questionnaire data collection methods through two primary channels. First, an online questionnaire was distributed via wjx.cn, a well-known Chinese online survey platform, yielding 203 valid responses. The platform randomly distributes questionnaires to its user base and includes quality control procedures and informed consent mechanisms to ensure data reliability and ethical compliance.121–123 Second, with assistance from Luoyang First People's Hospital and its affiliated hospitals in Luoyang, Henan Province, China, in contacting patients, an online questionnaire was distributed through QR code scanning, yielding 107 valid responses. The combined sample resulted in 310 valid questionnaires for structural equation modeling analysis using SmartPLS 4.0 software.
Respondent inclusion criteria were: (1) Adults aged 18 years or older; (2) hospital visits at least once in the past three months; (3) use of hospital self-service systems during visits, including self-service registration machines, self-service payment, mobile appointment booking, or electronic medical record inquiry; (4) voluntary participation in the study.
Ethical considerations
This study adhered strictly to the ethical principles of the Declaration of Helsinki, with approval number EC-2025-0601. All participants provided written informed consent prior to participation. The study purpose and data use were disclosed transparently to all respondents to ensure full understanding and voluntary participation. All personal information was anonymized, and data privacy was strictly protected. Respondents retained the right to withdraw from the study at any time.
Sample characteristic
As shown in Table 2, the final sample comprised 310 valid questionnaires. Gender distribution showed 172 female respondents (55.48%) and 138 male respondents (44.52%). Age distribution revealed the 41–50 age group as the largest segment with 96 respondents (30.97%), followed by the 31–40 age group with 78 respondents (25.16%), the 51–60 age group with 72 respondents (23.23%), the 18–30 age group with 35 respondents (11.29%), and the 60 and above age group with 29 respondents (9.35%). Educational attainment showed 112 respondents (36.13%) with bachelor's degrees, 95 respondents (30.65%) with associate's degrees, 78 respondents (25.16%) with high school diplomas or below, and 25 respondents (8.06%) with master's degrees or above. Monthly income distribution indicated that 112 respondents (36.13%) earned between 2500 and 4000 yuan, 89 respondents (28.71%) earned between 4001 and 6000 yuan, 58 respondents (18.71%) earned below 2500 yuan, 38 respondents (12.26%) earned between 6001 and 8000 yuan, and 13 respondents (4.19%) earned above 8000 yuan. Medical visit frequency showed that 156 respondents (50.32%) visit doctors 2–3 times per year, 89 respondents (28.71%) visit 4–6 times per year, 45 respondents (14.52%) visit once per year, and 20 respondents (6.45%) visit more than 6 times per year.
Demographic characteristics of respondents.

Findings
Common method bias assessment
To ensure data quality, common method bias was assessed through multiple approaches. Multicollinearity was evaluated using variance inflation factor (VIF) values, with results showing VIF values for all paths ranged from 1.000 to 1.714, well below the critical threshold of 5.0.124,125 These findings indicate no severe multicollinearity issues among model variables, confirming that predictor variables maintain relatively independent explanatory roles for the dependent variable.
Additionally, potential common method bias was evaluated using Harman's single-factor test. Results indicated that the first principal component explained 34.2% of variance, below the critical threshold of 50%. 126 To provide further verification, we conducted supplementary analysis using the measured latent marker variable technique following by Miller and Simmering. 127 Comparison of models with and without the marker variable showed minimal changes in R² values (maximum change = 0.012) and path coefficients (maximum change = 0.010). These findings collectively suggest no serious common method bias in the study data, confirming acceptable data quality.
Measurement model evaluation
Measurement model reliability was assessed using Cronbach's α and composite reliability (CR) metrics. As shown in Table 3, Cronbach's α values for all measurement items ranged from 0.799 to 0.941, substantially exceeding the recommended threshold of 0.70. 124 CR values for constructs ranged from 0.871 to 0.958, all exceeding the recommended standard of 0.70. 124 These results demonstrate good internal consistency reliability for the measurement tools employed.
Reliability and validity analysis of the measurement model.

Note. AVE: average variance extracted; TC: technical convenience; TSIQ: technical safety and information quality; DD: digital distrust; PSR: perceived systems reliability; GTHP: global trust in healthcare providers; PB: practical barriers; UDT: uncertainty and doubts about therapy.
Convergent validity was examined through factor loadings and average variance extracted (AVE) for each measurement item. As shown in Table 3, AVE values for each construct ranged from 0.576 to 0.850, all exceeding the recommended standard of 0.50. 128 Factor loadings for most measurement items exceeded the recommended threshold of 0.70.129,130 Although the standardized factor loading for measurement item PSR2 was 0.698, slightly below the typical threshold of 0.70, this item was retained as the construct's AVE and CR already met established criteria.131,132
Discriminant validity
Discriminant validity was evaluated using Fornell–Larcker criteria and HTMT ratio analysis. As shown in Table 4, Fornell–Larcker criteria analysis showed that the square root of AVE for alFl constructs exceeded the correlation coefficient between that construct and other constructs, meeting established discriminant validity criteria. 128
Discriminant validity analysis (Fornell–Larcker criterion and HTMT ratio).

Note. Bold diagonal values represent square root of AVE for each construct. Off-diagonal values below the bold diagonal represent inter-construct correlations (Fornell–Larcker criterion). AVE: average variance extracted; TC: technical convenience; TSIQ: technical safety and information quality; DD: digital distrust; PSR: perceived systems reliability; GTHP: global trust in healthcare providers; PB: practical barriers; UDT: uncertainty and doubts about therapy.
HTMT ratio analysis revealed all values between constructs ranged from 0.201 to 0.838, well below the recommended threshold of 0.90. 133 These findings confirm good discriminant validity between different constructs, indicating that the study constructs are conceptually well-differentiated.
Hypothesis testing
As shown in Table 5, all proposed hypotheses received statistical support. Direct effects analysis reveals that TC (β = 0.204, t = 2.592, p = 0.010) and TSIQ (β = 0.432, t = 6.422, p = 0.000) significantly enhance PSR, supporting H1 and H2. PSR exhibits a strong positive impact on GTHP (β = 0.521, t = 9.021, p = 0.000), supporting H3. GTHP significantly reduces both UDT (β = −0.234, t = 4.953, p = 0.000) and PBs (β = −0.410, t = 8.393, p = 0.000), supporting H4 and H5.
Hypothesis testing results.

Note. TC: technical convenience; TSIQ: technical safety and information quality; DD: digital distrust; PSR: perceived systems reliability; GTHP: global trust in healthcare providers; PB: practical barriers; UDT: uncertainty and doubts about therapy.
TC and TSIQ also demonstrate direct effects on GTHP. TC (β = 0.207, t = 3.136, p = 0.002) and TSIQ (β = 0.131, t = 2.172, p = 0.030) both directly influence GTHP, supporting H6 and H7. Regarding mediating effects, PSR significantly mediates the effects of TC (β = 0.106, t = 2.566, p = 0.010) and TSIQ (β = 0.225, t = 5.455, p = 0.000) on GTHP, supporting H8 and H9.
DD significantly negatively moderates the effect of TSIQ on PSR (β = −0.191, t = 3.049, p = 0.002), supporting H10.
The R² values for the endogenous constructs showed varying explanatory capacity. GTHP (R² = 0.528) and PSR (R² = 0.361) demonstrated acceptable explained variance, while PBs (R² = 0.168) and UDT (R² = 0.055) showed relatively low explained variance. 114 These results will be discussed in the discussion section.
Moderation effect analysis
To further understand the moderating role of DD, this study constructed a moderation effect diagram as shown in Figure 2. The Figure 2 illustrates how the strength of the influence of TSIQ on PSR varies at different levels of DD (mean minus one standard deviation, mean, and mean plus one standard deviation). The results indicate that when DD is at a low level (mean minus one standard deviation, red line), the positive influence of TSIQ on PSR is strongest, with the steepest slope. When DD is at a moderate level (mean, blue line), this positive influence weakens. When DD is at a high level (mean plus one standard deviation, green line), the positive impact of TSIQ on PSR further weakens, with the gentlest slope.
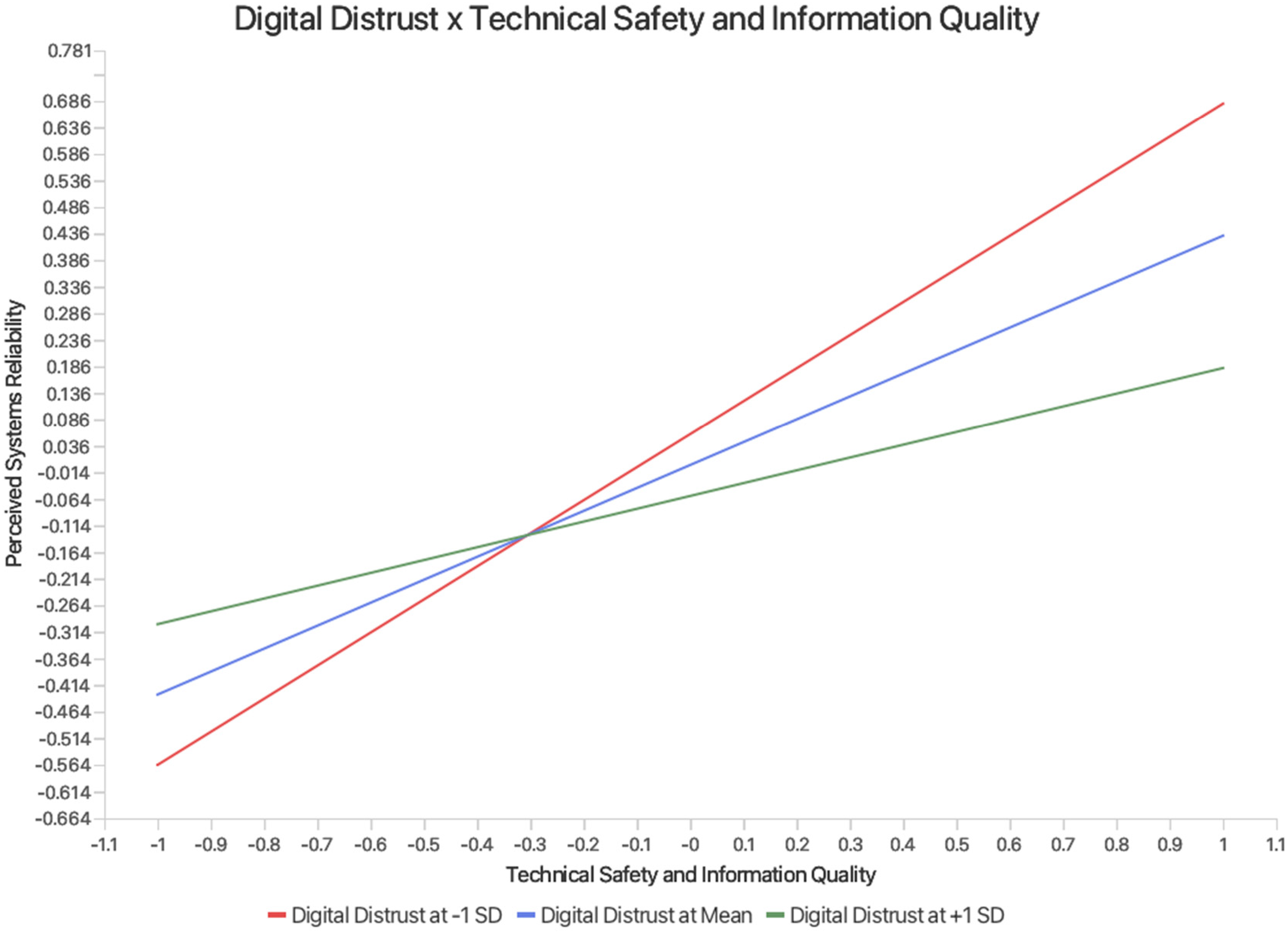
Moderating effect of digital distrust on the relationship between technical safety and information quality and perceived systems reliability.
This result validates Hypothesis H10, which states that DD significantly negatively moderates the impact of TSIQ on PSR. Specifically, the higher the level of patients’ distrust in digital technology, the weaker the promotional effect of TSIQ on the perception of system reliability. This indicates that DD weakens the positive effects of TSIQ, highlighting the need for healthcare institutions to pay special attention to addressing patients’ concerns about digital technology when promoting self-service systems.
Simple slope analysis (at DD = −1, 0, +1 SD) revealed practical thresholds for the moderating effect. When DD reaches approximately 1.74 standard deviations above the mean, the conditional slope of TSIQ on PSR decreases to a minimal level (β ≤ 0.10). At 2.26 standard deviations above the mean, the slope approaches zero, indicating that further improvements in safety and information quality yield no meaningful gains in perceived reliability for patients with very high DD.134,135
Discussion
This study, based on organizational trust theory and trust transfer theory, examined how TC and TSIQ of hospital self-service systems influence patients’ trust in healthcare providers and the role of such trust in improving treatment adherence. The study identified two interrelated key findings: First, PSR plays a crucial mediating role in the process of establishing patients’ GTHP, exerting a strong positive influence (β = 0.521, p < 0.001), making it the most important single pathway in the entire trust chain. Second, organizational trust established through self-service systems is significantly associated with improved patients’ treatment adherence, including lower levels of UDT and fewer PBs.
When analyzing the mechanisms through which TC and TSIQ influence GTHP, the data revealed an unexpected finding: These two constructs follow entirely different influence pathways. The direct effect of TC on GTHP (β = 0.207, p = 0.002) was significantly stronger than its mediating effect through PSR (β = 0.106, p = 0.010). In contrast, TSIQ primarily exert their effects through the mediating path, with their indirect effect through PSR (β = 0.225, p < 0.001) far exceeding their direct effect (β = 0.131, p = 0.030). This difference reflects fundamental disparities in how patients process TC and TSIQ in healthcare environments. Convenience, as an intuitive and perceptible feature, allows patients to immediately experience and quickly form judgments about the hospital's overall service capabilities, 136 thus more directly influencing trust in healthcare providers. Safety, as a relatively hidden technical feature, is difficult for patients to directly perceive its quality level. 137 Therefore, patients tend to integrate their perceptions of information security and quality into a comprehensive assessment of the system's overall reliability, and then indirectly establish trust in healthcare providers through this perception of system reliability. 138
This cognitive pattern difference can be further understood from the characteristics of the Chinese healthcare service context. Previous studies have found that in China, convenience and practicality are often important considerations in patients’ decisions to share health information. 139 While safety is also a concern, it is typically not the primary decisive factor. In this context, TC, as a directly perceivable and experiential functional feature, is more easily recognized by patients and converted into an intuitive judgment of the hospital's service level, thereby being associated with a stronger direct trust effect. In contrast, TSIQ are more often viewed as necessary safeguards rather than differentiating advantages. Patients need to evaluate the overall performance of self-service systems comprehensively to convert safety into trust in the hospital, thereby showing stronger mediating effects. This differentiated cognitive pathway reveals that the trust effects of TC and TSIQ exhibit distinct hierarchical and conditional characteristics, a phenomenon that is particularly pronounced in specific cultural contexts. This pattern could be understood within the cultural context of higher power distance in China's healthcare system.140,141 In this environment, patients may be accustomed to accepting the authoritative position of healthcare institutions and are more inclined to directly attribute good performance of technological systems to the overall capabilities of hospitals, thereby amplifying the trust transfer effect from technological systems to the organizational level.
The cross-cultural applicability of these mechanisms requires careful evaluation. In jurisdictions with strict data protection regulations like the EU GDPR, patients may have stronger demands for transparency and control, whereby safety and information quality cues might carry greater relative weight in trust formation.142–144 Some cross-national studies also suggest that different countries exhibit variations in privacy expectations and adoption intentions regarding contact tracing applications. 145 Furthermore, at the technological ecosystem level, the prevalence of payment and digital services varies across countries, which may alter the baseline for convenience and subsequently influence the role of the same convenience features in trust formation. 146 Given differences in institutional environments, governance frameworks, and technological ecosystems, the relationship between patient trust and healthcare institutional technology may manifest differently across contexts.
DD exhibits a significant negative moderating effect (β = −0.191, p = 0.002). According to organizational trust theory, an individual's propensity to trust significantly influences their perception and interpretation of trustee characteristics. DD, as the opposite manifestation of trust propensity in digital environments, reflects patients’ overall distrust of digital health services. 102 The results indicate that for patients with high DD propensity, even if the hospital performs excellently in terms of TSIQ, their perception of PSR is still significantly inhibited. This phenomenon validates the theoretical prediction that individual differences influence the trust cognition process: The trustor's prior attitudes systematically modulate their evaluation of the trustee. 36 Specifically, for patients with high DD, even if TSIQ are well-performed, their improvement in PSR remains limited. This digital skepticism suggests potential challenges in medical contexts: Patients might be more likely to opt for traditional manual services, or may experience excessive caution and anxiety during use, potentially affecting their service experience and efficiency. 88 More importantly, this distrust of technological systems may be associated with reduced utilization of digital convenience services provided by hospitals, potentially limiting their access to technological benefits of technological advancements in healthcare. 147
The establishment of GTHP is associated with a significant reduction in patients’ resistance to treatment. The results confirm that trust in healthcare providers is negatively associated with patients’ UDT (β = −0.234, p < 0.001) and Perceived PBs (β = −0.410, p < 0.001). These two effects collectively confirm that organizational trust established through self-service systems is significantly associated with higher willingness to cooperate with treatment. More importantly, the effect of trust on PBs (β = −0.410) is significantly stronger than its effect on UDT (β = −0.234). This differential pattern may stem from the fundamental differences in the mechanisms underlying the formation of these two types of treatment barriers. For PBs, overcoming them primarily depends on patients’ personal willingness and behavioral decisions, which are governed by their subjective perceptions and judgments. 84 When patients develop trust in healthcare institutions, this trust may be associated with stronger motivation to cooperate, potentially encouraging them to adjust their personal schedules and overcome practical difficulties such as time conflicts.148,149 In this unidirectional decision-making process, trust plays a crucial motivational role.
In contrast, the alleviation of UDT exhibits a more complex formation mechanism. Studies by Wu et al. 80 and Kirby et al. 84 indicate that patients’ confidence in treatment plans often requires the combined influence of multiple factors, including the quality of doctor–patient communication, the doctor's professional explanations, and the degree of personalization of the treatment plan. Notably, the establishment of this confidence is inherently a bidirectional interactive process. Unlike PBs, which primarily depend on the patient's personal willingness, the alleviation of treatment doubts involves the transmission of medical expertise and adjustments to the patient's cognition, a process that requires the synergistic interaction of multiple complex factors. Therefore, in medical contexts, organizational trust alone has a relatively limited role in alleviating such doubts.
The explanatory boundaries of the model may reflect the complexity of treatment adherence mechanisms. While organizational trust showed significant associations with treatment barriers, the relatively low explained variance for UDT (R² = 0.055) and PBs (R² = 0.168) suggests that these constructs may be largely influenced by factors outside the technical trust framework. Although Hair Jr et al. 114 noted that acceptable R² thresholds vary across research contexts, with values as low as 0.10 considered satisfactory in certain disciplines,65,123 the observed explanatory power indicates the presence of unmeasured factors. These may include clinical variables (disease severity, treatment complexity), personal characteristics (health literacy, economic constraints), and contextual factors (healthcare accessibility, provider communication quality). While this reflects limitations of the current model, it may also reveal the complex network of factors between technology and patient treatment attitudes in the digital age, providing direction for future research to explore emerging human-machine trust mechanisms.
Based on the above analysis, the core finding of this study is the validation of PSR's key mediating role between TC and TSIQ and GTHP. PSR plays an important bridging role in transforming technical experiences into organizational trust, which is associated with treatment adherence through lower levels of UDT and PBs.
This finding suggests that in the design and management of hospital self-service systems, enhancing patients’ perception of the overall reliability of the system should be the core strategy for trust-building. By optimizing the technical experience to enhance perceptions of system reliability, thereby supporting organizational trust and treatment compliance, this constitutes the basic logic of trust management in digital healthcare environments.
Theoretical implications
This study integrates organizational trust theory and trust transfer theory to construct and validate path mechanisms through which technological systems influence patient organizational trust in digital healthcare environments. The framework expands and deepens existing trust theory in four key aspects. First, while previous studies have emphasized the importance of users’ trust in technical systems themselves in digital healthcare services.67,150,151 there remains a lack of mechanistic explanatory models to elucidate how this trust transfers to healthcare organizations. This study draws on trust-building logic in organizational trust theory to propose that technical systems serve as intermediary links connecting patients’ technical perceptions with their overall trust in healthcare organizations, thereby filling the gap in explaining the pathway from technical trust to organizational trust. Empirical results show that TC and TSIQ jointly influence GTHP through the mediating effect of PSR, highlighting the significant value of technical systems in organizational trust-building.
Second, this study introduces a structural path perspective based on trust transfer theory to explain how technological trust transfers to trust evaluations of organizations in digital healthcare contexts. Trust transfer theory suggests that individuals can extend their trust in one object to another associated object based on structural or brand-related associations. 24 In digital healthcare contexts, patients’ overall trust in healthcare institutions is often rooted in their interaction experiences with technological systems, and the perception of system reliability constitutes the key mechanism for this trust extrapolation. This process reflects that, in highly institutionalized digital healthcare environments, trust has shifted from traditional interpersonal foundations to reliance on technological structures. 152 In contexts of highly complex systems and significant information asymmetry, patients rely on “trusted access points” constructed by technical systems to facilitate trust transformation. 153 This study thus extends the applicability of trust transfer theory in high-tech dependency scenarios, revealing the intrinsic logic of structural trust pathways in organizational-level trust formation.
Third, building on organizational trust theory assumptions regarding trust propensity, this study explicitly identifies DD as a technical trust propensity variable in digital healthcare contexts,102,154 and incorporates it into the trust path structure to construct a moderation mechanism. Unlike traditional organizational trust models that set trust propensity as a background variable, 36 this study found that DD significantly interferes with the relationship between TSIQ and PSR at the path level, exhibiting structural-level moderation effects. This finding enriches the path moderation dimension of organizational trust theory and expands the applicability of trust transfer theory across different trust propensity groups, revealing how individual-level trust characteristics shape the effectiveness of technical trust transfer.
Fourth, based on the theoretical logic that trust reduces defensive reactions and enhances cooperative behavior, 36 this study introduced this mechanism into digital healthcare contexts for empirical testing, further confirming the behavioral functions of organizational trust in alleviating patients’ treatment doubts and operational barriers. The research results validate that overall trust significantly reduces patients’ skepticism and resistance during the treatment process, emphasizing that trust is not merely a psychological assessment but also an important psychological foundation driving cooperative and compliant behavior. This expansion clarifies the behavioral consequences of organizational trust in healthcare services, providing richer empirical support for its theoretical application in the digital health field.
Finally, this study further emphasizes the importance of conducting digital system trust research from the patient perspective in digital healthcare environments. User-perspective digital trust research in commercial contexts indicates that user trust is typically shared between platforms and merchants and can be restored through guarantee, reputation, or compensation mechanisms.155,156 For example, consumers can transfer their trust in self-operated e-commerce platforms to live streaming shopping scenarios. 157 Platform reputation can reduce risk perception and enhance trust in merchants. 158 In C2C e-commerce, third-party certification and perceived website quality can also facilitate trust transfer to unfamiliar sellers. 159 However, in healthcare environments, patient trust in systems directly extends to overall trust in hospitals and ultimately affects treatment adherence. Due to the high sensitivity of health and medical data, healthcare digital systems may cause severe and difficult-to-repair trust losses once they malfunction, making healthcare digital trust characterized by high value and low fault tolerance.160,161
Practical contribution
This study explores trust mechanisms in technological systems within digital healthcare contexts, providing findings relevant to individual, organizational, and policy considerations. At the individual level, the findings reveal that DD significantly weakens the positive influence of technological security and information quality on perceptions of system reliability, particularly among patients with higher levels of DD. Even when system performance is excellent, their trust remains notably suppressed. This cognitive bias might hinder patients from fully utilizing digital convenience services, potentially affecting their medical efficiency and treatment experience. Therefore, healthcare institutions can consider providing more actionable measures to enhance patient trust, such as appropriately simplifying operation interfaces in interface design to reduce costs for patients when using the system,162,163 adding real-time security prompts in self-service systems (such as “this data transmission has been encrypted”) to help patients more intuitively perceive that their personal information is protected, 164 while maintaining human service windows to provide necessary guidance and support for patients who have concerns about digital services. 165 These measures not only help enhance trust but may also improve patient treatment adherence to some extent. 166
At the organizational level, this study validated the differing pathways of technological convenience and technological security in organizational trust construction: The former directly enhances trust, while the latter primarily relies on the mediating pathway of system reliability perception. These findings suggest that managers could incorporate PSR as a core trust mechanism in performance evaluation or key performance indicators for digital projects, for instance by tracking system downtime, response times, or system reliability experiences collected through patient satisfaction scales to ensure continued attention to these issues. 161 Given the differences in digital system trust levels among different groups, hospitals might also consider appropriately deploying digitally literate staff to provide basic guidance or training for patients with low motivation to use digital services, which may help enhance their trust in digital systems, improve user experience, and support service equity. 167
At the policy level, this study suggests that evaluation of digital healthcare service systems should not be limited to technical performance and operational functionality but could also consider incorporating patients’ system trust pathways. Research findings indicate that organizational trust built through technical experiences not only enhances patients’ overall acceptance of services but also effectively alleviates doubts and resistance during treatment, thereby improving compliance outcomes. Therefore, policymakers may need to consider incorporating trust-related mechanisms into evaluation and regulatory frameworks, such as adding patient trust measurements to performance assessments or quality evaluation systems, and further strengthening institutional development for data security and privacy protection to consolidate the public's trust foundation in digital healthcare systems. Meanwhile, for groups with lower trust levels, it may be necessary to provide brief digital support measures when needed to avoid structural risks arising from DD. 168
Conclusion
This study examined a phenomenon in digital healthcare environments where human-machine interactions between patients and hospital self-service systems play a role in patients’ formation of trust in healthcare institutions. The finding that PSR serves as a mediating mechanism suggests that in highly digitized healthcare environments, technical system characteristics may influence the cognitive pathways through which patients establish institutional trust. This phenomenon reflects the importance of technological systems’ role in healthcare services, where technical systems are no longer merely tools but become a window through which patients evaluate the credibility of healthcare institutions, subsequently affecting their treatment adherence. It is noteworthy that for patients with higher levels of DD, the effectiveness of this process may differ. This study provides a theoretical perspective for trust mechanism research in digital healthcare environments while offering some practical references for healthcare institutions’ digital development. Future research could further validate these findings across different cultural contexts and healthcare systems and employ longitudinal designs to deepen understanding of causal relationships.
Limitation and future recommendation
This study has several methodological and contextual limitations. First, the sampling approach may introduce systematic bias. Online questionnaires and in-hospital QR codes are more likely to reach patients familiar with digital technology, potentially excluding those with lower digital literacy. The sample also skewed toward middle-aged and higher-educated populations, and interaction patterns among elderly or low-income groups may differ, thereby weakening the representativeness of the results. Second, the cross-sectional design and complete reliance on self-reporting jointly limit causal inference. Although common method bias testing was conducted, social desirability bias and recall bias may still exist, and the lack of objective behavioral data validation further weakens the strength of causal claims. Third, the model's explanatory power has limitations, particularly the relatively low explained variance for treatment adherence-related constructs, suggesting the presence of important factors not included in the model. Finally, the research context primarily derives from China's healthcare environment, and cultural and institutional differences may affect cross-cultural applicability; meanwhile, this study focuses on hospital self-service systems, and the applicability of conclusions to other digital healthcare technologies remains to be verified.
Future research can advance in the following directions to address these limitations. First, adopt short-cycle longitudinal designs, completing two follow-ups within the same institution, tracking changes from initial contact to repeated use, and controlling baseline characteristics to enhance causal inference. Second, combine mixed methods through semi-structured interviews or focus groups to supplement cognitive and emotional explanations for the mechanism of technical trust transfer to organizational trust, and deeply explore other important factors affecting treatment adherence. Third, introduce objective behavioral data under compliance conditions, such as system usage logs and appointment attendance rates, for triangulation with self-report scales. Fourth, improve sampling strategies through offline questionnaires or telephone interviews, and collaborate with community health institutions to cover digitally underserved populations and compare trust formation differences across groups. Fifth, identify and measure potential confounding variables and develop more refined statistical control strategies.
Footnotes
Acknowledgements
The authors would like to thank the healthcare professionals at Luoyang First People's Hospital and its affiliated hospitals for their support in data collection. We also extend our gratitude to all participants who voluntarily completed the questionnaire and made this research possible.
Author contributions
LXZ was responsible for conceptualization, data collection, data analysis, and manuscript drafting.
WMHWH provided supervision, theoretical guidance, and critical revisions of the manuscript.
SHMA contributed to methodological validation and assisted with technical interpretation of the data.
All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.