
Abstract
Background
This study aims to explore the factors related to fact-checking health information and the moderating role of gender on the effects of explored factors. Based on social cognitive theory (SCT) and social role theory (SRT), we established a research model to explore the factors of fact-checking on health information and the role of gender.
Methods
To validate the research model, data were collected by survey method and analyzed by partial least squares technique.
Results
The analysis results present that personal factors (self-efficacy and outcome expectancy), and environmental factors (perceived skepticism and perceived ambiguity) have significant impacts on fact-checking about health information. Meanwhile, our results reveal that gender moderates the effects of outcome expectancy, perceived skepticism, and perceived ambiguity on users’ fact-checking.
Conclusion
Our study uses SCT to explore the factors impacting fact-checking, while we combine it with SRT to understand the gender differences in the process of fact-checking health information in social networking sites.
Keywords
Introduction
Social networking sites (SNSs) are internet-based platforms that enable users to generate content and connect with their friends and others. 1 SNSs changed the way people socialize and promoted communication between users. Users can acquire and share health information on SNSs (e.g. Facebook, TikTok, WeChat, and Twitter), just for leisure or to solve the health issues they encounter in daily life. Such as COVID-19, people use SNSs to seek and share information about the crisis 2 and discuss health issues related to the crisis with other users.3,4 Therefore, SNSs could serve as an important communication platform to afford health information.
However, SNSs as a tool for communication can drive the spread of misinformation and disinformation. Misinformation and disinformation (widely considered or interchangeably with fake news) can be defined as any content such as information, news, messages, or articles that is misleading and deceptive. 5 Some studies have shown that many Nigerians are vulnerable to fake news in SNSs, 6 which negatively affects society and individuals. 7 This therefore calls for the need to assist users to become less vulnerable to misinformation and disinformation on SNSs, especially in the field of health. Almost anyone can post health information on SNSs. Some studies have shown that during COVID-19, a large amount of vague and incorrect health information was disseminated in SNSs leading to information overload in countries around the world.8–11 Meanwhile, the quality of health information posted on TikTok has raised concerns about the spread of unverified information causing social media fatigue among the public.12,13 Users may even unconsciously encounter various forms of misinformation and disinformation in SNSs, which might hinder individuals’ engagement in health behaviors. 14 For example, studies in Iran and Spain have shown that false statements about adverse side effects of vaccines increase vaccine hesitancy and potential health risks for people.15,16 Therefore, fact-checking before sharing on SNSs is critical to reducing disinformation and misinformation.
Fact-checking refers to users verifying information posted on SNSs that they will share with other users or use for their own needs. Users may or may not check the information accurately, but their efforts on fact-checking would contribute to alleviating the possibility of accepting inaccurate information in SNSs. Therefore, we focus on the act of fact-checking in this study. The existing literature on fact-checking health information focuses on a single aspect of environmental or cognitive influences.17–19 Although some studies have shown that personal factors influencing fact-checking online health information include information literacy,
17
metacognition,
20
altruism, and personal norms,
21
environmental factors have been neglected. In addition, some studies have also emphasized the influence of environmental factors on fact-checking online health information, such as threat appraisal,
18
perceived authenticity,
22
social media fatigue,
23
and message type,
24
but have not adequately considered the influence of personal factors (The details of our literature review are in Appendix A). Thus, we ground on the three main factors in social cognitive theory (SCT) which include environmental, personal, and behavioral factors to explore factors of fact-checking and their impacts. Meanwhile, males and females play different social roles that may affect their social behaviors.25,26 Given fact-checking in SNSs is a kind of social behavior that impacts people's social interaction with others in SNSs, males and females may behave differently in fact-checking health information on SNSs. Gender differences are shown in information sharing,27,28 information seeking,29,30 and information technology usage.31,32 However, few studies have examined the role of gender in fact-checking health information on SNSs. Therefore, social role theory (SRT) could complement SCT to understand the gender differences in the process of fact-checking health information in SNSs. By following problematization approach,
33
we challenge the assumptions of existing literature that neglect the contextual characteristics of fact-checking health information in SNSs by adopting a systematic theoretical view to include contextual characteristics from environmental and personal perspectives. Meanwhile, we also problematize existing literature by clarifying one of the boundary conditions of fact-checking health information in SNSs. Therefore, this study proposes two research questions:
What are the factors influencing users’ fact-checking on SNSs? How could gender moderate the effects of the above factors of fact-checking?
To address the above research questions, we developed a research model based on SCT to explore the factors of fact-checking and SRT to understand the moderating role of gender. An anonymized survey was conducted to validate the research model. Discussion, implications, limitations, and future directions are provided based on the analysis results. This study has three main contributions: First, whereas existing studies typically adopt a single theoretical perspective, we integrate SCT and SRT to provide a more comprehensive explanation of the motivations for fact-checking health information on SNSs. Second, although previous studies have explored fact-checking on health information, few studies focus on gender differences in fact-checking health information on SNSs, a gap that has important implications for public health interventions. Third, our findings can directly guide the design of gender-specific strategies to combat health-related misinformation and disinformation, providing policymakers and regulators with actionable insights to reduce the risk of health-related misinformation and disinformation among gender-specific user groups.
Objectives of the study
Based on two research questions of this study, this study aims to:
To explore the effects of personal factors (self-efficacy, outcome expectancy) and environmental factors (perceived skepticism, perceived ambiguity) on fact-checking health information on SNSs based on SCT. To examine gender moderates the role of the above factors of fact-checking and utilizing SRT to explain behavioral differences between males and females.
Theoretical foundation
Social cognitive theory
SCT proposes that individuals can learn by observing and imitating others and acting in a social environment. 34 Individual behavior changes are not only affected by personal cognitive factors but also by environmental factors. The personal and environmental factors interact with people's behaviors dynamically with feedback loops. According to SCT, individual cognitive factors describe the individual's perceived ability to perform a behavior successfully and the likelihood that this behavior may lead to a particular outcome. 35 Environmental factors reflect the characteristics of the information environment in SNSs. Thus, people's fact-checking not only comes from personal motivation but is also influenced by environmental factors perceived by participants, we leverage SCT to support our theorizing of fact-checking.
Among the personal factors, two factors are emphasized: self-efficacy and outcome expectancy. 34 To be specific, self-efficacy emphasizes the judgment about an individual's ability to complete certain tasks, while outcome expectancy reflects the individual's judgment about the possible outcome of the task. When faced with fact-checking online health information, individuals have an incentive to persist only if they believe in their abilities to obtain the intended outcome, such as reputation and recognition. Thus, self-efficacy and outcome expectancy are critical for fact-checking which requires individuals’ active involvement. In addition, according to Bandura (2001), 36 motivation and action depend largely on the social environments that person's perception. SNSs as a tool for communication can drive the spread of misinformation and disinformation,37,38 which may amplify individuals’ perceived ambiguity and perceived skepticism of online information,22,39,40 and hinder individuals’ engagement in health behaviors. Therefore, we propose two factors related to the attributes of information that may trigger people to verify whether the information is authentic or useful: perceived skepticism and perceived ambiguity. Based on this theory, we explore the factors that impact people's fact-checking from a personal and environmental perspective. To be specific, we use self-efficacy and outcome expectancy as the personal factors, while perceived skepticism and perceived ambiguity as the environmental factors.
Social role theory
The moderating role of gender is understood based on SRT in our study. The different division of social roles between males and females leads to gender differences in social behavior. 25 The social role of the male is independent and competent, while the social role of the female is friendly and unselfish. 25 In terms of processing and judging information, males are “selective processors,” task-oriented, and goal-oriented, 41 while females are “comprehensive processors,” focusing on the internal relationships between things. 42 Meanwhile, males tend to have confident and independent behavioral patterns, while females tend to have facilitating and friendly behaviors. 43 Therefore, given fact-checking of health information may involve their social networks, they would behave differently in line with their gender. Therefore, we can use SRT to understand the differential effect of gender.
Previous studies have used SRT to explain the moderating role of gender. For example, Goh and Zhang (2025) used SRT to investigate gender differences in the way they use the internet. 44 Li et al. (2021) studied gender differences in information disclosure in location-based services based on SRT. 45 Wu & Zheng (2023) investigated gender differences in social media overload drawing from SRT. 46 Therefore, it is validated to apply SRT to analyze gender differences.
To conclude, our study uses SCT to explore the factors impacting fact-checking, while we combine it with SRT to understand the gender differences in the process of fact-checking health information in SNSs. We integrate SCT and SRT for two reasons: First, SRT could complement SCT to understand the gender differences in the process of fact-checking health information in SNSs. While SCT identifies pervasive drivers of fact-checking behavior, it cannot explain gender differences. SRT can fill the gap that the different division of social roles between males and females leads to gender differences in fact-checking. Second, integrating SCT and SRT can address the gap in the literature regarding the theoretical foundations and strengthen the rationality of the proposed model. A single theory cannot capture how social structure regulates cognitive processes. In the context of health misinformation and disinformation in SNSs, SCT suggests that users’ fact-checking is driven by personal factors (self-efficacy, outcome expectancy) and environmental factors (perceived skepticism, perceived ambiguity). SRT enhances our conceptual model by moderating the role of the above factors of fact-checking through gender. Therefore, this integration provides a more complete explanation to understand fact-checking deeper and more thoroughly.
Research model and hypothesis development
Based on SCT and SRT, we propose a research model for fact-checking health information on SNSs. We hypothesize that personal factors, which include self-efficacy and outcome expectancy, and the environmental factors which contain perceived skepticism and perceived ambiguity influence the fact-checking health information. Then, fact-checking could link to people's sharing checked facts behavior. Meanwhile, the effects of personal and environmental factors are assumed to be moderated by gender. Besides, age, education, the intensity of using SNSs, and length of using SNSs serve as control variables in this model. The hypothetical relationships are shown in Figure 1.

Research model and hypothesized relationships.
Self-efficacy and fact-checking
Bandura (1986, 1989) posited that the changeability or controllability of the environment represents individual’ beliefs and abilities to practice self-efficacy.34,47 Thus, the effect of self-efficacy on verifying health information should depend on individual beliefs. Self-efficacy refers to an individual's beliefs of completing a task and impacting effort and persistence. 48 Self-efficacy determines how long individuals will persevere and how much effort they will spend on the solution. The higher the self-efficacy, the greater the effort and persistence. 49 Thus, effort and persistence would promote conducting specific behaviors. In our study, self-efficacy would motivate people to verify information when the information environment of SNSs is cluttered. Because self-efficacy determines people's effort and persistence to verify the disinformation and misinformation, then people would spend effort to find and verify the health information on SNSs. Therefore, we hypothesize that:
H1: Self-efficacy positively affects fact-checking of health information on SNSs.
Outcome expectancy and fact-checking
Bandura (1986) noted that outcome expectancy is a necessary component for the individual to perceive control or action. 34 Outcome expectancy focuses on the results that an action will bring. Thus, outcome expectancy refers to the individual's judgment of probable outcome, which is mainly related to the reward for completing a certain task. 34 Material rewards, reputation, and recognition are usually the expected results of the individual's behavior. The expected reward will positively motivate individual behaviors. In our study, when users find that verifying information about health information on SNSs could help them gain recognition from other users on SNSs, they perceived the recognition as a reward for themselves. Such perceived rewards may drive them to have fact-checking of health information on SNSs. Thus, we hypothesize that:
H2: Outcome expectancy positively affects fact-checking of health information on SNSs.
Perceived skepticism and fact-checking
According to Bandura (2001), motivation and action depend largely on the social environments that persons perceive. 36 Perceived skepticism refers to one's perception of doubting, disbelieving, and questioning information of health information on SNSs. 50 Such skepticism results after people question health information on SNSs and carefully consider their quality. 51 Therefore, perceived skepticism reflects the environment of SNSs. When people face health information on SNSs and question the credibility of the information, they will be acutely aware of the existence of fake information. Then, they are more likely to check whether it's fact. 52 Thus, we hypothesize that:
H3: Perceived skepticism positively affects fact-checking of health information on SNSs.
Perceived ambiguity and fact-checking
According to Hawley (2010), humans’ cognitive processes are influenced by perceived outcomes within the context of their environment, which in turn influence how certain behaviors are performed. 53 Perceived ambiguity can be defined as one's perception of the degree of uncertainty in judgment.54,55 Inaccurate health information fosters confusion and perceptions of ambiguity. 56 Perceived ambiguity may induce people's negative emotional states, such as anxiety. 57 Perceptions of uncertainty are also shown to be related to anxiety in previous literature. 58 To deal with the negative emotional states, people would take action to reduce the perception of ambiguity, such as verifying the information. In our study, when the health information disseminated is perceived as uncertain, 59 they would feel anxiety or worry about using the information. Then, they would verify the health information to reduce their anxiety or worry. Therefore, we can hypothesize that:
H4: Perceived ambiguity positively affects fact-checking of health information on SNSs.
Fact-checking and sharing checked facts
Bandura (1986) noted that human cognition affects the implementation of certain behaviors. 34 To gain personal benefits, an individual's fact-checking behavior triggers sharing checked facts. Thus, fact-checking can be defined as people's efforts to verify the existence of information through a variety of different sources.52,60 However, fact-checking is not the ultimate goal and does not produce direct feedback. To realize the value of fact-checking about health information on SNSs, people will share their checked facts to earn social benefits, such as reputation, which is an external reward that provokes people to share checked facts on SNSs.61,62 Therefore, after checking the fact of health information on SNSs, people are willing to share the checked facts to realize their value on SNSs. Thus, we hypothesize that:
H5: Fact-checking positively affects sharing checked facts about health information on SNSs.
The moderating effect of gender
To explicate gender differences in fact-checking, it is necessary to explain how males and females perceive and behave differently on SNSs. Eagly (1987, 1991) noted that females and males behave differently because of their distributions into different social roles in a specific environment.25,63 These behavioral differences are driven by the typical characteristics of roles commonly held by females and males. Females are characterized as communal, and males are characterized as agentic. 26 Genders’ social behaviors are likely to contribute to gender differences in fact-checking health information on SNSs. Thus, SRT is suitable for explaining gender differences in the influence of self-efficacy, outcome expectancy, perceived skepticism, and perceived ambiguity on fact-checking health information.
For the effect of self-efficacy, since males appear to be more confident than females in their ability to search and judge information on the SNSs, 64 they may be more likely to check the health information than females. Previous studies have shown that males have more positive computer-related self-efficacy than females.65,66 Towards the effect of outcome expectancy, since the male is task-oriented and goal-oriented, while a female is social-oriented and intrinsically compassionate, 67 males would pay more attention to the outcome of fact-checking about health information than females. Meanwhile, fact-checking is thought to be associated with a goal-oriented approach rather than a social-oriented approach. 25 Therefore, we hypothesize that:
H6a: Self-efficacy has a stronger impact on fact-checking for males than females.
H6b: Outcome expectancy has a stronger impact on fact-checking for males than females.
Regarding the effect of perceived skepticism, because a female who is considered to be a more comprehensive information processor than a male, would take more information clues, including inconsistent clues to make decisions,68,69 females are more likely to seek more clues and verify health information than males when they feel the information is suspicious. Considering the effect of perceived ambiguity, since females have a lower tolerance for ambiguity in medical information, 70 they also would have a higher propensity to reduce the ambiguity by verifying health information than males. Therefore, we hypothesize that:
H6c: Perceived skepticism has a stronger impact on fact-checking for females than males.
H6d: Perceived ambiguity has a stronger impact on fact-checking for females than males.
Research method
Measurement instrument
The survey method was chosen for this study for two reasons: First, the survey is suitable for measuring six latent constructs of this study and capturing subjective perceptions that are not directly observable. 71 Second, previous studies have shown that the survey is commonly the measurement tool of choice for studies, collecting a wide range of data about people's behaviors and attitudes, among other constructs.5,18,72 The measurement instrument was developed by adapting previously validated scales and further modified to suit the current context, as outlined in Appendix B. Items for self-efficacy were adapted from Chen et al. (2001), 73 and items for outcome expectancy were from Zmud & Robert (1999). 74 Items for perceived skepticism were from Thakor & Goneau-Lessard(2009). 75 Items for perceived ambiguity were adapted from Kardes et al. (2007). 76 Items for fact-checking were from Flanagin & Metzger (2000). 77 Items for sharing checked facts were from Lin & Wang (2020). 78 Finally, items for organizational commitment were from Herath and Rao (2009). 79 All items were measured by using a 5-point Likert scale (from “1 = strongly disagree” to “5 = strongly agree”). In addition, our study included several control variables, such as age, education, length, and experiences of using social network sites.80,81
We used a back-translation method to translate the survey instrument from English to Chinese and planned to collect data in China. 82 By following the back-translation method, one bilingual author translated the developed English version into Chinese, while another bilingual author translated the Chinese version back into English. Then they compared the back-translation version with the original one to examine the degree of consistency between the two versions. After confirming the translated survey instrument, a pilot survey was conducted by interviewing twelve social network site users. Four experts in medical informatics and information systems were also surveyed in the pilot to provide overall evaluations of the quality of our survey instrument. We revised the questionnaire according to their comments and suggestions. The questionnaire was designed by the authors and contained three sections: knowledge about fact-checking online health information, basic information and main questions. The final questionnaire is attached in Appendix C.
Data collection
In order to collect data, we chose a digital platform with paid survey services (The URL of the company is https://www.wjx.cn/). According to Gever (2024), 83 there are three reasons for choosing to collect data in digital platforms. First, data could be collected in large quantities from different sources by using digital platforms. Second, digital platforms allow for real-time data collection and monitoring which ensure timely collection of data. Third, data collection through digital platforms is more cost-effective. Therefore, it is appropriate to leverage digital platforms to collect our data.
A simple random sampling was adopted in this study. Since the aim of this study was mainly to investigate users’ fact-checking and sharing checked facts about health information on SNSs, we randomly invited respondents who had checked the facts about health information on SNSs to fill out our questionnaire through the online survey platform. Respondents obtained consent to participate in this study before completing the questionnaire. Details of the consent are presented in Appendix D. Our data collection plan has been submitted to and obtained approval from the Ethics Committee of Tongji Medical College of Huazhong University of Science and Technology (No. 2024S246).
To ensure the quality of data collection, we referred to recent guidelines for online surveys to take several actions in the data collection. 84 First, to ensure study instructions were clear, a pilot test was conducted with 20 participants. Second, participants filled out an informed consent form before they completed the questionnaires, which included verifying and blocking web robots by asking participants to correctly answer a set of tests (e.g. identifying pictures and typing words). Third, only respondents who checked their health information were invited and paid to participate in the questionnaire. Fourth, to prevent the same participant from completing the questionnaire many times, examining IP addresses and removing duplicates were applied by the market research company. To determine the required number of minimum participants, we performed the power analysis using the G∗Power. 85 Based on the input parameters, the minimum required sample size was 129 with actual power = 0.95. After 3 weeks of the survey, a total of 381 participants opened the survey, of which 46 (12.07%) had no experience with fact-checking and exited the welcome page. The study excluded 34 (10.15%) incomplete questionnaires and those who did not pass the attention traps or reverse-coded questions. A total of 301 questionnaires were retained in the study, representing a response rate of 89.9%. We finally decided on 301 valid samples that fit the minimum required sample size and were sufficient for SEM.
The demographic information of our final sample is summarized in Table 1, including age, gender, education level, experiences of using SNSs, and length of using SNSs within each day. The sample included 301 respondents, with 44.2% male and 55.8% female. The largest percentage of respondents fell within the age range of >30 years (52.2%), followed by 25–30 years (25.9%) and <25 years (21.9%). The majority of respondents held undergraduate degrees (86.4%), followed by master's degrees and above (10.6%) and high school degrees (3%). In terms of using SNSs within each day, 25.6% reported using it within 2 h each day, 55.8% used it 2–4 h each day, and 18.6% used it over 4 h each day. Regarding experiences of using SNSs, 1.3% reported using it within 1 year. 27.9% used it for 1–5 years, and 70.8% used it for 5 years or more. The sample is suitable for studying fact-checking in SNSs as its gender and age distributions are consistent with the SNS user population as released by CNNIC in 2025. 86
Demographic information of sample participants.

Data analysis
This study uses the partial least square (PLS) to analyze collected data based on SmartPLS. 87 We chose PLS for four reasons. 88 First, PLS can account for the maximum variance of the endogenous construct. Therefore, we can better predict users’ fact-checking behavior based on our proposed factors. Second, PLS is robust to models containing six observed variables and rarely faces convergence issues. Third, PLS is suitable for non-normally distributed data. By using the Shapiro–Wilk tests, we found our data is not normally distributed (p < 0.05). Fourth, this study contains 301 samples, PLS can obtain results with a smaller sample size and achieve a high level of statistical power. Therefore, PLS is suitable to be used in our study. The measurement and structural models are analyzed by PLS algorithm and bootstrapping, respectively. 89
Measurement model analysis
In Table 2, the results of reliability and convergent validity are presented. The values of Cronbach's alpha are between 0.61 and 0.88, 90 and composite reliabilities are above 0.7, 91 then, indicating good reliability for the measurement model. Meanwhile, all the values of average variance extracted (AVE) of each item are above 0.5, and item loadings are also above 0.7, indicating the measurement model has a good convergence validity. 92 Furthermore, we judge the discriminant validity by comparing the square root of the AVE of constructs with their correlation coefficients. Table 3 shows that values of the square root of AVE of each construct are larger than their correlation with other constructs, which implies a good discriminant validity for the measurement model. 93 In addition, the Heterotrait-Monotrait Ratio (HTMT) is included and Table 4 reveals that all values of HTMT in this study are less than 1.00, 94 which further strengthens the good discriminant validity of this measure. Hence, we conclude that the quality of the measurement model is sufficient to test hypothesized relationships.
Construct reliability and convergent validity.

Legends: FC: fact-checking; OE: outcome expectancy; SE: self-efficacy; SCF: sharing checked facts; PA: perceived ambiguity; PS: perceived skepticism; AVE: average variance extracted.
Discriminant validity.

Legends: FC: fact-checking; OE: outcome expectancy; SE: self-efficacy; SCF: sharing checked facts; PA: perceived ambiguity; PS: perceived skepticism.
Heterotrait-Monotrait ratio (HTMT).
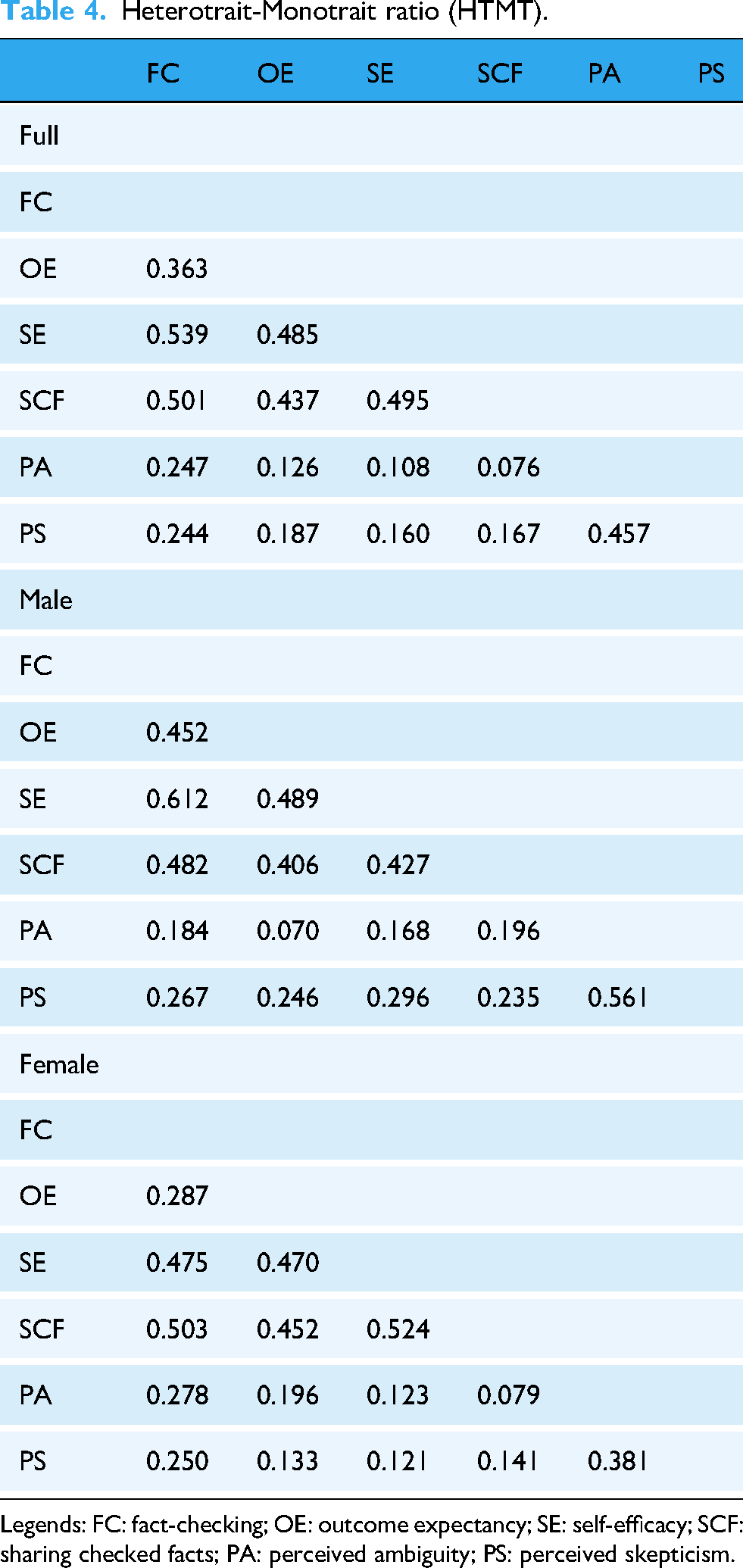
Legends: FC: fact-checking; OE: outcome expectancy; SE: self-efficacy; SCF: sharing checked facts; PA: perceived ambiguity; PS: perceived skepticism.
Given the data was obtained through a cross-sectional survey, it is important to examine whether common method bias (CMB) becomes a problem in our study. First, Harman's single-factor test was conducted by using principal component analysis. 95 The results showed the first factor in the unrotated solution explained 25.39% of the variance, which is less than 50%. Second, a marker variable technique was also used to assess the CMB. 96 We chose organizational commitment as the marker variable, which has no theoretical relevance to our research model. The analysis result presented that organizational commitment was not related to fact-checking about health information (β = 0.063, p > 0.05). Therefore, CMB was unlikely to be an issue in our study.
Structural model analysis
We examined the structural model by testing the hypothesized relationships in Table 5. It can be found that the main effects in the model have been significantly verified and analyzed. The R2 values for fact-checking and sharing checked facts in this study model were 0.208 and 0.152 both higher than 0.1, 97 indicating that the structural model in this study has an acceptable predictive ability.
Results of hypotheses testing.

Legends: FC: fact-checking; OE: outcome expectancy; SE: self-efficacy; SCF: sharing checked facts; PA: perceived ambiguity; PS: perceived skepticism.
Note: *=0.05 significance; **=0.01 significance; ***=0.001 significance.
Structural results in Figure 2, for personal factors, self-efficacy (β = 0.308, p < 0.001) and outcome expectancy (β = 0.124, p < 0.05) have a significant impact on fact-checking. Therefore, H1 and H2 are supported. Meanwhile, considering the environmental factors, both perceived skepticism (β = 0.111, p < 0.05) and perceived ambiguity (β = 0.159, p < 0.01) significantly affect fact-checking. Therefore, H3 and H4 are supported. Finally, fact-checking (β = 0.343, p < 0.001) has a significant effect on sharing checked facts. Therefore, H5 is supported. To conclude, the analysis results show that SCT is appropriate to be used in our study and has been verified in our research.

Structural results. Note: *=0.05 significance; **=0.01 significance; ***=0.001 significance.
Meanwhile, we also consider the roles of control variables, including age, education, length, and intensity of using SNSs, and find that the length of using SNSs has a significant impact on fact-checking (β = 0.124, p < 0.05) and sharing checked facts (β = 0.128, p < 0.05). In addition, age is associated with sharing checked facts significantly (β = 0.127, p < 0.05).
Moderating effect analysis
To test gender differences in this study, we used the multi-group analysis. First, separate tests were conducted for the male and female groups to obtain the path coefficients. The results are described in Table 6 and Figure 3. We then used the formula (
where Spooled = pooled estimator for the variance, t = t-statistic with N1 + N2 – 2° of freedom, SEi = standard error of path in structural model of gender i, PCi = path coefficient in structural model of gender i.) proposed by Keil et al. (2000) 98 to compare the differences in path coefficients between male and female groups (see Table 7). Figure 3 reveals that gender differences exist in our study. Especially, the R2 indicates that the research model explains 26.6% of the variance in fact-checking and 15.2% of the variance in sharing checked facts for the male subgroup. In contrast, for the female subgroup, the model accounts for 22.1% of the variance in fact-checking and 17.6% of the variance in sharing checked facts.
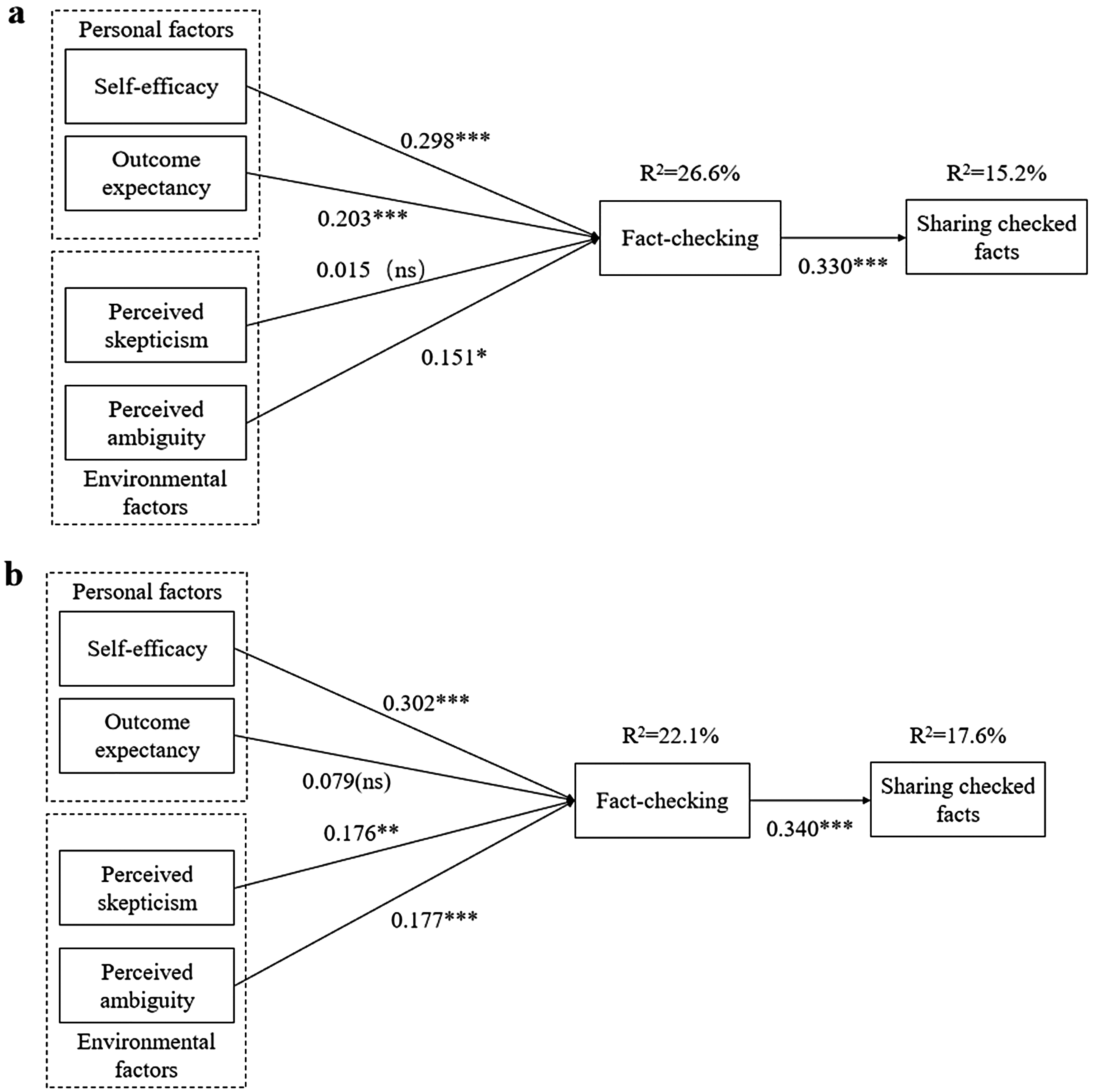
(a) PLS analysis for the male sample (N1 = 133). Note: *=0.05 significance; **=0.01 significance; ***=0.001 significance; ns = statistically not significant. (b) PLS analysis for the female sample (N2 = 168). Note: *=0.05 significance; **=0.01 significance; ***=0.001 significance; ns = statistically not significant. PLS: partial least square.
Hypotheses, path coefficients, and t-values.

Note: *=0.05 significance; **=0.01 significance; ***=0.001 significance; ns = statistically not significant.
Standardized comparisons of paths between female and male groups.
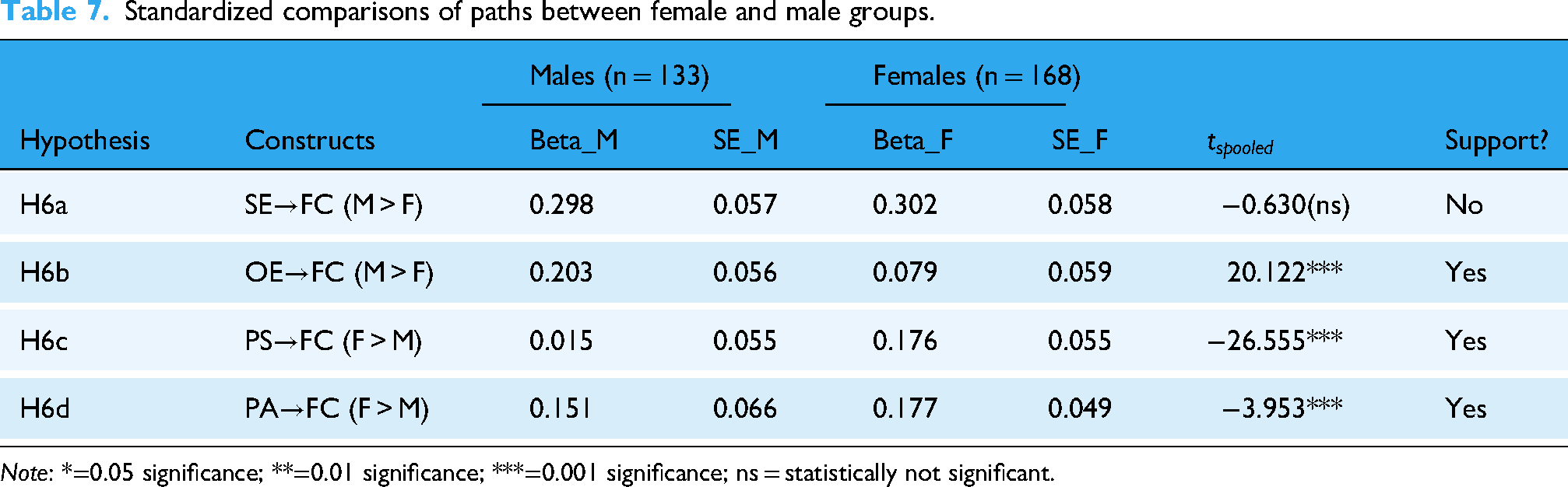
Note: *=0.05 significance; **=0.01 significance; ***=0.001 significance; ns = statistically not significant.
Based on the comparison results presented in Table 7 for personal factors, outcome expectancy has a stronger effect on fact-checking for males than for females (
Discussion
Based on SCT, we theoretically propose and validate the effect of personal and environmental factors on fact-checking. In terms of personal factors, self-efficacy (β = 0.308, p < 0.001) and outcome expectancy (β = 0.124, p < 0.05) have positive effects on fact-checking of health information on SNSs. The findings are consistent with earlier studies that found that self-efficacy99,100 and outcome expectancy101,102 significantly influence fact-checking. This suggests that individuals are more likely to engage in fact-checking health information in SNSs when they believe in their ability to obtain expected outcomes, such as reputation and recognition. Furthermore, our results indicate that self-efficacy is a stronger predictor of fact-checking than outcome expectancy. This aligns with Bandura's (2001) 36 view that capability beliefs are foundational to behavioral implementation, whereas outcome expectations are secondary motivators. Faced with cluttered information in SNSs, users need to be sure that they can discern misinformation before they consider the expected benefits of fact-checking.
From the dimension of environmental factors, perceived skepticism (β = 0.111, p < 0.05) and perceived ambiguity (β = 0.159, p < 0.01) positively influence fact-checking health information on SNSs. In addition, this study shows that people are more likely to generate skepticism after questioning health information on SNSs and carefully considering its quality, which is in line with prior literature.103,104 This suggests that individuals are more likely to fact-check online information when people question and disbelieve the credibility of the information. As highlighted by Wenzel (2019), 105 United States residents would try to find a credible source for fact-checking when they were confronted with ambiguous environments. Accordingly, this study shows that perceived ambiguity plays a crucial role in fact-checking behavior, but contradicts studies such as Guigon et al. (2024), 106 they found that the demand for disambiguating information became increasingly ineffective as individuals were attracted by the ambiguity of the news. The study indicates that fact-checking positively effects on sharing checked facts (β = 0.343, p < 0.001). The significance of fact-checking in this study aligns with previous findings107,108; however, it contradicts the findings of Anne et al.(2024), 109 they indicated that the potential limitations of fact-checking and emphasized personal ideology negatively effects on sharing checked facts on SNSs.
Based on SRT, we test the moderating effect of gender on individuals’ fact-checking about health information on SNSs empirically. To be specific, males pay more attention to the outcome expectancy of fact-checking on health information than females (
Theoretical implications
This study provides some theoretical contributions. First, we extend SCT into SNSs by dividing factors of fact-checking health information on SNSs into personal and environmental factors. Compared with previous literature, such as that by Wu (2023), 21 primarily emphasized fact-checking aspects of personal factors. They overlooked the characteristics of misinformation in SNSs. Furthermore, a recent study by Liu et.al (2021) 22 emphasized the influence of environmental factors on fact-checking but did not adequately consider the fact that fact-checking requires active involvement by individuals. To fill these gaps, we ground on solid theory-SCT by considering both personal (self-efficacy and outcome expectancy) and environmental characteristics (perceived skepticism and perceived ambiguity) to explore the factors of fact-checking health information systematically. Meanwhile, our study results also show that the proposed personal factors and environmental factors have significant impacts on fact-checking. The validated factors enrich the literature on fact-checking and reflect the characteristics of health information and SNSs.
Second, this study uses gender as a moderating variable to reflect the boundary condition of our proposed research model. Few previous literatures have focused on the moderating effect of gender on fact-checking of health information. Our analysis results show the significant moderating role of gender in the effects of personal and environmental factors which validate the core principles of Eagly and Wood (1991). 25 To be specific, males are goal-oriented, they pay more attention to the outcome of fact-checking health information. In contrast, females are social-oriented, they are more likely to be influenced by informational and environmental cues, such that perceived skepticism and perceived ambiguity of information are shown to have a stronger influence on their fact-checking of health information. Therefore, these findings connect health behavior and gender studies, providing an in-depth understanding of fact-checking health information on SNSs with gender differences.
Third, we integrate SCT and SRT to provide a comprehensive understanding of fact-checking health information on SNSs. These two theories play different but complementary roles in establishing our research model. SCT supports us in exploring the factors of fact-checking on health information, while SRT guides us in understanding the moderating effect of gender on the proposed factors. Since these two theories both concern people's behaviors in a social context, we could integrate them to better understand people's social behaviors. 115 Therefore, by integrating the two theories, we not only explore the factors on fact-checking of health information on SNSs, but also uncover gender as the boundary condition of the effects of explored factors.
Practical implications
Besides the theoretical implications, this study has practical implications. First, fact-checking of health information can be encouraged from a personal perspective. For example, policymakers and regulators should take into consideration the importance of media literacy in combating the impact of health-related disinformation and misinformation, as it may contribute to increasing users’ self-efficacy. Such improved media literacy will empower people to adequately read and assess information on SNSs before sharing it. 116 Meanwhile, the managers of SNSs could set up feedback mechanisms like highlighting real-time recognition of information verification, such as likes, and reputation ratings, 101 to stimulate verifiers’ sense of self-achievement based on the effects of outcome expectancy.
Second, fact-checking of health information also can be encouraged based on an environmental perspective. The managers of SNSs could provide alerts or notifications of potential disinformation and misinformation on SNSs. Fact-checking alerts could be flagging features applied to help users quickly spot disinformation and misinformation. The alerts could also be warnings showing that some information is highly risky and encourage users to evaluate or avoid the inaccuracy of the information carefully. In addition, the managers of SNSs could provide AI-based fact-check services that facilitate users to quickly confirm the credibility of information. 117 Meanwhile, policymakers could advocate improving individuals’ digital literacy which could improve users’ ability and awareness to discern the authenticity of information. 118
Third, gender differences should be taken into account for fact-checking about health information. Our study shows that males are more focused on outcome expectancy in fact-checking compared to females. Therefore, the managers of SNSs could use reward-based gamification elements to increase males’ extrinsic motivation 119 and enhance the fun of verifying information by males. For example, reward-based gamification elements such as badges, points, and leaderboards could be added to SNSs for fact-checking. Meanwhile, our research results show that females emphasize perceived skepticism and perceived ambiguity in fact-checking than males. Therefore, managers of SNSs could provide more targeted notifications for female users.
Limitations and future directions
This study contains some limitations. First, we focus only on the factors of fact-checking and do not consider the consequences of fact-checking in this study. Detecting the consequences of fact-checking quantitatively could help determine whether users’ fact-checking is effective. Therefore, future studies could explore the consequences of fact-checking to highlight the role of fact-checking further.
Second, more factors can be considered to study fact-checking. For example, many factors like trust or rumor awareness which have been confirmed in previous literature also could be considered in our study in the future. 52 Meanwhile, in addition to gender, future research can further explore the role of other individual differences, such as age or e-health literacy as the moderators.
Third, our study could be validated in other contexts, not just in SNSs. Our study results may be limited in understanding the fact-checking of health information on SNSs. However, people not only verify and share information in SNSs but also in other online applications or offline environments. Therefore, in the future, we can explore factors of fact-checking on other sensitive topics in other contexts.
Fourth, our study used a cross-sectional survey, in which the dynamics of constructs may not be captured. The variables included in our study may be changed over time. Meanwhile, since the measurements of independent and dependent variables were performed at the same point in time, the time sequence of the change of independent and dependent variables could not be shown in the cross-sectional survey. Therefore, future studies can use longitudinal research designs to collect data on different variables at different times.
Conclusions
Based on SCT and SRT, we proposed a research model to explore the factors related to fact-checking health information and the moderating role of gender on the impacts of the explored factors. Our study results support the effect of explored factors on users’ fact-checking. Meanwhile, gender is shown to moderate the effects of outcome expectancy, perceived skepticism, and perceived ambiguity but not on self-efficacy. Our study shows the necessity of encouraging users’ fact-checking on health information and provides guidance for managers and policymakers of SNSs in motivating fact-checking.
Footnotes
Acknowledgments
This work partially was supported by a grant from the National Natural Science Foundation of China (72004071 and 72474074), grants from the Fundamental Research Funds for the Central Universities (2024WKYXQN005).
Ethical considerations
This study received ethical approval from the author's institutional review board in 2024 (No. 2024S246). Respondents gave written consent for the survey and signature before starting interviews.
Authorship contribution statement
JX contributed to formal analysis, investigation, and writing—original draft. TW contributed to conceptualization, methodology, writing—review & editing, and supervision. ZC contributed to writing—review & editing. LZ contributed to review & editing, project administration, and funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work partially was supported by a grant from the National Natural Science Foundation of China (72004071 and 72474074), grants from the Fundamental Research Funds for the Central Universities (2024WKYXQN005).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix A. Literature review of fact-checking of health information on SNSs
To understand the literature of fact-checking of online health information systematically and comprehensively, we survey previous literature and present the result in Table 1. We summarize previous literature from four aspects: authors and years, Theory, IVs, and Findings. According to Table 1, The existing literature on fact-checking online health information focuses on a single aspect of environmental or cognitive influences. Meanwhile, few studies integrate both personal and environmental factors to study the factors of online health information fact-checking. Therefore, we challenge the assumptions of existing literature that neglect the contextual characteristics of fact-checking health information in SNSs by adopting a systematic theoretical view to include contextual characteristics from environmental and personal pe rspectives.
Literature review of fact-checking of health information on SNSs
Authors and years
Theory
Ivs
Findings
Liu et.al (2021)1
stimulus-organism-response model (SOR)
perceived authenticity
perceived importance
perceived trustThe result indicates that the positive effect of perceived authenticity and perceived importance have positive effects on verifying rumors, while perceived trust has a negative effect on verifying rumors.
Wu (2023)2
Influence of Presumed Media
Influence (IPMI) modelAttitude
Personal norms
AltruismThe result indicates that the applicability of the IPMI model is in the context of fact-checking health information on social media before sharing.
Khan and Idris
(2019)3Theory of Reasoned Action (TRA)
Information literacy
Attitude
Background factorsThe results show that combat misinformation on social media is explained by income and level of education, information literacy, and attitude toward information verification.
Kožuh and
Čakš (2023)4/
Fact-checking intent
News literacy
News trustThe findings reveal that users’ intent to fact-check information in social media is predicted by news literacy, news trust, and fact-checking.
Sun and Ma
(2023)5Protection motivation theory (PMT)
Threat appraisal
Coping appraisalThe results show that threat appraisal and coping appraisal impact fact-checking behavioral intentions.
Schuetz et.al
(2021)6/
Awareness
Active social media use
Social media homophilyThe results show that awareness of fake news and active social media use enhance fact-checking of COVID-19 fake news, while social media homogeneity reduces
COVID-19 fact-checking.
Lee and
Romazan
(2021)7/
Media literacy
MetacognitionThe results show that media literacy is positively associated with health information fact-checking behavior. In addition, metacognition mediates the positive correlation between media literacy and fact- checking behavior.
Sharma and
Kapoor
(2022)8Heuristic systemic model (HSM)
Cognitive overload theory (COT)Message polarity
(positive versus negative) Message type
(news versus rumors)The results show that for the Indian users, a message with negative polarity results in higher verification behavior. On the contrary, for US users, messages with positive polarity lead to higher behavioral intentions.
Zhou
et.al.(2025)9/
Passive versus active social media involvement
Social media fatigueThe results present that passive and active social media involvement is negatively and positively associated with health information fact-checking, respectively. Besides, the relationships between the two ways of social media involvement and health information fact-checking are mediated by social media fatigue.
1. Liu Y, Jiang Y, Zhang S, et al. Verifying Online Health Rumors on Social Media: An Empirical Research Based on the Stimulus -Organism-Response Framework. WHICEB 2021 Proceedings 2021; 46.
2. Wu Y. Predicting Fact-Checking Health Information Before Sharing Among People with Different Levels of Altruism: Based on the Influence of Presumed Media Influence. Psychology Research and Behavior Management 2023; 16: 1495-1508. DOI: 10.2147/PRBM.S404911.
3. Khan ML and Idris IK. Recognise misinformation and verify before sharing: a reasoned action and information literacy perspective. Behaviour & Information Technology 2019; 38: 1194-1212. DOI: 10.1080/0144929X.2019.1578828.
4. Kožuh I and Čakš P. Social Media Fact-Checking: The Effects of News Literacy and News Trust on the Intent to Verify Health-Related Information. Healthcare 2023; 11: 2796.
5. Sun M and Ma X. Combating health misinformation on social media through fact-checking: The effect of threat appraisal, coping appraisal, and empathy. Telematics and
Informatics 2023; 84: 102031. DOI: https://doi.org/10.1016/j.tele.2023.102031.
6. Schuetz SW, Sykes TA and Venkatesh V. Combating COVID-19 fake news on social media through fact checking: antecedents and consequences. Eur J Inform Syst 2021;
30: 376-388. DOI: 10.1080/0960085X.2021.1895682.
7. Lee DKL and and Ramazan O. Fact-Checking of Health Information: The Effect of Media Literacy, Metacognition and Health Information Exposure. Journal of Health Communication 2021; 26: 491-500. DOI: 10.1080/10810730.2021.1955312.
8. Sharma A and Kapoor PS. Message sharing and verification behaviour on social media during the COVID-19 pandemic: a study in the context of India and the USA. Online Information Review 2022; 46: 22-39. DOI: 10.1108/OIR-07-2020-0282.
9. Zhou X, Wenjing P and and Jiang S. Combating Health Misinformation Through Fact-Checking: The Role of Active Versus Passive Social Media Involvement. International Journal of Human–Computer Interaction 2025: 1-14. DOI: 10.1080/10447318.2025.2476705.
Appendix B. Constructs and measurements
Constructs
Items
Sources
Self-efficacy
1. I am confident that I will be able to achieve the goal of verifying health information.
2. I can overcome the challenges of verifying health information if I invest the necessary effort.Chen et al., (2001)1
Outcome expectancy
If I verify health information:
1. My peers on social network sites will perceive me as competent.
2. I will increase my sense of accomplishment.
3. I will be seen as higher in status by my peers on social network sites.Zmud & Robert, (1999)2
Perceived skepticism
1. In general, health information in the SNSs does not present a true picture of the risks associated with health issues.
2. The messages conveyed in health information in the SNSs do not show life as it really is.
3. The consequences shown in most health information in the SNSs are not realistic.Thakor & Goneau-Lessard, (2009)3
Perceived ambiguity
1. I am struggling to make a decision using the health information on SNSs.
2. I feel uncertain about using health information on SNSs.Kardes et al., (2007)4
Fact-checking
1. I will seek out other sources to validate health information.
2. I will check to see who the author of the health information is.
3. I will verify the qualifications or credentials of the author of health information.Flanagin & Metzger, (2000)5
Sharing checked facts
1. I intend to share verified health information on SNSs in the future.
2. I plan to share verified health information on SNSs.
3. I will try to share verified health information on SNSs in my daily life.Lin & Wang, (2020)6
Organizational
commitment1.I am willing to put in a great deal of effort, beyond what is normally expected, in order to help my organization be successful.
2. I really care about the fate of my organization.
3. I really care about the fate of my organization.Herath and Rao
(2009)7
1. Chen G, Gully SM and Eden D. Validation of a New General Self-Efficacy Scale. Organizational Research Methods 2001; 4: 62-83. DOI: 10.1177/109442810141004.
2. Zmud and Robert. Social Cognitive Theory and Individual Reactions to Computing Technology: A Longitudinal Study. MIS Quarterly 1999; 23: 145-158. DOI: 10.2307/249749.
3. Thakor M and Goneau-Lessard K. Development of a scale to measure skepticism of social adverting among adolescents. Journal of Business Research 2009; 62: 1342-1349. DOI: 10.1016/j.jbusres.2008.10.023.
4. Kardes FR, Fennis BM, Hirt ER, et al. The Role of the Need for Cognitive Closure in the Effectiveness of the Disrupt-Then-Reframe Influence Technique. Journal of Consumer Research 2007; 34: 377-385. DOI: 10.1086/518541.
5. Flanagin A and Metzger M. Perceptions of Internet Information Credibility. Journalism & Mass Communication Quarterly 2000; 77: 515-540. DOI: 10.1177/107769900007700304.
6. Lin X and Wang X. Examining gender differences in people's information-sharing decisions on social networking sites. International Journal of Information Management 2020; 50: 45-56. DOI: https://doi.org/10.1016/j.ijinfomgt.2019.05.004.
7. Herath T and Rao HR. Protection motivation and deterrence: a framework for security policy compliance in organisations. Eur J Inform Syst 2009; 18: 106-125.
Appendix C. Detail of the full questionnaire
Dear Sir/Madam
I would like to invite you to participate in this survey, which will make an important contribution to the research on “Fact-checking of health information on Social Networking Sites”. Your participation in this survey is totally voluntary and you can withdraw at any time.
The information collected in this survey will be used for research purposes exclusively, and no personal or identifiable information will be collected. By proceeding with this survey, you indicate that you have read this consent form and agree to participate in this study. Please be assured that you will not be personally identifiable in any reports or publications generated from this study.
1. Which social networking sites have you used recently? (Multiple choice)
□ WeChat □ Weibo □ Tiktok □ Rednote □ Other: ___________
2. Have you ever fact-checked health information on social networking sites?
○ Yes ○ No (automatically withdraw from the questionnaire)
3.What are your main channels for fact-checking online health information? (Multiple choice)
□ Government websites (e.g., WHO, NHC)
□ Peer-reviewed scientific journals
□ Official government social networking site accounts
□ Social networking sites opinion leaders
□ Other: ___________
4. What are the main forms of sharing verified health information on social networking sites? (Multiple choice)
□ Original posts □ Reposts/shares □ Comments □ Likes □ Other: ___________
5. How often do you roughly share health-related information on social networking sites?
○Once each year ○Once each month ○Once each week
○Once each day ○ Multiple times daily
6. Your age:
○ <18 years old
○ 18-25 years old
○ 25-30 years old
○ >30 years old
7. Your Gender:
○ Male ○ Female
8. Your Level of Education:
○High school ○Undergraduate degree ○Master’s degree and above
9. Up to now, how long have you been using social networking sites:
○ Within 6 months ○ 6 months to 1 year ○ 1-3 years ○ 3 -5 years ○ Over 5 years
10.How much time on average do you spend on social networking sites a day?
○Within 1 hour ○1-2 hours ○ 2-3 hours ○3-4 hours ○ Over 4 hours
11. How do you feel about your health status?
○Strongly unhealthy ○ Unhealthy ○ Neutral ○ Healthy ○Strongly healthy
Please answer the following questions according to your experience with fact-checking and sharing health information on social networking sites.
Questions
Options
I am confident that I will be able to achieve the goal of verifying health information.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I can overcome the challenges of verifying health information if I invest the necessary effort.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
My peers on social network sites will perceive me as competent.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I will increase my sense of accomplishment.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I will be seen as higher in status by my peers on social network sites.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
In general, health information in the SNSs does not present a true picture of the risks associated with health issues.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
The messages conveyed in health information in the SNSs do not show life as it really is.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
The consequences shown in most health information in the SNSs are not realistic.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I am struggling to make a decision using the health information on SNSs.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I feel uncertain about using health information on SNSs.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I will seek out other sources to validate health information.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I will check to see who the author of the health information is.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I will verify the qualifications or credentials of the author of health information.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I intend to share verified health information on SNSs in the future.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I plan to share verified health information on SNSs.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I will try to share verified health information on SNSs in my daily life.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I am willing to put in a great deal of effort, beyond what is normally expected, in order to help my organization be successful.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
I really care about the fate of my organization.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
For me, my organization is the best of all possible organizations for which to work.
1-Strongly disagree 2-Disagree
3-Neutral 4-Agree 5- Strongly agree
Appendix D. Survey Participation Consent Form
Researchers at Huazhong University of Science and Technology invite you to participate in a research study. The aim of this study is to explore the factors related to fact-checking of health information on Social Networking Sites. Your participation in this survey is totally voluntary and you can withdraw at any time.
The information collected in this survey will be used for research purposes exclusively, and no personal or identifiable information will be collected.
By proceeding with this survey, you indicate that you have read this consent form and agree to participate in this study. Please be assured that you will not be personally identifiable in any reports or publications generated from this study.