
Abstract
Background
Social robots are increasingly used to support older adults living with dementia by providing not only reminders and companionship but also emotional support, engagement through conversation, and a sense of comfort. Engaging older adults living with dementia in the codesign process ensures that their unique needs and challenges are met, thereby enhancing the relevance and usability of these technologies. However, limited evidence exists on effective engagement strategies for codesigning with older adults living with dementia. This scoping review aims to explore the facilitators and barriers to codesigning social robots with older adults living with dementia.
Methods
Following the Joanna Briggs Institute scoping review methodology, we searched six databases including Medline, CINAHL, Web of Science, PsycINFO, IEEE Xplore, and Google Scholar (for grey literature). The inclusion criteria focused on studies involving older adults with dementia in the codesign of social robots. After screening 513 records, six studies met eligibility criteria. Data extraction covered study characteristics, codesign activities, and identified facilitators and barriers.
Results
The analysis identified three facilitators: adapted methods for people with dementia, the application of theoretical frameworks to guide codesign, and the inclusion of caregivers in the codesign process. Identified barriers included: unclear roles and information, unfamiliar and uncomfortable environments, and a lack of diversity among participants.
Conclusions
This scoping review underscores the need for evidence-based frameworks and inclusive strategies to support the meaningful involvement of older adults living with dementia in social robot codesign. Addressing identified barriers and leveraging facilitators can enhance engagement and ensure that social robots better align with the lived experiences and needs of this population. Future research should explore supportive approaches that promote a more collaborative and dementia-friendly design process.
Introduction
Individuals living with dementia have diverse physical, emotional, and communication needs. 1 Social robots are designed to support these needs by offering interactive and personalized experiences.2,3 They serve a range of functions, including providing conversation and companionship, 4 offering emotional support, 5 assisting with activities of daily living, 6 and promoting cognitive stimulation through activities such as memory games. 7 Additionally, social robots act as nonjudgmental conversational partners, helping reduce social isolation and stigma. 8 Social assistive robots (SARs), in particular, are developed to engage in social interactions while also offering task-oriented support, such as reminders and facilitation of therapeutic interventions. 9 To ensure these technologies are both effective and user-friendly, it is crucial to adopt a collaborative and inclusive design approach that centers on the lived experiences of people with dementia.
Codesign plays a crucial role in this process by actively involving end users in decision-making, ensuring that technology aligns with their needs and preferences. However, the terminology surrounding user involvement—cocreation, codesign, and coproduction—is often used interchangeably, leading to conceptual ambiguity.10–12 Vargas et al. 13 distinguish codesign as a participatory, multi-stakeholder approach to problem-solving that spans all phases of design, from problem identification to evaluation. In contrast, coproduction occurs primarily during the implementation phase, optimizing available resources. Within the context of social robots, codesign involves diverse stakeholders—including older adults with dementia (primary users), caregivers or relatives (secondary users), and staff, healthcare managers, and community members (tertiary users)—as equal partners throughout the design process. 10 This inclusive approach fosters meaningful engagement and ensures that social robots are developed to meet the real-world needs of their users.
Moreover, involving older adults with dementia in the codesign process is also ethically significant. 14 To facilitate meaningful engagement of older adults with dementia in the codesigning process, it is essential to incorporate core ethical principles, including autonomy, respect for personhood, informed consent, and the right to participate meaningfully. 15 The active involvement of individuals living with dementia ensures that technologies reflect their lived experiences, preferences, and needs, rather than being shaped solely by clinicians, caregivers, or designers.15–18 With appropriate support and ethical safeguards, their participation can foster empowerment and lead to the development of inclusive, person-centred social robots that are meaningful and supportive in their daily lives.3,18
Despite the benefits of codesign, several challenges exist. Older adults with dementia may experience difficulties articulating their needs or navigating the codesign process, making meaningful participation challenging. 16 Researchers may also face obstacles in recruiting a diverse group of participants across different stages of dementia and care settings. Additionally, implicit age-related biases may lead to assumptions about older adults’ ability to contribute to the codesign process, potentially resulting in social robots that do not fully address their needs. 17 Overcoming these barriers requires thoughtful facilitation, adaptive methods, and a commitment to inclusive engagement. 18
Engaging users in the codesign of social robots is essential in this rapidly advancing field, ensuring the robots are technologically sophisticated and closely aligned with the users’ needs, preferences, and emotional states. 19 Current social robots, such as PARO, Joy for All, Stevie, Tangy, and Mario, as well as telepresence robots, have benefited from feedback and experiences with their use from older adults with dementia and caregivers.20–24 However, there is limited knowledge about the codesign process in social robots, specifically involving older adults with dementia. 25
A systematic review of nine studies identified six key phases in codesign: (1) assessing background knowledge and evidence, (2) evaluating user needs to inform intervention and technology, (3) developing intervention content, (4) prototype testing, (5) real-world testing, and (6) implementation. 26 Notably, user involvement was predominantly concentrated in the later stages—prototype testing, real-world testing, and implementation—while early-stage engagement, such as assessing background knowledge and user needs, was largely overlooked. Similarly, a systematic review of codesign in technology 27 found that only one of 28 studies specifically focused on older adults with dementia, and that study developed heuristics rather than SARs. 28 Another review identified a study involving SARs but noted that people with dementia were not directly involved in the codesign process. 29 These gaps highlight a critical need for further research on codesigning social robots with older adults with dementia.
This scoping review aims to systematically map the existing literature on the facilitators and barriers to codesigning social robots with older adults living with dementia. By synthesizing current evidence, this scoping review aims to identify effective strategies that promote inclusive participation and enhance the codesign process for this population. The central research question guiding this review is: What has been reported in the literature regarding the facilitators and barriers to codesigning social robots with older adults living with dementia?
Methods
Our research team included a patient partner living with dementia (LJ), an academic researcher (LH), and five research trainees (IC, KW, SMK, YZ, and JW) from diverse disciplines, including nursing (LH, IC, SMK, JW), social work (KW), and medicine (YZ). The interdisciplinary nature of the team was a key strength of the study. Team members contributed diverse expertise, including ethics, inclusion, advocacy, and clinical knowledge of dementia. This range of perspectives enriched our understanding of the codesign process and ensured attention to both relational and practical dimensions of working with people living with dementia. The involvement of team members with lived experience of dementia enhanced the study's real-world relevance by grounding the work in the priorities of those most affected. The interdisciplinary collaboration enabled a comprehensive analysis of how codesign may support quality of life and helped us examine the relevance, acceptability, and real-world application of codesigned social robots for older adults living with dementia. All team members actively contributed to each stage of the scoping review, including study design, item selection, data extraction and analysis, and manuscript preparation. We met biweekly for one-hour discussions via Zoom to ensure collaborative decision-making.
A scoping review was selected to identify knowledge gaps and clarify key factors related to the concept of codesigning social robots with people living with dementia. The aim was to map the extent, range, and nature of the existing literature rather than to assess the quality of evidence or measure specific outcomes. A systematic review was deemed less suitable due to the heterogeneity in study designs, populations, and definitions of codesign, as well as the current lack of standardized outcome measures. Scoping reviews are particularly suited to exploring broad and under-researched topics.30,31 This scoping review followed the Joanna Briggs Institute (JBI) methodology, 32 which was originally proposed by Arksey and O’Malley 30 and further refined by Levac et al. 31
JBI methodology of scoping review is a widely adopted framework for scoping reviews in healthcare. A scoping review protocol was preregistered and published. 33 The review was conducted between November 2023 and December 2024. Ethics approval was not required as the study exclusively examined publicly available literature. To enhance methodological rigor and transparency, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) checklist 34 (Table S1).
Eligibility criteria
Participants
This review included studies involving older adults with dementia, defined as individuals aged 60 years and older with any form of dementia, in accordance with the World Health Organization 35 classification.
Concept
The scoping review is designed to map facilitators and barriers to codesigning the physical form of social robots with older adults with dementia. Social robots were classified based on their appearance and functions. 36 Appearance-based classifications distinguish robots by their physical form, ranging from humanoid robots designed to resemble humans to animal-like or abstract robotic designs. Function-based classifications categorize social robots according to their roles, such as companion robots (providing emotional support and social interaction), assistive robots (aiding with daily tasks like reminders and mobility support), and telepresence robots (facilitating remote communication between individuals). These classifications help determine the most appropriate design and interaction style for engaging older adults with dementia in meaningful and supportive ways.
Context
This scoping review considers both community and institutional settings. Community settings encompass nonmedical environments such as community centers, workplaces, libraries, schools, and workshops, where older adults with dementia may engage in social and recreational activities. Institutional settings included hospitals, assisted living facilities, and long-term care homes, where social robots may be integrated into daily care routines to provide companionship, cognitive stimulation, and task support. Given that codesigning social robots with older adults with dementia is an emerging research area, no geographical restrictions were applied to ensure a comprehensive and globally inclusive synthesis of available evidence.
Types of sources
This review considered literature published in English between January 2000 and December 2024, encompassing a wide range of sources to ensure a comprehensive understanding of the topic. Primary research studies, including qualitative, quantitative, and mixed-methods research, were included to capture diverse methodological approaches. Additionally, grey literature, such as opinion papers, policy documents, and reports, was considered to incorporate perspectives beyond traditional academic research.
Search strategy
Guided by the JBI scoping review protocol methodology, 32 we followed a three-step process to systematically identify relevant literature. First, a preliminary search was conducted in MEDLINE, CINAHL, and the JBI Database of Systematic Reviews and Implementation Reports to identify key terms and index terms related to dementia, codesign, and social robots. Next, a comprehensive search was performed using these identified keywords and index terms across MEDLINE, CINAHL, Web of Science, PsycINFO, IEEE Xplore, and Google Scholar, ensuring broad coverage of relevant studies. Lastly, hand searching was conducted by manually reviewing the reference lists of included studies to identify additional publications that met the inclusion criteria. A detailed search strategy table is provided in Supplementary File 1 (Table S2). To enhance methodological rigor, the first author (LH), an expert in dementia, codesign, and social robotics, supervised the search process. Additionally, a university librarian was consulted to refine the search strategy, optimize database selection, and validate search terms, ensuring a comprehensive and systematic approach to the literature search.
Study/source of evidence selection
All identified citations were collected and uploaded into the Covidence systematic review tool (Veritas Health Innovation Ltd, Melbourne, Australia), 37 where duplicates were removed. A total of 513 studies were initially retrieved through the comprehensive search. After removing duplicates, 439 studies remained for screening. Two research trainees (IC and SMK) independently reviewed the titles and abstracts of these studies, applying predefined inclusion and exclusion criteria (Table 1) to determine eligibility. Following this initial screening, full-text reviews and data extraction were conducted for the selected studies. Any discrepancies or disagreements during the screening and extraction process were resolved through discussion with a third reviewer (LH) to ensure consistency and accuracy in the selection of relevant studies.
Inclusion and exclusion criteria.
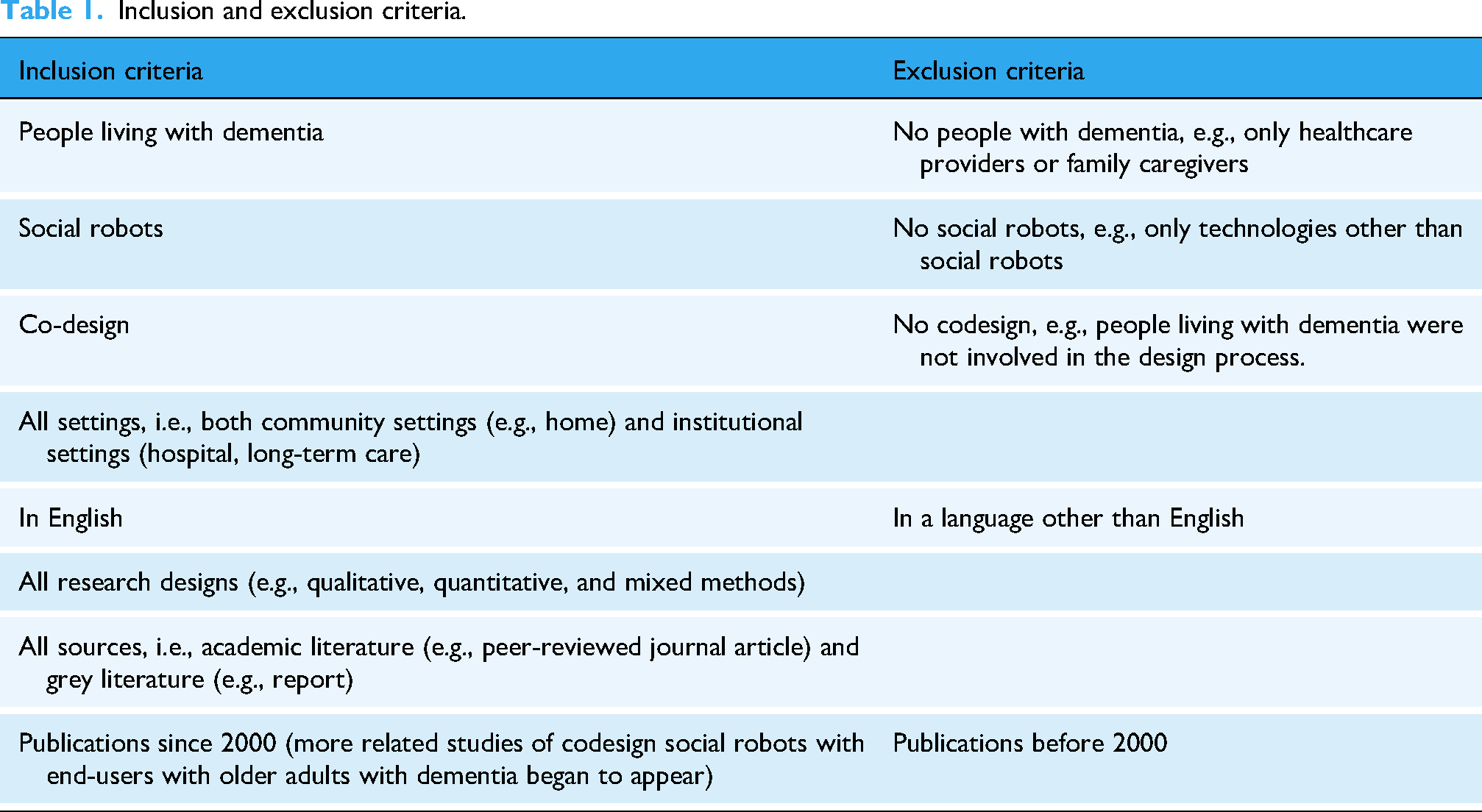
A total of 424 items were excluded, leaving 15 studies for further assessment. Two research trainees independently conducted full-text reviews of the selected studies, applying the predefined inclusion and exclusion criteria. Nine articles were excluded for the following reasons: incorrect population (not involving people with dementia, n = 4), lack of codesign (n = 2), and irrelevance to social robots (n = 3). Based on feedback from the research team, including insights from our patient partner with lived experience (LJ) and the academic researcher with expertise in dementia, codesign, and social robotics (LH), six studies were included in the final review. Figure 1 presents the PRISMA flow diagram, detailing the study selection process.

PRISMA flow diagram.
Data extraction
We organized the selected articles into a spreadsheet, capturing key details such as author, publication year, country, context, research design, population, sample size, codesign activities, social robots, and identified barriers and facilitators. This structured approach enabled consistency in data collection and facilitated comparative analysis across studies.
Data synthesis and analysis
A narrative synthesis approach was employed to integrate findings from studies with varying designs and reporting styles. By summarizing results narratively, we ensured alignment with the study objectives and research questions. We then performed reflexive thematic analysis guided by Braun et al.. 38 Data extracted from the selected articles were systematically analyzed and categorized into emerging themes to identify patterns across studies. Two team members (IC and JW) independently conducted data extraction and thematic analysis, followed by collaborative discussions on the synthesis and analysis with the entire research team. This iterative process ensured rigor by incorporating diverse perspectives and refining thematic interpretations. The team discussion, including members with lived experience, clinicians, and academic experts, ensured the themes were conceptually sound, grounded in the data, and reflective of diverse perspectives. Final themes were refined through consensus, contributing to a rich and nuanced understanding of the topic.
Results
The scoping review identified six studies that met the eligibility criteria for exploring the codesign of social robots with people living with dementia. The characteristics of the studies and relevant data related to the review questions were summarized in Table 2. The studies were conducted in the USA (n = 2),18,39 Mexico (n = 1), 40 Canada (n = 1), 6 the UK (n = 1), 41 and a joint study between South Korea and New Zealand (n = 1). 5 In terms of study design, five studies employed qualitative methodologies,5,6,18,39,41 while one study utilized a mixed-methods approach. 40
Summary of studies in scoping review.

Population, sample size, and setting
The studies included in this review had relatively small sample sizes, comprising a total of n = 55 older adults living with dementia, with a range of 5‒12 participants per study. Not all studies explicitly described the stages of dementia or provided detailed demographic characteristics of participants. These studies highlight the diverse settings in which social robot codesign takes place, including home environments, memory care facilities, retirement villages, and simulated home labs, reflecting different contexts of dementia care and engagement.
Codesign sessions and social robots
All six studies included a robot testing phase, though the duration of interactions varied. Wang et al. 6 asked participants to complete two daily activity tasks with a social robot, but the exact interaction time was not reported. Wairagkar et al. 41 conducted testing over 10 weeks, primarily gathering feedback from caregivers and two individuals living with dementia to assess the role of social robots in supporting health and well-being. However, direct codesign engagement with people living with dementia was not explicitly mentioned.
Gasteiger et al. 5 conducted a one-week home-based interaction phase, but the number of participants living with dementia in each phase was not specified. Hsu et al. 18 structured their codesign process into five weekly sessions, each lasting 45 min, during which participants interacted with social robots for 15‒45 min per session. Mitchell and Zhao 39 facilitated focus group discussions in which participants interacted with social robots for approximately two and a half hours. Cruz-Sandoval et al. 40 provided 14 sessions, each lasting 30 min, allowing participants to interact with a socially assistive robot in a structured therapeutic setting.
The types of social robots used in these studies varied significantly. One study tested a tele-operated robot designed to assist individuals with dementia in activities of daily living and instrumental activities of daily living. 6 Wairagkar et al. 41 developed a conversational robot and a digital social robot for mobile devices, featuring natural language processing and facial expression capabilities to engage users with daily questions and digital assistance.
Two studies designed and tested humanoid robots.5,18 Each humanoid robot served distinct daily care functions tailored to the needs of older adults and provided emotional and social support to people living with dementia.5,18 Mitchell and Zhao 39 utilized an AI-powered socially assistive robot for companionship and cognitive support. Cruz-Sandoval et al. 40 designed socially assistive robots that acted as therapy facilitators for older adults with dementia. These studies highlight the diversity in codesign engagement, robot functionalities, and testing durations, underscoring the importance of tailoring social robot interactions to the unique needs of older adults with dementia.
Facilitators and barriers to codesigning social robots with people living with dementia
Using thematic analysis, 38 two team members independently coded the extracted data from the selected studies. This process involved reading and rereading the data to gain familiarity, generating initial codes based on both explicit and implicit meanings within the data. These codes were then organized into meaningful categories that captured recurring concepts related to the facilitators and barriers of codesigning social robots with older adults living with dementia. Next, the researchers grouped these categories into preliminary themes. The themes were then discussed and iteratively refined with the whole research team. Our analysis identified key facilitators and core barriers to the codesign of social robots with people living with dementia (Figure 2). The primary facilitators include adapted methods tailored to address the needs of older adults living with dementia, the application of theoretical frameworks to guide the codesign process, and the inclusion of caregivers to support communication and engagement. Conversely, significant barriers include unclear roles and information, unfamiliar and uncomfortable environments, and a lack of diversity among participants, which limits the representativeness of findings. These factors are explored in detail in the following section.
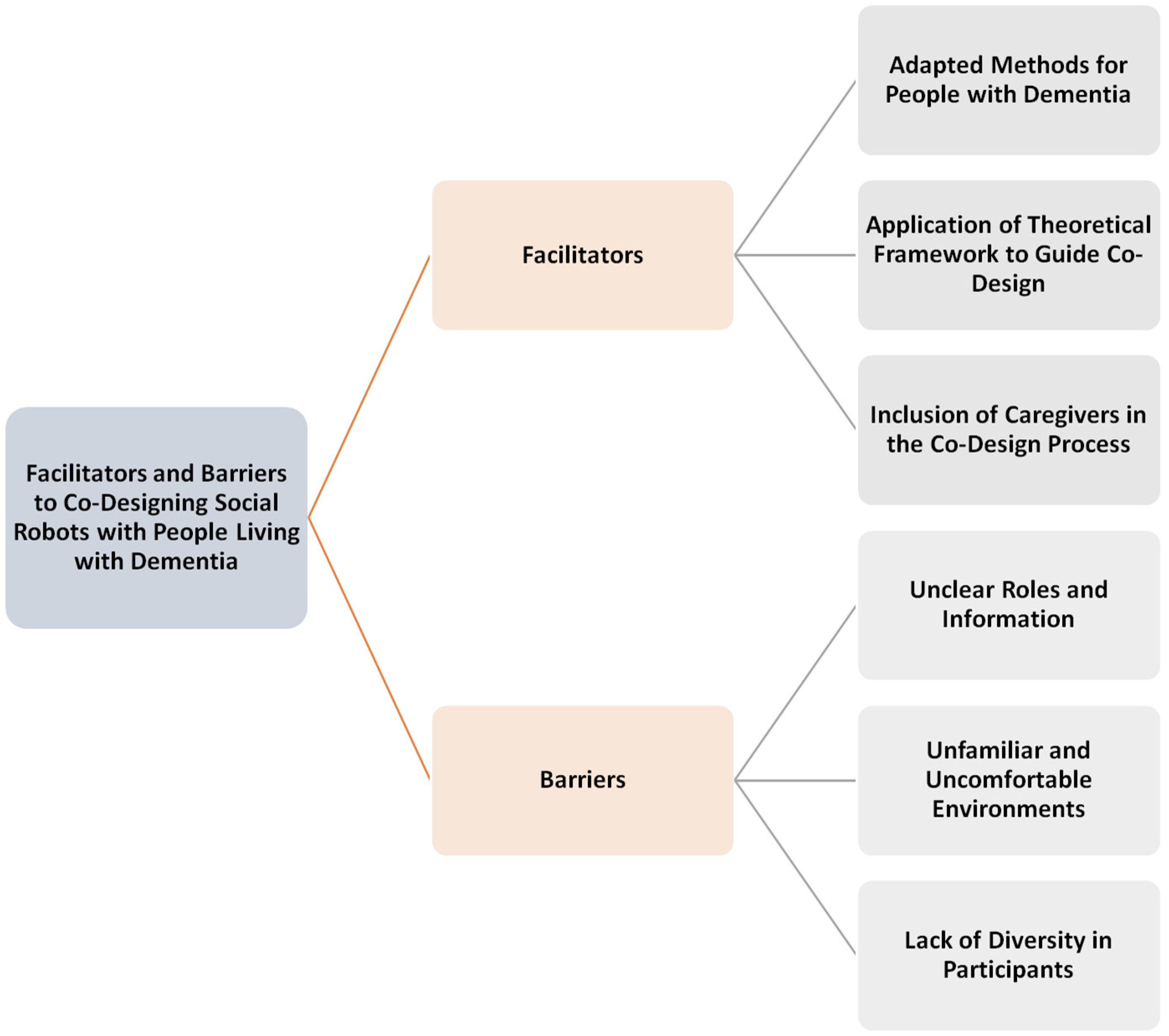
Facilitators and barriers.
Facilitators
Adapted methods for people with dementia
Most studies emphasized the importance of extended contact with social robots for older adults living with dementia in the codesign process. The interaction time ranged from 15- to 45-min sessions, weekly to daily, over 10 weeks in selected home-based studies.6,18,40,41 Increased interaction time helped participants feel more comfortable, develop a better understanding of the robots, and provide more meaningful feedback.20,42 One participant from Hsu et al.
18
study expressed their affection and engagement with the robot, stating: I think he's the cutest thing in the world. And I’d love to take him home…Well, we’ll just learn how to communicate the best we could… Take him home and show it to the kids. And they would just go crazy over it.
18
(p2679)
These studies also found that having a consistent facilitator and using the same robot across sessions helped support participant engagement, provided comfort, and reduced anxiety.6,18,40,41
Small group sizes (2–3 participants per session) provided more opportunities for interaction and allowed for detailed discussions and feedback on specific aspects of robot design.18,39 Additionally, regular evaluations ensured that individuals participated voluntarily and felt comfortable throughout the codesign process. 18
Conventional codesign activities may not always align with the cognitive abilities and engagement preferences of people living with dementia, which can hinder their participation. 18 To enhance engagement and accommodate the cognitive abilities of older adults living with dementia, researchers implemented several adaptations in the codesign process. Multimedia tools, such as video scenarios and screen-based games, were used to prompt engagement and help participants visualize the functions of social robots.5,40 Focus group discussions provided a structured format for participants to express their preferences and share their perspectives on robot design. 40 Additionally, placing social robots in interview areas allowed participants to interact with them while responding to questions, making feedback more relevant and experience-based. 40 To support memory and comprehension, researchers provided large-font printouts and session recaps, helping participants retain information and maintain continuity across multiple sessions. 18 Simplified design questions were also used to ensure participants could comfortably express their opinions without feeling overwhelmed. 18 To reduce social desirability bias, Gasteiger et al. 5 recommended unsupervised and voluntary interactions with robots, allowing participants to engage naturally without external influence. Similarly, unrestricted interactions, where participants explored robots at their own pace without rigid instructions, fostered a sense of autonomy and comfort. 41 These adaptations demonstrate the importance of flexibility and inclusivity in codesigning social robots with people living with dementia.
Researchers also emphasized the need for reflection throughout the codesign process. 18 Maintaining a balanced ratio of older adults and care partners in codesign sessions ensured that the perspectives of both people living with dementia and their caregivers were equally represented. 6 In some cases, conducting separate interviews with individuals with dementia and their care partners allowed participants to share their experiences more openly, without feeling influenced by their caregiver's presence. 6
Application of theoretical frameworks
The codesign activities implemented throughout the process play a crucial role in shaping the understanding and willingness of older adults living with dementia to continue participating in the design process. 18 To facilitate engagement, researchers adapted theoretical frameworks to structure codesign activities, ensuring alignment with the values and care philosophies of the care settings in which participants were living.18,40 It is important for researchers to consider whether an adapted framework aligns with the ethos of the care home or setting where participants reside to promote meaningful participation. 18
Hsu et al. 18 adapted the Eden Alternative Framework of Well-Being, which was already embedded in the memory care facility where the study took place. The Eden Alternative approach emphasizes enhancing residents’ personhood and overall well-being in dementia care. Guided by this framework, researchers integrated codesign activities into participants’ daily routines, incorporating familiar and enjoyable activities such as singing, selecting clothes, and dancing. By aligning robot design activities with everyday experiences, participants were more engaged and found greater meaning in contributing to the design process.
Cruz-Sandoval et al. 40 proposed a three-cycle approach to structure collaboration with older adults with dementia in codesign. The framework consisted of three phases: engagement, automation, and efficacy.
Engagement Cycle: Researchers conducted semi-structured interviews and focus groups with caregivers and healthcare professionals to gather insights on how to refine interactive strategies for the codesign workshops. An example of this was interactive music therapy group sessions, where participants were encouraged to engage with robots through familiar and enjoyable activities.
Automation Cycle: Based on the insights gathered, researchers developed and evaluated the autonomous functions of the SAR, focusing on preferred communication styles, response mechanisms, and music selections to ensure the robot's interactions were tailored to participants’ preferences.
Efficacy Cycle: The final phase involved 14 group therapy sessions over nine weeks, during which the SAR facilitated structured activities. The aim was to assess the long-term impact of the social robot on quality-of-life outcomes for older adults with dementia.
Inclusion of caregivers in the codesign process
Family and peer feedback play a crucial role in facilitating the codesign of social robots and encouraging participation in activities.5,6 Two studies incorporated caregivers and relatives of people living with dementia into the codesign process through semi-structured interviews, ensuring that their insights and observations informed the development of robots.39,41 Similarly, Hsu et al. 18 found that the presence of friends and spouses in codesign workshops fostered a more engaging and supportive environment, where peer-to-peer feedback and group interactions helped familiarize participants with the robot. Caregivers played a critical role in interpreting the expressions and affective responses of older adults living with dementia, enhancing researchers’ understanding of participant engagement. 6
To create a comfortable and engaging codesign experience, researchers implemented strategies such as grouping individuals with familiar peers, enabling participants to support and interact with each other. 18 This approach was particularly beneficial for individuals who were initially shy or hesitant to engage with the robots. One participant, despite facing language barriers, felt more secure, comfortable and eventually participated in codesign activities due to the positive reinforcement and encouragement from another participant. 18 The study also highlighted the importance of positive reinforcement in supporting participants’ engagement and confidence in expressing their feedback. Beyond interpersonal support, the research site itself played a key role in facilitating the codesign process. A supportive research environment—including strong collaboration with clinical staff—helped streamline participant recruitment and ensure that activities were tailored to residents’ needs. 5 Staff members, such as care home directors, who were familiar with participants’ preferences and daily routines, provided valuable insights that informed the planning of codesign activities. 18
In addition to family and peer involvement, researchers’ backgrounds and expertise also influenced the codesign experience. Wang et al. 6 emphasized that researchers with clinical and research experience in dementia care brought valuable perspectives to the process but needed to avoid making assumptions about older adults’ and caregivers’ expectations during interviews. Hsu et al. 18 further suggested the potential of intergenerational interactions, where younger participants engaged with older adults in codesign activities, promoting interest, comfort, and cross-generational learning.
Barriers
Unclear roles and information
A recurring challenge highlighted in three studies5,6,18 was the ambiguity surrounding the codesign process for social robots. Many older adults living with dementia found codesigning robots to be confusing, with some feeling unqualified to contribute their thoughts because they could not envision how social robots would be relevant to their future lives.6,18 Hsu et al. 18 further noted that some participants perceived robot design as a task meant for programmers, leading them to question their role in the codesign process. As one participant expressed: “I [was] very confused. So, what is the purpose of the [social robot]?” 18 (p2675)
Similarly, Gasteiger et al. 5 reported that instructions for installing games on social robots were unclear, and participants struggled to understand how these features could be integrated into the robot's design. The lack of clear communication and structured guidance in the codesign process led to frustration and discouragement, which in turn negatively affected group dynamics and reduced participants’ interest in engaging in future codesign research. 18
Unfamiliar and uncomfortable environments
A persistent challenge identified across all six studies was the impact of unfamiliar environments on participants’ comfort and engagement. Older adults living with dementia often experience anxiety or fear in unfamiliar spaces, which can negatively affect their perceptions of and interactions with social robots. 6 To enhance feelings of safety, Hsu et al. 18 modified the study setting, shifting from a closed-room environment to an open space, where participants could see others coming and going. This open setting provided reassurance and reduced feelings of isolation, allowing participants to engage more freely. Similarly, Gasteiger et al. 5 and Cruz-Sandoval et al. 40 conducted their studies in retirement villages and the lounges of geriatric residences, where participants already lived and felt familiar with their surroundings.
Lack of diversity in participants
Two of the included studies18,39 identified the limited diversity of participants as a challenge in the codesign process. Hsu et al. 18 suggested that participants’ backgrounds could influence their openness to technology and the extent of their engagement with researchers, potentially affecting the codesign process. Similarly, Mitchell and Zhao 39 highlighted the lack of representation from individuals with diverse cultural backgrounds and demographic characteristics, limiting the range of perspectives incorporated into social robot design.
Discussion
This scoping review highlighted that research on codesigning social robots with people living with dementia remains limited. Although the concept of codesign is increasingly emphasized in dementia care, our findings reveal inconsistencies in its application and reporting across studies. In many cases, the involvement of people living with dementia was limited to the later stages of development, such as usability testing or feedback on prebuilt prototypes, rather than through sustained engagement across the full design process. This suggests that while codesign is often cited as a guiding principle, its practical implementation is frequently partial or symbolic, rather than integrated and participatory. Greater transparency, methodological clarity, and earlier involvement of end users are needed to ensure that codesign efforts genuinely reflect the priorities and experiences of people living with dementia.
This review highlights the value of incorporating the broader theoretical framework of the ethics of care in the design of social robots with people living with dementia. 43 A key tenet of the ethics of care is the recognition that human beings are inherently relational, embedded in and shaped by relationships. Accordingly, the ethics of care calls for a focus not only on individuals but also on their surrounding relationships. This perspective is reflected throughout the review. The articles in our review underscore the importance of building trust among researchers, older adults living with dementia, and robots through consistent and relationship-centered engagement and a relational approach in the codesign process. For example, long-term involvement, regular introductions, assigning the same facilitators across sessions, and using the same social robots in each session helped participants feel more secure and engaged in the codesign activities. 18 Moreover, familiar and supportive individuals, such as family members, caregivers, or trusted friends, also played a vital role in fostering inclusion, reducing anxiety, and enhancing participation.5,18,39,41
Another key feature of the ethics of care is the emphasis on contextual factors. This is also evident in the facilitators and barriers identified in the review. For example, people living with dementia may face challenges in participating without appropriate support; however, when methods are adapted to their specific needs, meaningful engagement becomes possible. Examples include smaller group sizes, the use of multimedia tools, and large-font printouts and written session recaps.18,39 Clear and precise communication is also essential, as some individuals may have shorter attention spans. 42 Additionally, the frequency and duration of sessions played a crucial role in enhancing codesign experiences. Repeated sessions helped participants gradually become familiar with the activities, facilitators, and social robots.18,40 Shorter sessions, such as those implemented in Hsu et al., 18 were particularly effective in preventing fatigue and maintaining engagement among older adults with dementia. Moreover, the physical and emotional environment played a vital role. Unfamiliar or uncomfortable settings could provoke anxiety and limit participation. Familiar and supportive environments, such as open spaces or familiar places where participants reside, help reduce stress and promote active engagement, allowing participants to feel more comfortable sharing their feelings.5,6,18,40,44 These findings highlight the importance of designing codesign processes that are not only inclusive but also attuned to the relational and environmental contexts in which people with dementia live and interact.
Despite the above-mentioned strategies on gathering input from participants with dementia, most studies still used traditional methods such as focus groups and interviews to collect feedback. Many of the included studies involved participants who were able to engage in verbal communication. There is a critical gap in understanding how to codesign social robots with individuals in the moderate to later stages of dementia, where verbal communication may be limited or nonexistent. Future research should explore intuitive, nonverbal interaction methods that better align with the cognitive and communication needs of this population, such as arts-based approaches, interactive storytelling, gesture recognition, touch-based interfaces, or emotion-based communication systems, or other creative techniques to accommodate diverse communication needs across all stages of dementia.
Additionally, there is a limited use of codesign frameworks to structure, execute, and evaluate codesign activities. The absence of a structured approach may lead researchers to overlook opportunities to involve participants at different stages of the codesign journey. Most studies included in the review engaged people with dementia only in the later phase to test and evaluate robots that had already been designed, rather than involving them in the planning and conceptualization of social robots. While not all individuals with dementia may wish to participate in every phase of codesign, having a well-defined framework can provide options for participation at different levels, ensuring authentic involvement and avoiding researcher-driven assumptions about participants’ roles. Embedding codesign in all stages, from needs identification to prototyping and implementation, would enable more meaningful and equitable collaboration.
Few studies discussed the role of constant evaluations and critical reflections by the researchers and the research team in addressing potential biases and assumptions in the codesign process. Future research should incorporate critical reflection sessions where research teams examine their own biases, assumptions, and decision-making processes throughout the study. Encouraging researchers and trainees to share lessons learned from their codesign experiences can further refine methods and promote more inclusive engagement with people living with dementia.
Finally, a significant limitation in existing studies is the lack of demographic diversity among participants. Most studies did not clearly document participant demographics, which limits insights into how different cultural, socioeconomic, and linguistic backgrounds may influence experiences with social robots. Given that social robots are intended for broad use, future research should prioritize diversity in participant recruitment to ensure that codesigned robots meet the needs of underrepresented populations.
Practical tips for co-designing social robots with people living with dementia
Based on the results, eight practical tips are recommended for future researchers to consider when codesigning social robots with people living with dementia. The easy-to-remember acronym, “INCLUSIVE,” which reflects the goal of making the codesign process more inclusive for people living with dementia.
Strengths and limitations
This scoping review was strengthened by an interdisciplinary approach, integrating insights from co-authors with lived experience of dementia and experts from multiple disciplinary backgrounds. The involvement of diverse perspectives enriched data interpretation, challenged assumptions, and provided a more holistic understanding of the facilitators and barriers in codesigning social robots. The inclusion of person living with dementia in the review process ensured that findings remained relevant, meaningful, and grounded in lived experience.
However, a key limitation of this review was the language restriction—only English-language publications were included, which may have resulted in the exclusion of studies published in other languages. This limitation underscores the need for future reviews to explore research published in multiple languages to capture broader, cross-cultural perspectives on the codesign process.
Conclusion
Codesigning social robots with older adults living with dementia and their caregivers is an innovative approach that empowers individuals to shape technologies that enhance their quality of life. This review highlights key facilitators and barriers. To guide future research, we propose the INCLUSIVE framework to support meaningful participation, ensuring social robots are truly beneficial and responsive to older people living with dementia. Future research must refine codesign methodologies, prioritize the specific needs of older adults living with dementia, and create supportive environments to honor the voices and preferences of these individuals.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251365066 - Supplemental material for Facilitators and barriers to codesigning social robots with older adults living with dementia: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251365066 for Facilitators and barriers to codesigning social robots with older adults living with dementia: A scoping review by Lillian Hung, Irene Chen, Joey Wong, Yong Zhao and Karen Lok Yi Wong, Sadaf Murad-Kassam, Lynn Jackson in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251365066 - Supplemental material for Facilitators and barriers to codesigning social robots with older adults living with dementia: A scoping review
Supplemental material, sj-docx-2-dhj-10.1177_20552076251365066 for Facilitators and barriers to codesigning social robots with older adults living with dementia: A scoping review by Lillian Hung, Irene Chen, Joey Wong, Yong Zhao and Karen Lok Yi Wong, Sadaf Murad-Kassam, Lynn Jackson in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors want to thank Katherine Miller, the Medical Research Librarian, at the University of British Columbia for her assistance.
Ethical approval
There are no human participants in this article, and informed consent is not required.
Author contributions
LH and IC conceived the scoping review concept and research questions, working closely with patient partner LJ on study design. IC, KLYW, SM, YZ, and JW contributed substantially to the first draft of the manuscript. LH and LJ critically reviewed and refined the scoping review. All authors approved the final manuscript and take responsibility for their contributions, ensuring its accuracy and integrity. LH and IC assumed responsibility for the overall content, including the study's design, integrity, and data accuracy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data supporting this review are included in this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.